
ABSTRACT
Severe acute respiratory syndrome coronavirus 2 related disease (COVID-19) is now responsible for one of the most challenging and concerning pandemics. By August 2020, there were almost 20 million confirmed cases worldwide and well over half-million deaths. Since there is still no effective treatment or vaccine, non-pharmaceutical interventions have been implemented in an attempt to contain the spread of the virus. During times of quarantine, immunization practices in all age groups, especially routine childhood vaccines, have also been interrupted, delayed, re-organized, or completely suspended. Numerous high-income as well as low- and middle-income countries are now experiencing a rapid decline in childhood immunization coverage rates. We will, inevitably, see serious consequences related to suboptimal control of vaccine-preventable diseases (VPDs) in children concurrent with or following the pandemic. Routine pediatric immunizations of individual children at clinics, mass vaccination campaigns, and surveillance for VPDs must continue as much as possible during pandemic.
In December 2019, a novel coronavirus, SARS-CoV-2, was first reported in Wuhan, China, and rapidly spread throughout the world, resulting in a pandemic within 3 months.Citation1 COVID-19 is the acute respiratory disease caused by this new virus. By August 2020, there were almost 20 million confirmed cases worldwide and well over half-million deaths.Citation2 Although the disease occurs in all age groups, mortality is mostly seen in older people and individuals with co-morbidities.Citation3–5 Since there is still no effective treatment or vaccine, measures implemented for the control of COVID-19 include non-pharmaceutical interventions (including serious curfews in some countries), canceling mass gathering activities, and mandating social distancing, school closures, and travel restrictions. While the impact of COVID-19 varies among countries worldwide, through these measures, societies are trying to reduce the use of healthcare facilities by decreasing the spread of the virus and minimizing virus-related morbidity and mortality rates.Citation6,Citation7 This has resulted in a disruption of commerce, travel, and health care During times of quarantine, routine health-care services and elective surgical procedures have been stopped in many health-care settings, and health-care professionals have been organized in such a way as to support or prioritize the care of increasing numbers of COVID-19 patients. At the same time, immunization practices in all age groups, especially routine childhood vaccines, have also been interrupted, delayed, re-organized, or completely suspended.Citation8 When immunization programs are stopped or interrupted for any reason, we may observe an increasing number of vaccine-preventable infections and related deaths, in addition to a fraction of the population that became susceptible to diseases that were controlled or even eliminated.Citation8 With control strategies to prevent the spread of COVID-19 affecting childhood and mass immunization campaigns worldwide, millions of children are now at risk of other deadly vaccine preventable diseases.Citation9 By contrast, in countries that are easing restrictions, there is a potential risk of outbreaks of diseases like measles, pertussis, and polio, among others.
The first epidemiological data from Wuhan showed that children make up a small portion of COVID-19 patients, and the need for intensive care among pediatric patients is very low.Citation10 Soon thereafter, data from Italy, Spain, and the United States (US), where the disease has spread widely, also showed that children constitute only a small number of hospitalized patients.Citation11–13 Infected children, as a group, seem to have a milder clinical course, lower hospitalization, and intensive care requirements, and in rare cases mortality.Citation14 Recently, case reports and case series from the United Kingdom, Italy, France, Switzerland, and the United States have raised concerns about a severe systemic disease manifestation related to SARS-CoV-2 infection in children. The US Centers for Disease Control and Prevention (CDC) has referred to this condition as “Multisystem Inflammatory Syndrome in Children (MIS-C) associated with COVID-19.”Citation15 Social distancing measures, such as closing schools and imposing lockdowns, have already had some beneficial effects on common childhood infections that are transmitted via droplets, respiratory secretions, or the fecal–oral route.Citation16 This has clearly been shown for influenza.Citation17–19 However, children remain at risk for these and other vaccine preventable diseases, particularly upon the gradual removal of isolation and quarantine conditions. Routine immunization remains a key intervention against vaccine-preventable diseases in children. Routine immunizations for pregnant women, adults, and elderly persons, and patients with chronic conditions, and higher risk, are also essential.
Routine immunizations during the COVID-19 pandemic
COVID 19 is disrupting life-saving immunization services around the world, putting millions of children – in industrialized as well as in low- and middle-income countries – at risk of vaccine-preventable diseases. Because of the risk of infection and the need to maintain physical distance during the early stages of the COVID-19 pandemic, many countries have temporarily and reasonably suspended preventive mass vaccination campaigns against diseases such as measles, polio, diphtheria, pertussis, polio, tetanus, meningitis.Citation20 Causes of the delayed/interrupted immunizations are due to parents’ fears, restrictions of movement/lockdown policies, changing priorities for COVID-19 among health-care personnel, and logistics delivery issues (i.e., vaccine transport delays). The World Health Organization (WHO), UNICEF, and GAVI, the Vaccine Alliance have reported that routine immunization programs have been substantially disrupted in at least 68 countries, affecting around 80 million children.Citation20 A further 24 million people are at risk of losing out on vaccines including measles, polio, rotavirus, meningitis, rubella, and human papillomavirus in GAVI-supported low-income countries.Citation20 Vaccines are of critical importance in these areas, which also have limited access to health services and treatments. Due to the risk of inadvertently contributing to the spread COVID-19, global health organizations have not been able to continue to support mass vaccination campaigns in some countries.Citation8,Citation21,Citation22 Of the 129 countries in which data were available, more than half reported moderate to severe disruptions, or total suspension of vaccination services during March – April 2020. There was a full cessation of routine immunizations from April 1–15, 2020 in Vietnam. In India, routine immunizations were disrupted due to health-care workers being re-organized in response to the pandemic. In Pakistan, polio catch-up immunization campaigns were postponed until June 1st, 2020.Citation8 A number of countries postponed immunization campaigns in the first 5 months of the pandemic, including: measles or measles-containing vaccines in 27 countries, inactivated polio vaccine in 7 countries, bivalent, or monovalent oral poliovirus vaccine in 39 countries, meningococcal conjugated A vaccine in 2 countries, yellow fever vaccine in 4 countries, typhoid vaccine in 2 countries, oral cholera vaccine in 5 countries, and Td (tetanus–diphtheria) vaccine in 7 countries.Citation20 While several mass immunization campaigns have been stopped to prevent the virus spreading, the results have been alarming. Diphtheria has recently resurged in countries like Venezuela, Pakistan, Nepal, Bangladesh, and Yemen where conflict and/or population displacement have seriously affected public health systems.Citation23 Cholera is now present in Bangladesh, Cameroon, Mozambique, South Sudan, and Yemen.Citation23
The WHO’s Strategic Advisory Group of Experts on Immunization issued a broader call, recommending that all preventive mass vaccination campaigns for other diseases be postponed because of social distancing issues.Citation22 The Global Polio Eradication Initiative recommended suspending polio vaccination campaigns until the second half of 2020.Citation21 As a result of the coronavirus pandemic, 46 poliovirus immunization campaigns in 38 countries, mostly in Africa have been suspended. During this time, a mutated vaccine-derived strain of poliovirus has been reported in >30 countries.Citation20 Following the suspension of these immunization activities, there has been a new polio outbreak in Niger.Citation24 In Pakistan and Afghanistan, wild poliovirus Type 1 have been reported, and cases of Type 2 poliovirus, mutated from the oral vaccine, have appeared in Chad, Ethiopia, Ghana, and Pakistan.Citation25
During the pandemic, 37 countries (home to 117 million unvaccinated children) suspended scheduled measles campaigns, and more will be postponed.Citation22 Before the pandemic, and despite the availability of an effective vaccine, the highly contagious measles virus continued to spread around the globe. In 2018, cases surged to an estimated 10 million worldwide, with 140,000 deaths, a 58% increase since 2016.Citation22 Measles outbreaks have been reported in diverse settings, including Madagascar and Ukraine.Citation26–28 In 2019, measles outbreaks infected more than 6,500 children in the Democratic Republic of the Congo where one-dose measles vaccine coverage was 57%.Citation22,Citation29 In 2019, in many countries faced vaccination coverage rates below the minimum needed for herd immunity; this posed a serious risk to children who were not vaccinated and indirectly threatened immunocompromised children and others who could not be vaccinated for other medical contraindications. Eighteen countries reported measles outbreak due to suspended measles campaigns. By 2020, 178 million people are at risk of skipping measles vaccines, according to the Measles and Rubella Initiative, even as measles flares across the globe, including in Afghanistan, Brazil, Cambodia, the Central African Republic, Iraq, Kazakhstan, Nepal, Nigeria, and Uzbekistan.Citation23
In many countries, vaccine hesitancy and refusal have become an important problem in recent years.Citation30 Several serious measles outbreaks have been seen in low- and middle-income countries (LMIC), due to other problems such as broken and underfunded health systems, which make it nearly impossible to deliver vaccines to those who need them.Citation24,Citation26 During the COVID-19 pandemic, families’ reluctance and fear to attend health-care services to administer childhood measles or measles–containing vaccines may lead to an increase in the number of unvaccinated children and further increased rates of measles disease and its complications.
The suspension of measles vaccination campaigns, which have occurred in 24 countries where measles remains an urgent health condition, could also have long-lasting implications.Citation22 Due to school closures, serious immunization disruptions may occur in countries where routine immunizations have been delivered in school settings. According to UNESCO data from April 15, 2020, 91% of the world’s school-age children have stopped their education due to the pandemic.Citation31 Measles is a disease that can cause serious morbidity and has a case-fatality rate of 0.2%, it is more highly contagious (basic reproduction rate; R0 as 12–16) than COVID-19.Citation32 If children are left unvaccinated, case numbers could quickly surge following a drop in the optimal population immunity and the suspension of these vaccination programs. Measles weaken the immune system for months or years, causing immune amnesia that leaves children susceptible to other infections.Citation33
Similarly, polio is an important concern, and suspending polio immunizations is a particularly relevant issue where the virus is likely to spread (e.g., Afghanistan and Pakistan) due to active circulation. The risk of polio spreading to other countries is real, and could negatively affect global polio eradication efforts.Citation21,Citation34
COVID-19 has virtually affected all countries of the world, regardless of their economic power, but represent a particular threat for LMIC’s, because of their limited political and economic leverage for battling the disease alongside other major problems, including efforts to control vaccine-preventable diseases. One preprint study has recently shown that, for each death caused by COVID-19 acquired from an immunization visit, there could be more than 100 children’s deaths in Africa, prevented by continuing routine immunizations. This suggests that the health benefits of deaths prevented by sustaining routine childhood immunization in Africa far outweigh the excess risk of COVID-19 deaths associated with vaccination clinic visits.Citation35 For this reason, ensuring the continuation of timely of measles and polio vaccine administration is vitally important for all countries, particularly since it is not known how long the pandemic will last. With existing inexpensive and effective vaccines, we still have a chance to control and eliminate these diseases. There is also collateral damage related to COVID-19. In the Democratic Republic of Congo, the measles epidemic since January 2020 alone has led to more than 60,000 cases and 800 deaths. Ebola, tuberculosis, and cholera are also striking the country.Citation23
After 5 months of pandemic, there is new information about the potential determinants of the decline of routine immunizations. Parental fears about potentially exposing their children to COVID-19 during routine follow-up visits may have led to the declines observed.Citation36 Some states in US have reported drops compared to the same period 1 year earlier, for measles and other vaccine preventable diseases. There, according to the Vaccines for Children Program between 2019 (January 7–April 21, 2019) and 2020 (January 6–April 19, 2020), there was a corresponding 21.5% decline in measles-containing vaccines administrations as of March 16, 2020.Citation36 In Michigan, when compared with the period from May 2016 to May 2019, approximately 50% of infants aged 5 months were up-to-date on all recommended vaccines in May 2020, while about two-thirds of children (66–68%) were up to date during the past 4 years.Citation37 In US, publicly funded vaccines including hepatitis, meningitis, polio, and rotavirus, were also sharply down compared to 2019. In New York City, vaccinations have been down 63% overall, and by 91% for children older than age two, in California, have been down 40%.Citation38 In Ohio, pediatric vaccination rates are down about 45%; where normally there were about 1,000 measles given shots in a month, in April 2020, there were just 32.Citation39 The Virginia Department of Health has reported that between March 15 and April 23, 2020, vaccinations dropped 45.7% compared to the same time period in 2019, with an 83% drop among children age 5 and younger. The human papilloma virus vaccine was among those with the largest drop-off, with65% lower coverage in 2020 than in April 2019.Citation40 During the first 3 weeks of the lockdown, the number of measles, mumps, and rubella vaccines delivered in England fell by 20%, and smaller drops were reported in infant vaccines in Scotland. In Indonesia, a recent study showed that 84% of immunization services have been disrupted by the COVID-19 pandemic, and 19.7% drop in measles–rubella vaccinations in April 2020.Citation41 In Ethiopia, when the pandemic struck, the country suspended measles campaign, though the country continues to report many new casesCitation23 Immunization coverage has dropped among adults too, due to similar concerns and fears about attending routine medical care.Citation42 In the United States, compared with May 2019, immunization rates dropped by 30% in adults, with the largest percentage drop among 19- to 49-year-olds.Citation43
A decline in immunizations could endanger the 90–95% vaccination coverage that is necessary for herd immunity against diseases such as measles, mumps, and whooping cough. Primary care vaccine intake is highest when parents feel safe, when parents receive timely notice that vaccines are due, and when health care workers have processes to ensure effective call-back and recall programs.Citation37 Despite the challenges brought on by the pandemic, several countries are making special efforts to continue immunizations.
Potential effects of existing vaccines on COVID-19 pandemic
Pneumococcal and influenza vaccines are also being discussed in the context of the COVID-19 pandemic. COVID-19 infections are severe among patients of all groups, but especially those over age 65.Citation3–5 An increase of COVID-19 frequency and mortality has also been seen in patients with chronic lung and cardiovascular diseases and diabetes, all of which are risk factors for pneumococcal infections.Citation44 Previous experience has shown that pneumococcal infection risk is also increased in patients with a previous influenza infection.Citation45 In studies conducted to date among COVID-19 patients, there is no data indicating an increased risk of pneumococcal infections; therefore, there has been no suggestion of applying pneumococcal vaccines (either conjugated or polysaccharide vaccines) to provide protection against COVID-19-associated pneumonia, including in the at-risk group of patients over 65 years of age.Citation46 A majority of countries include conjugated pneumococcal vaccines in their national childhood immunization programs and recommend conjugated and/or polysaccharide vaccines for high-risk groups and elderly people. Routine immunizations that include pneumococcal vaccines for children and high-risk adults should continue according to previously developed schedules, to reduce the need for hospital admissions for vaccine-preventable diseases.
The effect of COVID-19 on seasonal influenza epidemics is unknown at this time. However, the confluence of COVID-19 and seasonal influenza during the fall and winter of 2020–2021 might result in considerable morbidity and mortality, and stress to the health system. Health systems and all of society alike must prepare for the likelihood of co-epidemics of COVID-19 and influenza.Citation47 In the Northern hemisphere, COVID-19 began to circulate toward the end of the seasonal influenza period, and social distancing and isolation/quarantine measures have resulted in a dramatic end to the spread of influenza.Citation48 There are limited data related to co-infection rates of influenza with COVID-19.Citation8,Citation49,Citation50 As influenza vaccination rates remain suboptimal for most populations, including those at greater risk for severe COVID-19, the co-circulation of viruses may result in increased mortality risk during the upcoming influenza season. Influenza tends to peak in Europe and the US between December and April of each year, and during the months of June through August in the Southern Hemisphere, therefore, the experience of countries in the Southern Hemisphere during their winter will be informative to Northern Hemisphere countries.Citation47 The Southern Hemisphere influenza season is beginning, as of this writing, but there is only low, or even no activity reported so far, probably due to lockdowns implemented in the region.Citation51 The majority of illnesses that are being reported is COVID-19. High influenza vaccine coverage would reduce influenza-related mortality while also helping to preserve the capacity and function of the health system during circulation of both influenza and COVID-19 viruses. The goal should be to attain high influenza vaccine coverage, including near-universal coverage among health-care personnel and other high-risk groups for COVID-19.Citation47,Citation52 Improving rates of seasonal influenza vaccination is critical for the management of the influenza and COVID-19 co-circulation anticipated in the next several months and until a COVID-19 vaccine is available.
The increased susceptibility to severe disease in the elderly and those with co-morbidities for COVID19, argues for a possible alteration in anti-viral host defense mechanisms additional to immunosenescence. Previous studies showed that live vaccines (i.e., BCG, oral polio vaccine, measles) induce heterologous protection against infections, likely by inducing interferon and with a long-term boosting of innate immune immunity mechanisms.Citation53 Data from clinical studies of the oral polio vaccine show that this approach reduced infant mortality by roughly 32%, reduced the burden of bacterial diarrheal disease, and has been associated with fewer episodes of acute otitis media diagnosed by medical doctors.Citation54 Measles and smallpox vaccines have also been associated with pronounced nonspecific protective effects against infectious diseases. Recent reports indicate that COVID-19 may result in suppressed innate immune responses. Some have proposed (hypothetically) that oral poliovirus vaccine, in particular, could provide temporary protection against COVID-19. Both poliovirus and coronavirus are positive-strand RNA viruses; thus, specific innate immunity mechanisms are likely to induce and affect these viruses. Advantages of oral poliovirus vaccines are low cost, ease of administration, availability and well-known safety profile.Citation54 Further randomized controlled trials with oral poliovirus vaccine may provide some information for potential beneficial effects of COVID-19 infections.Citation55
Another controversial issue concerning vaccines is the suggested protective effect of the tuberculosis Bacillus Calmette–Guerin (BCG) vaccine on COVID-19 infections.Citation56,Citation57 Such an effect has not been demonstrated in clinical studies, and observational data have not clearly shown that, in countries where the BCG vaccine is routinely administered, the frequency and mortality of COVID-19 is less common.Citation56 It has been suggested that countries without universal policies of BCG vaccination (such as Italy, the Netherlands, and the US) have been more severely affected, compared to countries with long-standing universal BCG policies (such as Portugal).Citation56,Citation58 The attributed potential nonspecific effects of the BCG vaccine in preventing COVID-19 remain a hypothesis, given multiple confounding factors. The BCG vaccine has been used in some countries during the newborn or early infancy periods, and the BCG vaccine offers consistent protection only against severe form of tuberculosis in children, but observational studies have shown that, during childhood, vaccinated children have better overall survival rates, including when facing respiratory viruses.Citation59,Citation60 In 2018, the BCG vaccine was shown to stimulate initial immune defenses well enough that it at least partly blocked another virus given experimentally 1 month later.Citation59 The WHO, however, has recommended not using the TB vaccine to fight COVID-19 until further studies are being conducted.Citation61 As of mid-June 2020, there were ongoing clinical trials to evaluate the effect of this TB vaccine among health care workers in the Netherlands, Australia, the United States, Egypt, and France.Citation62–65
Routine immunizations in children and adults with suspected or confirmed COVID-19 infections
There is currently no evidence that vaccination would increase the risk of a child becoming infected with COVID-19, or affect the course of the disease in a child who has been inadvertently vaccinated during the asymptomatic phase or incubation period.Citation66 In general, routine infant and school-age immunization should not be postponed. Most children with COVID-19 are asymptomatic or have mild symptoms, therefore testing before vaccination is not recommended. There is no clear guidance on the administration of routine vaccines in children with COVID-19, or those who have tested positive for the virus but who have no symptoms or known contact. Individuals with signs of acute respiratory infection, including mild symptoms such as sore throat or runny nose, may postpone regular immunization until they have recovered during the COVID-19 pandemic. Anyone with suspected, possibly, or confirmed COVID-19 and those who are close to a case should not attend scheduled appointments for immunization during their isolation time. Patients with COVID-19 infections present with different symptoms and signs, including fever, cough, runny nose, and gastrointestinal issues. The presence of fever may cause confusion concerning vaccine side effects or the progression of the illness; therefore, vaccines can be postponed until illness resolution, in cases of acute febrile illness.Citation66,Citation67 The CDC recommends deferring vaccinations of anyone infected with SARS-CoV-2, regardless of symptoms, until they meet the criteria to discontinue isolation. Although mild illness is not a contraindication to vaccination, deferring makes it possible to avoid exposing health-care personnel or other patients to COVID-19. Among confirmed cases of infection, it would be reasonable to postpone vaccinations until resolution of the illness, particularly in hospitalized and moderate and severe cases. It is also prudent to delay the administration of any live vaccines among COVID-19 patients who have been treated with immunoglobulin or plasma, according to routine live vaccine use protocols. Mild symptoms such as fever and/or cough are not necessarily a contraindication for vaccination.Citation66–68 In line with normal procedures, health-care providers should make recommendations based on a risk–benefit assessment severity of symptoms and risk and severity of vaccine preventable diseases. If the practitioner decides against vaccination on that day, the normal vaccination schedule for the child should be resumed as soon as possible after he or she recovers. If post-exposure prophylaxis with vaccine or immunoglobulins is required (e.g., measles, hepatitis A, hepatitis B, rabies, meningococcus, varicella), it should be given without delay. There is no known interference between the COVID-19 test or between COVID-19 and the tuberculin test.Citation67
Vaccination of newborns is considered an essential service, particularly in low- and middle-income countries, where BCG and hepatitis B vaccine are administered before maternity discharge. In cases of mothers with a laboratory-confirmed diagnosis of COVID-19, asymptomatic newborns could be vaccinated according to local recommendations with BCG and hepatitis B vaccine. If the newborn presents COVID-19 symptoms, the BCG vaccine should be postponed and the hepatitis B vaccine might be administered within the first 24 hours of life.Citation69
Immunization measures during the COVID-19 pandemic
The WHO recommends that all routine vaccinations be administered as scheduled, even during the COVID-19 pandemic. Routine immunization sessions should continue, using special measures and precautions, to the extent possible and as permitted within the local COVID-19 response context. This includes routine immunization for infants, children, adolescents, pregnant women, high-risk groups, and adult health-care providers.Citation68 Any interrupted immunization services should be resumed and catch-up vaccinations offered as quickly as possible.Citation66
Following the existing guidelines on COVID-19 infection prevention measures during immunization sessions, health-care providers should prioritize primary series vaccinations, especially for measles–rubella- or poliomyelitis-containing vaccines and other combination vaccines. Mass vaccination campaigns should be avoided until the COVID-19 situation resolves. Newborns should be vaccinated as per the national immunization schedule in maternity hospitals, and vulnerable population groups should still receive pneumococcal and seasonal influenza vaccines.Citation66 New vaccines should be delayed from introduction to national immunization schedules. It should be communicated clearly to the community and health-care professionals alike the rationale for the inclusion of immunizations among the priority health services provided during the COVID-19 pandemic. The risks from VPDs and the benefits of vaccination should also be reiterated.Citation66,Citation67
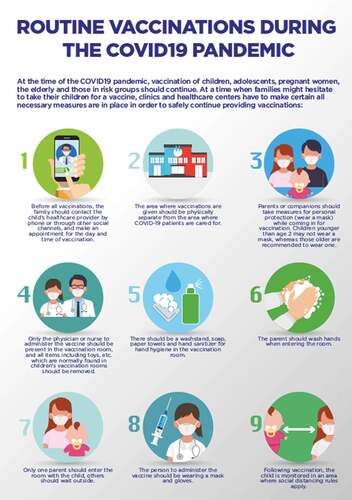
For routine pediatric immunization visits, prior to the appointment, children, parents, and caregivers should be advised not to attend if they have any COVID-19 symptoms. Control measures should include all forms of protection for vaccine providers, those being vaccinated, and those accompanying them, to reduce the risk of transmission. It is also advised that parents consider combining vaccination visits with well-baby visits and that they reduce the number of rooms visited by bundling medical examinations and vaccination services during such visits. When visiting a healthcare institution, wearing a mask is beneficial for everyone. In the US, masks are recommended for those age 2 and older, while in Europe they are suggested for those over the age of 12.Citation70 Hand hygiene facilities (soap and/or sanitizers) should also be provided. In pediatric settings, all toys should be removed from immunization rooms, and social distancing opportunities should be considered by requiring appointments (). There are no additional personal protective equipment requirements during routine immunizations; a surgical mask is sufficient. Patients should avoid crowded waiting rooms by scheduling well-checks and immunizations in advance. Only one parent (wearing a mask) should attend the immunization clinic with a child. Clinics should provide ventilated areas and ensure the feasibility of social distancing for caretakers and children awaiting immunization. For vaccines not included in national immunization programs (i.e., optional ones), the parent should collect the vaccine from a pharmacy and deliver it in accordance with cold chain transfer protocols. After the pandemic period, if some patients have missed age-appropriate immunizations, there is no need to re-start an immunization series or to add extra doses. Longer than recommended intervals between doses typically do not affect immunogenicity and potential protection. Immunization service providers should also start enumerating the cohorts of children who have missed their vaccine doses and develop an action plan for custom catch-up immunization services. All available communication technology should be used to communicate about immunization services, including setting appointments and reporting adverse events following an immunization.
Figure 1. Control measures for immumization visit during the COVID-19 Pandemic: Including appointment, wearing a mask, hand hygiene, social distancing and immunization room
Perhaps in a later phase of the pandemic, alternate locations could be considered for school or seasonal influenza vaccinations, while maintaining social distancing and enhanced infection control strategies. Units should be created where COVID-19 patients are not cared for, so patients may receive routine vaccinations without risk of exposure. By designating specific appointment times, it is possible to ensure that only well patients are in the clinic during those times. Appointments also minimize the number of people present in the clinic at once.
Vaccine hesitancy/refusal has been one of the most important health problems in recent years, and during the COVID-19 period, the most radical groups have continued to share false and non-evidence-based opinions with the community.Citation30 Many of these theories posed during the pandemic have the risk of increasing future vaccine refusals. One of the most important observations during the period has been that the speed of transmission of false information about the disease is much faster and more dangerous than the speed of the spread of the virus.Citation71
Reduced access to critical health-care facilities and medications is known to establish circumstances in which patients use substandard drugs and/or dosages. This could lead to increased morbidity and mortality caused by human immunodeficiency virus infection, tuberculosis, and malaria, as well as leading to the rise and spread of drug-resistant diseases.Citation72 These populations need protection not only from the pandemic, but also from the consequences of non-pharmaceutical interventions. In addition to low- and middle-income countries, other vulnerable populations for the pandemic and mitigation strategies consequences are refugees and migrants. The pandemic has had an enormous effect on mobility, border and migration management, and on global migrant populations’ health, social, and economic situation. There now needs to be an immediate concerted effort to link these communities with national and global responses to COVID-19.Citation73 During the pandemic, immunization program for refugees and immigrants should not be neglected.
COVID-19 pandemic represents one of the most challenging and concerning public health crisis of this generation. While the efforts to control of COVID-19 have resulted in the temporary pause of preventive immunization campaigns, even in the absence of active outbreaks of vaccine-preventable disease, it should be kept in mind that delaying vaccination campaigns will likely result in an increased risk of resurgence of vaccine-preventable diseases that were controlled or eliminated. The WHO has also recommended that countries continue surveillance for vaccine-preventable diseases to determine where pathogens are circulating and which children are most at risk.Citation74 Routine pediatric immunizations of individual children at clinics must continue as much as possible during the pandemic. Parents are sometimes fearful about bringing their children to a clinic, but close relationships between the parents and the vaccinators and implementation of safeguards to reduce the risk of exposure and infection would resolve this problem.
The ongoing COVID-19 pandemic is a reminder of the importance of vaccination as a critical public health strategy for disease prevention and control. Public health officials have agreed that the most important global protection strategy, and the best method for controlling the SARS-CoV-2 pandemic, is a vaccine. An effective vaccine will require a minimum of 1–2 years to be developed, using the most optimistic forecast.Citation75–78 It is unknown how long the pandemic will last, or what the course of the virus spread will be after the first wave. While some of the strategies used to slow the spread of the virus in the community include using telemedicine, instead of face-to-face encounters, for routine medical visits, every effort should be made to continue routine immunizations for children and persons at risk for vaccine-preventable diseases. The potential for vaccine shortages related to closing borders and limited transport during the pandemic are also causes for concern. The disruption of routine health-care services and attendance to routine medical home visits due to social distancing and isolation conditions can continue. Although we know that there will be many demands on health systems and frontline health-care workers during and beyond the threat of COVID-19, continuing preventive health services, especially children’s vaccinations, are of great importance for the months and years to come. Whenever possible, providers are encouraged to prioritize newborn care and vaccination of infants and children when a healthcare practice can only provide limited well-child visits. Otherwise, we will inevitably see serious consequences related to suboptimal control of vaccine-preventable diseases in children concurrent with or following the SARS-CoV-2 pandemic.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
References
- Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, Wu Y, Zhang L, Yu Z, Fang M, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020 Feb 24. doi:10.1016/S2213-2600(20)30079-5.
- WHO Coronavirus Disease (COVID-19) Dashboard. [accessed 2020 Aug 6]. https://covid19.who.int.
- Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, Cereda D, Coluccello A, Foti G, Fumagalli R, et al. COVID-19 lombardy ICU network. baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020 Apr 6:e205394. doi:10.1001/jama.2020.5394.
- Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, Huang H, Zhang L, Zhou X, Du C, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with Coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020 Mar;13:e200994. doi:10.1001/jamainternmed.2020.0994.
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–62. doi:10.1016/S0140-6736(20)30566-3.
- Ferguson NM, Laydon D, Nedjati-Gilani G, Imai N, Ainslie K, Baguelin M, Bhatia S, Boonyasiri A, Cucunuba Perez Z, Cuomo-Dannenburg G, et al. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand. 2020 [accessed 2020 Jun 29]. https://spiral.imperial.ac.uk/bitstream/10044/1/77482/14/2020-03-16-COVID19-Report-9.pdf.
- Prem K, Liu Y, Russell TW, Kucharski AJ, Eggo RM, Davies N, Jit M, Klepac P,, . The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: a modelling study. Lancet Public Health. 2020 Mar 25. doi:10.1016/S2468-2667(20)30073-6.
- Nelson R. COVID-19 disrupts vaccine delivery. Lancet Infect Dis. Apr 17 2020. doi:10.1016/S1473-3099(20)30304-2.
- Weller C. While we wait for a COVID-19 vaccine, let’s not forget the importance of the vaccines we already have. [accessed 2020 Jun 29]. https://wellcome.ac.uk/news/while-we-wait-covid-19-vaccine-lets-not-forget-importance-vaccines-we-already-have.
- Liu W, Zhang Q, Chen J, Xiang R, Song H, Shu S, Chen L, Liang L, Zhou J, You L, et al. Detection of Covid-19 in children in early January 2020 in Wuhan, China. N Engl J Med. 2020 Apr 2;382(14):1370–71. doi:10.1056/NEJMc2003717.
- Porcheddu R, Serra C, Kelvin D, Kelvin N, Rubino S. Similarity in case fatality rates (CFR) of COVID-19/SARS-COV-2 in Italy and China. J Infect Dev Ctries. 2020 Feb 29;14(2):125–28. doi:10.3855/jidc.12600.
- Tagarro A, Epalza C, Santos M, Sanz-Santaeufemia FJ, Otheo E, Moraleda C, Screening CC. Severity of Coronavirus disease 2019 (COVID-19) in children in Madrid, Spain. JAMA Pediatr. Apr 8 2020. doi:10.1001/jamapediatrics.2020.1346.
- CDC COVID-19 Response Team. Coronavirus disease 2019 in children – United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep. 2020 Apr 10;69(14):422–26.doi:10.15585/mmwr.mm6914e4.
- Götzinger F, Santigo-Garcia B, Noguera-Julian A, Lanaspa P, Lancella L, Carducci FIC, Gabrowska N, Velizarova S, Prunk P, Osterman V, et al. COVID-19 children and adolescents in Europe: A multinational, multicenter cohort study. Lancet Child Adolesc Health. 2020 Jun 25. doi:10.1016/S2352-4642(20)30177-2.
- Capone CA, Subramony A, Sweberg T, Schneider J, Shah S, Rubin L, Schleien C, Epstein S, Johnson JC, Kessel A, Misra N. Characteristics, cardiac involvement, and outcomes of multisystem inflammatory disease of childhood (MIS-C) associated with SARS-CoV-2 infection. J Pediatr. 2020 Jun 14. doi:10.1016/j.jpeds.2020.06.044.
- Safadi MAP. The intriguing features of COVID-19 in children and its impact on the pandemic. J Pediatr (Rio J). Apr 14 2020. doi:10.1016/j.jped.2020.04.001.
- Viner RM, Russell SJ, Croker H, Packer J, Ward J, Stansfield C, Mytton O, Bonell C, Booy R. School closure and management practices during coronavirus outbreaks including COVID-19: a rapid systematic review. Lancet Child Adolesc Health. Apr 6 2020. doi:10.1016/S2352-4642(20)30095-X.
- House T, Baguelin M, van Hoek AJ, Flasche S, White P, Sadique MZ, Eames K, Read J, Hens N, Melegaro A, et al. Can reactive school closures help critical care provision during the current influenza pandemic? PLoS Curr. 2009 Oct 23;1:RRN1119. doi:10.1371/currents.RRN1119.
- Hens N, Ayele GM, Goeyvaerts N, Aerts M, Mossong J, Edmunds JW, Beutels P. Estimating the impact of school closure on social mixing behaviour and the transmission of close contact infections in eight European countries. BMC Infect Dis. 2009 Nov 27;9:187. doi:10.1186/1471-2334-9-187.
- [accessed 2020 Jun 29]. https://www.who.int/news-room/detail/22-05-2020-at-least-80-million-children-under-one-at-risk-of-diseases-such-as-diphtheria-measles-and-polio-as-covid-19-disrupts-routine-vaccination-efforts-warn-gavi-who-and-unicef.
- Roberts L. Global polio eradication falters in the final stretch. Science. 2020 Jan 3;367(6473):14–15. doi:10.1126/science.367.6473.14.
- Niger reports new polio outbreak. [accessed 2020 Jun 29]. https://www.who.int/immunization/diseases/measles/statement_missing_measles_vaccines_covid-19/en/.
- Hoffman J, Maclean R Slowing the Coronavirus is speeding the spread of other diseases. New York Times. 22 Jun 2020. https://www.nytimes.com/2020/06/14/health/coronavirus-vaccines-measles.html. [accessed 2020 Jun 29]
- [ accessed 2020 Jun 29]. https://www.afro.who.int/news/niger-reports-new-polio-outbreak.
- [accessed 2020 Jun 29]. http://polioeradication.org/polio-today/polio-now/this-week/.
- Roberts L. Why measles deaths are surging - and coronavirus could make it worse. Nature. 2020 Apr;580(7804):446–47. doi:10.1038/d41586-020-01011-6.
- Mortier C, Mailhe M, Amrane S, Lagier JC. Measles from Madagascar. Travel Med Infect Dis. 2019 May–Jun;29:58–59. doi:10.1016/j.tmaid.2019.04.003.
- Wadman M. Measles epidemic in Ukraine drove troubling European year. Science. 2019 Feb 15;363(6428):677–78. doi:10.1126/science.363.6428.677.
- Mahase E. Measles: democratic Republic of the Congo recorded over 6000 deaths last year. BMJ. 2020 Jan 8;368:m57. doi:10.1136/bmj.m57.
- Hotez PJ, Nuzhath T, Colwell B. Combating vaccine hesitancy and other 21st century social determinants in the global fight against measles. Curr Opin Virol. 2020 Feb 26;41:1–7. doi:10.1016/j.coviro.2020.01.001.
- [ accessed 2020 Jun 29]. https://en.unesco.org/covid19/educationresponse.
- Moss WJ. Measles. Lancet. 2017;390(10111):2490–502. doi:10.1016/S0140-6736(17)31463-0.
- Behrens L, Cherry JD, Heininger U, the Swiss Measles Immune Amnesia Study Group. The susceptibility to other infectious diseases following measles during a three year observation period in Switzerland. Pediatr Infect Dis J. 2020 Feb 14. doi:10.1097/INF.0000000000002599.
- Education: From disruption to recovery. [ accessed 2020 Jun 29]. http://polioeradication.org/polio-today/polio-now/this-week/.
- Abbas K, Procter SR, van Zandvoort K, Clark A, Funk S, Mengistu T, Hogan D, Dansereau E, Jit M, Flasche S. Benefit-risk analysis of health benefits of routine childhood immunisation against the excess risk of SARS-CoV-2 infections during the COVID-19 pandemic in Africa. medRxiv. 2020. doi:10.1101/2020.05.19.20106278.
- Santoli JM, Lindley MC, DeSilva MB, Kharbanda EO, Daley MF, Galloway L, Gee J, Glover M, Herring B, Kang Y, et al. Effects of the COVID-19 pandemic on routine pediatric vaccine ordering and administration - United States, 2020. MMWR Morb Mortal Wkly Rep. 2020 May 15;69(19):591–93. doi:10.15585/mmwr.mm6919e2.
- Bramer CA, Kimmins LM, Swanson R, Kuo J, Vranesich P, Jacques-Carroll LA, Shen AK. Decline in child vaccination coverage during the COVID-19 pandemic - michigan care improvement registry, May 2016-May 2020. MMWR Morb Mortal Wkly Rep. 2020 May 22;69(20):630–31. doi:10.15585/mmwr.mm6920e1.
- Fernandez M. Vaccinations are plummeting amid coronavirus pandemic. [accessed 2020 Jun 29]. https://www.axios.com/children-coronavirus-vaccinations-d2e86bd2-034e-4cc9-82b9-156fb9621f4f.html.
- [accessed 2020 Jun 29]. https://www.cleveland.com/news/2020/06/ohio-pediatric-vaccines-drop-by-45-during-coronavirus-pandemic-hospital-official-reports.html.
- [ accessed 2020 Jun 29]. https://www.virginiamercury.com/2020/04/27/virginia-pediatricians-report-troubling-decline-in-vaccination-rates-as-covid-19-pandemic-continues/.
- Saxena S, Skirrow H, Bedford H. Routine vaccination during covid-19 pandemic response. BMJ. 2020 Jun 16;369:m2392. doi:10.1136/bmj.m2392.
- [ accessed 2020 Jun 29]. https://jakartaglobe.id/news/immunization-should-continue-amid-pandemic-health-ministry/.
- Vaccine rates for all ages drop dramatically during COVID-19 – Medscape. [accesssed 2020 Jun 8]. https://www.medscape.com/viewarticle/931913#vp_2.
- Torres A, Blasi F, Dartois N, Akova M. Which individuals are at increased risk of pneumococcal disease and why? Impact of COPD, asthma, smoking, diabetes, and/or chronic heart disease on community-acquired pneumonia and invasive pneumococcal disease. Thorax. 2015;70(10):984–89. doi:10.1136/thoraxjnl-2015-206780.
- Martin-Loeches I, van Someren Gréve F, Schultz MJ. Bacterial pneumonia as an influenza complication. Curr Opin Infect Dis. 2017;30(2):201–07. doi:10.1097/QCO.0000000000000347.
- [ accessed 2020 Jun 29]. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters.
- Gostin LO, Salmon DA. The dual epidemics of COVID-19 and influenza: vaccine acceptance, coverage, and mandates. JAMA. Jun 11 2020. doi:10.1001/jama.2020.10802.
- Bayham J, Fenichel EP. Impact of school closures for COVID-19 on the US health-care workforce and net mortality: a modelling study. Lancet Public Health. 2020 Apr 3;pii: S2468-2667(20)30082–7. doi:10.1016/S2468-2667(20)30082-7.
- Wu D, Lu J, Ma X, Liu Q, Wang D, Gu Y, Li Y, He W. Coinfection of influenza virus and severe acute respiratory syndrome coronavirus 2 (SARS-COV-2). Pediatr Infect Dis J. Apr 13 2020. doi:10.1097/INF.0000000000002688.
- Ding Q, Lu P, Fan Y, Xia Y, Liu M. The clinical characteristics of pneumonia patients coinfected with 2019 novel coronavirus and influenza virus in Wuhan, China. J Med Virol. Mar 20 2020. doi:10.1002/jmv.25781.
- [accessed 2020 Jun 29]. https://www.who.int/influenza/surveillance_monitoring/updates/latest_update_GIP_surveillance/en/.
- Mendelson M. Could enhanced influenza and pneumococcal vaccination programs help limit the potential damage from SARS-CoV-2 to fragile health systems of southern hemisphere countries this winter? Int J Infect Dis. 2020 Mar 16;94:32–33. doi:10.1016/j.ijid.2020.03.030.
- Netea MG, Giamarellos-Bourboulis EJ, Domínguez-Andrés J, Curtis N, van Crevel R, van de Veerdonk FL, Bonten M. Trained immunity: a tool for reducing susceptibility to and the severity of SARS-CoV-2 infection. Cell. 2020 May 28;181(5):969–77. doi:10.1016/j.cell.2020.04.042.
- Chumakov K, Benn CS, Aaby P, Kottilil S, Gallo R. Can existing live vaccines prevent COVID-19? Science. 2020 Jun 12;368(6496):1187–88. doi:10.1126/science.abc4262.
- OPV as Potential Protection Against COVID. [ accessed 2020 Jun 29]. https://clinicaltrials.gov/ct2/show/NCT04445428?term=oral+polio&cond=covid+19&draw=2&rank=1.
- Miller A, Reandelar MJ, Fasciglione K, Roumenova V, Li Y, Otazu GH. Correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19: an epidemiological study. medRxiv. 2020. doi:10.1101/2020.03.24.20042937.
- Singh S. Bcg vaccines may not reduce Covid-19 mortality rates. medRxiv. 2020. doi:10.1101/2020.04.11.20062232.
- A database of global BCG vaccination policies and practices. 2020 [accessed 2020 Jun 29]. http://www.bcgatlas.org/.
- Moorlag SJCFM, Arts RJW, van Crevel R, Netea MG. Non-specific effects of BCG vaccine on viral infections. Clin Microbiol Infect. 2019 Dec;25(12):1473–78. doi:10.1016/j.cmi.2019.04.020.E.
- Garly M-L, Martins CL, Balé C, Baldé MA, Hedegaard KL, Gustafson P, Lisse IM, Whittle HC, Aaby P. BCG scar and positive tuberculin reaction associated with reduced child mortality in West Africa: a non-specific beneficial effect of BCG? Vaccine. 2003;21(21–22):2782–90. doi:10.1016/s0264-410x(03)00181-6.
- [ accessed 2020 Jun 29]. https://www.who.int/news-room/commentaries/detail/bacille-calmette-gu%C3%A9rin-(bcg)-vaccination-and-covid-19.
- [ accessed 2020 Jun 29]. https://www.cebm.net/covid-19/does-bcg-vaccination-protect-against-acute-respiratory-infections-and-covid-19-a-rapid-review-of-current-evidence/.
- BCG vaccine for health care workers as defense against COVID 19 (BADAS). [accessed 2020 Jun 29]. https://clinicaltrials.gov/ct2/show/NCT04348370?term=bcg+vaccine&cond=COVID&cntry=US&draw=2&rank=1.
- Application of BCG vaccine for immune-prophylaxis among egyptian healthcare workers during the pandemic of COVID-19. [accessed 2020 Jun 29]. https://clinicaltrials.gov/ct2/show/NCT04350931?term=bcg+vaccine&cond=COVID&draw=2&rank=2.
- Efficacy of BCG vaccination in the prevention of COVID19 Via the strengthening of innate immunity in health care workers (COVID-BCG). [accessed 2020 Jun 29]. https://clinicaltrials.gov/ct2/show/NCT04384549?term=bcg+vaccine&cond=COVID&cntry=FR&draw=2&rank=1.
- Vaccination Guidance During a Pandemic. [ accessed 2020 Jun 29]. https://www.cdc.gov/vaccines/pandemic-guidance/index.html.
- Interim guidance on continuity of immunization programs during the COVID-19 pandemic. [accessed 2020 Jun 29]. https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/interim-guidance-immunization-programs-during-covid-19-pandemic.html.
- Immunization in the context of COVID-19 pandemic. https://www.who.int/publications/i/item/immunization-in-the-context-of-covid-19-pandemic. [accessed 2020 Jun 29]
- Vaccinations of newborns in the context of the COVID-19 Pandemic. https://iris.paho.org/bitstream/handle/10665.2/52226/PAHOFPLIMCOVID-19200010_eng.pdf?sequence=1&isAllowed=y. [accessed 2020 Jun 29]
- https://services.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/masks-and-children-during-covid-19/. [ accessed 2020 Jun 29]
- Zarocostas J. How to fight an infodemic. Lancet. 2020;395(10225):676. doi:10.1016/S0140-6736(20)30461-X.
- Amimo F, Lambert B, Magit A. What does the COVID-19 pandemic mean for HIV, tuberculosis, and malaria control? Trop Med Health. 2020 May 13;48:32. doi:10.1186/s41182-020-00219-6.
- Kluge HHP, Jakab Z, Bartovic J, D’Anna V, Severoni S. Refugee and migrant health in the COVID-19 response. Lancet. 2020 Apr 18;395(10232):1237–39. doi:10.1016/S0140-6736(20)30791-1.
- Roberts L. Pandemic brings mass vaccinations to a halt. Science. 2020;368(6487):116–17. doi:10.1126/science.368.6487.116.
- Yamey G, Schäferhoff M, Hatchett R, Pate M, Zhao F, McDade KK. Ensuring global access to COVID-19 vaccines. Lancet. Mar 31 2020. doi:10.1016/S0140-6736(20)30763-7.
- Amanat F, Krammer F. SARS-CoV-2 vaccines: status report. Immunity. 2020 Apr 14;52(4):583–89. doi:10.1016/j.immuni.2020.03.007.
- Cohen J. Vaccine designers take first shots at COVID-19. Science. 2020 Apr 3;368(6486):14–16. doi:10.1126/science.368.6486.14.
- Thanh Le T, Andreadakis Z, Kumar A, Gómez Román R, Tollefsen S, Saville M, Mayhew S. The COVID-19 vaccine development landscape. Nat Rev Drug Discov. Apr 9 2020. doi:10.1038/d41573-020-00073-5.