
ABSTRACT
Prevalence of different HPV genotypes is changing after HPV vaccination. The associated risks are needed for optimizing cervical cancer screening.
To estimate HPV type-specific prevalence, odds ratio (OR), and positive predictive value (PPV) for cervical cytological abnormalities, we determined 41 different HPV genotypes in cervical samples from a population-based sample of 8351 women aged 18–51 years before HPV vaccination era (V501-033; NCT01077856).
Prevalence of HPV16 was 4.9% (95% CI: 4.4–5.5) with the PPV for high-grade cytology 11.2%, and OR 11.9 (95% CI: 8.5–16.5). Carcinogenic HPVs included in the nonavalent vaccine (HPV16,18,31,33,45,52,58) had a population prevalence of 14.4% (95% CI: 13.5–15.4), with PPV of 8.0% (95% CI: 6.8–9.3) and OR 23.7 (95% CI: 16.0–63.5) for high-grade cytology. HPV types currently included in most screening tests, but not vaccinated against (HPV35,39,51,56,59,66,68) had a joint prevalence of 8.5% (95% CI: 7.8–9.2) with PPV of 4.4% (95% CI: 3.3–5.7) and OR of 2.9 (95% CI: 2.0–4.0) for high-grade cytology. The other 27 non-carcinogenic genotypes had a prevalence of 11.8%, PPV of 2.9% (95% CI:2.1–3.9), and OR 1.5 (95% CI: 1.1–2.2.) for high-grade cytology.
These results suggest that HPV screening tests in the post-vaccination era might perform better if restricted to the HPV types in the nonavalent vaccine and screening for all 14 HPV types might result in suboptimal balance of harms and benefits.
Background
The high-risk types of human papillomavirus (HPV) cause several human cancers, particularly cervical cancer.Citation1 The established practice of cervical cancer prevention is transforming from using cytology-based screening with HPV-follow-up to HPV-based screening with cytology follow-up,Citation2-5 and prophylactic vaccines that are highly effective against the targeted HPV types and related cervical abnormalities.Citation6–8 Large metanalyses of case series have described the type-specific epidemiology of HPV.Citation9–11 Longitudinal, population-based, and multi-country studies may provide additional data on which HPV types are more prevalent and contribute the most to cervical disease in organized screening programs.
Over the course of years research has identified that HPV16 has the highest oncogenic potential of the over 200 HPV genotypes identified,Citation12-15 while HPV18,31,33,35,39,45,51,52,56,58,59 are also classified as carcinogenic to humans, HPV68 as probably carcinogenic, and HPV26,30,34,53,66,67,69,70,73,82,85,97 as possibly carcinogenic.Citation16 Consequently, almost all commercially available HPV DNA detection methods that are used in screening have been developed to target HPV16,18,31,33,35,39,45,51,52,56,58,59,66,68.Citation17 For use in screening programs with the aim to identify women who might be at elevated risk for cervical cancer. Coupled with appropriate clinical action(s), diagnostic verification and treatment, cervical cancer can be prevented. Prophylactic HPV vaccines, however, eliminate the risks related to the viral infection by targeting either HPV16,18 (2-valent [2 v] HPV vaccine), HPV6,11,16,18 (4 vHPV vaccine), or HPV6,11,16,18,31,33,45,52,58 (9 vHPV vaccine).Citation8 As the prevalence of vaccine types in populations with high vaccine coverage is reported to be very low when the vaccine is administered at an early age, methods and strategies developed for screening-based pre-vaccination HPV burden are likely to perform differently. For HPV-vaccinated populations, several mathematical models suggest less frequent screening with HPV testing rather than with cytology.Citation18,Citation19 Similar conclusions have been drawn from recent clinical studies reporting a decline in the predictive value of cytology for precancers in populations vaccinated at early ages.Citation2
Cervical cancer control programs in the 4 Nordic countries (Denmark, Iceland, Norway, and Sweden) are provided through organized healthcare programs that include both organized screening,Citation20 and mass-vaccination against HPV using either the 2 v or 4 vHPV vaccine.Citation21–24 The objective of this study (V501-033; NCT01077856) is to estimate the HPV type-specific prevalence by age and by cytological abnormality, as well as HPV type specific risks for cytological abnormalities in the general female population in Denmark, Iceland, Norway, and Sweden prior to large-scale use of HPV vaccines. Our study was conducted within the rigorous framework of the population-based cervical screening programs in the Nordic region, with all HPV testing performed in the WHO reference lab, and provides a critical reference of background data to design optimal organized screening strategies for HPV-vaccinated birth cohorts.
Methods
Overall design
To perform surveillance and ensure both quality of the program and high attendance among the target population, mandatory reporting of all cervical cancer screening-related activities and diagnoses has been introduced in Denmark, Iceland, Norway, and Sweden.Citation20,Citation25 A comprehensive surveillance infrastructure allows screening program providers to track the individual screening history of each female resident and intervene when deviations from the recommended screening guidelines are observed. Information is collected from all private and public healthcare providers, regardless of age and including all screening-related events performed within and outside the organized program.
During the period of 2006–2009, we collected the residual liquid-based cytology (LBC) samples from routine Pap smear screening to estimate HPV type-specific prevalence in the female population. Assuming variation in baseline HPV prevalence from 5% to 25% in the general population, we intended to enroll 1000 consecutive screening attendees aged 18–26 years and 1000 women aged 27–50 years from each country in order to estimate HPV type-specific prevalence and 95% confidence interval (CI) with 80% power at a 0.05% significance level.
The Research Ethics Committee/Data Protection Agency approved the study in each of the participating countries and decided the requirements for informed consent. In Denmark, the requirement for informed consent was waived. In Norway and Sweden, information about the study, a form for declining participation (opt-out), and a pre-paid return envelope was sent to the registered addresses of all women. In Iceland, potential participants received information about the study and an opt-out form when they attended the Cancer Detection Clinic.
Participants
A total of 16,550 consecutive residual specimens were obtained from women attending the 2006–2008 cervical cancer screening in 1) Copenhagen, Denmark, 2) Reykjavik, Iceland, 3) South- and North-Trondheim County in Norway, and 4) Stockholm and Malmö in Sweden. Altogether, 8926 participants with consecutive samples from age groups 18–26 and 27–50 years were included in this study (Denmark 2352, Iceland 2372, Norway 2019, Sweden 2183), while the rest of the samples were frozen. Concurrent cytology diagnoses by Bethesda classification for each participant were obtained from the population-based health registries operating in each country: 1) the Pathology Data Bank in Denmark, 2) the database of the Cancer Detection Clinic in Iceland, 3) the Cytology Registry in Norway, and 4) the Swedish National Cervical Screening Registry.Citation26 Cytology diagnoses were classified according to the 2001 Bethesda System .Citation27 Women with an unsatisfactory cytology (N = 461) were excluded from the statistical analyzes.
Laboratory analyses
PreservCyt solution (PreservCyt® Solution, Hologic, Inc., UK) medium was used in the majority of the subjects in all countries. LBC samples were stored at +4°C for a maximum of 3 months before they were received by the WHO HPV LabNet Global Reference Laboratory in Malmö, Sweden. DNA extraction and PCR strategy have previously been defined.Citation28 HPV genotyping was performed with a Luminex system (Biorad, CA, USA) with type-specific probes for 41 individual HPV types, including 2 variants of HPV35 and HPV58 with sequence variation in the probe target sequence (HPV 6,11,16,18,26,30,31,32,33,35,35 6624:A,39,40,42,43,44,45,51,52,53,54,55,56,58,58 668A,59,61,62, 66,67,68 subtype A, 68 subtype B,69,70,73,74,81,82,83,86,87,89,90 and 91) and two general probes broadly reactive with most HPV types. We excluded 98 participants with invalid or missing HPV results.
We categorized cytology diagnoses as “normal“, i.e., those negative for intraepithelial lesions or malignancy, and all remaining diagnoses were grouped as “abnormal.” Atypical squamous cells of undetermined significance and low-grade squamous intraepithelial lesions were grouped as “low-grade,” and atypical squamous cells that cannot exclude high-grade, atypical glandular cells of undetermined significance, high-grade squamous intraepithelial lesions, adenocarcinoma in situ, or cervical cancer were grouped as “high-grade cervical intraepithelial lesions.”
Statistical analysis
The study was designed to enroll an equal number of participants at ages 18–26 and 27–51 years in each country. As Norway, Denmark, Sweden, and Iceland have comparable risk factors for HPV infection,Citation29–32 and with minor differences between HPV positivity rates observed, we pooled countries in statistical analyses to facilitate our aim to estimate HPV type-specific prevalence by age at screening (age groups 18–23, 24–26, 27–29, 30–34, 35–39, and 40–51 years). The prevalence of HPV for types or combinations was estimated as the number of positive specimens for a given HPV type (or combinations of HPV types) divided by the total number of specimens with a valid PCR result (β-globin PCR positive by real-time PCR) for a given stratum. The prevalence estimates were weighted for unequal sampling fractions across countries, age groups, and cytology (normal vs. abnormal). We calculated the weights as the inverse of the sampling fractions from the country and age-group sampling strata, rescaled by post-stratification on additional cytology information (normal vs. abnormal) retrieved from the national screening registries (Supplementary Table 1). Prevalence estimates were weighted using the R complex survey software,Citation33,Citation34 and for the HPV prevalence CIs we used methods for proportions with a small expected number of positive counts.Citation35 Kernel smoothing was applied to prevalence curves.Citation36
Genotype-specific prevalence was estimated irrespective of potential coinfections. Hence, a specimen was counted as positive for a given HPV type whether it was positive only to that specific type, or also positive to additional HPV types. HPV genotype-specific prevalence for single infections, i.e., specimens positive only to one particular HPV genotype is also provided. For prevalence referring to groups of HPV-types, a specimen was defined as positive if it included at least one of the HPV-types of the given group. “Any HPV” refer to specimens positive to at least one of the tested HPV genotypes. “Carcinogenic HPV” refer to specimens positive to 16,18,31,33,35,39,45,51,52,56,58,59 and/or 68).Citation17 “Non-carcinogenic HPV” refer to specimens positive to 6,11,26,30,32,40,42,43,44,53,54,55,61,62, 66,67,69,70,73,74,81,83,86,87,89,90 and/or 91. “2 v”, “4 v” and “9 v” refer to specimens positive to 16 and/or 18; 6,11,16 and/or 18; and 6,11,16,18,31,33,45,52 and/or 58, respectively, based on HPV types targeted by prophylactic vaccines. To assess HPV prevalence in a hypothetical setting we assumed that vaccine-targeted HPV-types were eradicated, a highly likely situation.Citation22–24,Citation37 The combined carcinogenic HPV types then excluded carcinogenic HPVs targeted by 2 v or 4 v (i.e., specimens positive to 31,33,35,39,45,51,52,56,58,59 and/or 68); and 9 v vaccines (i.e., specimens positive to 35,39,51,56,59 and/or 68). HPV genotype-specific prevalence for single infections, i.e., specimens positive only to one particular HPV genotype is also provided.
Positive predictive value (PPV) was estimated as the number of specimens of a given cytology category positive to an HPV type (or combination of types) divided by the total number of specimens positive to the same HPV type (or combination of types), irrespective of cytology category. We estimated age-adjusted odds ratios for high-grade and low-grade cytology among women with HPV infection of the specified type compared with women negative to the specified type and having normal cytology. Each PPV and OR point-estimates were calculated regardless of co-infections and with 95% confidence intervals to assess the precision reflecting the number of events observed.
Results
HPV results and cytology diagnoses were available for 8367 women: 2319 in Denmark, 2310 in Iceland, 1972 in Norway, and 1766 in Sweden (). Altogether, there were 3528 women 18–26 years old (827, 861, 1031, and 809 from Denmark, Iceland, Norway, and Sweden, respectively). More than half (58%) of samples were from women older than age 26 (27–51 years). For 7524 (90%) subjects, the concurrent cytology was normal while 661 (8%) had low-grade and 182 (2%) had high-grade diagnoses.
Table 1. Distribution of participants by age at screening, country, and corresponding cytology abnormalities in Denmark, Iceland, Norway, and Sweden, in 2006–2008
In order to provide a comprehensive overview that would allow comparing all carcinogenic and non-carcinogenic HPV types, we performed comprehensive HPV genotyping. 40 different HPV types were detected, with the overall prevalence of 25.3% (95% CI: 24.1–26.5) (). The combined prevalence of 13 different carcinogenic HPV types was 18.1% (95% CI: 17.1–19.1) and 11.8% (95% CI: 11.0–12.7) for the 26 different non-carcinogenic HPV types. The combined prevalence of HPV types targeted by each of the 2 v, 4 v, and 9 v HPV vaccines was 6.6% (95% CI: 5.9–7.2), 7.8% (95% CI: 7.1–8.5), and 14.4% (95% CI: 13.5–15.4), respectively (). When we ignored HPV16,18 or HPV16,18,31,33,45,52,58, a hypothetical scenario after successful immunization with 2 v and 4 v or 9 v vaccine, the overall carcinogenic HPV prevalence of 18% was reduced to 14.2% (95% CI: 13.3–15.1) or 7.5% (95% CI: 6.8–8.2), respectively. The overall type-specific prevalence varied, with HPV16 being the most prevalent type at 4.9% (95% CI: 4.4–5.5). In contrast, thirteen non-carcinogenic types (HPV26,30,32,40,44,55,61,62,69,74,83,87,90) had a type-specific prevalence of 0.1% or less. HPV31 and HPV42 were the second most prevalent infections, with 2.9% for each (Supplementary Table 2).
Table 2. Weighted prevalencea of 40 HPV types measured, carcinogenic HPVb, non-carcinogenic HPVc, the 5 most common HPV types in declining order, vaccine-targeted carcinogenic HPV types in combinationd,e,f, and a hypothetical prevalence of remaining carcinogenic HPVs if vaccine-targeted HPVs would be eliminatedg,h, by age group
The combined prevalence of carcinogenic and non-carcinogenic HPVs was highest among the youngest age groups (). In the 18–23 age group, nearly half of the population, 46.2% (95% CI: 43.3–49.0) was positive for at least one carcinogenic HPV type and about a third, 30.0% (95% CI: 27.5–32.7) was positive for non-carcinogenic HPV types. A higher prevalence of carcinogenic HPV than non-carcinogenic HPV became gradually less apparent by increasing age until after 38 years of age, when carcinogenic and non-carcinogenic HPV types were equally common in women with normal cytology (). The 46% prevalence of carcinogenic HPVs in the 18–23 age group was reduced to 37.1% (95% CI: 34.4–39.9) when we assumed no positivity to HPV16,18 and to 23.2% (95% CI: 20.9–25.6) when we assumed no positivity to HPV16,18,31,33,45,52,58. Carcinogenic HPV prevalence of 36.6% in the 24–26 age group was similarly reduced to 28.5% (95% CI: 26.2–31.0) and 16.0% (95% CI:14.2–18.0), respectively.
Figure 1. The age-specific prevalence of carcinogenic HPV types and non-carcinogenic HPV types among those with normal cytology. Abbreviation: HPV = human papillomavirus
Overall, HPV16,31,42,52,56,51,18,39,45,70 (in declining order) were the ten most common HPV types (Supplementary Table 2). HPV16 and HPV42 were among the five most common HPV types in all age groups, with HPV16 being the most common in all age groups except those 40–51 years (). HPV31 was the second most common in age groups 18–23 and 24–26 years, at 9.3% and 6.6%, respectively. In age groups 18–23 and 24–26 years, 5.2% and 2.3% were positive to HPV6, respectively. Of carcinogenic HPV types, HPV35 and HPV58 always ranked lower than ten of the most common HPVs in all age groups.
In total, we detected 40, 36, and 23 different HPV types among those with normal, low-grade, and high-grade cytology (Supplementary Table 3). Prevalence of six carcinogenic HPVs (16,18,31,45,52,58) and HPV66 increased with the increasing severity of cytology, while HPV53 was equally prevalent in low- and high-grade cytology (Supplementary Table 3). Prevalence of carcinogenic HPV33,35,39,51,59,68 and non-carcinogenic HPV42,43,67,70,73,81,89 was highest in low-grade cytology; however, HPV53 and 56 were highest in high-grade cytology as a single infection.
In screening, excessive testing of women with typically self-resolving low-grade lesions would be regarded as harms while exams yielding in high proportion of women who need to be treated for cervical disease would be regarded as benefits. Hence, the high PPV for high-grade cytology and low PPV for low-grade cytology would likely provide a favorable balance between harms and benefits. We observed large variation by age when detecting high-grade cytology in those positive to carcinogenic HPVs, with PPVs ranging between 14.3% in the age-group of 35–39 years and 3% in the age-group of 18–23 years. However, only for 35–39 years old HPV16,18 positives had PPV point estimates for high-grade cytology higher than the PPV for low-grade cytology (). After ignoring positivity to the carcinogenic HPVs targeted by 2- or 4-valent HPV vaccine and 9-valent HPV vaccine, the age-specific PPVs for low-grade cytology ranged between 5.7% (95% CI: 0.7–19.2) and 23.5% (95%CI: 12.8–37.5) for both categories, i.e. those positive to HPV31,33,35,39,45,51,52,56,58,59,68 and those positive to HPV35,39,51,56,59,68. The PPVs for high-grade cytology were low for both groups, with only 4.3% (95% CI: 3.3 − 5.5) among those positive to the HPV31,33,35,39,45,51,52,56,58,59,68 and 2.3% (95% CI: 1.2 − 4.0) of those positive to HPV35,39,51,56,59,68. In contrast, for the non-carcinogenic HPVs the PPV for the concomitant low-grade and high-grade cytology was 19.1 (95% CI:17.2 − 21.2) and 2.9 (95% CI:2.1 − 3.9), respectively. We observed large differences in PPVs between carcinogenic HPV types: the PPV for low-grade cytology was 23.4% for HPV16 and 30.6% for HPV39 (the highest PPV for low-grade cytology) while the PPV for high-grade cytology was 11.2 for HPV16 and 3.7% for HPV39 (Supplementary Table 4).
Table 3. Positive predictive valuea for concomitant low-grade and high-grade cytology, combined as carcinogenic HPVb, 2 v and 4v HPV Vaccine vaccine-targeted carcinogenic HPV types in combination c, HPV types targeted by 9valent HPV vaccined, 27 non-carcinogenic HPV typesg and age
While PPV is a useful metric of the predictive value of the screening test and is commonly used in public health, odd ratio provides an insight to the etiological fraction of the infection which can be related to the lesion. We, therefore, present both metrics which complement each other with 95% confidence intervals to illustrate the precision of the point estimates which is determined by the number of events observed. Of 13 HPV genotypes significantly associated with high-grade cytology, 11 were classified as carcinogenic, with the highest OR for HPV16 (11.9 [95% CI: 8.5–16.5]) (). Among those positive to carcinogenic HPV53,35,39, the observed increased risk was at borderline significance only. Significantly elevated risk for low-grade cytology was observed for 23 genotypes, including all carcinogenic HPV genotypes, and the highest OR was observed for HPV39 (4.6 [95% CI: 3.4–6.1]) ().
Figure 2. Adjusted odds ratios with 95% CIs for high-grade (A) and low-grade (B) cytology diagnoses among women positive to specified HPV type with HPV infection of the specified type compared with women having normal cytology. Carcinogenic HPV types are marked in red. Abbreviations: CI = confidence interval; HPV = human papillomavirus; OR = odds ratio
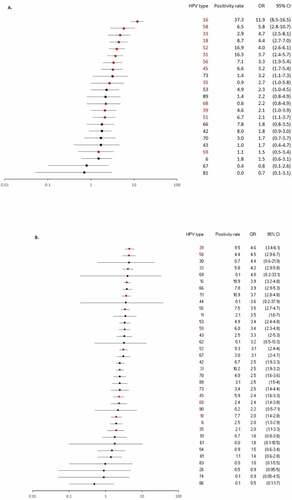
Compared to normal cytology, for those positive to at least one of the carcinogenic HPVs, we observed OR 28.2 (95% CI: 17.9–46.2) for high-grade cytology and 9.3 (95% CI: 7.6–11.3) for low-grade cytology. Similarly, for non-carcinogenic HPV, we observed OR 1.5 (95% CI: 1.1–2.2) for high-grade cytology and 3.3 (95% CI: 2.8–4.0) for low-grade cytology. For those positive to at least one of the carcinogenic HPVs included in the 9 v vaccine, we observed OR 23.7 (95% CI: 16.0–36.5) for high-grade cytology. In contrast, the overall weighted prevalence was 8.5% (95% CI: 7.80–9.2) for the types included in most HPV screening tests, but excluded from the vaccines (i.e., HPV35,39,51,56,59,66,68), with the PPV and OR for: 1) high-grade cytology of 4.4% (95% CI 3.3–5.7) and 2.9 (95% CI: 2.0–4.0), respectively; 2) low-grade cytology 22.6% (95% CI: 20.3–25.1) and 4.3 (95% CI: 3.6–5.1), respectively. For the five most common non-carcinogenic genotypes, HPV42,53,66,70,73, the OR for high-grade cytology was 1.9 (95% CI: 1.3–2.8) and for low-grade cytology the OR was 3.4 (95% CI: 2.8–4.1).
Discussion
In our population-based study, we observed high prevalence, but limited risk for cytological abnormalities of HPV types not targeted by HPV vaccines in women below 30 years of age. Regardless of age, we demonstrate almost always higher probability, i.e. PPV, for simultaneous low-grade cytology than for high-grade cytology among those positive to individual HPV types. This adds further to the evidence of the distinctive oncogenic potential of individual HPV types commonly referred to as carcinogenic and as well the age dependency of these HPV types, and the overall contribution of non-carcinogenic HPVs to the large share of total HPV prevalence. Our results imply that HPV technology detecting 14 different HPV types (16,18,31,33,35,39,45,51,52,56,58,59,68 and 66) might be suboptimal with regard to detection of high-grade lesions at low population prevalence of positivity. Our data suggest that screening strategies might perform better if restricted to the HPV types targeted by the nonavalent vaccine and when applied in an age-optimized manner. Several HPV screening tests that could be used for such strategies are already commercially available.
In agreement with others, we observed an overall higher prevalence of mucosal carcinogenic compared to non-carcinogenic HPV types, specifically in younger ages.Citation38,Citation39 With HPV16 as the most prevalent and with the highest risk for simultaneous high-grade cytology. Although the HPV prevalence decreased with increasing age which most likely reflects decreased exposure to HPV in these unvaccinated birth cohorts, after age of 35 years the prevalence of non-carcinogenic and carcinogenic HPVs was comparable. HPVs targeted by the 2 v and 4 v HPV vaccines contributed about a third of the overall 18% prevalence of carcinogenic HPV types, while HPV types targeted by the 9 v vaccine contributed about 80%. The same HPV types were also associated with increased risk for high-grade cytology: compared to normal cytology, the risk of high-grade cytology was 11.9 times higher for HPV16 but only non-significantly increased for HPV68 and HPV59. Also, PPV for high-grade lesions varied from 11.2% for HPV16 to 3% for HPV59. In screening, however, guidelines recommend detection of carcinogenic HPV as a group in (non-vaccinated) women 30 years and older.Citation40 We conventionally categorized 13 HPV types as carcinogenic.Citation4,Citation16 Of which oncogenic potential (i.e., risk for high-grade cytology) for individual HPVs varied. The group of 13 different carcinogenic HPVs had a 28- and 9 times higher OR for high-grade and low-grade cytology, respectively; those positive to HPV types included in most HPV screening tests, but excluded from the vaccines (HPV35,39,51,56,59,66,68) had only 2.9 times higher OR for high-grade lesions. The latter was comparable with the risks for high-grade and low-grade lesions we observed for the five most common non-carcinogenic types. Thus, the HPV types detected in screening considerably affect the harms and benefit balance of the entire program, an observation, which was supported by a recent study confirming clinical benefit of immediate colposcopy referral for all HPV16/18-positive women whereas women with other hrHPV infections are triaged with cytology in a pre-vaccinated population.Citation41One should notice that in Asian countries, for example, HPV58 has been reported to have a far more oncogenic profile compared with the Nordic countries,Citation42,Citation43 implying that regional/geographical differences should be considered in establishing an optimal screening program.
Now, the optimal screening scenario should be considered for the scenario when all 2 v and 4 v HPV vaccine-targeted HPV types are eliminated, with an assumed prevalence of carcinogenic HPVs reduced to 28% among those who enter the screening program. This simplified assumption does not include the effect of possible cross-protection that the HPV vaccination might confer against non-vaccine types.Citation44 Nor the possibility that exposure to HPVs and related cervical lesions might increase over time.Citation45 As expected, the potential effect of the 9 v vaccine would be higher, with a reduction in carcinogenic HPV prevalence to 16% at screening start, but with practical implications in the more distant future, because the 9 vHPV vaccine was licensed and became available in 2016. In contrast, the first birth cohorts of routinely vaccinated girls enter the cervical cancer screening program already in 2022 (Norway), 2020 (Denmark), and 2023 (Sweden) and we expect very low prevalence of HPV16 and HPV18, given documented high 14 years efficacy of the 4 v vaccine.Citation6 And the additional benefit from herd immunity.Citation46 In addition, the number of high-grade lesions to be screened and treated is expected to be reduced at least by 50% through vaccination,Citation44 implying that diagnostic yields of precancers requiring treatment among screen positives will likely be low. Yet, when we ignored any positivity to HPV types targeted by the 4 v vaccine, the prevalence of 11 carcinogenic types in the age at screening start, i.e. 24–26 was still 28.5%, which is likely too high to justify the switch from cytology screening to HPV screening, if the current technology based on the detection of 14 specific HPV types is used. Strategies using modern HPV tests focusing on the 9 HPV vaccine types are likely to perform better. Use of the 9 v vaccine would hypothetically reduce the combined prevalence of remaining carcinogenic HPV types (HPV35,39,51,56,59,68) to 7.5%. The clinical value, however, may be limited if the contemporary screening technology will be used to detect the remaining HPV39,51,59,68 types and precancers with lower potential for progression. Two recent studies based on mathematical models suggest implementing a longer screening interval and delayed screening start for HPV-vaccinated women.Citation18,Citation47 Immediate delay of screening age, however, would inevitably change the epidemiology of the asymptomatic precancer, which has an extremely high burden among women younger than 30 years.Citation20 Therefore, when the first vaccinated cohorts come to screening, public health providers need to consider screening tools and strategies based on updated empirical data and mathematical models.
Only one-quarter of all 40 HPV types propagate in the population and most likely maintain persistent infection. This feature is well described for carcinogenic HPV types.Citation48 Interestingly, the non-carcinogenic HPV42 and HPV70 types were among the most prevalent types overall, and specifically in women older than 35 years. We also document that positivity to the five most common non-carcinogenic HPVs had a significant 1.9 times elevated risk of having high-grade than normal cytology. Although the biological role of individual non-carcinogenic HPVs for progression of cervical cancer is negligible, it is possible that at least some non-carcinogenic HPVs have developed a distinctive adaptive mechanism to thrive and produce viral progenies.Citation49 Therefore, a post-vaccination surveillance to detect changes in the entire spectrum of HPV types affecting cervical mucosa can improve understanding of relationships between HPV types.
Our study should not be overinterpreted as we had no invasive cancer cases in the cohort, the study was cross-sectional, and disease assessment was based on concomitant cytology diagnosis and was not histologically confirmed. Histological grading is considered a golden standard for the clinical management of precancers, where self-limiting cervical intraepithelial neoplasia (CIN) grade 1 are discriminated from CIN 2/3 which require treatment. Sub-optimal inter-and intra-observer variability of the histological grading specifically for CIN2.Citation50-52 is perhaps even better described than uncertainty in reproducing cytological diagnosis.Citation53 And suggest substantial interpretive variability for disease assessment regardless of cytological or histological assessment of the disease. To our knowledge, it is the largest population-based HPV prevalence study performed in the Nordic region on a large set of mucosal HPV types, representing the typical distribution of cytological abnormalities in the screening population.Citation54 The rigorous study design included identical HPV detection methodology in all countries at a centralized, WHO-certified laboratory, weighted prevalence estimates, and simultaneous conduct of sample collection in all countries. These are important elements that allowed us to enhance representability of the data and comparability between the countries. Furthermore, cytology classification based on information from national registries was a useful benchmark in assessing the real-world impact needed for the translation of results into existing healthcare practices. Finally, the study design allows empirical observations of the emerging trends in HPV prevalence by repeating sample collection. Reduction in prevalence of HPV types in the screening population was observed five years later, reflecting the influx of HPV-vaccinated women in cohorts who enter screening.Citation55
The understanding that persistent infection with high-risk HPV is a necessary cause of cervical cancer has led to developments in new technologies and transformed cervical cancer prevention programs. As a result, the high-risk HPV test is gradually replacing cytology testing in nationwide screening programs and women with immunity against HPV16 and 18 are about to enter screening age. We detected a high prevalence of the HPV types included in common HPV testing kits but not targeted by the HPV vaccines. HPV screening tests which include all oncogenic HPV types in the post-vaccination era are likely to detect predominantly low-grade lesions. Risk profiles of high-grade and low-grade cytology in our study suggest that current screening of HPV-vaccinated cohorts might perform better if restricted to the HPV types in the nonavalent vaccine. Further research is needed for developing post-vaccination cervical cancer screening strategies with optimal balance of harms and benefits to inform public health practices and policy.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Supplemental Material
Download MS Word (64 KB)Acknowledgments
Editorial support was provided by Emily Cullinan, PhD, CMPP of The Lockwood Group. This assistance was funded by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. We would like to thank Jon E. Stek, MS, and Karyn Davis, BA, of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA for editorial assistance.
Disclosure statement
Mari Nygård has received research grants through her affiliating institute from MSD Norway. Bo T. Hansen and Suzanne Campbell report that their affiliating institute received grants from MSD Norway during the conduct of the study. Susanne K. Kjaer reports lecture fees from Sanofi Pasteur, MSD, and Merck & Co., Inc., Kenilworth, NJ, USA, and scientific advisory board fee and unrestricted research grants through her institution from Merck & Co., Inc., Kenilworth, NJ, USA. Maria Hortlund, Camilla Lagheden, and Joakim Dillner report that their affiliating institute received grants from Sanofi Pasteur, MSD, and Merck & Co., Inc., Kenilworth, NJ, USA. Christian Munk reports that he received lecture fees and support for conference participation from Sanofi Pasteur, MSD. Laufey Tryggvadóttir and Lara G. Sigurdardottir report that their affiliating institute received research grants from MSD Denmark ApS. Kai-Li Liaw is an employee of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Kenilworth, NJ, USA.
Supplementary materials
Supplemental data for this article can be accessed online at http://doi.org/10.1080/21645515.2020.1814097.
Additional information
Funding
References
- Zur Hausen H. Papillomaviruses and cancer: from basic studies to clinical application. Nat Rev Cancer. 2002;2(5):342–50. doi:10.1038/nrc798.
- Kinney WK, Perkins RB, Sawaya GF. Equal management of equal risks: what should be used as the standard for cervical cancer prevention? J Low Genit Tract Dis. 2018;22(3):237–41. doi:10.1097/LGT.0000000000000402.
- IARC Working group. IARC handbooks of cancer prevention: cervix cancer screening. Vol. 10. Lyon (France): IARC Press; 2005. Available at http://publications.iarc.fr/Book-And-Report-Series/Iarc-Handbooks-Of-Cancer-Prevention/Cervix-Cancer-Screening-2005
- European Commission. European guidelines for quality assurance in cervical cancer screening. In: editors, Anttila A, Arbyn M, De Vuyst H, Dillner J, Dillner L, Franceschi S, Patnick J, Ronco G, Segnan N, Suonio E, et al.Luxembourg: European Union; 2015. Available at https://publications.europa.eu/en/publication-detail/-/publication/a41a4c40-0626-4556-af5b-2619dd1d5ddc
- Melnikow J, Henderson JT, Burda BU, Senger CA, Durbin S, Weyrich MS. Screening for cervical cancer with high-risk human papillomavirus testing: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018;320(7):687–705. doi:10.1001/jama.2018.10400.
- Kjaer SK, Nygard M, Dillner J, Brooke Marshall J, Radley D, Li M, Munk C, Hansen BT, Sigurdardottir LG, Hortlund M, et al. A 12-year follow-up on the long-term effectiveness of the quadrivalent human papillomavirus vaccine in 4 Nordic countries. Clin Infect Dis. 2018;66(3):339–45. doi:10.1093/cid/cix797.
- Lehtinen M, Lagheden C, Luostarinen T, Eriksson T, Apter D, Harjula K, Kuortti M, Natunen K, Palmroth J, Petäjä T, et al. Ten-year follow-up of human papillomavirus vaccine efficacy against the most stringent cervical neoplasia end-point—registry-based follow-up of three cohorts from randomized trials. BMJ Open. 2017;7(8):e015867. doi:10.1136/bmjopen-2017-015867.
- Schiller JT, Castellsague X, Garland SM. A review of clinical trials of human papillomavirus prophylactic vaccines. Vaccine. 2012;30(Suppl 5):F123–138. doi:10.1016/j.vaccine.2012.04.108.
- Clifford GM, Gallus S, Herrero R, Muñoz N, Snijders PJ, Vaccarella S, Anh P, Ferreccio C, Hieu NT, Matos E, et al. Worldwide distribution of human papillomavirus types in cytologically normal women in the International agency for research on cancer HPV prevalence surveys: a pooled analysis. Lancet. 2005;366(9490):991–98. doi:10.1016/S0140-6736(05)67069-9.
- de Sanjose S, Diaz M, Castellsague X, Clifford G, Bruni L, Muñoz N, Bosch FX. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: a meta-analysis. Lancet Infect Dis. 2007;7(7):453–59. doi:10.1016/S1473-3099(07)70158-5.
- Bzhalava D, Guan P, Franceschi S, Dillner J, Clifford G. A systematic review of the prevalence of mucosal and cutaneous human papillomavirus types. Virology. 2013;445(1–2):224–31. doi:10.1016/j.virol.2013.07.015.
- Karolinska Institutet. International Human Papillomavirus (HPV) Reference Center. [Accessed September 16, 2018]. www.hpvcenter.se
- Schiffman M, Wentzensen N. Human papillomavirus infection and the multistage carcinogenesis of cervical cancer. Cancer Epidemiol Biomarkers Prev. 2013;22(4):553–60. doi:10.1158/1055-9965.EPI-12-1406.
- Kjaer SK, Frederiksen K, Munk C, Iftner T. Long-term absolute risk of cervical intraepithelial neoplasia grade 3 or worse following human papillomavirus infection: role of persistence. J Natl Cancer Inst. 2010;102(19):1478–88. doi:10.1093/jnci/djq356.
- Dillner J, Rebolj M, Birembaut P, Petry KU, Szarewski A, Munk C, de Sanjose S, Naucler P, Lloveras B, Kjaer S, et al. Long term predictive values of cytology and human papillomavirus testing in cervical cancer screening: joint European cohort study. BMJ. 2008;337:a1754. doi:10.1136/bmj.a1754.
- IARC Working Group. IARC Monographs - 100B: human Papillomaviruses. Lyon (France): WHO Press: International agency for research on cancer; 2012. http://monographs.iarc.fr/ENG/Monographs/vol100B/mono100B-11.pdf.
- Bouvard V, Baan R, Straif K, Grosse Y, Secretan B, El Ghissassi F, Benbrahim-Tallaa L, Guha N, Freeman C, Galichet L, et al. A review of human carcinogens–Part B: biological agents. Lancet Oncol. 2009;10(4):321–22. doi:10.1016/S1470-2045(09)70096-8.
- Pedersen K, Burger EA, Nygard M, Kristiansen IS, Kim JJ. Adapting cervical cancer screening for women vaccinated against human papillomavirus infections: the value of stratifying guidelines. Eur J Cancer. 2018;91:68–75. doi:10.1016/j.ejca.2017.12.018.
- Petry KU, Bollaerts K, Bonanni P, Stanley M, Drury R, Joura E, Kjaer SK, Meijer CJLM, Riethmuller D, Soubeyrand B, et al. Estimation of the individual residual risk of cervical cancer after vaccination with the nonavalent HPV vaccine. Hum Vaccin Immunother. 2018;14(7):1800–06. doi:10.1080/21645515.2018.1450125.
- Nygard M, Hansen BT, Dillner J, Munk C, Oddsson K, Tryggvadottir L, Hortlund M, Liaw K-L, Dasbach EJ, Kjær SK, et al. Targeting human papillomavirus to reduce the burden of cervical, vulvar and vaginal cancer and pre-invasive neoplasia: establishing the baseline for surveillance. PLoS One. 2014;9(2):e88323. doi:10.1371/journal.pone.0088323.
- Baandrup L, Blomberg M, Dehlendorff C, Sand C, Andersen KK, Kjaer SK. Significant decrease in the incidence of genital warts in young danish women after implementation of a national human papillomavirus vaccination program. Sex Transm Dis. 2013;40(2):130–35. doi:10.1097/OLQ.0b013e31827bd66b.
- Baldur-Felskov B, Dehlendorff C, Munk C, Kjaer SK. Early impact of human papillomavirus vaccination on cervical neoplasia–nationwide follow-up of young Danish women. J Natl Cancer Inst. 2014;106(3):djt460. doi:10.1093/jnci/djt460.
- Leval A, Herweijer E, Ploner A, Eloranta S, Fridman Simard J, Dillner J, Young C, Netterlid E, Sparén P, Arnheim-Dahlström L, et al. Quadrivalent human papillomavirus vaccine effectiveness: a Swedish national cohort study. J Natl Cancer Inst. 2013;105(7):469–74. doi:10.1093/jnci/djt032.
- Feiring B, Laake I, Bakken IJ, Greve-Isdahl M, Wyller VB, Håberg SE, Magnus P, Trogstad L. HPV vaccination and risk of chronic fatigue syndrome/myalgic encephalomyelitis: A nationwide register-based study from Norway. Vaccine. 2017;35(33):4203–12. doi:10.1016/j.vaccine.2017.06.031.
- Vaccarella S, Franceschi S, Engholm G, Lonnberg S, Khan S, Bray F. 50 years of screening in the Nordic countries: quantifying the effects on cervical cancer incidence. Br J Cancer. 2014;111(5):965–69. doi:10.1038/bjc.2014.362.
- Elfstrom KM, Sparen P, Olausson P, Almstedt P, Strander B, Dillner J. Registry-based assessment of the status of cervical screening in Sweden. Journal of Medical Screening. 2016;23(4):217–26. doi:10.1177/0969141316632023.
- Solomon D, Nayar R. The Bethesda System for reporting cervical cytology. Second. New-York, USA: Springer-Verlag New-York, Inc.; 2004.
- Soderlund-Strand A, Eklund C, Kemetli L, Grillner L, Törnberg S, Dillner J, Dillner L. Genotyping of human papillomavirus in triaging of low-grade cervical cytology. Am J Obstet Gynecol. 2011;205(2):145e1–16. doi:10.1016/j.ajog.2011.03.056.
- Eliasen M, Kaer SK, Munk C, Nygård M, Sparén P, Tryggvadottir L, Liaw K-L, Grønbæk M. The relationship between age at drinking onset and subsequent binge drinking among women. Eur J Public Health. 2009;19(4):378–2. doi:10.1093/eurpub/ckp023.
- Hansen BT, Kjaer SK, Munk C, Tryggvadottir L, Sparén P, Hagerup-Jenssen M, Liaw K-L, Nygård M. Early smoking initiation, sexual behavior and reproductive health - a large population-based study of Nordic women. Prev Med. 2010;51(1):68–72. doi:10.1016/j.ypmed.2010.03.014.
- Jensen KE, Munk C, Sparen P, Tryggvadottir L, Liaw KL, Dasbach E, NYGÅRD M, KJAER SK. Women’s sexual behavior. Population-based study among 65,000 women from four Nordic countries before introduction of human papillomavirus vaccination. Acta Obstet Gynecol Scand. 2011;90(5):459–67. doi:10.1111/j.1600-0412.2010.01066.x.
- Olesen TB, Jensen KE, Nygard M, Tryggvadottir L, Sparén P, Hansen BT, Liaw K-L, Kjaer SK. Young age at first intercourse and risk-taking behaviours–a study of nearly 65 000 women in four Nordic countries. Eur J Public Health. 2012;22(2):220–24. doi:10.1093/eurpub/ckr055.
- R Core Team. R: A language and environment for statistical computing. Vienna (Austria): R Foundation for Statistical Computing; 2012.
- Lumley T. Complex surveys: a guide to analysis using R. Hoboken (NJ): Wiley & Sons; 2010. Available at https://onlinelibrary.wiley.com/doi/book/10.1002/9780470580066
- Korn EL, Graubard BI. Confidence intervals for proportions with small expected number of positive counts estimated from survey data. Surv Methodol. 1998;24:193–201.
- Lewandowski GS, Vaccarello L, Copeland LJ. Surgical issues in the management of carcinoma of the cervix in pregnancy. Surg Clin North Am. 1995;75(1):89–100. doi:10.1016/S0039-6109(16)46536-9.
- Orumaa M, Kjaer SK, Dehlendorff C, Munk C, Olsen AO, Hansen BT, Campbell S, Nygård M. The impact of HPV multi-cohort vaccination: real-world evidence of faster control of HPV-related morbidity. Vaccine. 2020;38(6):1345–51. doi:10.1016/j.vaccine.2019.12.016.
- Bonde J, Rebolj M, Ejegod DM, Preisler S, Lynge E, Rygaard C. HPV prevalence and genotype distribution in a population-based split-sample study of well-screened women using CLART HPV2 human papillomavirus genotype microarray system. BMC Infect Dis. 2014;14(1):413. doi:10.1186/1471-2334-14-413.
- Bruni L, Diaz M, Castellsague X, Ferrer E, Bosch FX, de Sanjose S. Cervical human papillomavirus prevalence in 5 continents: meta-analysis of 1 million women with normal cytological findings. J Infect Dis. 2010;202(12):1789–99. doi:10.1086/657321.
- von Karsa L, Arbyn M, De Vuyst H, Dillner J, Dillner L, Franceschi S, Patnick J, Ronco G, Segnan N, Suonio E, et al. European guidelines for quality assurance in cervical cancer screening. Summary of the supplements on HPV screening and vaccination. Papillomavirus Res. 2015;1:22–31. doi:10.1016/j.pvr.2015.06.006.
- Hashim D, Engesaeter B, Baadstrand Skare G, Castle PE, Bjørge T, Tropé A, Nygård M. Real-world data on cervical cancer risk stratification by cytology and HPV genotype to inform the management of HPV-positive women in routine cervical screening. Br J Cancer. 2020;122(11):1715–23. doi:10.1038/s41416-020-0790-1.
- Lee EH, Um TH, Chi HS, Hong YJ, Cha YJ. Prevalence and distribution of human papillomavirus infection in Korean women as determined by restriction fragment mass polymorphism assay. J Korean Med Sci. 2012;27(9):1091–97. doi:10.3346/jkms.2012.27.9.1091.
- Chan PK, Ho WC, Yu MY, Pong WM, Chan AC, Chan AK, Cheung T-H, Wong MCS, To K-F, Ng H-K, et al. Distribution of human papillomavirus types in cervical cancers in Hong Kong: current situation and changes over the last decades. Int J Cancer. 2009;125(7):1671–77. doi:10.1002/ijc.24495.
- Malagon T, Drolet M, Boily MC, Franco EL, Jit M, Brisson J, Brisson M. Cross-protective efficacy of two human papillomavirus vaccines: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(10):781–89. doi:10.1016/S1473-3099(12)70187-1.
- Hansen BT, Kjaer SK, Arnheim-Dahlstrom L, Liaw KL, Juul KE, Thomsen LT, Frederiksen K, Elfström KM, Munk C, Nygård M, et al. Age at first intercourse, number of partners and sexually transmitted infection prevalence among Danish, Norwegian and Swedish women: estimates and trends from nationally representative cross-sectional surveys of more than 100 000 women. Acta Obstet Gynecol Scand. 2020;99(2):175–85. doi:10.1111/aogs.13732.
- Chow EP, Danielewski JA, Fehler G, Tabrizi SN, Law MG, Bradshaw CS, Garland SM, Chen MY, Fairley CK. Human papillomavirus in young women with chlamydia trachomatis infection 7 years after the Australian human papillomavirus vaccination programme: a cross-sectional study. Lancet Infect Dis. 2015;15(11):1314–23. doi:10.1016/S1473-3099(15)00055-9.
- Landy R, Windridge P, Gillman MS, Sasieni PD. What cervical screening is appropriate for women who have been vaccinated against high risk HPV? A simulation study. Int J Cancer. 2017;142(4):709–18. doi:10.1002/ijc.31094.
- Doorbar J. Molecular biology of human papillomavirus infection and cervical cancer. Clin Sci (Lond). 2006;110(5):525–41. doi:10.1042/CS20050369.
- Egawa N, Egawa K, Griffin H, Doorbar J. Human papillomaviruses; epithelial tropisms, and the development of neoplasia. Viruses. 2015;7(7):3863–90. doi:10.3390/v7072802.
- Carreon JD, Sherman ME, Guillen D, Solomon D, Herrero R, Jerónimo J, Wacholder S, Rodríguez AC, Morales J, Hutchinson M, et al. CIN2 is a much less reproducible and less valid diagnosis than CIN3: results from a histological review of population-based cervical samples. Int J Gynecol Pathol. 2007;26(4):441–46. doi:10.1097/pgp.0b013e31805152ab.
- Ismail SM, Colclough AB, Dinnen JS, Eakins D, Evans DM, Gradwell E, O’Sullivan JP, Summerell JM, Newcombe RG. Observer variation in histopathological diagnosis and grading of cervical intraepithelial neoplasia. BMJ. 1989;298(6675):707–10. doi:10.1136/bmj.298.6675.707.
- Robertson AJ, Anderson JM, Beck JS, Burnett RA, Howatson SR, Lee FD, Lessells AM, McLaren KM, Moss SM, Simpson JG, et al. Observer variability in histopathological reporting of cervical biopsy specimens. J Clin Pathol. 1989;42(3):231–38. doi:10.1136/jcp.42.3.231.
- Stoler MH, Schiffman M. Interobserver reproducibility of cervical cytologic and histologic interpretations: realistic estimates from the ASCUS-LSIL Triage Study. Jama. 2001;285(11):1500–05. doi:10.1001/jama.285.11.1500.
- Skare G, Lönnberg S, Bjorge T, Trope A. Masseundersøkelsen mot livmorhalskreft. Årsrapport 2015: Kreftregisteret. Institutt for populasjonsbasert kreftforskning. Oslo, Norway: Kreftregisteret; 2016.
- Dillner J, Nygard M, Munk C, Hortlund M, Hansen BT, Lagheden C, Liaw K-L, Kjaer SK. Decline of HPV infections in Scandinavian cervical screening populations after introduction of HPV vaccination programs. Vaccine. 2018;36(26):3820–29. doi:10.1016/j.vaccine.2018.05.019.