ABSTRACT
An uninterrupted supply of vaccines at different supply chain levels is a basic component of a functional immunization programme and care service. There can be no progress toward achieving universal health coverage and sustainable development without continuous availability of essential medicines and vaccines in healthcare facilities. Shortages of vaccines, particularly at health facility level is an issue of grave concern that requires urgent attention in South Africa. The causes of vaccine stock-outs are multifactorial and may be linked to a broader systems issue. These factors include challenges at higher levels such as delays in the delivery of stock from the pharmaceutical depot; health facility level factors, which include a lack of commitment from healthcare workers and managers; human resource factors, such as, staff shortages, and lack of skilled personnel. Therefore, there is a compelling need to address the factors associated with shortages of vaccines in health facilities. This paper highlights the challenges of vaccine availability in South Africa, the associated factors, the available interventions, and recommended interventions for the expanded programme on immunization in South Africa. We propose a system redesign approach as a potentially useful intervention.
Introduction
The availability of health commodities at the point of service delivery is a fundamental component of the health system and also crucial for achieving universal health coverage (UHC).Citation1,Citation2 Immunization coverage is also used as an indicator for monitoring the coverage of essential services and measuring the progress of Sustainable Development Goal (SDG) 3.8.Citation3 One of the factors contributing to missed opportunities for vaccination in children is vaccine stock-outs.Citation4–6 Vaccine shortages and stock-outs may greatly compromise the health system and impede the attainment of specific health goals. Vaccine stock-outs result in targeted recipients being turned away, which leads to a decrease in immunization coverage and, ultimately, outbreaks of vaccine-preventable diseases may occur.Citation7 Furthermore, repeated and on-going shortages may dent the image of the immunization programme, lead to a decline in demand for immunization services, and further undermine national and global efforts on disease control.Citation8
This paper highlights the challenges of expanded programme on immunization in South Africa, with a focus on vaccine availability and the associated factors. We also discuss the available interventions developed to improve vaccine availability in South Africa and the barriers to their successful implementation.
The Expanded Programme on Immunization (EPI) in South Africa and the occurrence of vaccine stock-outs
The EPI in South Africa (EPI-SA), which became an entity in 1995 with the birth of democracy,Citation9 is aimed at reaching and protecting every child eligible for vaccination.Citation10,Citation11 Before EPI-SA, there were different fragmented programmes in the former Bantustans (TBVC States), non-independent homelands, and what was said to be South Africa.Citation10 Since the establishment of the EPI-SA, significant milestones have been achieved. Some of the milestones include the elimination of polio, with the last reported wild poliovirus case in 1989; elimination of neonatal tetanus in 2002; and the introduction of new vaccines such as rotavirus vaccine and pneumococcal conjugate vaccine (PCV) in 2009 and human papillomavirus (HPV) vaccine in 2014.Citation10 The introduction of PCV in South Africa led to a dramatic decline in cases of pneumococcal diseases in both children and adults.Citation12 In 2009, South Africa became the first country in Africa to self-finance a nationwide introduction of childhood vaccination against rotavirus and Streptococcus pneumoniae, free of charge to recipients.Citation9 Currently, the country has 11 antigens in its immunization schedule (). Despite these achievements, the EPI-SA is faced with significant challenges such as reported outbreaks of vaccine-preventable diseases, including measles and diphtheria in several parts of South Africa,Citation4 as well as concerns around immunization coverage.Citation5,Citation9,Citation13,Citation14 A recent secondary analysis of the 2016 South African Demographic and Health Survey (SADHS) showed that incomplete vaccination was recorded among 40.8% of children eligible for vaccination.Citation15
There are a number of factors associated with low immunization coverage. These may generally be divided into three categories: the health system, users of health services, and health care providers. The shortages and stock-outs of vaccines, especially at the facility level, are a serious challenge faced by the EPI in South Africa and form the crux of this paper. Vaccine shortages have been reported in many parts of the country and became a serious challenge with introducing new vaccines.Citation13,Citation16
South Africa is one of the few countries in Africa that seems to have a routine survey for stock-outs at the service delivery levels since 2013. There is a yearly telephonic survey to measure stock-outs in primary healthcare facilities, which is conducted by Stop Stock-out Project (SSP). In 2015 the SSP reported that stock-outs ranged from as low as 4% to 13% (). This routine survey revealed that stock-out rates could vary significantly between regions in a country, which is an important finding for health managers and policymakers. In 2019, a study in the Eastern Cape province of South Africa showed that 77% of facilities had a stock-out of at least one vaccine,Citation20 which is higher than the figures reported by the SSP while a similar study conducted in 2013 in Gauteng province in South Africa reported a 29% stock-out rate.Citation13 Furthermore, almost all the vaccines in the immunization schedule have been affected by stock-outs. For example, the Eastern Cape study in 2019 found that BCG, rotavirus, and measles vaccines were the vaccines most affected by stock-outs. In Tshwane District under Gauteng province, the hexavalent BCG and OPV were the most affected by stock-outs in 2013.Citation13
Furthermore, it has been reported that vaccine stock-outs occur regardless of whether a health facility has a pharmacist or pharmacist’s assistants, implying that other factors could be at play.Citation20 With these high rates of stock-outs, the department of health’s emphasis on “Every day is an Immunisation Day”Citation8 may not be achieved as some patients may be turned away due to lack of vaccines at the health facilities. Therefore, reports of vaccine stock-outs must be taken seriously, no matter how short the duration may be.
Causes of vaccine stock-outs at the health facility level in South Africa
Evidence from studies conducted in South Africa has shown that vaccine stock-outs in health facilities are mostly linked to poor stock management.Citation13,Citation21 Vaccine stock management is a critical aspect of the supply chain. It helps maintain complete and accurate records of vaccine stock transactions, vaccines’ condition and ensure continuous availability of vaccines to the target population.Citation13,Citation22,Citation23 Vaccine stock management at the health facility level involves activities that are expected to be performed daily. This procedure includes: checking and monitoring vaccines upon arrival at the facility; storage of vaccines in the vaccine fridge according to the temperature sensitivity of a specific vaccine, checking and recording fridge temperature readings twice daily; checking and ensuring the corresponding matching doses of diluents where applicable; recording stock issued for immunization sessions and stock borrowed by other facilities where applicable and ensuring checking stock balance against the minimum stock levels. Physical stock counts should be carried out as often as stated in the policy to validate stock records.Citation24,Citation25 Poor stock management implies the inability to manage stock adequately. This is said to occur when there is a failure to place orders on time, poor forecasting of stock needs, overstocking, and also poor cold chain maintenance.
Other factors that are associated with vaccine stock-outs in health facilities in South Africa include challenges at higher levels, such as delays in stock delivery from the pharmaceutical depot, coupled with poor communication between the depot and the facilities.Citation13,Citation20 Such delays could be due to the geographic location of health facilities. For example, a study in Mozambique showed that facilities farther away from the supply depot might experience more stock-outs than those closer to the depots.Citation26 The geographic location may also influence the health workers employed at the facilities; health workers are generally more motivated to work in urban rather than rural areasCitation20 Additionally, human resource factors, such as staff shortages and lack of skilled personnel,Citation21 could lead to vaccine stock-outs. Furthermore, electronic tools that may have been introduced too fast may have left behind the understanding or acceptance by health workers.
Interventions available to mitigate vaccine stock-outs in primary healthcare facilities in South Africa
Understanding the challenges and constraints of supply chain systems is essential for developing interventions targeting the specific challenges to improve this system’s performance.Citation27 Interventions that can increase vaccine availability at the facility level include addressing challenges at all levels of the cold chain, including the district and provincial depot level and facility level. These interventions include clearing back orders at the depot; ensuring regular and timely delivery of vaccine stocks at facilities; notifying facilities timely in case of delays in deliveries or when there are expected; providing clear guidelines to facilities and officials responsible for stock management; visits by the district or sub-district managers to the health facilities; effective supportive supervision and refresher training for health workers in the facilities and their managers.
Use of electronic stock management systems in primary health care settings
Over and above the abovementioned interventions, digital technology should be considered. The rapid global expansion of digital technology provides an opportunity for mitigating the challenges of commodity distribution and stock-outs.Citation2 This might be an excellent opportunity for the feasibility of stock cards to be investigated and possibly, replaced with electronic stock management systems in primary health facilities. Such systems should integrate both stock monitoring and recording, stock reporting, and possibly, immunization coverage. A scoping review has shown that digital devices such as computers, mobile devices, and digital screens designed to improve the quality of vaccine records and stock visibility are commonly used in low and middle-income countries.Citation28 These interventions have led to increased vaccine availability, improved accuracy of records, and reduced response times. Some of the interventions highlighted in this review can be applied to the South African context. For example, electronic reminders for the managers who receive reports on stock levels may trigger a response.
South Africa has started using digital systems with the Stock Visibility Solution (SVS), which aims to ensure the continuous availability of essential drugs at facilities. The SVS involves using a mobile application designed to enable health facilities to monitor and capture stock levels daily. This system is designed such that managers up the supply chain can have access to the stock levels when reports are sent to them.Citation29 When the stock levels from a facility are uploaded from a health facility, all managers and coordinators who access the system receive this information in real-time. These reports are usually sent weekly. This is expected to prompt the managers to respond to any facility with shortages, enabling the health workers to replenish stock proactively.Citation16
In most cases, it is sub-district managers or other persons responsible for overseeing facilities within their region that respond.Citation30,Citation31 When the managers receive the reports, they are supposed to call facilities with low stock levels to confirm whether the item has been ordered from the depot. The manager can also attempt to source the item from other facilities where it is in stock. This stock redistribution ensures that medicines are always available in the facilities, and patients are not turned away due to stock-outs. However, a recent study on the experiences with and perceptions of the Stock Visibility Solution (SVS) by health care workers has revealed potential barriers to the efficient use of this system.Citation29 These include a lack of response from managers, and the perceived extra workload by some HCWs, coupled with staff shortages. A situation where there is no higher level of managers and coordinators’ supervision leads to a state where there is no sense of responsibility and no sense of accountability. Therefore, it is evident that having a device that reports shortages to a higher level is not enough if managers do not take the responsibility to act on the reports and are not held accountable for the outcomes of their actions. Holding managers accountable for their actions and the results thereof are critical. Failure to respond to essential stock shortages in health facilities has a serious impact on children and caregivers being turned away because of vaccine-stock shortages.
Implementation of interventions must be closely monitored by monitoring the intervention measures themselves and the expected outcomes. These interventions can reduce the magnitude and frequency of stock-outs, improve the accuracy of records, enhance responses from managers, and improve the efficiency of the supply chain.
Interventions targeted at human resources
Human resources form the backbone of every supply chain. They are of great value considering the current complex operating environment and the increasing strain caused by new vaccines and expanding immunization programmes.Citation32 Therefore, skilled, accountable, motivated, and empowered personnel at all health system levels are needed to drive the interventions to strengthen the supply chain to ensure sustainability.Citation32 Therefore, the following interventions for human resources are recommended:
Training and supervision of healthcare workers
Most primary health care facilities, especially those in rural areas, are operated by health workers who may not have undergone formal training in vaccine stock management. A key leveler for change is to ensure that persons with the right skills and attitude are involved in vaccine management.Citation33 Therefore, these HCWs need to be trained and retrained at intervals on managing pharmaceuticals and vaccines. Such training should include specific qualities and requirements of vaccines, forecasting, cold chain management, and wastage. Besides, managers may also benefit from such trainings.Citation34 Studies conducted in different countries, including India, Nigeria, Benin, and Mozambique, have shown that these training led to improved supply chain performance and increased availability of vaccines.Citation35–38
In addition to training, the managers should always supervise and support health workers involved in stock management, to ensure that they follow standard stock management guidelines and respond when reports indicate vaccine shortages. Sub-district programme managers and supervisors should conduct regular visits to facilities and act on the challenges they find.
Performance appraisal and holding managers and responsible officials accountable
Having ensured that health workers are adequately trained and have the necessary competency to manage vaccine stock and other essential medicines, the next step is to ensure that HCWs and their managers deliver on their roles as expected and held responsible for their actions. The systems should include supportive supervision for facilities and ensuring that facilities appreciate the magnitude of the challenge of vaccine stock-outs and promptly communicate and report challenges with vaccine stock. Supervision should also cover the use of SVS.
Human resources standards for pharmacy personnel concerning the staffing of health facilities allocation should be established. If possible, more pharmacist’s assistants should be dedicated entirely to pharmaceuticals management, and the nurses, for example, can focus on their primary duties in the facilities.
A system redesign approach
To address the challenges of vaccine stock out, ensure a highly effective supply chain that delivers a continuous, uninterrupted supply of vaccines at all levels, up to the service delivery level, there is a need to understand what the challenges are and where the weaknesses in the supply chain are. The need for an overhaul and restructuring of the stock management and information system in South Africa has been recommended to ensure the uninterrupted availability of vaccines at service delivery points.Citation13 A system redesign is an approach that can be used to achieve this process of restructuring through a framework that can be used to analyze, design, and implement solutions.Citation39
A system redesign approach offers a blueprint that can improve any vaccine supply chain system component, including programme requirements, distribution, warehousing and storage, human resources, equipment, stock management, monitoring, planning, and information.Citation28,Citation39 This approach also helps determine how different components in the supply chain influence each other and how changes in a particular component can affect the overall performance of the immunization supply chain.Citation40 It also provides managers and decision-makers with the evidence and confidence required to improve the supply chain’s performance.Citation39
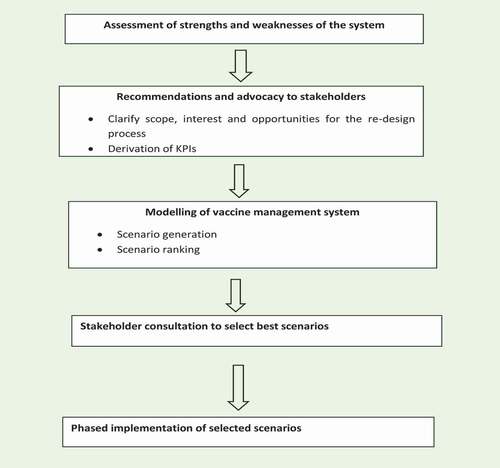
A typical system redesign approach is comprised of several steps.Citation39,Citation41,Citation42 Firstly, an assessment will be conducted to determine whether vaccine management practices are up to expected standards and diagnose overall strengths and weaknesses in the vaccine supply chain. This is then followed by recommendations and advocacy to stakeholders to clarify scope, interest, and opportunities. The primary stakeholders that will be considered in addressing the issue include the immunization managers at national, provincial, district, and facility levels, and HCWs involved in vaccine management. A strategic group-decision is then held with stakeholders to derive key performance indicators (KPIs) such as barriers, facilitators, and thresholds for the improvement options. This is followed by modeling the vaccine management system and scenario generation using various improvement and redesign options. This involves developing a simulation model of the vaccine supply chain, which could serve as a “virtual laboratory” to test the effects of different changes and filtering out the most promising redesign and improvement options. All the likely scenarios are assessed based on the KPIs outlined in the second step. Subsequently, the scenarios are ranked into a set of ‘best-in-class’ scenarios and a set of minor scenarios. The best scenarios are selected after stakeholder consultation, and phased implementation of the selected scenario is done using a targeted phased approach. The project can then be evaluated, and a decision on how to expand the implementation is made. The scenario is a living model that will be reassessed and optimized when a new set of questions arises.Citation39,Citation41,Citation42 shows a schematic diagram of a system redesign process.
The system redesign approach has been used in many developing countries, including African countries. For example, Benin and Mozambique used this approach to reduce the multi-tiered distribution systems to more streamlined and more uncomplicated systems to improve efficiency in distributing vaccines. This change addressed constraints with storage capacity and transportation delays and led to increased cost savings, vaccine availability, and improved services.Citation41,Citation43 In Nigeria, the system design was used to address storage capacity issues in the supplying stores, leading to increased vaccine availability.Citation39 In Ethiopia, this approach was used to improve the distribution practices, leading to a more efficient supply of vaccines at service delivery points.Citation39
Conclusion
South Africa needs an uninterrupted supply of vaccines at different supply chain levels, especially at the lowest level. If the EPI is to reach the immunization coverage targets set and the universal health coverage goal is to be achieved. Vaccine stock-outs are a serious challenge that should be addressed urgently. Interventions such as the SVS face some challenges in implementation and by themselves have a limited role because the causes of vaccine stock-outs are multifactorial and linked to broader systems challenges. We propose a system redesign approach to address the challenges of vaccine stock-outs and other essential medicines.
Additional information
Funding
References
- Bigdeli M, Peters DH, Wagner AK. Medicines in health systems: advancing access, affordability and appropriate use [Internet]. 2014 [accessed 2019 Feb 13]. www.who.int .
- World Health Organisation (WHO). WHO guideline: recommendations on digital interventions for health system strengthening. Geneva. [Internet]. Licence CC BY-NC-SA 3.0 IGO2019 [ accessed 2019 May 9]. https://apps.who.int/iris/bitstream/handle/10665/311941/9789241550505-eng.pdf?ua=1 .
- United Nations. Sustainable development goals [Internet]. 2010 [accessed 2020 Dec 2];1–7. https://www.un.org/sustainabledevelopment/health/ .
- Burnett RJ, Mmoledi G, Ngcobo NJ, Dochez C, Seheri LM, Mphahlele JM. Impact of vaccine stock-outs on infant vaccination coverage : a hospital-based survey from South Africa. Int Health. 2018;1–6. doi:10.1093/inthealth/ihx046.
- Le Roux K, Akin-Olugbade O, Katzen LS, Laurenzi C, Mercer N, Tomlinson M, Rotheram-Borus MJ. Immunisation coverage in the rural Eastern Cape - Are we getting the basics of primary care right? Results from a longitudinal prospective cohort study. South African Med J. 2017;107:52–55. doi:10.7196/SAMJ.2017.v107i1.11242.
- Mothiba TM, Tladi FM. Challenges faced by professional nurses when implementing the expanded programme on immunisation at rural clinics in Capricorn District, Limpopo. African J Prim Heal Care Fam Med [Internet]. 2016 [accessed 2020 Aug 3];8:a923–2928.
- SAGE. Pre-empting and responding to vaccine supply shortages. SAGE April 2016 Executive summary [Internet]. 2016 [accessed 2018 Feb 22]. http://www.who.int/immunization/sage/meetings/2016/april/1_Mariat_shortages_SAGE_2016.pdf .
- World Health Organisation (WHO). Addressing the global shortage of medicines and vaccines Report by the Secretariat [Internet]. [accessed 2018 Mar 6]. http://apps.who.int/gb/ebwha/pdf_files/EB140/B140_19-en.pdf .
- Wiysonge CS, Ngcobo NJ, Jeena PM, Madhi SA, Schoub BD, Hawkridge A, Shey MS, Hussey GD. Advances in childhood immunisation in South Africa: where to now? Programme managers’ views and evidence from systematic reviews. BMC Public Health [Internet]. 2012;12:578. http://www.ncbi.nlm.nih.gov/pubmed/22849711 .
- Ngcobo NJ. The impact of the immunisation programme on vaccine-preventable diseases in South Africa: a review of progress over a 10- to 15-year period. South African J Epidemiol Infect. 2008;23:9–13. doi:10.1080/10158782.2008.11441292.
- Massyn N, Barron P, Day C, Ndlovu N, Padarath A. District Health Barometer 2018/19 [Internet]. Durban Heal Syst Trust. 2020 [accessed 2020 Aug 3];19. https://www.hst.org.za/publications/DistrictHealthBarometers/District+Health+Barometer+2018-19+Web.pdf .
- Von Gottberg A, De Gouveia L, Tempia S, Quan V, Meiring S, Von Mollendorf C, Madhi SA, Zell ER, Verani JR, O’Brien KL, et al. Effects of vaccination on invasive pneumococcal disease in South Africa. N Engl J Med. [Internet] 2014;371:1889–99. doi:10.1056/NEJMoa1401914.
- Ngcobo NJ, Kamupira MG. The status of vaccine availability and associated factors in Tshwane government clinics. South African Med J. 2017;107:535. doi:10.7196/SAMJ.2017.v107i6.12149.
- Burnett RJ, Mmoledi G, Ngcobo NJ, Dochez C, Seheri LM, Mphahlele MJ. Impact of vaccine stock-outs on infant vaccination coverage: a hospital-based survey from South Africa. Int Health [Internet]. 2018;10:376–81. https://www.scopus.com/inward/record.uri?eid=2-s2.0-85051785250&doi=10.1093%2Finthealth%2Fihy036&partnerID=40&md5=5e4620d8cf0e2a70a377953514e75ead .
- Ndwandwe D, Nnaji CA, Mashunye T, Uthman OA, Wiysonge CS. Incomplete vaccination and associated factors among children aged 12–23 months in South Africa: an analysis of the South African demographic and health survey 2016. Hum Vaccin Immunother [Internet]. 2020. doi:10.1080/21645515.2020.1791509.
- Médecins Sans Frontières (MSF), the Rural Doctors Association of Southern Africa (RuDASA), the Rural Health Advocacy Project (RHAP), the Treatment Action Campaign (TAC) S and the SAHCS. Stop Stockouts Project (SSP) Stockouts National Survey [Internet]. Stop Stock Proj Stock Natl Surv. 2016. http://www.groundup.org.za/media/uploads/documents/StopStockoutsSurvey2016.pdf .
- Médecins Sans Frontières (MSF), the Rural Doctors Association of Southern Africa (RuDASA), the Rural Health Advocacy Project (RHAP), the Treatment Action Campaign (TAC) S and the SAHCS. Stock Outs in South Africa - A National Crisis [Internet]. 2013 [accessed 2019 Jun 1]. https://stockouts.org/Download/stop_stockouts_report_2013pdf_1.pdf .
- Médecins Sans Frontières (MSF), the Rural Doctors Association of Southern Africa (RuDASA), the Rural Health Advocacy Project (RHAP), the Treatment Action Campaign (TAC) S and the SAHCS. Stock outs in South Africa. Second Annual Report. 2014 Stock Outs Survey [Internet]. Stop Stock Proj Stock Natl Surv. 2015 [accessed 2019 Jun 1]. https://stockouts.org/Download/stockouts_2014_final_online.pdf .
- Médecins Sans Frontières (MSF), the Rural Doctors Association of Southern Africa (RuDASA), the Rural Health Advocacy Project (RHAP), the Treatment Action Campaign (TAC) S and the SAHCS. 2015 Stock Outs National Survey Third Annual Report – south Africa [Internet]. Stop Stock Proj Stock Natl Surv. 2016 Aug [accessed 2018 Dec 12]. https://stockouts.org/Download/2015_stock_outs_national_survey.pdf .
- Iwu CJ, Ngcobo N, Mccaul M, Mangqalaza H, Magwaca A, Chikte U, Wiysonge CS. Vaccine stock management in primary health care facilities in OR Tambo District, Eastern Cape, South Africa. Vaccine [Internet]. 2020;38:4111–18. doi:10.1016/j.vaccine.2020.04.019.
- Iwu CJ, Ngcobo N, Jaca A, Wiyeh A, Pienaar E, Chikte U, Wiysonge CS. A systematic review of vaccine availability at the national, district, and health facility level in the WHO African Region. Expert Rev Vaccines [Internet]. 2020 [accessed 2020 Aug 1]. https://www.tandfonline.com/doi/abs/10.1080/14760584.2020.1791088 .
- Hasselback L, Dicko M, Viadro C, Ndour S, Ndao O, Wesson J. Understanding and addressing contraceptive stockouts to increase family planning access and uptake in Senegal. BMC Health Serv Res [Internet]. 2017 [accessed 2018 Mar 6];17. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5446687/pdf/12913_2017_Article_2316.pdf .
- Kagashe GA, Massawe T. Medicine stock out and inventory management problems in public hospitals in Tanzanua: a case of Dar es Salaal region hospitals. Int J Pharm [Internet]. 2012 [accessed 2019 Jul 1];2:252–59. http://www.pharmascholars.com .
- Asfar A, Kartlogu U. Vaccine stock management: guidelines on stock records for immunization programme and vaccine store managers [Internet]. 2006. http://apps.who.int/iris/handle/10665/69629 .
- WHO Immunization Practices Advisory Committee. Immunization Supply Chain and Logistics: a neglected but essential system for national immunization programmes [Internet]. In: SAGE Meeting of April 2014. 2014 [accessed 2018 Mar 23]; 1–19. http://apps.who.int/iris/bitstream/handle/10665/131568/WHO_IVB_14.05_eng.pdf?sequence=1 .
- Hasselback L, Crawford J, Chaluco T, Rajagopal S, Prosser W, Watson N. Rapid diagnostic test supply chain and consumption study in Cabo Delgado, Mozambique: estimating stock shortages and identifying drivers of stock-outs. Malar J. 2014;13:1–10. doi:10.1186/1475-2875-13-295.
- Yadav P. Health product supply chains in developing countries: diagnosis of the root causes of underperformance and an agenda for reform. Heal Syst Reform. 2015;1:142–54. doi:10.4161/23288604.2014.968005.
- Iwu CJ, Jaca A, Abdullahi LH, Ngcobo NJ, Wiysonge CS. A scoping review of interventions for vaccine stock management in primary health-care facilities. Hum Vaccines Immunother. 2019;15:2666–72. doi:10.1080/21645515.2019.1607130.
- Iwu CJ, Ngcobo N, Cooper S, Mathebula L, Mangqalaza H, Magwaca A, Chikte U, Wiysonge CS. Mobile reporting of vaccine stock-levels in primary health care facilities in the Eastern Cape Province of South Africa: perceptions and experiences of health care workers. Hum Vaccin Immunother [Internet]. 2020;1–7. doi:10.1080/21645515.2019.1700713.
- Mandimika N Enhancing medicine availability through innovation. The stock visibility system. In: The health systems trust conference [Internet]. 2016 [accessed 2019 May 21]. https://www.hst.org.za/hstconference/hstconference2016/Presentations/svs_hst_conference_20160503.pdf .
- Polity. Aaron Motsoaledi Address by Minister of Health, o. DoH Aaron Motsoaledi Address by Minist. Heal. Occas. Stock Visibility Syst. Improv. access Availab. Essent. Med. Midrand: South Africa launch; 2016
- Kasonde M, Steele P. The people factor: an analysis of the human resources landscape for immunization supply chain management. Vaccine. 2017;35:2134–40. [Internet]. doi:10.1016/j.vaccine.2017.01.084.
- Brown AN, Prosser W, Zwinkels D. Who is preparing the next generation of immunization supply chain professionals? Vaccine. 2017;35:2229–32. doi:10.1016/j.vaccine.2016.12.076.
- Rao R, Schreiber B, Lee BY. Immunization supply chains: why they matter and how they are changing. Vaccine [Internet]. 2017;35:2103–04. http://linkinghub.elsevier.com/retrieve/pii/S0264410X1730275X .
- Guillermet E, Alfa DA, Gbodja R, Jaillard P. Professional changes induced by a redesigned immunization supply chain in the Com?? Health Zone, Benin. Vaccine [Internet]. 2017;35:2189–94. doi:10.1016/j.vaccine.2016.12.074.
- Aina M, Igbokwe U, Jegede L, Fagge R, Thompson A, Mahmoud N. Preliminary results from direct-to-facility vaccine deliveries in Kano, Nigeria. Vaccine [Internet]. 2017;35:2175–82. doi:10.1016/j.vaccine.2016.11.100.
- Prosser W, Jaillard P, Assy E, Brown ST, Matsinhe G, Dekoun M, Lee BY. System redesign of the immunization supply chain: experiences from Benin and Mozambique. Vaccine. 2017;35:2162–66. doi:10.1016/j.vaccine.2016.09.073.
- Gilbert SS, Thakare N, Ramanujapuram A, Akkihal A. Assessing stability and performance of a digitally enabled supply chain: retrospective of a pilot in Uttar Pradesh, India. Vaccine [Internet]. 2017;35:2203–08. doi:10.1016/j.vaccine.2016.11.101.
- World health organisation (WHO). System design approach to improve the immunization supply chain [Internet]. WHO/IVB/18.012018. [ accessed 2020 Jul 28]. https://apps.who.int/iris/bitstream/handle/10665/272853/WHO-IVB-18.01-eng.pdf?ua=1 .
- Chen SI, Norman BA, Rajgopal J, Assi TM, Lee BY, Brown ST. A planning model for the WHO-EPI vaccine distribution network in developing countries. IIE Trans (Institute Ind Eng). 2014;46:853–65.
- Brown ST, Schreiber B, Cakouros BE, Wateska AR, Dicko HM, Connor DL, Jaillard P, Mvundura M, Norman BA, Levin C, et al. The benefits of redesigning Benin’s vaccine supply chain. Vaccine [Internet]. 2014;32:4097–103. doi:10.1016/j.vaccine.2014.04.090.
- Decouttere C, Vandaele N, Lemmens S, Bernuzzi M. The vaccine supply chain multathlon: the reconciliation of technology, economy and access to medicines [Internet]. Springer; 2016. doi:10.1007/978-3-319-24418-1.
- Lee BY, Haidari LA, Prosser W, Connor DL, Bechtel R, Dipuve A, Kassim H, Khanlawia B, Brown ST. Re-designing the Mozambique vaccine supply chain to improve access to vaccines. Vaccine [Internet]. 2016 [accessed 2018 Aug 29]; 34:4998–5004. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5547748/pdf/nihms886969.pdf .
Appendix A.
Table A1. The current EPI schedule in South Africa.Citation11
Figure A1. The proportion of facilities reporting stock-outs of all South Africa’s EPI vaccines across the nine provinces in South Africa, between 2013–2015 (Source: STOP STOCK OUTS PROJECTCitation17–19).
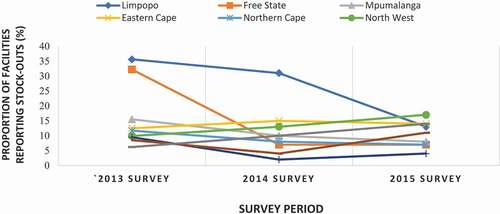
Figure A2. A schematic diagram of a system redesign process.Citation39,Citation41,Citation42