
ABSTRACT
Several novel efforts have been put forth to make a readily available vaccine against the global pandemic of COVID-19. However, there seems to appear vaccine-taking hesitancy among the general people. Against this backdrop, this current study sets to assess the vaccine-taking intention, ways to overcome the vaccine-taking reluctance among Bangladeshi people and explore their knowledge, perceptions, and attitude toward the COVID-19 vaccine. To this end, this study leveraged on a cross-sectional survey, which was consisted of 1377 respondents covering the eight divisions of Bangladesh. The descriptive statistical method and ordinal logistics regression were employed to explore and rationalize our study outlined objectives. Empirical findings revealed that approximately 71% of the respondents had adequate knowledge about the COVID-19 vaccine, whereas 46% of the respondents were willing to be vaccinated against COVID-19 while the rest of the respondents were hesitant to take the vaccine. However, concern about the potential side effects was one of the core reasons for vaccine-taking hesitancy. Assuring the common people about vaccine safety and efficacy, along with easing the registration procedure, can ameliorate people’s confidence to get vaccinated. Meanwhile, about 60% of the respondents believed that a vaccine could help Bangladesh win the battle against COVID-19 and will allow back to normal life. Although the government has taken some pragmatic action steps to promote the vaccination rate, it is recommended that the mass vaccination program should be extended to the grassroots level with proper extension community support and easing the registration process.
Introduction
Since December 2019, the deadly unprecedented coronavirus (SARS-Cov-2) disease has threatened millions of lives, and still, it continues its rampage all around the globe.Citation1 On 11 March 2020, the World Health Organization (WHO) announced this disease as a pandemic,Citation2,Citation3 as the virus continues to spread from the seafood market of Wuhan, China, to every corner of the earth.Citation4,Citation5 Apart from health threats, the COVID-19 has triggered dire financial and economic distress throughout the globe, including those of the biggest economies (e.g., USA, UK, Germany, China, France, Italy, and Spain).Citation6 However, underdeveloped and developing countries are digesting the worst wound induced by the economic and financial crisis that may lead many vulnerable communities to food shortage.Citation7,Citation8What is more concerning is that the healthcare system in most nations, whether developed, or developing, or underdeveloped, is in grave turmoil due to COVID-19.Citation9 Furthermore, according to a recent study, immune-related pharmaceutical products in the United States have experienced shocks from the economic downturn.Citation10 Thus, it might result in yet another health crisis in many parts of the globe.Citation10 Against the backdrop, as the pandemic moves way further, a potential vaccine can help get rid of the anathema. Scientists underwent magnificent research works to discover the magic to bring us back to a new normal. Breaking all the records in the history of medical science, several potential vaccines have been developed in the quickest possible time phase. So far, 77 vaccines are under active investigation in animal health, among which 8 received approval for use.Citation11 Among them, the vaccine manufactured by BioNTech-Pfizer and Moderna Inc. proved to be 90% or more effective, whereas the vaccine of Oxford-AstraZeneca found 70% effective in terms of generating antibodies against the deadly virus.Citation12–14 Primarily, vaccination programs are targeted at older ones and adults aged over eighteen since no vaccine testing was attempted for anyone around the world under this age. Therefore, until and unless extensive research is undertaken on children and teenagers, it is recommended to keep them away from the inoculation program.Citation15 Apart from this, children and youth are found to be less severely affected by coronavirus than adults and older people.Citation16,Citation17
However, the success of the inoculation program hinges upon the people’s intention and decision to get vaccinated. The low acceptance of available vaccines for high-risk infection has been attributed to a pandemic public health paradox,Citation18 which significantly contributes to vaccine hesitancy. Reportedly, vaccine hesitancy refers to unwillingness or refusal to take a vaccine despite their availability.Citation19 It is worth mentioning that hesitation in getting a vaccine led to a massive outbreak of disease previously,Citation20 since vaccine always remains a dilemma among general people.Citation21
Bangladesh, likewise nations around the globe, is endeavoring to escape the tremor of the pandemic. In doing so, the Bangladesh government decided to import the COVIDSHIELD vaccine, manufactured by the Serum Institute of India using the Oxford-Astrazeneca vaccine patent.Citation22The rationale for choosing this vaccination may be ascribed to the fact that, unlike other leading vaccines, the Oxford-Astrazeneca vaccine is relatively inexpensive and can be stored easily in the refrigerator (2–8 Degree Celsius).Citation23 However, along with COVIDSHIELD, Bangladesh has also started to import others such as the vaccine of Pfizer, Sinopharm, and Moderna in recent times during the second phase of the inoculation program. As the mass inoculation program is making its way on 7 February 2021, tensions arise among general people regarding the vaccine. Also, some perpetrators are squandering their time pervading fabricated information on the vaccine. Under the circumstances, with the vaccination program is in proximity, peoples’ knowledge, attitude, and perception toward the COVID-19 vaccine must be addressed from the socio-economic ground. It will not only help disclose people’s choices toward the vaccine but also provide possible guidelines to improve the mass vaccination program for policymakers.
Over the last months, some studies devoted themselves to explore vaccine acceptability among people in different countries. An investigation led by Peretti-Watel et al.Citation24 revealed that about 4.7% of adults in Australia, 27% of adults in France, and 20% of adults in the USA are likely to defy the vaccine. However, the latest study led by Khubchandani et al.Citation25 unveiled that about 22% of people more or less likely to refuse the vaccine in the USA. Research on vaccine acceptability has also been conducted in the UK, Canada, Denmark, Germany, Italy, Portugal, unveiling the interesting and diversified outcomes.Citation26 Besides, Barello et al.Citation27 found that 13.9% of students refused to take the vaccine in Italy. Meanwhile, Thorneloe et al.Citation28 concluded that younger people are more intend to refuse the vaccine.
Despite being a pressing issue, to our best knowledge, this is one of the first empirical studies that has been conducted to expose the Bangladeshi people’s hesitancy toward the COVID-19 vaccine. However, our study contributes in several ways to the current extant literature on COVID hesitancy. Firstly, the intention to be vaccinated against COVID-19 according to the respondent’s socio-demographic factors is assessed in this study. Secondly, we try to expose people’s knowledge, attitude, and perception toward the COVID-19 vaccine. Thirdly, we intend to analyze the possible reasons that ensue vaccine-taking hesitancy. Lastly, we focus on several courses of action that may ease the vaccine-taking reluctance among sampled area.
Methods
Study design
A cross-sectional survey was enacted between January 31 to February 6, 2021. However, the mass vaccination program of Bangladesh onsets on 7 February. Therefore, to uncover people’s preoccupation regarding the vaccine, we halted our survey the day before the vaccination program commenced. People aged above eighteen and those who agreed to participate in the interview were included as respondents. The study covered respondents from every eight divisions of Bangladesh to portray a more substantiated and countrywide picture in our research. It also helped discover the overall scenario of the country. Our study adopted both web-based data collection and a face-to-face interview. The link created for online data collection was arbitrarily circulated through social media sites (i.e., Facebook, WhatsApp, and Messenger) and shared directly via e-mail with the researcher’s contact list. The personal face-to-face interview was also conducted by maintaining at least 2 m physical distance in some isolated regions of the country where there are no proper internet facilities.
Study tool and data collection
A structured questionnaire was developed and tested in a pilot study through 20 participants. Evaluating the public views from the pilot study, we revised the survey questionnaire and confirmed it with a total of 56 questions. An online survey portal, KoBo Toolbox, was created to expedite the questionnaire formation for online data collection. After that, we briefly specified the research purposes to the respondents, and they were approached for participating in the survey. However, the response rate was approximately 65%. The survey questionnaire was designed both in English and Bangla for the convenience of respondents. The questionnaire had six parts where Part-A represented the socio-demographic profile of the respondents (11 questions), Part-B denoted participant’s vaccine-taking decisions (2 questions), Part-C described the questions about what efforts can be implemented to reduce people’s hesitancy to take the vaccine (8 questions), Part-D contained the knowledge about COVID-19 vaccine (8 questions). Besides, Part-E indicated the respondent’s perception of the available COVID-19 vaccine (17 questions), and Part-F denoted attitude toward the COVID-19 vaccine (10 questions).
Sampling and validation
The sample size was determined following the convenience sampling technique since it is one of the most prevalent non-probability sampling techniques.Citation29,Citation30 The sample size estimation was based on the presumption that the probability of having adequate knowledge, perceptions, and positive attitude toward the coronavirus vaccine was 50.0%, with a 95% confidence interval and 5% margin of error. Based on the above estimation method, the minimum required sample size was 384 participants. However, as the survey ended, a total of 1377 samples was collected, which exceeded the minimum sample needed for this study. Besides, we employed Kaiser–Meyer–Olkin (KMO) sampling adequacy test to ensure that the collected sample was sufficient; the minimum acceptable value for this test is 0.6.Citation31 However, the estimated value of the KMO test was 0.89, implying that the sample used for this study was adequate. Furthermore, collected data were assessed to verify the internal consistency reliability using Cronbach’s alpha and the intra-class correlation coefficient. The results showed acceptable internal consistency reliability (with Cronbach’s alpha = 0.772 and the intra-class correlation coefficient was 0.955).
Data analysis
The descriptive statistical techniques, i.e., frequency and percentage, were employed to summarize data on socio-demographic characteristics, vaccine-taking hesitancy, knowledge, attitude, and perceptions toward the COVID-19 vaccine. Knowledge about the COVID-19 vaccine was estimated based on the responses to eight general questions about the COVID-19 vaccine. One point was added to the total score for each correct response, while one point was subtracted for each incorrect response. The total score ranges from – 8 to 8 on the arithmetic scale. Then, the respondents were categorized as having adequate knowledge for a cumulative score of more than or equal to one and inadequate knowledge who had less than one point in total. Respondents’ attitude toward the COVID-19 vaccine was measured through a 5-point Likert-type scale (Strongly disagree = 1, Disagree = 2, Not sure = 3, Agree = 4, Strongly agree = 5). To assess participants’ perceptions toward the COVID-19 vaccine, we asked a series of Yes/No/Not sure statements to the respondents. Besides, the intention to be vaccinated against the COVID-19 vaccine according to the respondent’s demographic characteristics was estimated by ordinal logistic regression. Data were analyzed by using the STATA version 15 software.
Ethics approval
Ethical approval was not required for this study since human participants were ensured following local legislation and institutional requirements. Besides, all proceeds of this research were carried out following the Helsinki Declaration principles of human subject investigation. Participation in this survey was anonymous and voluntary, assuring consent of prospective respondents before the interview. Data accumulated for this research was treated confidentially.
Empirical results
Socio-demographic and clinical characteristics of the respondents
shows the personal and clinical characteristics of the studied participants. Among the participants, more than half (56.64%) were males, and nearly half of the participants (48.17%) were young, whereas only 25.04% were more than 51 years aged. Approximately 60% of the respondents were university graduates, and only 18.53% completed primary education. By occupation, 27.37% of the participants were students, while 12.20% and 5.09% were day laborers and farmers, respectively. The monthly income of a large proportion of the participants (48.58%) ranged from 200$ to 500$. Almost more than half of the participants (54.47%) reported their residence in urban areas, whereas 19.83% and 25.71% were from rural and semi-urban areas, respectively. All participants stated that they had heard about the COVID-19 vaccine. The most commonly listed sources from where they know about the vaccine were social media (40.96%), followed by television (26.80%). Within the participants, 64.49% claimed that they were not affected by COVID-19, 13.27% were infected by COVID 19, and 23.32% did not test even. However, only 8.08% of respondents’ family members got affected by the coronavirus. Besides, 55.26% of participants were ill during the pandemic having chronic diseases including, e.g., Asthma, kidney failure, Diabetes, and others.
Table 1. Participants’ characteristics (N = 1377)
Knowledge about the COVID-19 vaccine
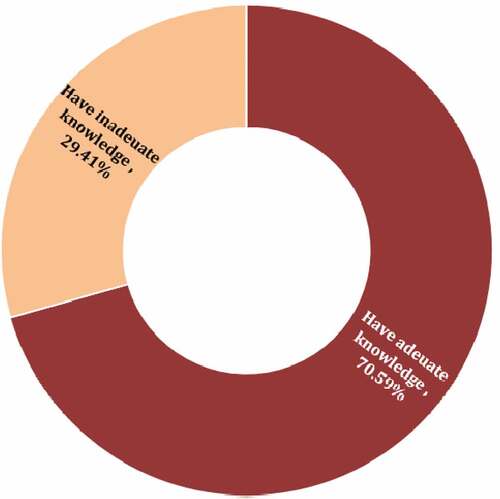
For the knowledge assessment, respondents were asked eight questions related to the COVID-19 vaccine. The statistics of respondents’ correct and incorrect answers to a particular question are presented in . Findings reveal that majority of the respondents were accurate for most of the questions. However, around fifty percent of the respondents were incorrect about the commencement date of the vaccination program and the age requirement for vaccination in Bangladesh. Besides, overall, 70.59% of respondents had adequate knowledge about vaccination programs ().
Table 2. Knowledge about COVID-19 vaccine (N = 1377)
Figure 1. Percentage of respondents having adequate and inadequate knowledge on COVID-19 vaccine.
Vaccination intentions among respondents
The details about the respondents’ intentions toward vaccination based on socio-demographic are summarized in . Overall, 45.76% of the participants were willing to be vaccinated whereas, 35.25% were not sure about getting inoculated, and 18.99% were denied the vaccination. Among the respondents’ age category, old respondents were more willing to be vaccinated. Besides, female participants were more inclined to get vaccinated than males. Respondents having graduation degrees were the largest category in ready to be vaccinated, where primary educated persons (18.18%) belonged to the minor category. Besides, in terms of profession, health professionals (76.92%) were more desired to have vaccinated, followed by government job holders (57.14%) and retired persons (45.45%). Moreover, participants living in the urban (50.00%), semi-urban areas (40.66%), and relatively wealthy persons were more intended to be vaccinated. However, looking at the closure, we found that presence of chronic disease, previous COVID-19 affected, and adequate knowledge about COVID-19 had a significant influence on vaccination intention. More than half of the chronic disease-affected participants and three-fourth of the respondents who got affected by COVID-19 were willing to be vaccinated. Besides, 69.07% of the respondents were ready to be vaccinated who had adequate knowledge about the COVID-19 vaccine. However, the likelihood of being COVID-19 vaccinated was significantly increased with older age, having more years of schooling, holding healthcare profession, living in urban or semi-urban areas. Besides, rich people having chronic diseases, tested for COVID-19 positive, and respondents possessing adequate knowledge about the COVID-19 vaccine were significantly associated with the intention to vaccinate against COVID-19.
Table 3. Percentage and odd ratio^ (95% CI) of “intention to get vaccinated against COVID-19“classified as yes, not sure and no according to participants characteristics (N = 1377)
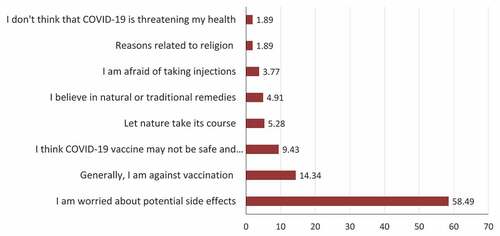
Findings from disclose that potential side effects of the vaccine were the primary concern for more than half of the participants (58.49%). However, a considerable number of participants (14.34%) were against the vaccination program, and approximately 10% of the respondents were concerned about the effectiveness of the vaccine. On the contrary, religious issues (1.89%), afraid of taking injections (3.77%), and belief in natural remedies (4.91%) were the least reported reasons for unwillingness or unsure of being vaccinated.
Figure 2. Reasons were given by respondents who were not willing or unsure whether they would like to take the COVID-19 vaccine in percent (N = 747).
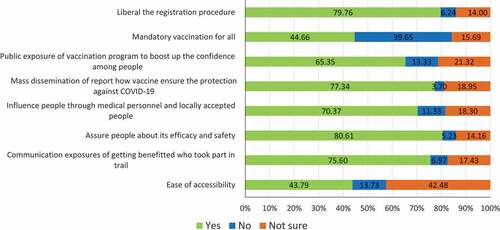
Lessening the hesitancy toward the vaccination program is the leading concern for Bangladesh now to attain a sizable inoculation rate. There may have a considerable number of strategies to lessen the vaccine hesitancy of the doubters. Assuring efficiency and safety (80%), details about the benefits of participants in the trial program (75.60%) can reduce the vaccine hesitancy (). Besides, public exposer programs (65.35%) and recommendations from medical personal or locally accepted people (70.37%) can boost the confidence for being vaccinated. However, nearly fifty percent of respondents were against the strategy of mandatory vaccines for all.
Figure 3. Ways to reduce the vaccine taking hesitancy among participants (N = 1377).
Perceptions of participants about COVID-19 vaccine
In our study, most of the participants (75.16%) had a dissatisfied perception about the side effects of the vaccine, and only 9.15% of respondents believed in the vaccine’s effectiveness (). Moreover, there had some prejudiced among the respondents like coronavirus disease is automatically curable (21.35%), antibiotics can cure the virus (22.66%), vaccine applicable only who got affected by COVID-19 (10.68%), and more stressfully some of the respondents (7.84%) believe the vaccine is not needed for Bangladesh. In addition, some of the participants (23.75%) believed media coverage about vaccination is exaggerated. Besides, more than 50% of respondents thought the vaccine is only applicable to patients with chronic disease, and developing immune systems by good diet practice can countervail the vaccine requirement. There were also some misconceptions about the vaccine among the participants. Some participants were concerned that vaccines were initially developed for business purposes (16.34%), and the vaccine would be overpriced (29.85%) in Bangladesh. However, more than fifty-five percent of participants were ready to buy the vaccine at an affordable price when available at the open market. Over and above, 56.62% of the participants believed that the vaccine would help Bangladesh win the battle against COVID-19.
Table 4. Perceptions about the COVID-19 vaccine (N = 1377)
Respondents’ attitude toward COVID-19 vaccine
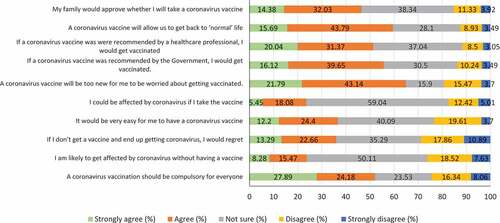
represents the information about the respondents’ attitude toward the COVID-19 vaccine. Around fifty percent of the respondents believed they need to get family permission to be vaccinated, and approximately sixty percent believed the vaccine would restore normal life in Bangladesh. However, a significant portion of participants agreed to be vaccinated if they are persuaded and recommended by the government (55.77%) and healthcare professionals (51.41%). Surprisingly, nearly one-quarter of respondents believed that they would get affected by coronavirus if they get vaccinated. Furthermore, roughly one-quarter of respondents thought access to vaccination would be difficult for them, whereas forty percent of the respondents were unsure about access to the vaccine. Moreover, thirty percent of the respondents claimed that they would not regret it if they ended up getting affected by COVID-19 without a vaccine. Only one-quarter of respondents believed that they were likely to get affected by COVID-19 without being vaccinated, where nearly 50% of the respondent were not sure.
Figure 4. Attitude toward COVID-19 vaccine (N = 1377).
Discussions
The COVID-19 pandemic is continuously plundering the global healthcare system as well as the social and economic situation. The absence of vaccines leads to this ravaged social and economic situation as well as thousands of deaths.Citation32,Citation33 In Bangladesh, the government starts its COVID-19 vaccination program on February 7, 2021. However, low vaccine coverage and hesitancy toward the vaccine among the Bangladeshi people can spoil the current efforts. Despite the fact that Bangladesh has several vaccination services, the entire newness of the COVID-19 vaccination roll-out raises concerns about vaccine delivery and acceptance. In this regard, this study tries to assess the reluctance toward the vaccine by studying the knowledge, perceptions, and attitude toward the COVID-19 vaccine in Bangladesh. As a result, our findings will be critical in establishing COVID-19 vaccination-related health education and awareness campaigns.
In assessing knowledge about the COVID-19 vaccine, this study found that more than seventy percent of the respondents had adequate knowledge about the vaccine. Disparate findings were reported in the earlier study related to the knowledge about the COVID-19 vaccine in Bangladesh.Citation34 However, the level of knowledge is higher than the previous studies on the knowledge about COVID-19 pandemic (not vaccine) among Bangladeshi people (61.2%)Citation35 and (33.0%).Citation36 This is because people are trying to keep more information about the pandemic and vaccine since it is a burning issue in the country’s present situation. The higher knowledge level among the participants about the COVID-19 vaccine could be linked with the government exposure or publicity about the COVID-19 vaccination. The rate of providing an appropriate answer of different questions in the knowledge assessment differed significantly from each question. For instance, the question regarding the name of the first vaccine-approved country, priority age for vaccination, and vaccine registration application received the highest rate of the wrong answers. In addition, a significant number of respondents failed to answer the correct vaccine name that the Bangladesh government has ordered recently. Although the government of Bangladesh and medical professionals disseminating the information to the general public continuously, there is also a misconception prevailing among common people.Citation37,Citation38
Findings revealed that forty-six percent of surveyed participants reported they intend to get vaccinated against COVID-19 once a vaccine becomes available to them, while it is pretty lower than China (83.8%)Citation39 and UK (64%),Citation40 even 53% of the participants were planning to get vaccinated in Pakistan.Citation41 However, vaccination intention may likely differ from actual vaccine uptake due to several demographic and economic factors. Therefore, it’s critical to investigate factors linked to vaccination intention early on, to formulate and support policy. We found that socio-demographic factors remarkably affect the vaccine-taking decision of the participants. Female and relatively old participants were more willing to be vaccinated than male and young participants because these groups of people are more vulnerable to COVID-19.Citation42 Besides, educated and wealthy respondents were interested in the vaccination program. These findings are aligned with recent studiesCitation35,Citation43 but contradict Neumann-Böhme et al.Citation26 who stated men were more willing to be vaccinated. The difference in vaccination intentions among the urban, semi-urban, and rural areas may be attributed to the low exposure of vaccination programs in rural areas.Citation44 Since the rural communities of Bangladesh are comparatively less exposed to media and updated information, they are more ambiguous about the vaccine with prevailing prejudices. This discrepancy of interest in vaccination between rural and urban areas can hamper the whole effort of the government against the COVID-19 pandemic. Our findings also reported that healthcare and government professionals were more interested in being vaccinated than people of other professions. Surprisingly, none of the farmers in our study were willing to be vaccinated. This finding can be attributed to a lack of constructive, and clear information about vaccination in rural areas. In addition, having a chronic disease, previously corona-affected people were significantly willing to be vaccinated, and this finding can be scrutinized based on their constant contact with the health professional. Popa et al.Citation45 also mentioned in their study continuous contact with physicians can reduce vaccine hesitancy.
However, we asked respondents the reason for their vaccine hesitancy. More than fifty percent of respondents were concerned about the side effects of vaccines, where a considerable number of participants believed the vaccine would not be safe and effective. But it is essential to convince them about the safety and effectiveness of the vaccine. Several scholars also agreed with the fact that public assurance should be ensured about vaccine safety and efficacy during mass vaccination programs.Citation26,Citation46 Otherwise, there is a potential risk of losing public interest to get vaccinated, ultimately losing possible herd immunity. Our findings also revealed that assuring the public about vaccine safety and efficiency (80.61%) can reduce vaccine hesitancy. According to this, mass dissemination of information about the vaccine’s effectiveness, details about the imported vaccine, and different promotional and communication activities can upgrade the confidence of people to take the vaccine. Beyond this, the vaccine should be available in a timely and easily accessible manner without any attrition.Citation47 In addition, this study suggested that a liberal registration procedure also can be a good strategy (79.76%) for increasing vaccination intention. However, the scarcity of the COVID-19 vaccine forced the government to develop strategies to vaccinate the elder class and front-fighters of coronavirus on a priority basis. Findings also revealed that nearly forty percent of respondents are against mandatory vaccination. In line with the results, Nitschke et al.Citation48 reported that the government should avoid enforcement in vaccination as it may prove a good strategy for a limited time but has a destructive impact on the social system.
A considerable number of participants had some prejudice about coronavirus disease and its vaccine, i.e., automatic curable, antibiotics can treat the virus, only corona affected person should be vaccinated. But, a substantial portion of respondents was not sure about these statements, and we believed that proper information dissemination and building trust could easily remove these kinds of prejudice. However, the government should take a strong initiative against antibiotic use. The use of antibiotics against coronavirus can significantly increase antibacterial resistance.Citation49 Besides, less than fifty percent respondents disagreed with the statement that vaccine was developed for business purpose and vaccine will be overpriced if it becomes available in the open market. Continued media coverage about the vaccine sale privately and vaccine price may be responsible for this misperception in Bangladesh.Citation50,Citation51 We also found that more than fifty percent of respondents were ready to buy vaccines at an affordable price. This acceptance rate in affordable price is lower than other countries, i.e., Indonesia (67–95%), USA (67–69%), and Ecuador (85%).Citation52–55 These findings can be attributed to the impoverished financial condition of the Bangladeshi people, compounded by the recent loss of livelihood during the COVID-19 pandemic.Citation56 Consequently, this loss in livelihood has also contributed to unemployment, hunger, malnutrition, and social unrest, resulting in a lack of financial resources to pay for the COVID-19 vaccine among the general public.Citation34
A considerable number of respondents had an attitude that they will get affected by the coronavirus if they take the vaccine. Moreover, approximately 65% of respondents opined that they would be too worried to take the COVID-19 vaccine since it is newly developed. New vaccine hesitancy is usual for the respondent; they are concerned it may be experimental without sufficient clinical trial, and the vaccine may not be appropriate for some category people like an allergic person, pregnant women, etc.Citation26 However, the majority of the respondents agreed to get vaccinated if the government and health professionals recommend them because they had trust and reliability in the healthcare professionals. Along with this, more than half of the selected respondents believe that vaccination programs can bring back a normal life.
In our study, a substantial number of participants were unsure about the different statements related to their perceptions of the COVID-19 vaccine. Good communication and dispatch of pertinent information can easily persuade them in the vaccination program. Constant dissemination of information about the coronavirus and vaccination program is needed to reduce vaccine hesitancy as well as to develop a more positive perception and attitude toward the COVID-19 vaccine. In addition, the government should take initiatives like launching health education programs through health authorities immediately to curb misinformation. It is also crucial to ensure the accessibility and affordability of vaccines for increasing the acceptance rate.Citation57
One of the main limitations of our study, majority of the data were collected through the online self-reporting method, subject to memory bias and social acceptability. Therefore, future research can be conducted in a more engaging way with the respondents like face to face interview through proportionate participation from all over the country. However, COVID-19 vaccination is now a primary concern for the country’s policymakers. Therefore, we believe our study will provide helpful information to the policymakers who want to vaccinate the majority proportion of people in Bangladesh to gain herd immunity against the coronavirus.
Concluding remarks
This study outlines the COVID-19 vaccine-taking hesitancy among Bangladeshi people and possible measures to increase the vaccine-taking intention. Besides, our study also demonstrates the knowledge, perceptions, and attitude toward the COVID-19 vaccine. Interestingly, a substantial portion of respondents is updated about the COVID-19 vaccine from social media and television, while approximately three-fourth of respondents have adequate knowledge about the COVID-19 vaccine. On the other hand, young less educated persons, farmers, and rural people are more hesitant to get vaccinated. Needless to know, targeting this portion of people with clear communication exposer of safety and efficacy of the vaccine and participation of rural community health clinic in vaccination program could ameliorate people’s overall intention to taking the vaccine. It is a dire concern that only less than half of the participants exposed their willingness to be vaccinated. Among those who are hesitant to be vaccinated claimed that they are worried about the potential side effects. However, as a remarkable portion of respondents reported to be defiant about the vaccine, it is not surprising that respondents’ perceptions and attitudes toward the vaccination program were unsatisfactory.
Recommendations and policy guidance
Indeed, to the best of our knowledge, this study is a novel approach in Bangladesh dedicated to revealing the vaccine-taking decision of general people. Given our findings, we may suggest some policies and recommendations that may guide the authority in expediting the mass vaccination program. First, vaccination awareness campaigns should be implemented immediately, especially in rural areas. Second, reports on the experiences of the people who received the vaccines should be disseminated widely. A campaign emphasizing mass vaccination irrespective of age, the public exposure of social benefits of vaccination, and influencing general people through locally accepted persons can increase the willingness to be vaccinated against COVID-19. Besides, doctors and healthcare professionals should play a key role in raising awareness about the vaccine among general people. Third, the vaccination registration procedure should be more convenient and easily accessible for all groups of people. Apart from online registration, in-person and booth registration can be implemented. Lastly, a combined effort from all the ministries concerned of the government, NGOs, different voluntary organizations, healthcare professionals, journalists, and the mass public can drive the country to a successful mass vaccination program in the battle against the pandemic should be pursued.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors are grateful to the participants of this study for sharing their information.
Data available statements
Data used for this study are confidential and cannot be shared publicly, however, can be found from the corresponding author upon reasonable request.
Additional information
Funding
References
- Zheng J. SARS-CoV-2: an emerging coronavirus that causes a global threat. Int J Biol Sci. 2020;16(10):1678–85. doi:10.7150/ijbs.45053.
- Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Bio Medica. 2020;91(1):157. doi:10.23750/abm.v91i1.9397.
- Ducharme J. Time. World health organization declares COVID-19 a “Pandemic.” Here’s what that means. 2020 [accessed 2021 June 11]. https://time.com/5791661/who-coronavirus-pandemic-declaration/.
- Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, Wang M. Presumed asymptomatic carrier transmission of COVID-19. Jama. 2020;323(14):1406–07. doi:10.1056/NEJMoa2001316.
- Yashavantha Rao HC, Jayabaskaran C. The emergence of a novel coronavirus (SARS‐CoV‐2) disease and its neuroinvasive propensity may affect COVID‐19 patients. J Med Virol. 2020;92(7):786–90. doi:10.1002/jmv.25918.
- Alola AA, Alola UV, Sarkodie SA. The nCOVID-19 and financial stress in the USA: health is wealth. Environ Dev Sustain. 2021;23(6):9367–78. doi:10.1007/s10668-020-01029-w.
- Meludu NT, Abolade T. Corona Virus, Climate Change, and Food Security. In: Leal Filho W, Oguge N, Ayal D, Adeleke L, da Silva I, editors. African handbook of climate change adaptation 2021. Cham: Springer; 2021. p. 563–79. https://doi.org/10.1007/978-3-030-45106-6_233.
- United Nations (UN). Sustainable development outlook 2020: achieving SDGs in the wake of COVID-19: scenarios for policymakers. Department of Economic and Social Affairs Economic Analysis; 2020 [accessed 9 July 2021]. https://www.un.org/development/desa/dpad/publication/sustainable-development-outlook-2020-achieving-sdgs-in-the-wake-of-covid-19-scenarios-for-policymakers/.
- Sundararaman T, Muraleedharan VR, Ranjan A. Pandemic resilience and health systems preparedness: lessons from COVID-19 for the twenty-first century. J Social Econ Dev. 2021. doi:10.1007/s40847-020-00133-x.
- Alola AA, Olowu FB. The health scare of COVID-19 amidst pandemics and the immune-related pharmaceutical products spillovers in the USA. Environ Sci Pollut Res. 2020;27(36):45949–56. doi:10.1007/s11356-020-11195-z.
- Zimmer C, Corum J, Wee S, Times NY. Coronavirus Vaccine Tracker 2021. [accessed 9 July 2021]. https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html.
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, Perez JL, Pérez Marc G, Moreira ED, Zerbini C, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. New Eng J Med. 2020;383(27):2603–15. doi:10.1056/NEJMoa2034577.
- Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R, Diemert D, Spector SA, Rouphael N, Creech CB, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. New Eng J Med. 2021;384(5):403–16. https://doi/full/10.1056/nejmoa2035389.
- Voysey M, Clemens SA, Madhi SA, Weckx LY, Folegatti PM, Aley PK, Angus B, Baillie VL, Barnabas SL, Bhorat QE, et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. 2021;397(10269):99–111. doi:10.1016/S0140-6736(20)32661-1.
- Velavan TP, Pollard AJ, Kremsner PG. Herd immunity and vaccination of children for COVID-19. Int J Infect Dis. 2020;98::14–15. doi:10.1016/j.ijid.2020.06.065.
- Felsenstein S, Hedrich CM. COVID-19 in children and young people. Lancet Rheumatol. 2020;2(9):e514–e516. doi:10.1016/S2665-9913(20)30212-5.
- Snape MD, Viner RM. COVID-19 in children and young people. Science. 2020;370(6514):286–88. doi:10.1126/science.abd6165.
- Reintjes R, Das E, Klemm C, Richardus JH, Keßler V, Ahmad A. Pandemic public health paradox”: time series analysis of the 2009/10 influenza A/H1N1 epidemiology, media attention, risk perception and public reactions in 5 European countries. PloS One. 2016;11(3):e0151258. doi:10.1371/journal.pone.0151258.
- Fadda M, Albanese E, Suggs LS. When a COVID-19 vaccine is ready, will we all be ready for it? Int J Public Health. 2020;65:711–12. doi:10.1007/s00038-020-01404-4.
- Larson H, de Figueiredo A, Karafillakis E, Rawal M. State of vaccine confidence in the EU 2018. Vol. 10. Luxembourg: Publications Office of the European Union; 2018. p. 241099. [accessed 21 February 2021]. https://www.quotidianosanita.it/allegati/allegato7138657.pdf.
- Kata A. Anti-vaccine activists, Web 2.0, and the postmodern paradigm–An overview of tactics and tropes used online by the anti-vaccination movement. Vaccine. 2012;30(25):3778–89. doi:10.1016/j.vaccine.2011.11.112.
- Business Standard. Bangladesh approves getting 30 mn doses of Covishield vaccine from India. 2021 [accessed 25 February 2021]. https://www.business-standard.com/article/current-affairs/bangladesh-approves-getting-30-mn-doses-of-covishield-vaccine-from-india-121010800256_1.html.
- Blankenship K. AstraZeneca hopes warmer storage needs for COVID-19 vaccine will be an advantage against mRNA competitors. FIERCE Pharma; 2020 [accessed 25 February 2021]. https://www.fiercepharma.com/manufacturing/astrazeneca-hopes-warmer-storage-needs-for-covid-19-vaccine-will-be-advantage-against
- Peretti-Watel P, Seror V, Cortaredona S, Launay O, Raude J, Verger P, Fressard L, Beck F, Legleye S, L’Haridon O, et al. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. Lancet Infect Dis. 2020;20(7):769–70. doi:10.1016/S1473-3099(20)30426-6.
- Khubchandani J, Sharma S, Price JH, Wiblishauser MJ, Sharma M, Webb FJ. COVID-19 vaccination hesitancy in the United States: a rapid national assessment. J Community Health. 2021;46(2):270–77. doi:10.1007/s10900-020-00958-x.
- Neumann-Böhme S, Varghese NE, Sabat I, Barros PP, Brouwer W, van Exel J, Schreyögg J, Stargardt T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur J Health Econ. 2020;21(7):977–82. doi:10.1007/s10198-020-01208-6.
- Barello S, Nania T, Dellafiore F, Graffigna G, Caruso R. Vaccine hesitancy among university students in Italy during the COVID-19 pandemic. Eur J Epidemiol. 2020;35(8):781–83. doi:10.1007/s10654-020-00670-z.
- Thorneloe R, Wilcockson H, Lamb M, Jordan CH, Arden M. Willingness to receive a COVID-19 vaccine among adults at high-risk of COVID-19: a UK-wide survey. [accessed 5 March 2021]. https://psyarxiv.com/fs9wk/download?format=pdf.
- Paul A, Nath TK, Mahanta J, Sultana NN, Kayes AI, Noon SJ, Jabed MA, Podder S, Paul S. Psychological and livelihood impacts of COVID-19 on Bangladeshi lower income people. Asia Pac J Public Health. 2021;33(1):100–08. doi:10.1177/1010539520977304.
- Alola UV, Avci T, Ozturen A. Organization sustainability through human resource capital: the impacts of supervisor incivility and self-efficacy. Sustainability. 2018;10(8):2610. doi:10.3390/su10082610.
- Cop S, Alola UV, Alola AA. Perceived behavioral control as a mediator of hotels’ green training, environmental commitment, and organizational citizenship behavior: a sustainable environmental practice. Bus Strategy Environ. 2020;29(8):3495–508. doi:10.1002/bse.2592.
- Fontanet A, Cauchemez S. COVID-19 herd immunity: where are we? Nat Rev Immunol. 2020;20(10):583–84. doi:10.1038/s41577-020-00451-5.
- Jones D, Helmreich S. A history of herd immunity. Lancet. 2020;396(10254):810–11. doi:10.1016/S0140-6736(20)31924-3.
- Islam MS, Siddique AB, Akter R, Tasnim R, Sujan MS, Ward PR, Sikder MT. Knowledge, attitudes and perceptions towards COVID-19 vaccinations: a cross-sectional community survey in Bangladesh. medRxiv. 2021. doi:10.1101/2021.02.16.21251802.
- Banik R, Rahman M, Sikder MT, Rahman QM, Pranta MU. Knowledge, attitudes, and practices related to the COVID-19 pandemic among Bangladeshi youth: a web-based cross-sectional analysis. J Public Health (Bangkok). 2021;16:1–11. doi:10.1007/s10389-020-01432-7.
- Paul A, Sikdar D, Hossain MM, Amin MR, Deeba F, Mahanta J, Jabed MA, Islam MM, Noon SJ, Nath TK, et al. Knowledge, attitudes, and practices toward the novel coronavirus among Bangladeshis: implications for mitigation measures. PloS One. 2020;15(9):e0238492. doi:10.1371/journal.pone.0238492.
- Rafe R. COVID: bangladesh vaccination drive marred by misinformation. 2021 [accessed 23 March 2021]. https://www.dw.com/en/covid-bangladesh-vaccination-drive-marred-by-misinformation/a-56360529
- Jara T. Covid-19 vaccination in Bangladesh: we must report responsibly on vaccine side-effects. 2021 [accessed 23 March 2021]. https://www.thedailystar.net/opinion/news/we-must-report-responsibly-vaccine-side-effects-2042689.
- Chen M, Li Y, Chen J, Wen Z, Feng F, Zou H, Fu C, Chen L, Shu Y, Sun C. An online survey of the attitude and willingness of Chinese adults to receive COVID-19 vaccination. Hum Vaccin Immunother. 2021;17(7):2279–88. doi:10.1080/21645515.2020.1853449.
- Sherman SM, Smith LE, Sim J, Amlôt R, Cutts M, Dasch H, Rubin GJ, Sevdalis N. COVID-19 vaccination intention in the UK: results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum Vaccin Immunother. 2021;17(6):1612–21. doi:10.1080/21645515.2020.1846397.
- Chaudhary FA, Ahmad B, Khalid MD, Fazal A, Javaid MM, Butt DQ. Factors influencing COVID-19 vaccine hesitancy and acceptance among the Pakistani population. Hum Vaccin Immunother. 2021. doi:10.1080/21645515.2021.1944743.
- Shahid Z, Kalayanamitra R, McClafferty B, Kepko D, Ramgobin D, Patel R, Aggarwal CS, Vunnam R, Sahu N, Bhatt D, et al. COVID −19 and older adults: what we know. J Am Geriatr Soc. 2020;68(5):926–29. doi:10.1111/jgs.16472.
- Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, Kimball S, El-Mohandes A. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2021;27(2):225–28. doi:10.1038/s41591-020-1124-9.
- Hasan K. Covid-19 vaccination: bangladesh on the right track. Dhaka Tribune; 2021 [accessed 23 March 2021]. https://www.dhakatribune.com/health/coronavirus/2021/02/14/covid-19-vaccination-bangladesh-on-the-right-track.
- Popa GL, Muntean AA, Muntean MM, Popa MI. Knowledge and attitudes on vaccination in Southern Romanians: a cross-sectional questionnaire. Vaccines. 2020;8(4):774. doi:10.3390/vaccines8040774.
- Jiang S. Don’t rush to deploy COVID-19 vaccines and drugs without sufficient safety guarantees. Nature. 2020:321–321. doi:10.1038/d41586-020-00751-9.
- Siciliani L, Wild C, McKee M, Kringos D, Barry MM, Barros PP, De Maeseneer J, Murauskiene L, Ricciardi W. Strengthening vaccination programmes and health systems in the European Union: a framework for action. Health Policy (New York). 2020;124(5):511–18. doi:10.1016/j.healthpol.2020.02.015.
- Nitschke JP, Forbes PA, Ali N, Cutler J, Apps MA, Lockwood PL, Lamm C. Resilience during uncertainty? Greater social connectedness during COVID‐19 lockdown is associated with reduced distress and fatigue. Br J Health Psychol. 2020. doi:10.1111/bjhp.12485.
- Miranda C, Silva V, Capita R, Alonso-Calleja C, Igrejas G, Poeta P. Implications of antibiotics use during the COVID-19 pandemic: present and future. J Antimicrob Chemother. 2020;75(12):3413–16. doi:10.1093/jac/dkaa350.
- Dhaka Tribune. Government to fix private vaccine price 2021 [accessed 24 March 2021]. https://www.dhakatribune.com/bangladesh/2021/01/18/health-minister-42-000-health-workers-being-provided-vaccination-training.
- Bdnews.com. Bangladesh’s Beximco could start private sales of AstraZeneca vaccine next month. 2021 [accessed 24 March 2021]. https://bdnews24.com/business/2021/01/12/bangladesh-s-beximco-could-start-private-sales-of-astrazeneca-vaccine-next-month.
- Malik AA, McFadden SM, Elharake J, Omer SB. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine. 2020;26:100495. doi:10.1016/j.eclinm.2020.100495.
- Reiter PL, Pennell ML, Katz ML. Acceptability of a COVID-19 vaccine among adults in the United States: how many people would get vaccinated? Vaccine. 2020;38(42):6500–07. doi:10.1016/j.vaccine.2020.08.043.
- Harapan H, Wagner AL, Yufika A, Winardi W, Anwar S, Gan AK, Setiawan AM, Rajamoorthy Y, Sofyan H, Mudatsir M, et al. Acceptance of a COVID-19 vaccine in southeast Asia: a cross-sectional study in Indonesia. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.00381.
- Sarasty O, Carpio CE, Hudson D, Guerrero-Ochoa PA, Borja I. The demand for a COVID-19 vaccine in Ecuador. Vaccine. 2020;38(51):8090–98. doi:10.1016/j.vaccine.2020.11.013.
- Shammi M, Bodrud-Doza M, Islam AR, Rahman MM. COVID-19 pandemic, socio-economic crisis and human stress in resource-limited settings: a case from Bangladesh. Heliyon. 2020;6(5):e04063. doi:10.1016/j.heliyon.2020.e04063.
- MacDonald NE. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–64. doi:10.1016/j.vaccine.2015.04.036.