
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Background
The school entry vaccination record check strategy (SECS) is an appropriate opportunity to recommend vaccines for students to improve vaccination coverage (VC). However, it is only utilized for providing necessary catch-up vaccination for students who are missing the Expanded Program on Immunization (EPI) vaccines in China. We aimed to address that gap and quantify the relationship between the SECS policy and the increase of coverage in varicella vaccine (VarV).
Methods
We employed a pretest and posttest quasi-experimental design to examine the effect of the upgraded SECS policy on the change of VarV coverage in newly enrolled students in Lu’an, 2019–2020.
Results
Eight hundred participants were randomly divided into the control group (C group, 31.8%), the telephone-based intervention group (T group, 31.2%), and the written notification intervention group (W group, 37.0%). Totally, 84 students received VarV during the study period, with a VC of 10.5%. The possibility of vaccination in the T group (RR = 4.9, 95% CI:2.2–10.9) and W group (RR = 5.2, 95% CI:2.4–11.5) was significantly higher than that in the C group (p< .001).
Conclusions
Our study demonstrates that the upgraded SECS produce a positive effect on improving the VC of VarV. This nudge strategy may decrease varicella outbreaks in schools in China, especially in provinces where VarV is not introduced into EPI.
Introduction
The varicella vaccine (VarV) has not been introduced into the Expanded Program on Immunization (EPI) in China, implying that it is voluntary and must be self-paid (approximate 26 USD). Therefore, although VarV has turned out to be safe and effective,Citation1 its coverage has been lower compared with EPI vaccines in China.Citation2,Citation3As a result, the vaccination coverage (VC) of VarV was suboptimal at the national level and varied by province, ranging from 21% to 98%.Citation4-6 And even at the prefecture level such as Lu’an, the VC of VarV varied by different years and counties, ranging from 48% to 86%.Citation3,Citation7 The disparity of VC might be caused by differing levels of economic development.Citation2 For example, developed provinces such as Shanghai have included the VarV in local EPI.Citation8 The long-term moderate level of VC can result in the accumulation of a critical mass of susceptible children in collective settings that increases the risk of outbreak. Previous studies have found that most outbreaks occurred in school settings.Citation7,Citation9,Citation10 Besides, the national surveillance data revealed that the proportion of school-related varicella outbreaks was the highest (38.5%) among all communicable disease public health emergencies,Citation11 suggesting that it is essential to conduct targeted intervention to prevent outbreak in school settings.
The policy interventions such as immunization requirements for school entry and checking of student vaccination records at school can optimize VC among school-aged children.Citation12,Citation13 However, the evidence of the effectiveness of checking vaccination status at school is predominantly from the recommendation of routine vaccines.Citation13-15 With the growing number of new vaccines and occurrence of outbreak, policymakers have attempted to consider changing school entry requirements to increase the VC of target vaccines such as the human papillomavirus vaccine.Citation16-18 Experience from countries that have adopted school entry requirements policy suggests that the school enrollment rate influence the feasibility and effectiveness of checking vaccination status at school.Citation13 Fortunately, the primary school enrollment rate was high due to universal and compulsory education in China.Citation19 Besides, the school entry vaccination record check strategy (SECS) has been required by law since 2005.Citation15 Therefore, SECS is an appropriate opportunity to recommend vaccines for school-aged children to improve coverage in China.
However, SECS is only utilized for providing necessary catch-up vaccination for students who are missing EPI vaccines in China.Citation15,Citation19 The overall effectiveness of recommendation for non-EPI vaccines based on SECS has not been fully evaluated. According to the experience of the SECS intervention of EPI vaccines, we hypothesis that SECS might produce a positive effect on improving the VC of non-EPI vaccines. Considering the continuous varicella outbreaks and the challenge of high varicella incidence has been formed in Lu’an,Citation3,Citation7 we attempt to upgrade the SECS by including non-EPI vaccines such as VarV into the checklist to increase VC levels to control varicella.
Materials and methods
Study area
Lu’an is a typical undeveloped and agricultural city located in the central region of China, with an area of 15.5 thousand square kilometers and about 5.88 million residents. According to the survey data from 2017–2019 (unpublished), there are about 98 thousand newly enrolled students in Lu’an each school year, including 50 thousand kindergarten students and 48 thousand primary school students.
Study design
We employed a pretest and posttest quasi-experimental design to examine the effect of the intervention on the change of the VC of VarV in newly enrolled students of 2019–2020 school year in Lu’an. This study was conducted from September 2019 to June 2020. The VC of VarV refers that children should be vaccinated at least one dose of VarV. Our design was based on upgrading the SECS to execute intervention measures, but we did not know the distribution of students who have not received VarV in each school. Thus, total randomization was impractical for this study. However, the quasi-experimental design is common in studies aiming to establish the effectiveness of health-related interventions and is also considered to be of relatively high-quality study design.Citation20 We controlled possible confounding factors by stratification and randomization in some procedures of the study (). Besides, we also extended the follow-up period (ten months) to fully collect control data and allow all participants to receive the intervention.
Figure 1. Selection procedure of schools for the quasi-experiment study in Lu’an, 2019–2020
Figure 2. Selection procedure of the enrollment of participants for the quasi-experiment study in Lu’an, 2019–2020
Interventions
In 2005, the Ministry of Health and the Ministry of Education in China jointly issued a school entry vaccination check requirement congruent with the law.Citation15 It required kindergartens and schools to check the vaccination status of newly enrolled students to ensure they have received all age-appropriate EPI vaccines, which was also named SECS.Citation15 However, it is only utilized for providing necessary catch-up vaccination for students who are missing EPI vaccines. The non-EPI vaccines, such as VarV and influenza vaccine, were not included in the checklist of SECS. In this study, we regarded SECS as an opportunity for intervention, and we upgraded this strategy by including non-EPI vaccines such as VarV into the checklist. We adopted two intervention measures, including the telephone-based intervention and the written notification intervention, which were also common measures in routine SECS work. The unvaccinated students who received doctor’s recommendations based on telephone notification formed the telephone-based intervention group (T group). The unvaccinated students who received written notification recommendations formed the written notification intervention group (W group). The written notification was delivered by students retuning a document to their caretakers or parents. The unvaccinated students without any recommendation formed the control group (C group). The intervention was carried out by the local vaccination clinic doctors who have been trained by Lu’an Center for Disease Control and Prevention (CDC).
Outcomes
The primary study outcome was to estimate the effect of the intervention on the change of VC of VarV in newly enrolled students in Lu’an. The secondary outcome was to examine which intervention is more effective between the T group and W group. We also compared the VC of VarV between the baseline survey and the final evaluation of the intervention activities. Furthermore, we investigated the distribution of the timing of receiving VarV among different groups.
Sample
The sample size was determined to provide 90% power at two-sided α = 0.05 to detect the difference between the control and intervention groups. We calculated the sample size by using the formula referred to the randomized controlled trial study:Citation21 , where a and b referred to the conventional multiplier for alpha (α = 0.05) and the conventional multiplier for power (β = 90%), respectively; p1 and p2 represented the expected VC in the intervention group and control group, respectively; q1 and q2 was the proportion of students without vaccination in the intervention group (1- p1) and control group (1-p2). We assumed that it is a small probability event for a child to receive VarV after three years of age without re-recommendation. Thus, we considered that the expected VC in the control group was 5% (p2 = 5%). We anticipated that the VC would be at least increased by 10% between the before and after the intervention period. Thus, we considered that the expected VC in the intervention group was 15% (p1 = 15%). Finally, we calculated that 184 participants were required in each intervention group and the control group to answer the primary research question. Considering 10–15% of students might be lost to follow-up or with unclear vaccination history, we eventually intend to enroll 210 unvaccinated students in each group.
Study procedure
We divided the study into four stages according to the protocol. At the first stage, we aimed to select schools for our research. The stratified sampling methodology for sampling the schools was adopted (). Step one: we selected at least one rural township and one urban township from each county in Lu’an. Step two: we selected three kindergartens and three primary schools from each township by using convenience sampling. Step three: three kindergartens chosen from the same township were randomly divided into the C group, the T group, and the W group; the same grouping method was used in primary schools. Finally, a total of 102 schools were selected. After we divided them into three groups equally, each group included 17 kindergartens and 17 primary schools. At the second stage, we conducted a baseline investigation to enroll the participants. Based on our previous studies,Citation3,Citation7 we considered that the VC of VarV ranged from 48% to 86%. Therefore, we need to investigate at least 4500 students to meet the sample size for enrolling participants. Finally, 5024 students were investigated, and 800 unvaccinated students were enrolled in the study (). To examine the effect of the intervention on the change of VarV coverage in newly enrolled students, we adopted predetermined intervention measures among students in the T group and W group at the third stage of the study. At the fourth stage, we followed up with the participants in the 1st month, the 3rd month, the 6th month, and the 10th month after the intervention through the Anhui Immunization Information Management System (AIIMS) to observe the VC. The AIIMS is an internet-based management platform maintaining immunization data for children living in Anhui province, which was described in detail in our previous study.Citation3
Ethical considerations
Our protocol was approved by the Academic Council of Lu’an CDC and is in accordance with the Helsinki Declaration of 1975. We obtained written informed consents from caretakers or parents before their children were vaccinated.
Data collection and statistical analysis
We designed a structured questionnaire that was sent to the vaccination clinic, where the study was conducted. Data collected in the questionnaire included demographic characteristics, VarV vaccination status, grouping situation, school type and location, and time of intervention, etc. The follow-up was done by EPI staff from Lu’an CDC, and the results of the follow-up were filled in the questionnaire. All collected data were entered into Epidata 3.1 software. Data cleaning and descriptive epidemiology analysis were performed by using Microsoft Excel 2016. Possible differences between different groups were tested by the chi-square test and Kruskal-Wallis test where appropriate. All the statistical analyses were performed using Epi Info™ software (version 7.2). Two-sided p values were reported to be statistically significant at < 0.05.
Results
VC of VarV at baseline
The characteristics and the VC among different groups are summarized in . A total of 5024 students were investigated, of which 4224 (84.1%) have been vaccinated with at least one dose of VarV. The overall VC in C group schools, T group schools, and W group schools was 84.9% (1429/1683), 84.9% (1402/1652), and 82.5% (1393/1689), respectively; and no significant difference was observed among the three groups (χ2 = 4.876, p = .087). However, subgroup analyses showed that the overall VC in primary school and rural school was significantly higher than that of kindergarten and urban school (p< .001).
Table 1. Vaccination coverage of varicella vaccine during the baseline survey among different intervention schools in Lu’an, 2019
Differences between the three groups at baseline
A total of 800 unvaccinated students were enrolled. They were randomly divided into the C group (31.8%), the T group (31.2%), and the W group (37.0%). To examine the comparability between the intervention group and control group, we compared the three groups on five possibly confounding variables through univariate analyses. We found that baseline characteristics were similar among three groups (p> .05) except the age between W group and T group (z= −2.259, p= .024). Characteristics of the three groups at baseline are presented in .
Table 2. Description and comparison between the control group and the intervention groups
Primary outcome
Eighty-four students received VarV during the study period, with a VC of 10.5%. The risk difference (RD) and relative risk (RR) by different subgroups are shown in . We found that seven (2.8%) participants received VarV in the C group and 34 (13.6%) of those in the T group (RR = 4.9, 95%CI: 2.2–10.9). Compared with the C group, 43 (14.5%) participants received VarV in the W group (RR = 5.2, 95%CI: 2.4–11.5). The intervention measure that was taken in the T group and W group for most subgroup students was effective compared with the C group, with RDs ranged from 8.3 to 23.2 and RRs ranged from 3.0 to 26.6. However, we found that the intervention measure for students from the urban area in the T group seems ineffective, where the RD was 0.3 (95%CI: −4.5–5.1) and the RR was 1.1 (95%CI: 0.4–3.3).
Table 3. Summary of varicella vaccine immunization status of 800 unvaccinated students at endpoint of the study
Secondary outcome
We compared the proportion of vaccinated students between the T and W groups at the endpoint to examine which intervention is more effective. We found that although the overall proportion of vaccinated students in the W group was slightly higher than the T group (14.5% vs. 13.6%), the difference was not statistically significant (χ2 = 0.096, p = .757). However, the intervention effect on the urban subgroup in the W group was superior to the T group (12.4% vs. 4.5%; RD = 7.9, 95%CI: 1.9–14.0; RR = 2.8, 95%CI:1.2–6.9).
The distribution of vaccination time among different groups
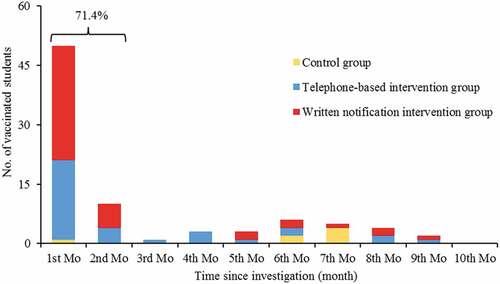
As shown in , 71.4% (60/84) of participants responded to the intervention in the first two months, and they received one dose of VarV. We noted that the proportion of vaccinated students in the first month was significantly higher than that in other periods, suggesting that the intervention effect appears to be short-term.
Figure 3. Distribution of the timing of varicella vaccine administration among 84 students during the follow-up period
Other findings
We summarized the VC of VarV among different observation group schools at the final evaluation of the intervention activities (). We found that the VC in the C group school, T group school, and W group school increased at the endpoint compared to baseline during the study period. The overall increased VC among all students was 1.7%, and the increased VC in the C group school, T group school, and W group school was 0.4%, 2.1%, and 2.5%, respectively. Interestingly, when we attempted to collect the information of the second dose of VarV among students who had received the first dose of VarV (student without intervention), we found that 39 students have received the second dose with a proportion of 1.0% (). We also observed that the proportion of receiving the second dose of VarV in W group schools was significantly higher than T group schools and C group schools (p< .001), indicating that the intervention based on written notification may have an indirect positive effect.
Table 4. Vaccination coverage of varicella vaccine during the baseline survey and the final evaluation of the intervention activities
Table 5. Summary of the second dose of varicella vaccination status for students who have administrated one dose of varicella vaccine
Discussion
In this quasi-experiment study, we demonstrated that the recommendation of VarV for unvaccinated students based on telephone or written notification intervention significantly increased the possibility of vaccination compared with the control group. However, the intervention measure in W group was more effective than that of the T group among urban students, whereas the T group intervention measure seems ineffective. We found that most students who responded to the recommendation would be vaccinated within one month. Furthermore, we observed that the intervention based on written notification might have an indirect positive effect.
Although varicella is benign in children,Citation22 we could not neglect the primary disease burden of a high number of cases and the indirect burden due to the need for parents to look after the affected children who will not be able to attend school.Citation23,Citation24 Fortunately, we observed that the VC in Lu’an has dramatically improved compared with the surveillance data in 2018, especially in primary school students (89.9% vs. 78.6%).Citation3 The findings can be explained by the fact that even in the voluntary era, parents are concern about the high varicella prevalence in schools and therefore take the initiative to administer the VarV for their children. We also found that the VC among kindergarten children was much lower than that of primary school, implying proactive intervention will have a better effect on the promotion of VarV coverage among kindergarten children. The previous literature also mentioned that the effects appear to be larger when the pre-intervention vaccination coverage was low.Citation25 However, respecting the autonomous decision-making of individual citizens and the physician’s support might also affect the effectiveness of the intervention.Citation17,Citation26 Therefore, we need further to assess physician support of recommending non-EPI vaccines for school entry and the parental willingness to vaccinate for their children.
Using the upgraded SECS that was based on recommending VarV for school-aged children, we showed that the overall VC among unvaccinated students from the T group and W group increased by 13.6% and 14.5%, respectively. Compared with the control group, both the telephone-based intervention measure (RR = 4.9, 95%CI: 2.2–10.9) and the written notification intervention measure (RR = 5.2, 95%CI: 2.4–11.5) led to a significant increase in VC of VarV. The intervention effect of the upgraded SECS seems more effective than the conventional intervention methods, such as health education, household monetary incentives, and provider prompts.Citation27,Citation28 This also proved that the SECS is an appropriate opportunity to recommend vaccines for children to improve coverage,Citation29-31 even if the recommended vaccine is a non-EPI vaccine, which is voluntary and must be self-paid in China. Although the overall intervention effect was similar between the T and W groups, the effect on the urban subgroup in the W group was superior to that in the T group. It could be partially explained by that parents from the urban area might be busy with urgent work when they receive the intervention telephone, so they did not care about the intention of the call. Fortunately, the written notification intervention measure will address similar problems like that. Therefore, we may be more inclined to take the written notification intervention measure in the future.
We also observed some interesting findings. For example, the effect of two intervention groups in primary school and rural areas were slightly superior to that of kindergarten and urban areas. For primary school children, most of the EPI vaccines have been completed, and they are less likely to receive recommended vaccines without intervention. However, parents also have noticed that varicella is a prevalent disease in primary school (children aged 5–9 years), and most outbreaks occurred in primary schools,Citation7,Citation32 so the intervention effect may be better. The fact that rural parents might be more likely to accept and pay for VarV than urban parents in our study merits further investigation. Another interesting finding is that although we did not recommend two doses of VarV during the study period, 39 students vaccinated the second dose of VarV with a proportion of 1.0%. But more interestingly, we observed that the proportion of receiving the second dose of VarV in W group school (2.0%) was significantly higher than T group school (0.7%) and C group schools (0.2%), indicating that the intervention based on written notification may have an indirect positive effect. The finding may be explained by the spillover effect, which was once observed in simultaneous vaccination of multiple vaccines during one health care visit.Citation16 Considering the written notification would be distributed to students in each W group school, those students who have received one-dose of VarV might also inadvertently receive the information about the vaccination. Therefore, we consider that the spillover effect may directly impact the VC of two doses of VarV when the upgraded SECS policy is fully implemented in Lu’an.
Strengths and limitations
Our study has some strengths. To the best of our knowledge, the SECS has never been applied to recommend the non-EPI vaccine for school entry students in China. We aimed to address that gap and to quantify the relationship between the SECS policy and the increase of coverage in VarV. Second, our intervention measures were only a small upgrade based on the routine SECS work, and no additional health resources have been invested. However, with this nudge strategy, the benefits of preventing and controlling vaccine-preventable diseases are apparent. Third, previous studies have demonstrated that a long-term moderate VC level may shift varicella infection to older ages.Citation3,Citation33 Therefore, our findings may help develop targeted public health strategies and reduce the disease burden, especially in regions where the VarV is not introduced into EPI.
Our findings are subject to the following limitations. The first limitation was that the townships and schools included in our study were selected by convenience sampling. Therefore, the actual coverage of VarV at the baseline might be overestimated. Second, as the follow-up period was too long, there was no way to determine whether the increased VC was attributable to the interventions or other factors. However, we found that most students received VarV within one month, indicating that the other factors might be negligible.
Conclusions
Our study demonstrated that the upgraded SECS produces a positive effect on improving varicella vaccination coverage. We believe our findings contribute to the control of varicella in school and stress the importance of considering adjusting the current SECS in China, especially in provinces where the VarV is not introduced into EPI. However, this is only an alternative policy, and the introduction of the VarV into EPI will be the key strategy for China to control varicella.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Authors’ contributions
Wei Qin designed and conceptualized this study. Wei Qin, Jian Song, and Tingyue Nie participated in the data analysis and drafted the manuscript. Hong Su and Shaoyu Xie critically reviewed and supervised the development of the paper. Yao Wang, Fan Pan, Ruyu Ni, Shishi Cheng, Xiangmei Meng, and Hailin Tao performed the field investigation and participated in the immunization record review. Xiaokang Xu was responsible for data visualization. All the authors reviewed and edited the final manuscript.
Acknowledgments
The authors are grateful for the contributions of the public health workers from Jin’an, Yu’an, Yeji, Jinzhai, Shucheng, Huoshan, and Huoqiu, who performed the field investigation and implemented interventions. Many thanks to interns from Wannan Medical College and Bengbu Medical College, who participated in data entry.
Additional information
Funding
References
- Marin M, Marti M, Kambhampati A, Jeram SM, Seward JF. Global varicella vaccine effectiveness: a meta-analysis. Pediatrics. 2016;137(3):e20153741. doi:10.1542/peds.2015-3741.
- Yue C, Li Y, Wang Y, Liu Y, Cao L, Zhu X, Martin K, Wang H, An Z. The varicella vaccination pattern among children under 5 years old in selected areas in China. Oncotarget. 2017;8(28):45612–18. doi:10.18632/oncotarget.17317.
- Qin W, Meng X, Zhang L, Wang Y, Xu X, Li K, Xie S. The impact of long-term moderate level of vaccination coverage for epidemiology of varicella in Lu’an, China: should we change immunisation strategy now. Epidemiol Infect. 2020;148:e74. doi:10.1017/S0950268820000667.
- Hu Y, Chen Y, Zhang B, Li Q. An evaluation of voluntary varicella vaccination coverage in Zhejiang province, East China. Int J Environ Res Public Health. 2016;13:6. doi:10.3390/ijerph13060560.
- Liu AP, Sun TT. Meta-analysis of varicella vaccine coverage among Chinese children. Chin J Vacc Immunization. 2017;23:698–704.
- Suo L, Lu L, Zhao D, Pang X. Impact of a 2-dose voluntary vaccination strategy on varicella epidemiology in Beijing, 2011–2017. Vaccine. 2020;38(20):3690–96. doi:10.1016/j.vaccine.2020.01.087.
- Qin W, Xu XK, Wang Y, Meng XM, Yang CW, Xia F, Su H. Clinical characteristics and risk factors associated with breakthrough varicella during varicella outbreaks. Hum Vaccin Immunother. 2020;16(8):1851–56. doi:10.1080/21645515.2019.1704574.
- Chen YF, Zhou Q, Liu JY, Gong RJ, Mao SQ, Ye ZJ, Wu QS. Characteristics of within-household varicella transmission events associated with school outbreaks in Shanghai, China, 2009–2018. Epidemiol Infect. 2020;148e127. doi:10.1017/S0950268820000448.
- Leung J, Lopez AS, Blostein J, Thayer N, Zipprich J, Clayton A, Buttery V, Andersen J, Thomas CA, Del Rosario M, et al. Impact of the US two-dose varicella vaccination program on the epidemiology of varicella outbreaks: data from nine states, 2005–2012. Pediatr Infect Dis J. 2015;34(10):1105–09. doi:10.1097/INF.0000000000000821.
- Wu QS, Wang X, Liu JY, Chen YF, Zhou Q, Wang Y, Sha JD, Xuan ZL, Zhang LW, Yan L, et al. Varicella outbreak trends in school settings during the voluntary single-dose vaccine era from 2006 to 2017 in Shanghai, China. Int J Infect Dis. 2019:8972–78. doi:10.1016/j.ijid.2019.09.009.
- Weng X, Wang R, Xiaoye LN, Yu L, Zhang Y. Epidemiological characteristics of communicable disease related public health emergencies in schools (child care settings) in China, 2014–2016. Dis Surveillance. 2019;34:446–50.
- Omer SB, Salmon DA, Orenstein WA, deHart MP, Halsey N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N Engl J Med. 2009;360(19):1981–88. doi:10.1056/NEJMsa0806477.
- Feldstein LR, Fox G, Shefer A, Conklin LM, Ward K. School-based delivery of routinely recommended vaccines and opportunities to check vaccination status at school, a global summary, 2008–2017. Vaccine. 2020;38:680–89.
- Attwell K, Navin MC, Lopalco PL, Jestin C, Reiter S, Omer SB. Recent vaccine mandates in the United States, Europe and Australia: a comparative study. Vaccine. 2018;36(48):7377–84. doi:10.1016/j.vaccine.2018.10.019.
- Duan M, Zheng J, Zhou L, Wang L, Cao L, Cao L, Cui J, He G, Xiao Q. Evaluation of a school entry immunization record check strategy in 4 counties of Ningxia and Hubei provinces, China. Vaccine. 2018;36(41):6231–36. doi:10.1016/j.vaccine.2018.07.070.
- Moss JL, Reiter PL, Truong YK, Rimer BK, Brewer NT. School entry requirements and coverage of nontargeted adolescent vaccines. Pediatrics. 2016;138:6. doi:10.1542/peds.2016-1414.
- Choe YJ, Park K, Park E, Kong I, Lee JK. School entry vaccination requirement program: experience from the Republic of Korea. Vaccine. 2018;36(37):5497–99. doi:10.1016/j.vaccine.2018.07.013.
- Ko JS, Goldbeck CS, Baughan EB, Klausner JD. Association between human papillomavirus vaccination school-entry requirements and vaccination initiation. JAMA Pediatr. 2020;174(9):861–67. doi:10.1001/jamapediatrics.2020.1852.
- Zuo S, Zhang D, Mu Q, Dai L, Du W, Xu F, Feng J, Heffelfinger JD. Increasing vaccination coverage: the school entry vaccination record check program in Guizhou province China, 2003–2018. Vaccine. 2020;38(46):7379–83. doi:10.1016/j.vaccine.2020.08.055.
- Handley MA, Schillinger D, Shiboski S. Quasi-experimental designs in practice-based research settings: design and implementation considerations. J Am Board Fam Med. 2011;24(5):589–96. doi:10.3122/jabfm.2011.05.110067.
- Noordzij M, Tripepi G, Dekker FW, Zoccali C, Tanck MW, Jager KJ. Sample size calculations: basic principles and common pitfalls. Nephrol Dial Transplant. 2010;25(5):1388–93. doi:10.1093/ndt/gfp732.
- Heininger U, Seward JF. Varicella. Lancet. 2006;368(9544):1365–76. doi:10.1016/S0140-6736(06)69561-5.
- WHO. Varicella and herpes zoster vaccines: WHO position paper, June 2014. Wkly Epidemiol Rec. 2014;89(25):265–87.
- Wutzler P, Bonanni P, Burgess M, Gershon A, Sáfadi MA, Casabona G. Varicella vaccination - the global experience. Expert Rev Vaccines. 2017;16(8):833–43. doi:10.1080/14760584.2017.1343669.
- Greyson D, Vriesema-Magnuson C, Bettinger JA. Impact of school vaccination mandates on pediatric vaccination coverage: a systematic review. CMAJ Open. 2019;7(3):E524–524E536. doi:10.9778/cmajo.20180191.
- Califano S, Calo WA, Weinberger M, Gilkey MB, Brewer NT. Physician support of HPV vaccination school-entry requirements. Hum Vaccin Immunother. 2016;12(6):1626–32. doi:10.1080/21645515.2016.1149275.
- Oyo-Ita A, Wiysonge CS, Oringanje C, Nwachukwu CE, Oduwole O, Meremikwu MM. Interventions for improving coverage of childhood immunisation in low- and middle-income countries. Cochrane Database Syst Rev. 2016;7CD008145. doi:10.1002/14651858.CD008145.pub3.
- Abdullahi LH, Kagina BM, Ndze VN, Hussey GD, Wiysonge CS. Improving vaccination uptake among adolescents. Cochrane Database Syst Rev. 2020;1CD011895. doi:10.1002/14651858.CD011895.pub2.
- Lopez AS, Kolasa MS, Seward JF. Status of school entry requirements for varicella vaccination and vaccination coverage 11 years after implementation of the varicella vaccination program. J Infect Dis. 2008;197(Suppl):2S76–81.
- Bugenske E, Stokley S, Kennedy A, Dorell C. Middle school vaccination requirements and adolescent vaccination coverage. Pediatrics. 2012;129(6):1056–63. doi:10.1542/peds.2011-2641.
- Thompson EL, Livingston MD 3rd, Daley EM, Zimet GD. Human papillomavirus vaccine initiation for adolescents following rhode island’s school-entry requirement, 2010–2016. Am J Public Health. 2018;108(10):1421–23. doi:10.2105/AJPH.2018.304552.
- Sui HT, Li JC, Wang M, Liu YM, Yin DP. Varicella epidemiology in China, 2005–2015. Chin J Vacc Immunization. 2019;25:155–59.
- Van Hoek AJ, Melegaro A, Zagheni E, Edmunds WJ, Gay N. Modelling the impact of a combined varicella and zoster vaccination programme on the epidemiology of varicella zoster virus in England. Vaccine. 2011;29(13):2411–20. doi:10.1016/j.vaccine.2011.01.037.