
ABSTRACT
Neisseria meningitidis serogroup B (MenB) is the most common cause of meningococcal disease in adolescents and young adults. In Australia, MenB vaccination has been available through private prescription since 2014 and has been recommended for at-risk groups including adolescents, young adults who smoke and people medically at risk. For each of these at-risk groups, we estimated cumulative annual coverage of MenB vaccination between 2014 and 2019. We also evaluated factors associated with vaccination coverage in 2019. Our analyses used electronic health records in the national MedicineInsight database for people regularly attending general practices. Cumulative vaccination coverage increased among the at-risk groups between 2014 and 2019: from 0.09% to 1.65% for adolescents, from 0.01% to 0.15% for young adults who smoke, and from 0.35% to 12.09% for people medically at risk. However, vaccination coverage in 2019 remained very low across these groups. Data sparsity prevented the evaluation of factors associated with vaccination coverage for smokers. We observed variation in the relative risk of being vaccinated by age, sex, socioeconomic and clinical factors for adolescents and people medically at risk. Still, the absolute magnitude of coverage was low across all subgroups examined, and indicates a need for strategies to increase vaccination uptake among at-risk groups irrespective of patient and practice characteristics. Our study provides baseline data for monitoring menB vaccination uptake among recommended groups in light of limited national data, especially for medically at-risk groups.
Introduction
Invasive meningococcal disease (IMD) is caused by the bacterium Neisseria meningitidis and affects 0.5–1.2 million people worldwide, each year.Citation1 Despite being rare, IMD can lead to death in up to 1 in 10 people infected. Moreover, up to 20% of survivors may have permanent physical and neurological sequelae.Citation2 IMD is most common in children under five years of age and adolescents (15–19 years of age), with the latter having the highest carriage rates (7%-37%) which contribute to spread of the bacteria.Citation1,Citation3 In Australia, the annual incidence of IMD is low (1.1/100,000 people in 2018) but it increased by 83% between 2013 and 2018 and peaked in 2017 at 1.5/100,000 people.Citation4
From thirteen known meningococcal serogroups, serogroups A, B, C, W and Y cause more than 95% of disease.Citation2 As in other developed countries, serogroup B has been dominant over time, likely due to lack of widespread use of a vaccine targeting this serogroup. It accounted for approximately 52% of cases in recent years.Citation5–7 The first meningococcal serogroup B (MenB) vaccine was introduced in the Australian market in 2014, and was initially available by private prescription only.Citation8,Citation9 The Australian Technical Advisory Group on Immunisation (ATAGI) recommend its use in populations at increased risk of IMD.Citation9 Currently, these populations include children and infants under two years old, Indigenous peoples aged 2–19 years, adolescents aged 15–19 years, young adults (aged 20–24 years) who smoke, live in close quarters or work in laboratories, or people with immunosuppressive conditions such as HIV, asplenia or treated with eculizumab.Citation10 From July 2020 MenB vaccination has been funded through Australia’s National Immunisation Program (NIP) for Indigenous infant and individuals of any age with asplenia, hyposplenia, complement deficiency or on eculizumab treatment.Citation9,Citation11
Monitoring meningococcal vaccination coverage and identifying factors associated with vaccination uptake are core components of an effective strategy to curb IMD and its devastating outcomes. Moreover, when combined with data from disease notification systems, vaccination coverage estimates can inform estimates of the real-world effectiveness of the vaccine.Citation12 However, no national estimates of MenB vaccine coverage in Australia have been published to date, and obtaining such estimates is challenging due to the lack of a comprehensive and nationally consistent source of data on vaccines administered. The Australian Immunisation Register (AIR) expanded to capture vaccinations given to people of all ages in 2016, however there is significant underreporting for adult vaccination and potential underreporting for non-funded vaccines.Citation13 The AIR also does not capture information on medical conditions, making assessment of coverage in at-risk groups challenging.Citation14 In this context, studies using secondary data such as electronic health records (EHR) from general practicesCitation15–18 have been increasingly used to estimate immunisation rates in Australia. This data source is particularly useful to estimate vaccinations predominantly delivered in general practices, such as MenB.
In this study, we aimed to calculate the first national estimates of cumulative annual MenB vaccination rates over the six years following introduction of this vaccine in Australia among three key at-risk groups: adolescents, young adults who smoke and people medically at risk. We also examined the characteristics associated with vaccination coverage within each at-risk group in the most recent year for which data were available to inform targeting of future MenB vaccination programs.
Methods
Setting and access to vaccines in the study period
Two multicomponent protein-based recombinant vaccines are available in Australia to prevent MenB disease in adolescents and adults: Bexsero® (4CMenB), introduced in the market in 2014 and Trumenba®, available since 2017. These vaccines include distinct proteins and are not interchangeable. Both require two or more doses and boosters are not recommended.Citation4
Free access to selected vaccines is provided through the NIP, and states and territories may fund additional programs, as needed. Outside of these government programs, vaccines can be obtained through private prescriptions. During our study period, MenB vaccines were not included in the NIP schedule, and the only state program was that in South Australia, where free MenB vaccinations have been available for children and adolescents since 2017 as part of school-based programs.Citation8,Citation9
Data source
Details of the MedicineInsight dataset has been published elsewhere.Citation19,Citation20 Briefly, it is a large-scale dataset of longitudinal de-identified data extracted from EHR from approximately 700 participating general practices across Australia. Each patient in a practice site has a unique identifying number which allows longitudinal records pertaining to the same patient to be linked. In 2018–2019, it included data on approximately 2.9 million patients who were seen at least once by a general practitioner (GP) in the participating practices. This represented approximately 13% of patients attending general practices in the country during 2018–2019.Citation20 MedicineInsight patients are broadly similar when compared to national MBS information for patients who visited a GP during 2018–2019, in terms of age, gender and socioeconomic status. However, there is an overrepresentation of patients in Tasmania (6.5% in MedicineInsight vs 2.2% nationally) and underrepresentation of patients in South Australia (2.6% vs 7.0%).Citation20
Study design and study population
We examined annual cross-sections from the MedicineInsight dataset between 1 January 2014 and 31 December 2019 to determine cumulative vaccination rates each year for regular general practice patients stratified by at-risk groups: adolescents aged 15–19 years, young adults (20–24 years old) who smoke, and people with relevant immunosuppressive disorders aged 10 years or older. Regular patients were defined as those who had at least three consultations in two consecutive years in a single general practice, including the calendar year of interest and the prior year.Citation21 This criterion minimizes the probability of including temporary patients or visitors for whom details on lifetime vaccination, health conditions and other risk behaviors are poorly captured in MedicineInsight. Historical records outside of this study period were consulted when identifying patient demographics, chronic health conditions and prior vaccination.
Age was calculated at the beginning of the year of interest, based on the patient’s year of birth. Patients’ current smoking status was defined as the most recent status recorded in the EHR, and included the options ‘nonsmoker’, ‘smoker’, ‘ex-smoker’, or ‘not recorded’. Patients were classified as having immunosuppressive disorders if terms related to the following conditions were recorded in the EHR: deficiency of complement components, functional or anatomic asplenia, bone marrow transplant or HIV. Furthermore, patients who were ever prescribed ‘eculizumab’ were also classified as having an immunosuppressive disorder (See Box 1).
Vaccination measures
MedicineInsight data contain fields in which immunisations and the date they were administered are recorded. These fields contain vaccinations administered at the practice or reported by the patient. The information can be recorded by health professionals using either standard codes or ‘free text’ descriptions. To identify MenB vaccinations from the immunisation field, we adapted algorithms previously described.Citation15,Citation16,Citation18 The algorithm searched for brand names of vaccines and synonyms, retrieving any record containing potentially eligible terms. In a second stage, we manually screened all terms recovered to exclude non-relevant records (See Box 2).
We considered a patient as vaccinated if he/she had a recorded vaccination within each year of interest or any time prior (e.g. for 2019 we looked for vaccination in 2019 or any time prior in the dataset), resulting in cumulative estimates of vaccination each year. Since MenB vaccines were introduced in 2014, we only searched records from 2014 onwards. The cumulative annual vaccination rate for each year was estimated as the number of individuals vaccinated divided by the total number of individuals who were considered regular patients that year within each at-risk group.
Covariates
Patient covariates included (i) sociodemographic characteristics [age, sex, rurality, and the socioeconomic indexes for area (SEIFA) of relative socioeconomic advantage and disadvantage (IRSAD) quintile – a macroeconomic indicator of socioeconomic status within an area/postcode compared to the rest of the country] (ii) clinical characteristics [immunosuppressive disorders, median number of clinical encounters in the prior year] (iii) behavioral characteristics [smoking status]. Practice characteristics included state/territory, rurality and IRSAD quintiles.
Rurality was assigned based on a mapping of each patient’s postcode of residence using the Australian Bureau of Statistics mapping of postcode to remoteness areas and classified as ‘Major city’, ‘Inner regional’, ‘Outer regional’, ‘Remote/Very remote’. IRSAD was assigned based on a mapping of Postcode 2016 to IRSAD quintiles from 1 (most disadvantaged) to 5 (most advantaged).
Statistical analysis
We carried out all analysis stratified by the three at-risk groups. Cumulative vaccination was calculated by year and presented as percentage of eligible regular patients with 95% confidence intervals (95% CI). We excluded data from South Australian practices in our measurement of adolescent vaccination, anticipating that the MedicineInsight data would have lower capture of adolescent vaccinations in South Australia due to delivery of vaccines via state-funded school-based programs.
We described overall characteristics of the study population in 2019 (the most recent year) as absolute numbers and percentages for categorical variables and means (SD) for continuous variables. The association between cumulative vaccination coverage in 2019 and sociodemographic, clinical, and behavioral characteristics were assessed via logistic regression using robust variance to account for clustering of patients within practices. The crude associations were fully and mutually adjusted for patients’ and practices’ characteristics using odds ratios (OR) and 95% CI. We also tested the final model for multicollinearity by assessing the variance inflation factor (VIF) and tolerance and model goodness of fit by assessing the Hosmer–Lemeshow test.
Analyses were performed in the statistical software SAS Enterprise Guide SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics and data access approval
This study was approved by the Royal Australian College of General Practitioners Human Research Ethics Committee (NREEC 20–006) and data access was granted by the independent MedicineInsight Data Governance Committee (Protocol 019–031).
Results
Our study’s annual cohorts varied from 77,188 to 89,042 adolescents, 17,373 to 16,067 young adults who smoke, and 4,810 to 5,559 people medically at risk of meningococcal infection (See ). As illustrated in the cohort selection diagram for the 2019 annual cohorts, most people excluded were non-regular patients for all at-risk groups examined ().
Figure 1. Cohort selection process for the 2019 annual cohorts
Characteristics of the study population for the 2019 annual cohorts ()
Adolescents: The mean age was 17.1 (SD <±0.1) years, and 57% were female. A high proportion resided in major cities (61%) or lived in areas from the third IRSAD quintiles or above (65%). Adolescents commonly attended practices in New South Wales (NSW; 35%) and those located in the most advantaged areas (25%). Few adolescents had medical conditions associated with an increased risk of IMD (n = 45, 0.05%).
Table 1. Characteristics of the three at-risk groups for the 2019 annual cohort
Young people who smoke: The mean age was 22.2 (SD <±0.1) years, and 52% were female. A high proportion of them resided in major cities (57%) or lived in lower socioeconomic status areas (first and second IRSAD quintiles, 46%). Young smokers commonly attended practices in NSW and Victoria or those located in the most disadvantaged areas (29%). Only a small number of young smokers had medical conditions associated with an increased risk of IMD (n = 13, 0.1%).
People medically at risk: The mean age was 56.8 (SD 1.0) years, with a large proportion aged 51 years or older (67%). A high proportion was male (63%), resided in major cities (62%) or lived in the most advantaged socioeconomic areas (26%). Most people attended practices located in major cities (64%), located in NSW and Victoria (31%-34%) or the most advantaged socioeconomic areas (33%). This group of people medically at risk had a higher median number of clinical encounters in general practices in the prior year compared to the other two at-risk groups examined (seven vs three). The most common medical conditions were asplenia or splenic dysfunction (n = 3,067, 55%), HIV infection (n = 1,705, 31%) and hematopoietic stem cell transplant (n = 795, 14%) [data not shown in table].
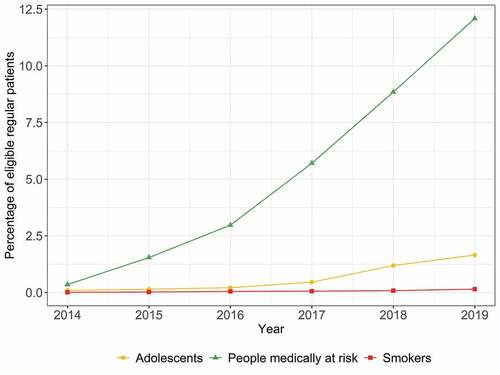
Cumulative MenB vaccination coverage (, )
Cumulative vaccination coverage increased from 2014 to 2019 among all at-risk groups examined, with the highest growth observed for people medically at risk. For this group, cumulative coverage rose from 0.35% (95% CI 0.18%, 0.53%) to 12.09% (9.12%, 15.06%). Coverage increased from 0.09% (0.05%, 0.13%) to 1.65% (1.23%, 2.08%) among adolescents, with higher growth from 2017 onwards within this group. Finally, whilst there was an increase in cumulative coverage amongst young adults who smoke (from 0.01% to 0.15%), the absolute magnitude remained very low during the study period.
Figure 2. Annual MenB vaccination coverage according to at-risk groups
Factors associated with MenB vaccination coverage ()
Due to sparse data for vaccinated young adults who smoke (n = 24), we only evaluated factors associated with vaccination coverage among adolescents and people medically at risk. For these at-risk groups, we observed significant variation in the relative risk of being vaccinated according to patient and practice characteristics.
Table 2. Meningococcal B coverage according to patient and practice characteristics and factors associated with being vaccinated for the 2019 annual cohorts
Adolescents: Older age was associated with lower vaccination coverage, with adolescents aged 17 to 19 years having 19%-42% less chance of being vaccinated than those aged 15 years. Males had a higher probability of being vaccinated (aOR = 1.21), as did adolescents living in higher socioeconomic areas (aOR = 1.76 to 4.80 across different categories), those having more than three encounters to general practices in the prior year (aOR = 2.02) or those with any relevant medical condition (aOR = 30.92). Finally, adolescents attending practices located in Tasmania were 21 times more likely to be vaccinated than those attending practices in NSW (aOR = 21.23). Despite these significant relative risks, crude vaccination coverage remained low at approximately 1–2% across all subgroups of adolescents examined. The only two exceptions were adolescents with relevant medical conditions and adolescents residing in Tasmania (31% and 9% of coverage, respectively).
People medically at risk: Older age was associated with lower vaccination coverage, with people aged 20 years or older having approximately 75% less chance of being vaccinated than those aged 10–14 years. Males also had a lower probability of being vaccinated than females (aOR = 0.52). A higher probability of having a recorded vaccination was observed among those attending general practices more than seven times in the prior year (aOR = 1.99) or those attending practices in Tasmania compared to people attending practices in NSW (aOR = 2.11). Despite these significant relative risks, crude vaccination coverage reached a maximum of 36% among people in medically at-risk aged 10–14 years.
Discussion
This study investigated cumulative rates of meningococcal B vaccination among three at-risk groups of invasive meningococcal disease in the Australian general practice setting, and provides the first national estimates of MenB vaccine coverage. Encouragingly, we found increased cumulative rates of immunisation in the years since the vaccine was introduced, especially among people with immunosuppressive disorders. However, coverage remains very low (<15%) across all subgroups evaluated. These results highlight the need for strategies to increase vaccination uptake and monitoring across the whole population of individuals at-risk of IMD.
The lowest rates of vaccination coverage were observed among young adults who smoke compared to other at-risk groups, which is consistent with prior reporting that people with unhealthy lifestyles are less likely to be vaccinated against other preventable conditions.Citation16,Citation22–24 This result is concerning since smoking facilitates meningococcal colonization of the nasopharynx, increasing carriage rates in a dose-response relationship for both smokers and people exposed to second-hand smoke.Citation25,Citation26 This low coverage may partly be explained by the recency (July 2018) of the recommendation to vaccinate young smokers against MenB,Citation9 and suggests a need for health promotion to this group, and that continued monitoring of vaccination coverage in this group would be valuable.
Reassuringly, we found increasing cumulative rates of vaccination among people with immunosuppressive disorders. This result is not surprising since people with chronic health conditions may visit general practices regularly, allowing for multiple vaccination opportunities.Citation16 However, the overall coverage was still modest (12%), consistent with the limited data available on MenB coverage among various at-risk subpopulations in other parts of the world, including asplenic or splenectomized patients (13%)Citation27 and men who have sex with men (14%-34%).Citation28,Citation29 High coverage is likely to be achievable through funded-vaccination programs, with a previous program targeting men who have sex with men in Victoria achieving 46% coverage for MenACWY vaccine among people living with HIV.Citation30 It would be worth evaluating whether this is achieved with the recent inclusion of the MenB vaccine in the NIP for people with specified medical risk conditions.
In Australia, adolescents have been identified as one of the key priority populations at-risk for MenB vaccination, with the peak of MenB disease occurring under four years of age and again between 15–19 years of age.Citation7 However, due to evidence of lack of indirect protection via reducing carriage, and uncertainty regarding the magnitude of clinical effectiveness for children and adolescents, current MenB vaccines are not subsidized for all adolescents in Australia (only subsidized for those with medical conditions, as of 2020).Citation8,Citation9,Citation11 As such, further investment in improved vaccine development, including reducing carriage and bacterial reservoirs (to reduce transmission), is needed. Meanwhile, increasing coverage amongst populations at-risk for direct protection is the most effective way to prevent IMD.Citation8
Our estimates show vaccination for MenB for adolescents is substantially lower than what can be achieved by funded programs. Jurisdictional data available for adolescent MenACWY vaccination show coverage of approximately 70% among students aged 14–19 years participating in school-based programs.Citation31,Citation32 It is well known that the provision of free vaccination at the point of care is one of the most effective ways to increase vaccination uptake, with the majority of people being vaccinated after they become eligible to receive funded vaccines.Citation15–17,Citation33 Additionally, school-based programs have been identified as more effective than general practices in achieving high uptake for this population.Citation34,Citation35 Interestingly, we observed the increase in MenB vaccination uptake after the peak of IMD cases reported in Australia in 2017Citation4 and after funding for vaccines targeting other meningococcal serogroups (i.e, MenACWY) for adolescents was implemented in most states and territories in the country.Citation9 These events may have increased awareness for serogroup B vaccination for adolescents among clinicians and the public in general.
Whilst we found variation in vaccination coverage according to sex, age, socioeconomic and clinical factors in adolescents and medically at-risk groups, the absolute magnitude of coverage was low amongst all subgroups examined, highlighting the need for strategies to increase MenB vaccination uptake among at-risk groups. This should be more straightforward for those with specified medical conditions now eligible for free vaccination under the NIP, however will be more challenging for groups not eligible. In the absence of any expansion of NIP eligibility criteria, equity of access to MenB vaccination will remain a significant issue, noting that obtaining the vaccine through private prescription is associated with an out-of-pocket cost of approximately USD 75 per dose.Citation36,Citation37 The variations we observed in coverage rates according to socioeconomic status of the patients’ area of residence suggest that financial barriers are preventing people from being vaccinated. Moreover, almost one-third of general practitioners do not regularly discuss unfunded vaccination options with their patients, with the cost of the vaccine and patients’ socioeconomic status being strong barries for prescribing non-funded vaccines.Citation38 Therefore, it is important that governments consider equity issues in their decision-making around funding MenB vaccines for populations at-higher risk of IMD, not merely cost-effectiveness assessment.
General practices play a key role in reducing the burden of vaccine-preventable diseases. Most people in Australia are immunised in general practices,Citation39 with GP recommendation being one of the strongest drivers of vaccination uptake.Citation40 This is reflected in the higher vaccination rates among people with increased visits to the GP across all at-risk groups examined. Considering all participants in our study had visited the general practices at least three times in the prior two years, encounters where patients were not vaccinated represent missed opportunities for MenB vaccination. Approaches to reduce those missed opportunities and vaccination hesitancy include assessing vaccination status in every clinical encounter, especially among adolescents who generally do not have regular preventive visits.Citation41,Citation42 Software that identifies people eligible for vaccination and provides reminders of these vaccines may assist physicians to discuss immunisation with their clients.Citation42 The use of evidence-based messages that are patient-friendly helps address both the lack of information about vaccination and builds trust with clients and carers in recommendations to vaccinate.Citation41 These approaches should be supported by broader strategies from public health authorities to increase awareness of recommendations, risk of disease, and benefits of vaccination among adolescents and adults.
Limitations of this study
Our study has several limitations. First, as MedicineInsight data do not capture vaccinations administered in workplaces, pharmacies, and other non-general practice immunisation settings unless recorded by the GP, the results likely underestimate coverage. The risk of underestimation affects the groups examined differently: while adolescents and young adults are infrequent users of healthcare services, people medically at risk are more likely to frequent healthcare services, increasing the opportunities for vaccination and its recording in the EHR even if administered in other settings. Second, MedicineInsight data collects data generated for clinical purposes so that the quality and accuracy of records depend on each practice and clinician standards. Third, patients may visit multiple general practices, and we were not able to link information for the same patient across various practice sites and the impact of this in our vaccination estimates is not possible to ascertain. Finally, our study population includes only patients regularly attending general practices, where these individuals may have different patterns of health services utilisation than the broader population.
Conclusion
Our study provides the first national estimates of meningococcal B vaccine coverage in Australia. Despite increased rates of meningococcal B vaccination coverage in the years since the vaccine was introduced, coverage remains suboptimal for all at-risk groups examined. The evaluation of coverage by patient and practices characteristics showed estimates were low across the board. These results highlight the need for interventions to increase vaccination uptake for direct protection against invasive meningococcal disease.
Noting the challenges in measuring vaccination coverage among adolescents and adults, particularly those with at-risk medical conditions, this study provides baseline data for monitoring meningococcal B vaccination uptake among recommended groups. There is likely particular value in evaluating whether recent vaccination funding for people medically at risk has led to improved vaccination uptake in this group. Our findings should also be of interest in other countries, given the limited data available on meningococcal B vaccine coverage in medically at-risk groups.
Disclosure of potential conflicts of interest
The study was funded by Pfizer who had no role in the design of the study, data collection, analysis or interpretation, nor in writing the manuscript. The Centre for Big Data Research in Health, UNSW Sydney has received funding from AbbVie to conduct research, unrelated to the present study. AbbVie did not have any knowledge of, or involvement in, the present study. C.G., K.C., and R.O. are all employees of NPS MedicineWise, the data custodian for MedicineInsight.
Acknowledgments
This research is supported by the National Health and Medical Research Council (NHMRC) Centre of Research Excellence in Medicines Intelligence (ID: 1196900). We thank Suzanne Blogg and Jill Thistlethwaite for critically revising this manuscript. We also thank Catherine Hughes for her contribution in the development of the recommendations. We are grateful to the general practices, general practitioners and patients who allow the use of de-identified information for MedicineInsight.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Stephens DS, Greenwood B, Brandtzaeg P. Epidemic meningitis, meningococcaemia, and Neisseria meningitidis. Lancet. 2007;369:2196–210. doi:10.1016/S0140-6736(07)61016-2.
- Rouphael NG, Stephens DS. Neisseria meningitidis: biology, microbiology, and epidemiology. Methods Mol Biol. 2012;799:1–20.
- Burman C, Serra L, Nuttens C, Presa J, Balmer P, York L. Meningococcal disease in adolescents and young adults: a review of the rationale for prevention through vaccination. Hum Vaccin Immunother. 2019;15:459–69. doi:10.1080/21645515.2018.1528831.
- Australian Government Department of Health. Invasive meningococcal disease National Surveillance Report. Semester 1: 1 January to 30 June 2019. Canberra (ACT). 2019 [accessed 2021 Feb 05]. https://www1.health.gov.au/internet/main/publishing.nsf/Content/5FEABC4B495BDEC1CA25807D001327FA/$File/IMD-surveil-report-Jan-June-2019.pdf .
- Vuocolo S, Balmer P, Gruber WC, Jansen KU, Anderson AS, Perez JL, York LJ. Vaccination strategies for the prevention of meningococcal disease. Hum Vaccin Immunother. 2018;14:1203–15. doi:10.1080/21645515.2018.1451287.
- Leca M, Bornet C, Montana M, Curti C, Vanelle P. Meningococcal vaccines: current state and future outlook. Pathologie-biologie. 2015;63:144–51. doi:10.1016/j.patbio.2015.04.003.
- Archer BN, Chiu CK, Jayasinghe SH, Richmond PC, McVernon J, Lahra MM, Andrews RM, McIntyre PB. Epidemiology of invasive meningococcal B disease in Australia, 1999-2015: priority populations for vaccination. Med J Aust. 2017;207:382–87. doi:10.5694/mja16.01340.
- Marshall HS, McMillan M, Koehler AP, Lawrence A, Sullivan TR, MacLennan JM, Maiden MCJ, Ladhani SN, Ramsay ME, Trotter C, et al. Meningococcal B vaccine and meningococcal carriage in adolescents in Australia. N Engl J Med. 2020;382(4):318–27. doi:10.1056/NEJMoa1900236.
- National Centre for Immunisation Research and Surveillance. Significant events in meningococcal vaccination practice in Australia; Sydney (NSW): National Centre for Immunisation Research and Surveillance; 2020 [accessed 2020 Aug 10]. https://www.ncirs.org.au/sites/default/files/2020-07/Meningococcal-history-July%202020.pdf .
- Australian Technical Advisory Group on Immunisation (ATAGI). Australian immunisation handbook. Canberra (ACT): Australian Government Department of Health; 2020 [accessed 2021 Mar 15]. https://immunisationhandbook.health.gov.au .
- Pharmaceutical Benefits Advisory Committee. Public Summary Document - November 2019 PBAC Meeting: Multicomponent Meningococcal group B vaccine: Injection 0.5 mL; Bexsero®. Canberra (ACT): PharmaceuticalBenefits Scheme; 2019 [accessed 2020 Dec 11]. https://www.pbs.gov.au/pbs/industry/listing/elements/pbac-meetings/psd/2019-11/multicomponent-meningococcal-group-b-vaccine-injection-0-5-bexsero .
- Snape MD, Medini D, Halperin SA, DeTora L, Drori J, Moxon ER. The challenge of post-implementation surveillance for novel meningococcal vaccines. Vaccine. 2012;30(Suppl 2):B67–72. doi:10.1016/j.vaccine.2011.12.126.
- Brynley Hull A, Dey A, Macartney K, McIntyre P, Beard F. Exploratory analysis of the first 2 years of adult vaccination data recorded on AIR. Sydney (NSW): National Centre for Immunisation Research and Surveillance; 2019.
- Tuckerman J, Blyth CC, Beard FH, Danchin MH. COVID-19 and changes in the National Immunisation Program: a unique opportunity to optimise the Australian Immunisation Register (AIR). Med J Aust. 2021;214(247–9.e1):247. doi:10.5694/mja2.50971.
- Lin J, Wood JG, Bernardo C, Stocks NP, Liu B. Herpes zoster vaccine coverage in Australia before and after introduction of a national vaccination program. Vaccine. 2020;38:3646–52. doi:10.1016/j.vaccine.2020.03.036.
- Frank O, De Oliveira Bernardo C, Gonzalez-Chica DA, Macartney K, Menzies R, Stocks N. Pneumococcal vaccination uptake among patients aged 65 years or over in Australian general practice. Hum Vaccin Immunother. 2020;16:965–71. doi:10.1080/21645515.2019.1682844.
- De Oliveira Bernardo C, Gonzalez-Chica DA, Stocks N. Impact of funding influenza vaccination on coverage among Australian children: a national study using MedicineInsight, a large general practice database. Hum Vaccin Immunother. 2020;16:630–35. doi:10.1080/21645515.2019.1664866.
- De Oliveira Bernardo C, Gonzalez-Chica DA, Chilver M, Stocks N. Influenza immunisation coverage from 2015 to 2017: a national study of adult patients from Australian general practice. Vaccine. 2019;37:4268–74. doi:10.1016/j.vaccine.2019.06.057.
- Busingye D, Gianacas C, Pollack A, Chidwick K, Merrifield A, Norman S, Mullin B, Hayhurst R, Blogg S, Havard A, et al. Data resource profile: medicineInsight, an Australian national primary health care database. Int J Epidemiol. 2019;48:1741–h.
- NPS MedicineWise. MedicineInsight general practice insights report: July 2018 – June 2019. NPS MedicineWise: Sydney (NSW); 2020 [accessed 2020 Nov 15]. https://www.nps.org.au/assets/Report-2018-19-GPIR.pdf
- The Royal Australian College of General Practitioners (RACGP). Standards for general practices. East Melbourne (Victoria): RACGP; 2017.
- Rodríguez-Rieiro C, Domínguez-Berjón MF, Esteban-vasallodomínguez-berjón MD, Cuadrado AR, Carrasco-Garrido P, Jiménez-García R. Coverage and predictors of influenza vaccine uptake among adults aged 16 to 59 years suffering from a chronic condition in Madrid, Spain. Hum Vaccin. 2011;7:557–62. doi:10.4161/hv.7.5.14984.
- Chen CH, Wu MS, Wu IC. Vaccination coverage and associated factors for receipt of the 23-valent pneumococcal polysaccharide vaccine in Taiwan: a nation-wide community-based study. Medicine. 2018;97:e9773. doi:10.1097/MD.0000000000009773.
- Looijmans-van den Akker I, van den Heuvel Pm Fau - Verheij TJM, Verheij Tj Fau - van Delden JJM, van Delden Jj Fau - van Essen GA, van Essen Ga Fau - Hak E, Hak E. No intention to comply with influenza and pneumococcal vaccination: behavioural determinants among smokers and non-smokers. Prev Med. 2007;45:380–85. doi:10.1016/j.ypmed.2007.07.009.
- Arcavi L, Benowitz NL. Cigarette smoking and infection. Arch Intern Med. 2004;164:2206–16. doi:10.1001/archinte.164.20.2206.
- Stuart J, Robinson P, Cartwright KV, Noah N. Effect of smoking on meningococcal carriage. Lancet. 1989;334:723–25. doi:10.1016/S0140-6736(89)90781-2.
- Bianchi FP, Stefanizzi P, Spinelli G, Mascipinto S, Tafuri S. Immunization coverage among asplenic patients and strategies to increase vaccination compliance: a systematic review and meta-analysis. Expert Rev Vaccines. 2021;20:1–12. doi:10.1080/14760584.2021.1886085.
- Holloway IW, Bednarczyk R, Fenimore VL, Goldbeck C, Wu E, Himmelstein R, Tan D, Randall L, Lutz CS, Frew PM. Factors Associated with Immunization Opinion Leadership among Men Who Have Sex with Men in Los Angeles, California. Int J Environ Res Public Health. 2018;15(5):939. doi:10.3390/ijerph15050939.
- Frew PM, Holloway IW, Goldbeck C, Tan D, Wu E, Jauregui J, Fenimore VL, Randall LA, Lutz CS, Mendel J, et al. Development of a measure to assess vaccine confidence among men who have sex with men. Expert Rev Vaccines. 2018;17:1053–61. doi:10.1080/14760584.2018.1541405.
- Martin-Sanchez M, Fairley CK, Bradshaw CS, Chen MY, Chow EPF. Meningococcal vaccine uptake among men who have sex with men in response to an invasive meningococcal C disease outbreak in Melbourne, Australia. Sex Transm Infect. 2020;96(4):246–50. doi:10.1136/sextrans-2019-054318.
- Hendry A, Hull B, Dey A, Reid S, Ennis S, Macartney K, Beard F. NSW annual immunisation coverage report 2018; Sydney (NSW): NSW Health; 2019. [accessed 2020 Nov 11]. https://www.health.nsw.gov.au/immunisation/Documents/2018-annual-coverage-report.pdf .
- Queesland Government. Queensland school immunisation program: 2019 annual report. 2020.
- Dyda A, McIntyre P, Karki S, MacIntyre CR, Newall AT, Banks E, Kaldor J, Liu B. Pertussis vaccination in a cohort of older Australian adults following a cocooning vaccination program. Vaccine. 2018;36:4157–60. doi:10.1016/j.vaccine.2018.05.109.
- Ward K, Quinn H, Menzies R, McIntyre P. A history of adolescent school based vaccination in Australia. Commun Dis Intell Q Rep. 2013;37:E168–74.
- Kassianos G, MacDonald P, Aloysius I, Reynolds A. Implementation of the United Kingdom’s childhood influenza national vaccination programme: a review of clinical impact and lessons learned over six influenza seasons. Vaccine. 2020;38:5747–58. doi:10.1016/j.vaccine.2020.06.065.
- OECD. Purchasing power parities (PPP) (indicator). 2021. [accessed 2021 Mar 02]. doi: 10.1787/1290ee5a-en.
- Chemist Warehouse. Price of meningococcal B vaccines Trumenba and Bexsero for private prescription. 2021 [accessed 2021 Mar 02]. https://www.chemistwarehouse.com.au
- Taylor KA, Stocks N, Marshall HS. The missing link: family physician perspectives on barriers and enablers to prescribing a new Meningococcal B vaccine and other recommended, non-government funded vaccines. Vaccine. 2014;32:4214–19. doi:10.1016/j.vaccine.2014.04.046.
- Hull B, Hendry A, Dey A, Brotherton J, Macartney K, Beard F. Annual immunisation coverage report 2017. Commun Dis Intell. 2018;2019:43. doi: 10.33321/cdi.2019.43.47.
- Marshall H, Clarke M, Sullivan T. Parental and community acceptance of the benefits and risks associated with meningococcal B vaccines. Vaccine. 2014;32:338–44. doi:10.1016/j.vaccine.2013.11.042.
- Azzari C, Diez-Domingo J, Eisenstein E, Faust SN, Konstantopoulos A, Marshall GS, Rodrigues F, Schwarz TF, Weil-Olivier C. Experts’ opinion for improving global adolescent vaccination rates: a call to action. Eur J Pediatr. 2020;179:547–53. doi:10.1007/s00431-019-03511-8.
- Hunter PMD, Fryhofer SAMD, Szilagyi PGMDMPH. Vaccination of adults in general medical practice. Mayo Clin Proc. 2020;95:169–83. doi:10.1016/j.mayocp.2019.02.024.
Appendix
Box 1. Terms and combinations used to identify immunosuppressive disorders.
Box 2. Search list for identifying vaccines.
Table A1.
Annual MenB vaccination coverage according to at-risk group