
ABSTRACT
The availability of safe and effective vaccines is a major breakthrough in controlling the COVID-19 pandemic. However, the success of the COVID-19 vaccination campaign relies on high uptake by the public. We monitored Quebecers’ attitudes and intention toward COVID-19 vaccination during the first and second waves of the pandemic. Since March 2020, online surveys are conducted every week in Quebec (Canada) to assess Quebecers’ adherence to recommended public health measures (3,300 respondents are surveyed every week through an online panel; respondents are not invited to answer the survey for 21 days after responding). Ten items measured respondents’ attitudes and intentions regarding COVID-19 vaccination. Logistic regression models were used to identify determinants of intention to be vaccinated against COVID-19. Intention to be vaccinated against COVID-19 ranged from 76%-66% between the first and second waves. The proportion of undecided adults remained stable (12%). Being a man; being 60 years of age and over; having a university education level; having or living with someone with chronic medical conditions and increased risk perceptions of COVID-19 were the strongest predictors of COVID-19 vaccine acceptance in multivariate analysis. During data collection, COVID-19 vaccine supply was very limited. It was reassuring to note that intention to be vaccinated is the highest among older age groups that are prioritized to be vaccinated first. As more doses and vaccines will be available it will be important to enhance vaccine acceptance and uptake, especially among adults younger than 60 years of age and Quebecers with lower risk perceptions of COVID-19.
Background
The availability of safe and effective vaccines is a huge progress to control the spread of SARS-CoV-2. Three vaccines are already approved for use in Canada and others are expected to be available in the near future.Citation1 In addition to equitable distribution of vaccines, to be successful in stopping the pandemic, high uptake of COVID-19 vaccines among the public will be needed.Citation2 In 2019, prior to the pandemic, the World Health Organization identified vaccine hesitancy – or delay in acceptance or refusal of vaccination despite availability of vaccination services,Citation3 as a major threat to global health.Citation4 For example, a survey of the likelihood of vaccine acceptance conducted in June 2020 in 19 countries indicated that 72% of the 13,426 participants were very or somewhat likely to receive a COVID-19 vaccine and it was 69% among Canadian respondents.Citation5 A recent survey among French-speaking nurses and general practitioners showed that 71% of these health professionals were willing to be vaccinated against COVID-19. However, these surveys also showed that up to one-quarter would not or are unsure about COVID-19 vaccination. This level of hesitation should not come as a surprise as it is similar to the proportion of those who hesitate for routine vaccines in high-income countries (HICs)Citation6 or of other surveys conducted among health care providers.Citation7
Quebec was the Canadian province with the highest incidence of COVID-19 in the first and second waves. Among its population of approximately 8,5 million Quebecers, a total of 57,041 COVID-19 cases and 9,883 deaths were reported in January 2021.Citation8 It is estimated that ~70-80% COVID-19 vaccine uptake is needed to generate community immunity (a question still under debate).Citation9 To reach community immunity against COVID-19, it will be crucial to address barriers to vaccine acceptance. A first and important step to do so is to have a good understanding of the sub-groups that are less likely to accept to be vaccinated. In this article, we report data on intention to be vaccinated against COVID-19 among representative samples of Quebec adults (18 years and older) collected in multiple surveys conducted during the first and second waves of the pandemic. We assessed sociodemographic and attitudinal determinants of positive intention to vaccinate.
Methods
Ethics approval
The surveys are conducted as part of a multicomponent plan to evaluate public health intervention to prevent COVID-19. The Ethics Review Board of the Center de recherche du CHU de Québec – Université Laval provided a waiver for the requirement for research ethics approval for this study (waiver 2021–5714). The specialized research firm is responsible of the informed consent process and data protection of voluntary participants. The research team receives anonymous data for analysis.
Design and recruitment
A series of cross-sectional surveys are ongoing in Quebec since March 2020 in order to assess Quebecers’ attitudes and behaviors during the pandemic.Citation10 The sample allocation was initially proportional to the population size of Quebec 16 health areas but over-sampling was necessary to produce reliable estimates for some of the larger regions. To meet these requirements, since July 2020, a representative sample of 3,330 Quebec respondents is recruited each week using a web panel with response rates around 10%. Invitation to participate are sent via e-mails. Adults 18 years of age and older able to answer the survey in the two Quebec official languages (French and English) are eligible to participate. There are no exclusion criteria. The survey is conducted by a specialized research firm with high-quality standards.Citation11 The firm is responsible of the recruitment process, the survey administration, and to ensure quality (e.g., preventing multiple entries from the same individual, removing careless responses). After having completed the questionnaire, respondents do not receive further invitation within the next 21 days. As all responses are anonymous, no information on respondents that could have completed the questionnaire at multiple time points is available.
Questionnaire
In addition to sociodemographic questions (i.e., age, gender, level of education, household composition, and employment), the questionnaire contains approximately 60 questions to examine Quebecers’ perceptions of COVID-19 risks, attitudes, beliefs and knowledge about the pandemic and the preventive measures (including adherence to conspiracy theories inspired by the Generic Conspiracist Beliefs scale developed by Bruder and collaboratorsCitation12) as well as behaviors regarding recommended measures. Some survey items are based on validated scales (ex.: mental health indicators) while others have been adapted from other surveys (ex.: perceptions of risks associated with COVID-19) or have been created by developed by the research team that includes behavioral science experts and professionals from Quebec Ministry of Health (ex.: Knowledge, beliefs and attitudes regarding preventive measures). The questionnaire is adjusted frequently based on changes in public health recommendations and COVID-19 epidemiology in the province. Items included in the analysis are detailed in Appendix 1.
Postal codes are also collected which allowed to identify respondents’ areas of residence (census metropolitan areas, cities >10,000 inhabitants, small cities and rural areas). Postal codes are also used to attribute Material Deprivation Index (MDI). MDI is declined in quintiles of population based on factor scores from indicators of Canadian Census data that reflects the deprivation of goods and conveniences based on average personal income; unemployment rate; and high school education rate in a specific geographic area.Citation13 The first quintile (Q1) indicates the best status (20% more privileged population), while the last quintile (Q5) refers to the worst status (20% more deprived population).
Impact of the pandemic on psychological well-being is also measure using Kessler’ psychological distress scale (K6)Citation14 and Keyes’ emotional well-beingCitation15 (findings of the surveys on mental health are described elsewhere).Citation16
In April–May, in September and in November–December 2020, 10 items assessed respondents’ attitudes and intention regarding COVID-19 vaccines. Two open-ended questions assessed respondents’ perceptions of the advantages and disadvantages of COVID-19 vaccination. All other questions were close-ended, and responses were recorded on a 5-point Likert scale (‘Completely Agree,’ ‘Somewhat Agree,’ ‘Somewhat Disagree,’ ‘Completely Disagree,’ ‘Don’t know’). One question measured acceptance of COVID-19 vaccines (I intend to get the vaccine against COVID-19 once available). The survey questions on vaccination were informed by our previous work.Citation6,Citation17
The research firm is responsible of programming and testing the online survey. Items in the questionnaire are randomized to prevent biases. To reduce number and complexity of the questions, an adaptive questioning is used (certain items, or only conditionally displayed based on responses to other items). A completeness check and a review step are possible for participants.
Statistical analysis
Data were weighted according to some sociodemographic characteristics (age, gender, location, language, education, household composition) to be representative of Quebec’s population.
Descriptive statistics were generated for all items of completed questionnaires. Open-ended questions were analyzed thematically in Microsoft Excel. Coding schemes were developed by MD based on the respondents’ comments and were discussed and refined among the research team.
Since the risk perception variables associated with COVID-19 (listed in Appendix 1) are highly correlated, we used multidimensional and clustering techniques to create an overall risk perception score. Three clusters have been created: respondents having high perceived risks of COVID-19, respondents with moderate risk perceptions and respondents having low perceived risks for COVID-19.
Finally, statistical models based on univariate and multivariate logistic regressions were performed with intention to vaccinate as the dependent variable for the period from November 27 to December 9. In addition to sociodemographic characteristics, independent variables that were tested are listed in Appendix 1. All analyses were performed using SAS version 9.4 and the threshold of statistical tests was α = 5%.
Results
Intention to be vaccinated against COVID-19 ranged from 76% to 66% between April and December 2020 (). The proportion of undecided adults remained stable at around 12%.
Figure 1. COVID-19 vaccine intentions among the general public and among health care workers, data collected between April 23 to December 9, 2020.
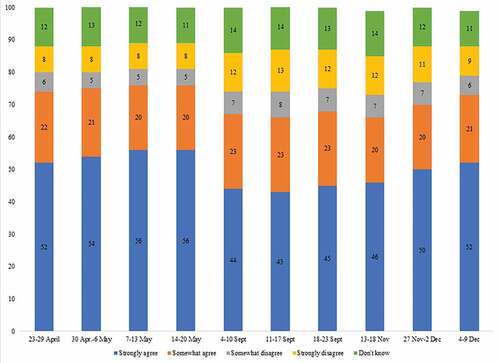
Intention to be vaccinated against COVID-19 increased with age and level of education (). Men, adults having chronic medical conditions (CMCs) or who lived with someone with CMCs had higher intention while vaccine intention was lower among those living in more deprived areas. There were no significant differences in vaccine intention between adults who answered the questionnaire in French or in English and between areas of residence. Vaccine intention does not differ when comparing respondents who were healthcare workers (HCWs) and those aged 18–64 years who were not (65% in HCWs vs 67% for others, data not shown in ).
Table 1. Vaccine intention and sociodemographic characteristics, data collected between November 27 and December 9, 2020
We compared intention to be vaccinated with risk perceptions and adherence to conspiracy theories (). Intention to be vaccinated was higher for those with higher risk perceptions (i.e., risks perception score including perceived risk of catching COVID-19, perceived seriousness of COVID-19, worries about catching or transmitting the virus and fear of losing a loved one due to COVID-19, Appendix 1). In contrast, those who adhere to conspiracy theories had significantly lower intention to be vaccinated against COVID-19 ().
Table 2. Vaccine intention and risk perceptions and adherence to conspiracy theories, data collected between November 27 and December 9, 2020
In surveys conducted between November 27 and December 9, 2020, the main reasons mentioned by those who did not intended to be vaccinated against COVID-19 were: fear of side effects (27%), concerns because it’s a new vaccine (24%), not trusting vaccines in general (24%), concerns regarding vaccine efficacy (8%) and contraindications to vaccination (4%) (data not shown). Fear of side effects remained the most frequent reason for not having the intention to be vaccinated across all data collection time points.
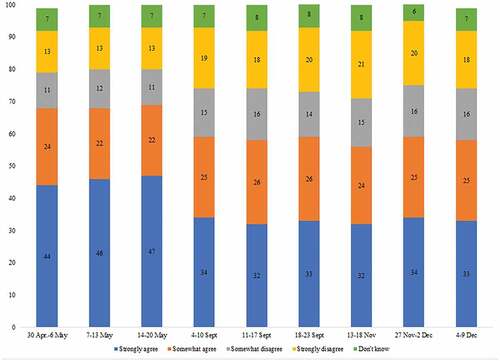
Perceptions regarding mandatory COVID-19 vaccination were also assessed. shows that support for mandatory vaccination decreased over time, with 68% of adults in favor of mandating COVID-19 vaccination in April compared to 59% in December. Similar level of support for mandatory COVID-19 vaccination was found among HCWs and the general public (data not shown in the Figure).
Figure 2. COVID-19 vaccine intentions among the general public and among health care workers, data collected between April 23 to December 9, 2020.
Findings of univariate and multivariate analysis are shown in . Very strong crude (non-adjusted) associations were observed in univariate analysis. However, in multivariate analysis, many of the observed relationships weakened and some even became not statistically significant. Being a man; being 60 years of age and over; having a university education level; having or living with someone with CMCs and increased risk perceptions of COVID-19 remained the strongest predictors of COVID-19 vaccine intention. Respondents who agree with the measures taken by the Quebec government, those who do not believe in conspiracy theories and those with negative emotional well-being were also very likely to intend to receive the COVID-19 vaccine.
Table 3. Determinants of COVID-19 vaccine intention, data collected between November 27 and December 9 2020
These variables are also strong predictors of being in favor of mandatory vaccination (Appendix 2). Male gender, being aged between 18 and 24 years old or 70 years or older, living in the most materially privileged areas, having a CMCs or living with a person with CMCs and high perceived risk of COVID-19 were the strongest predictors of being in favor of mandatory vaccination.
Discussion
COVID-19 vaccination started in mid-December in Quebec. As vaccination was being rolled-out, the number of COVID-19 vaccine doses available in Canada was very limited.Citation18,Citation19 Priority groups for vaccination were established. People living in long-term care facilities and health care workers were among the first groups to be offered vaccination.Citation20 In January 2021, 65% of health care workers, 14% of residents in public long-term care facilities and 6% of those living in private long-term care facilities had received a first dose of COVID-19 vaccine.Citation21 In this context, assessing determinants of vaccine acceptance may not be perceived of utmost importance. Indeed, our findings are reassuring. Approximately three out of four Quebecers intend to be vaccinated. The strongest predictor of COVID-19 vaccination intentions was being aged 60 years or older which is also reassuring as older age groups are prioritized to be vaccinated first.Citation20 A stable proportion of around 12% were unsure about COVID-19 vaccination. As our surveys were conducted before the approval of the first COVID-19 vaccine in Canada, being unsure regarding hypothetical vaccines with unknown safety and efficacy profiles is not unexpected or irrational. However, the fact that 15% had low or no intention to be vaccinated is not negligeable. It is well known that the undecided or slightly hesitant are more receptive to public health messaging and more likely to accept vaccine if their concerns are adequately addressed than those with stronger negative views about vaccines.Citation6,Citation22,Citation23 In the context of growing misinformation,Citation24 vaccine hesitancy can become an important barrier to the future success of the COVID-19 vaccination campaigns.
In our surveys, adherence to conspiracy theories and low risk perceptions regarding COVID-19 were associated with unwillingness to receive a COVID-19 vaccine. Conspiracy theories are defined as ‘explanations for important events that involve secret plots by powerful and malevolent groups.’Citation25 COVID-19 provides an ideal context to develop conspiracy theories, as they tend to arise in societal crisis situations that generate uncertainty.Citation26 Different other studies have also shown that beliefs in conspiracy theories are negatively associated with adoption of preventive measures and vaccination intentions.Citation27–29
The perception of risk has long been studied in the context of adoption of preventive health behaviors, including vaccination.Citation30 Higher risk perceptions is predictive of behaviors when people believe that effective protective actions are available and when they are confident in their self-efficacy.Citation31 In the context of vaccination, this means that if the perceived threat of COVID-19 is high and if vaccines are perceived as an effective, safe and accessible means of protection, intention to vaccinate will be higher. Recent studies also have highlighted that perceived risks of SARS-CoV-2 increase the likelihood of adoption of COVID-19 preventive measures and willingness to receive a future COVID-19 vaccine.Citation32–34
Finally, our surveys showed that a majority of Quebecers are supportive of mandating COVID-19 vaccinations. Although it is unlikely that vaccination will be mandatory until supply are sufficient, these responses highlight positive attitudes toward vaccination.Citation35,Citation36
This study has limitations. Respondents were invited to participate from a web panel in a short time. Response rates were then considered low and may lead to non-representative samples of the population in this non-probabilistic samples. Moreover, although the web panel we used is the largest in Canada,Citation11 there is also a global risk of lower representation of some groups (newcomers, people who have no Internet access or who do not read French or English). We cannot exclude a participation bias, with those more interest in the topic being more likely to respond to our questionnaire. The weighting process makes it possible to correct the samples but this does not correct all these representativeness biases. Finally, as with all survey, there is social desirability bias (i.e., respondents who provided answers that are perceived as what will be viewed positively). However, the fact that the questionnaire was anonymous should have reduce this bias.
Conclusion
Many surveys to assess vaccine attitudes among Canadians have been recently published.Citation36–39 Our findings appear to be more positive (i.e., higher proportion of respondents who intend to be vaccinated). In the context of the pandemic, opinions regarding vaccines are highly volatile and influenced by discourse in the mainstream media. The repeated surveys over time using the same items and the large number of respondents (3,330 per week) make us confident that our data are representative of Quebecers’ opinion over time. Of note is the fact that willingness to be vaccinated does not necessarily translate into action. Vaccine uptake is shaped by many different factors, of which access to vaccination services is of paramount importance.Citation40 Our findings could however to develop tailored interventions to enhance vaccine acceptance targeted to groups that are less willing to be vaccinated (i.e., younger adults, those feeling less at risk, those with lower level of education and those living in more deprived areas). The launch of COVID-19 vaccination provides an important opportunity to address vaccine hesitancy in Canada. Beyond providing information about the safety and effectiveness of COVID-19 vaccines, successful strategies will need to be culturally sensitive, tailored and multicomponent (i.e., increase access to vaccination services, address vaccine hesitancy, build support among community leaders and engage healthcare providers).Citation41
Disclosure of potential conflicts of interest
The authors have no conflicts of interest to disclose.
Acknowledgments
The author would like to thank Ms Mélanie Tessier and Mr Louis Rochette for their contribution to the overall project.
Additional information
Funding
Notes on contributors
Ève Dubé
Dr. Ève Dubé is a medical anthropologist at the Institut national de santé publique du Québec. She is also a researcher at the Centre de recherche du CHU de Québec-Université Laval and an Invited Professor in the department of Anthropology at Université Laval. Most of her research focuses on the socio-cultural aspects of vaccination.
Maude Dionne
Maude Dionne is a scientific advisor at the Institut national de santé publique du Québec. She graduated a bachelor’s degree in psychology and a master’s degree in public health from Université Laval. She is interested in vaccination, prevention and health promotion.
Catherine Pelletier
Catherine Pelletier is a research assistant in the Infectious Diseases group at the Centre de recherche du CHU de Québec-Université Laval. She received a bachelor’s degree in microbiology and a master’s degree in public health from Université Laval. She is interested in vaccination, prevention and health promotion.
Denis Hamel
Denis Hamel is a scientific coordinator and statistician at the Institut national de santé publique du Québec since 2000. He graduated a master’s degree in statistics from Université Laval. He is a specialist in survey methodology.
Souleymane Gadio
Souleymane Gadio is a biostatistician scientific advisor at the National Institute of Public Health of Quebec. He evolves in particular as methodological support in the information management, analysis and dissemination unit at the Population Health Information and Studies Office. He received a master’s degree in biostatistics from Université Laval.
References
- National Advisory Committee on Immunization. Recommendations on the use of COVID-19 vaccines. Ottawa, Ontario, Canada: Government of Canada; 2021 [accessed 2021 Mar 18]. https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/recommendations-use-covid-19-vaccines.html#b1.
- Wood S, Schulman K. Beyond politics - promoting Covid-19 vaccination in the United States. N Eng J Med. 2021;384(7):e23. doi:10.1056/NEJMms2033790.
- MacDonald NE. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–64. doi:10.1016/j.vaccine.2015.04.036.
- World Health Organization. Ten threats to global health in 2019. Geneva, Switzerland: World Health Organization; 2019 [accessed 2021 Jan 26]. https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
- Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, Kimball S, El-Mohandes A. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2020;27(2):225–28. doi:10.1038/s41591-020-1124-9.
- Dubé E, Laberge C, Guay M, Bramadat P, Roy R, Bettinger J. Vaccine hesitancy: an overview. Hum Vaccin Immunother. 2013;9(8):1763–73. doi:10.4161/hv.24657.
- Verger P, Fressard L, Collange F, Gautier A, Jestin C, Launay O, Raude J, Pulcini C, Peretti-Watel P. Vaccine hesitancy among general practitioners and its determinants during controversies: a national cross-sectional survey in France. EBioMedicine. 2015;2(8):891–97. doi:10.1016/j.ebiom.2015.06.018.
- Institut national de santé publique du Québec. Données COVID-19 au Québec. Québec, Canada: Institut national de santé publique du Québec; 2021 [accessed 2021 May 26]. https://www.inspq.qc.ca/covid-19/donnees.
- Anderson RM, Vegvari C, Truscott J, Collyer BS. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet. 2020;396(10263):1614–16. doi:10.1016/S0140-6736(20)32318-7.
- Institut national de santé publique du Québec. COVID-19: sondages sur les attitudes et comportements des adultes québécois. Québec, Canada: Institut national de santé publique du Québec; 2020 [accessed 2021 Jan 26]. https://www.inspq.qc.ca/covid-19/sondages-attitudes-comportements-quebecois.
- Leger. Panel book. 2020 [accessed 2021 Feb 26] https://2g2ckk18vixp3neolz4b6605-wpengine.netdna-ssl.com/wp-content/uploads/2020/01/PANEL-BOOK-LEO-EN.pdf.
- Bruder M, Haffke P, Neave N, Nouripanah N, Imhoff R. Measuring individual differences in generic beliefs in conspiracy theories across cultures: conspiracy mentality questionnaire. Front Psychol. 2013;4:225. doi:10.3389/fpsyg.2013.00225.
- Pampalon R, Raymond G. A deprivation index for health and welfare planning in Quebec. Chronic Dis Can. 2000;21:104–13.
- Kessler RC, Green JG, Gruber MJ, Sampson NA, Bromet E, Cuitan M, Furukawa TA, Gureje O, Hinkov H, Hu C-Y, et al. Screening for serious mental illness in the general population with the K6 screening scale: results from the WHO World Mental Health (WMH) survey initiative. Int J Methods Psychiatr Res. 2010;19(S1):4–22. doi:10.1002/mpr.310.
- Keyes CLM. Brief description of the mental health continuum short form (MHC-SF). Atlanta, GA: Emory University; 2009 [accessed 2021 Feb 4]. https://www.aacu.org/sites/default/files/MHC-SFEnglish.pdf.
- Dionne M, Roberge M, Brousseau-Paradis C, Dubé E, Hamel D, Rochette L, et al. COVID-19 - Sondages sur les attitudes et comportements des adultes québécois: pandémie, bien-être émotionnel et santé mentale - 12 janvier 2021. Québec, Canada: Institut national de santé publique du Québec; 2021.
- Dubé E, Gagnon D, Ouakki M, Bettinger JA, Witteman HO, MacDonald S, Fisher W, Saini V, Greyson D. Measuring vaccine acceptance among Canadian parents: a survey of the Canadian immunization research network. Vaccine. 2018;36(4):545–52. doi:10.1016/j.vaccine.2017.12.005.
- Tasker JP. Pfizer to temporarily reduce vaccine deliveries to Canada, minister says. CBC News; 2021 Jan 15 [accessed 2021 Feb 15]. https://www.cbc.ca/news/politics/pfizer-temporarily-reducing-vaccine-deliveries-1.5874645.
- Public Services and Procurement Canada. Statement from the honourable anita anand, minister of public services and procurement, on moderna vaccine delivery. Ottawa, Ontario, Canada: Government of Canada; 2021 Jan 29 [accessed 2021 Feb 15]. https://www.tpsgc-pwgsc.gc.ca/comm/vedette-features/2021-01-29-00-eng.html.
- Comité sur l’immunisation du Québec. Avis préliminaire sur les groupes prioritaires pour la vaccination contre la COVID-19 au Québec. Québec, Canada: Institut national de santé publique du Québec; 2020.
- Institut national de santé publique du Québec. Données de vaccination contre la COVID-19 au Québec. Québec, Canada: Institut national de santé publique du Québec; 2021 [accessed 2021 May 26]. https://www.inspq.qc.ca/covid-19/donnees/vaccination.
- Gagneur A, Lemaître T, Gosselin V, Farrands A, Carrier N, Petit G, Valiquette L, De Wals P. A postpartum vaccination promotion intervention using motivational interviewing techniques improves short-term vaccine coverage: promoVac study. BMC Public Health. 2018;18(1):811. doi:10.1186/s12889-018-5724-y.
- Leask J. Target the fence-sitters. Nature. 2011;473:443–45. doi:10.1038/473443a.
- Burki T. The online anti-vaccine movement in the age of COVID-19. Lancet Digit Health. 2020;2(10):e504–e5. doi:10.1016/S2589-7500(20)30227-2.
- Douglas KM, Sutton RM, Cichocka A. The psychology of conspiracy theories. Curr Dir Psychol. 2017;26(6):538–42. doi:10.1177/0963721417718261.
- van Prooijen J-W, Douglas KM. Conspiracy theories as part of history: the role of societal crisis situations. Mem Stud. 2017;10(3):323–33. doi:10.1177/1750698017701615.
- Freeman D, Waite F, Rosebrock L, Petit A, Causier C, East A, Jenner L, Teale AL, Carr L, Mulhall S, Bold E. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychol Med. 2020;1–13. doi:10.1017/S0033291720001890.
- Marinthe G, Brown G, Delouvée S, Jolley D. Looking out for myself: exploring the relationship between conspiracy mentality, perceived personal risk, and COVID-19 prevention measures. Br J Health Psychol. 2020;25(4):957–80. doi:10.1111/bjhp.12449.
- Romer D, Jamieson KH. Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc Sci Med. 2020 Oct;263:113356. doi:10.1016/j.socscimed.2020.113356.
- Brewer NT, Chapman GB, Gibbons FX, Gerrard M, McCaul KD, Weinstein ND. Meta-analysis of the relationship between risk perception and health behavior: the example of vaccination. Health Psychol. 2007;26(2):136–45. doi:10.1037/0278-6133.26.2.136.
- Brewer NT, Chapman GB, Rothman AJ, Leask J, Kempe A. Increasing vaccination: putting psychological science into action. Psychol Sci Public Interest. 2017;18(3):149–207. doi:10.1177/1529100618760521.
- Karlsson LC, Soveri A, Lewandowsky S, Karlsson L, Karlsson H, Nolvi S, Karukivi M, Lindfelt M, Antfolk J. Fearing the disease or the vaccine: the case of COVID-19. Pers Individ Differ. 2021 Apr;172:110590. doi:10.1016/j.paid.2020.110590.
- Caserotti M, Girardi P, Rubaltelli E, Tasso A, Lotto L, Gavaruzzi T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc Sci Med. 2021 Mar;272:113688. doi:10.1016/j.socscimed.2021.113688.
- Faasse K, Newby J. Public perceptions of COVID-19 in Australia: perceived risk, knowledge, health-protective behaviors, and vaccine intentions. Front Psychol. 2020;11:551004. doi:10.3389/fpsyg.2020.551004.
- Largent EA, Persad G, Sangenito S, Glickman A, Boyle C, Emanuel EJ. US public attitudes toward COVID-19 vaccine mandates. JAMA Netw Open. 2020;3(12):e2033324. doi:10.1001/jamanetworkopen.2020.33324.
- IPSOS. Support for mandatory COVID vaccination in Canada rises to 64%, up points since November. Toronto, Québec, Canada: IPSOS; 2021 [accessed 2021 Feb 16]. https://www.ipsos.com/sites/default/files/ct/news/documents/2021-01/vaccines-factum-2021-01-16-v1.pdf.
- Vaccin contre la COVID-19: hausse importante du nombre d’indécis. Sherbrooke, Québec, Canada: Université de Sherbrooke; 2021 Feb 11 [accessed 2021 Feb 15]. https://www.usherbrooke.ca/actualites/nouvelles/nouvelles-details/article/44574/.
- Angus Reid Institute. Itching for injection: number of Canadians who say they want to be vaccinated ASAP against COVID-19 surges. Vancouver, British Columbia, Canada: Angus Reid Institute; 2021 Jan 11 [accessed 2021 Feb 15]. https://angusreid.org/canada-covid-vaccine-january/.
- Leger. Leger’s North American tracker: February 1st. 2021 [accessed 2021 Feb 15]. https://2g2ckk18vixp3neolz4b6605-wpengine.netdna-ssl.com/wp-content/uploads/2021/02/Legers-North-American-Tracker-February-1st-2021-min.pdf.
- Seale H, Heywood AE, Leask J, Sheel M, Durrheim DN, Bolsewicz K, Kaur R. Examining Australian public perceptions and behaviors towards a future COVID-19 vaccine. BMC Infect Dis. 2021;21(1):120. doi:10.1186/s12879-021-05833-1.
- Thomson A, Vallée-Tourangeau G, Suggs LS. Strategies to increase vaccine acceptance and uptake: from behavioral insights to context-specific, culturally-appropriate, evidence-based communications and interventions. Vaccine. 2018;36(44):6457–58. doi:10.1016/j.vaccine.2018.08.031.
Appendices
Appendix 1.
Theoretical concepts and survey items
Appendix 2
Determinants of supporting mandatory vaccination against COVID-19, Data collected between November 27 and December 9 2020