
ABSTRACT
Purpose
We explored the willingness to pay for booster dose of COVID-19 vaccine among health-care workers in Taizhou, China.
Methods
A population-based self-administered online questionnaire evaluating the willingness of health-care workers to pay for booster vaccination of COVID-19 vaccine was conducted in Taizhou, China. Of the 1102 health-care workers received the invitation, 1072 (97.3%) had received twice vaccination of COVID-19 vaccine.
Results
There were 1569 (53.1%) out of 1072 health-care workers not willing to pay for thebooster dose of COVID-19 vaccines, 348 (32.5%) were willing to pay less than 100CHY for the booster dose of COVID-19 vaccines, only 155 (14.5%) were willing to pay more than 100 CHY. The factors related to willingness to pay for booster dose of COVID-19 vaccines were education level (c2 = 9.42, P = .01) or whether they had adverse effect to COVID-19 vaccines (c2 = 11.87, P < .01) .
Conclusion
This study found that about half of health-care workers were willing to pay for booster dose of inactivated SARS-CoV-2 vaccines in Taizhou, China, most of them are willing to pay less than 100 CHY. Health-care workers' willingness to pay for booster dose of COVID-19 vaccines were related to sex, education level, whether they had adverse effect to COVID-19 vaccines.
Introduction
The ongoing pandemic of coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has made a serious public health threat worldwide with millions of people at risk.Citation1 Safe and effective prophylactic vaccines are needed to contain the pandemic,Citation2 as the most effective method to return to normal life is a COVID-19 vaccine that prevents disease, asymptomatic infection, and transmission.Citation3 It is well known that a single dose does not immunize 100% of those who receive it.Citation4,Citation5 Coupled that the SARS-CoV-2 is prone to mutation and the vaccine is time-sensitive, it requires us to take booster shots on top of previous COVID-19 vaccination. Declines in vaccine efficacy over time are also believed to be responsible for the resurgence of the epidemic.Citation6
Previous studies have indicated that health-care workers (HCWs) have a higher risk of SARS-CoV-2 infection.Citation7–9 Therefore, vaccinating health-care workers could block transmission of SARS-CoV-2 and have beneficial knock-on effects in the wider community, which is necessary to achieve herd immunity across all the groups that potentially contribute to the transmission of SARS-CoV-2. Although receiving booster dose of COVID-19 vaccines is particularly important, vaccination cost is an essential issue for the promotion of receiving booster vaccination.
How countries, particularly low- and middle-income economies, should pay the coronavirus disease 2019 (COVID-19) vaccine is an important and understudied issue.Citation10 The acceptability of COVID-19 vaccine and willingness to pay (WTP) were assessed to provide insights into future demand forecasts and pricing considerations.Citation11 Being a health-care worker, having a high income, and having high perceived risk were associated with higher WTP.Citation10 Although the vaccine is now free of charge for all persons in China, it may not be immunized for life. As vaccine effective-ness declines and the virus mutates, it is likely that vaccines will need to be re-vaccinated in the future. Given the limited medical resources available, vaccine use is likely to be costly. Therefore, it is very important to assess the willingness of health-care workers to pay for COVID-19 vaccine for COVID-19 prevention and control. This study was conducted to explore the WTP for booster dose of COVID-19 vaccine among health-care workers in Taizhou, China.
Methods
Study design and population
We organized a population-based, anonymous, cross-sectional online survey in the WeChat-incorporated Wen-Juan Xing platform (Changsha Ranxing Information Technology Co., Ltd., Hunan, China). The target population are hospital staffs who had received twice vaccination of COVID-19 in a medical center in Taizhou, China. In September 2021, the survey was sent to all health-care workers of the hospital (n = 4191) from a list, 1,102 hospital staff accepted the survey invitation via WeChat, the response rate is 26.3%, and 1,072 of them had received twice COVID-19 vaccinations, with an overall vaccination rate of 97.3%. This study exempted informed consent and was approved by the Ethics Committee of Taizhou Hospital, Zhejiang Province, China (Approval number : K20210823). All procedures are carried out in accordance with the guidelines of our institutional Ethics Committee and in compliance with the principles of the Declaration of Helsinki. We performed a logical check of data, excluding those who were under the age of 18 or over the age of 70, excluding those who answered within 120 s. Information about all participants is kept anonymously.
Structured questionnaires
The content of the questionnaire was as follows: (1) basic demographic information, such as gender, age, occupational class, professional title, education level and underlying diseases; (2) Screen health-care workers who had received two doses of COVID-19 vaccination by a question: ‘Have you been vaccinated against COVID-19? ’(Three response options: none, once, twice); (3) In order to understand the willingness to pay, health-care workers were asked, ‘If you have to pay for the booster dose of COVID-19 vaccine, would you like to get it?’ The response options were ‘very willing’, ‘willing’, ‘unwilling’ or ‘very unwilling’. Almost all of the questions are closed, providing checkboxes for responses.(4) Then,they were asked ‘What is the maximum price you are willing to pay for the booster dose of COVID-19 vaccine?’,and the answer was ‘less than 100 CHY’, ‘100–199 CHY’, ‘200–299 CHY’,‘300–399 CHY’,‘400–499 CHY’,‘be equal or greater than 500 CHY’.
Statistical analysis
We converted continuous data, such as age, to classified data. Considering that individuals’ median WTP for COVID-19 vaccination was CNY 100 (USD 14.5) in China,12 also due to the small number of responses for ‘200–299 CHY’,‘300–399 CHY’,‘400–499 CHY’,‘be equal or greater than 500 CHY’, we classified willing-to-pay into three levels: no,0–99 CHY, and ≧100 CHY. Counts and frequency distributions were displayed for categorical data, and univariate analysis was used to find the useful factors. Only variables that were significant at the P < .05 level in the univariate analysis were then selected for the multinomial logistic regression analysis.
The associations of potential factors, such as sex, age, education level and adverse effects of COVID-19 vaccination were assessed by P values, the odds ratio (OR) and a 95% confidence interval (CI). All data were analyzed using IBM SPSS Statistics software (version 26.0; SPSS Inc., Chicago, IL, USA). A P-value less than 0.05 was considered as statistically significant.
Results
Of the 1102 health-care workers received the invitation, 1072 (97.3%) had received twice vaccination of COVID-19 vaccine. These people are our target population.As showed in , 569 (53.1%) of 1072 health-care workers were not willing to pay for the booster dose of COVID-19 vaccines, 348 (32.5%) of 1072 health-care workers were willing to pay 0–99 CHY for the booster dose of COVID-19 vaccines, only 155 (14.5%) of 1072 health-care workers were willing to pay greater than or equal to 100 CHY. The characteristics of those who had received twice the vaccination of COVID-19 vaccine are provided in . Included 905 female and 167 male, among them,435 female (48.1%,435/905) and 68 male (40.1%,68/167) were willing to pay for the booster dose of COVID-19 vaccines. And, 76.87% of the participants were aged below 40 years, and more than a half (63.6%) were nurse. Moreover, 77.8% of the participants were undergraduate and above, the vast majority (88.4%) of participants did not have underlying disease, while 88.2% of them did not have adverse effect of the two previous doses of COVID-19 vaccines.
Figure 1. The proportion of willingness to pay for booster dose of inactivated SARS-CoV-2 vaccines among health-care workers.
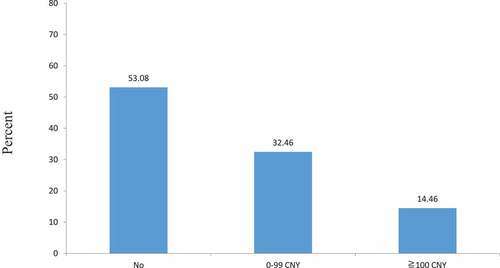
Table 1. Univariate analysis of factors associated with willingness to pay for booster dose of COVID-19 vaccine among health-care workers (n = 1072).
shows that health-care workers’ willingness to pay for booster dose of COVID-19 vaccines were related to education level (χ2 = 9.42, P = .01) or whether they had adverse effect to COVID-19 vaccines (χ2 = 11.87, P <.01). The results of the multinomial logistic regression analysis are presented in . It indicated that willing-to-pay at the price of CNY 0–99 vs. not willing-to-pay, male (P = .04, OR = 1.5, 95% CI: 1.0–2.3), health-care workers without adverse effect (P <.01, OR = 2.0, 95% CI: 1.2–3.1) were associated with their willingness to pay for booster dose of COVID-19 vaccines. While willing-to-pay at the price of CNY ≧100 vs. not willing-to-pay, college and below (P = 0.02, OR = 0.6, 95% CI:.3–0.9), health-care workers without adverse effect (P = .03, OR = 2.0, 95% CI: 1.1–3.7) were associated with their willingness to pay for booster dose of COVID-19 vaccines.
Table 2. Multinomial logistic regression analysis of factors associated with willingness to pay for booster vaccination of COVID-19 vaccine among health-care workers (n = 1072).
Discussion
The COVID-19 pandemic has dramatically affected the lives of people around the world, affecting their health and economic well-being, that could prompt people to buy vaccines. But the willingness of different populations in different countries to pay for vaccines is markedly different, influenced by many different factors. Income and education levels and having family members with COVID-19 increased the likelihood of persons paying for a vaccine.Citation13 Annual family income, employee size in the workplace, and whether considering the COVID-19 pandemic in China in a declining trend affected respondents’ WTP significantly.Citation12
Many previous studies have shown that the WTP for vaccination against COVID-19 from different cross-sectional studies was very different.Citation10–22 However, the related studies did not use the same question design, making comparison of results impossible. For example, the Wang 2021 studyCitation12 found that 90% of the adults in China were willing to pay for a COVID-19 vaccine. But that study has a “refused” category that made it possible to conclude that 91% of the adults would accept a COVID-19 vaccine. In addition, the price of WTP for one dose of vaccine against COVID-19 range from US$2.4 to US$231.9, the prices vary nearly 100 times in different countries and regions. Generally speaking, this is closely related to the level of economic development of the country. As for the research on the willingness-to-pay for COVID-19 vaccine of different occupational groups, previous studies have shown that patients with depression or anxiety disorder have higher willingness-to-pay than the general population,Citation18 and teachers have lower willingness-to-pay.Citation19 According to the different willingness to pay in different income groups, some scholars have suggested the governments can provide the vaccine-free to low-income groups and allow those with higher incomes to acquire the vaccine through the private sector by paying. This will be useful especially for countries with economic difficulties.Citation13
As protection against SARS-CoV-2 infection has waned after a two-dose schedule of COVID-19 vaccines, policy makers have begun to consider the implications for periodic or seasonal third dose, also known as a booster, vaccination against COVID-19 to protect the most vulnerable patients, and mitigate health-care and economic impacts.Citation23 But few data exist on COVID-19 vaccines given as a third (booster) dose.Citation23 It is clear that the behavior and willingness of health workers to administer booster vaccines is very important for the vaccination of society as a whole.
Our study showed that only 46.9% of 1072 health-care workers were willing to pay for the booster dose of COVID-19 vaccines. We found it is much lower than the general public’s willingness-to-pay for COVID-19 vaccines in previous studies in China.Citation12,Citation15,Citation17 As health-care workers, their willingness to pay for COVID-19 vaccine is actually lower than that of the general public, which is probably mainly due to their optimistic judgment on the COVID-19 situation in China. This may be closely related to China’s cultural background, that is, whether WTP of medical staff is lower than that of the general public is related to the fact that they think hospitals are responsible for providing vaccines for them for occupational protection. Currently, most health-care workers in China work full-time in public hospitals, and our research objects are also health-care workers in public hospitals. Most of them probably believe hospitals or the government are responsible for providing vaccines for them for occupational protection, or at least should pay part of their vaccine costs. Of course, this cannot rule out vaccine fatigue or bias caused by studies in different parts of China.
We also found that health-care workers’ willingness to pay for booster dose of COVID-19 vaccines were related to education level or whether they had adverse effect to COVID-19 vaccines. This is similar to some studies that focus on factors associated with willingness to pay for two previous doses of COVID-19 vaccine.Citation12,Citation13,Citation17
We first analyze different payments of booster dose of COVID-19 vaccines and find that the influencing factors of willingness to pay are different under different payment amounts. Male, health-care workers without adverse effect were associated with their willingness to pay for booster dose of COVID-19 vaccines when the price is CNY 0–99 CHY. This means men are more likely than women to pay less than 100 CHY for vaccines among health-care workers. Education level and adverse effect were associated with their willingness to pay when the price is ≧100 CHY. That is to say, health-care workers who were undergraduate and above are more likely than college and below to pay ≧100 CHY for vaccines.
This suggests that, in order to improve the willingness to pay for booster dose of COVID-19 vaccines, the publicity and education of the benefits of vaccination should be strengthened among men and those with low education levels. This is very important for the next step of COVID-19 control.
Limitation
Some limitations of this study need to be discussed. First, due to the one study hospital, the sample may not be fully representative of the health-care works of China. The response rate was relatively low (26.3%), and the survey respondents were likely to be younger and healthier than the general population, given that they are young and healthy enough to be employed in health care, which may result in selection bias.
Second, generalization of the findings still requires causal relationship. The results are not necessarily applicable to other occupational groups. Third, the online data collection method is a limitation of this study, which could potentially lead to over-reporting lower WTP for booster dose of COVID-19 vaccine. Fourth, our estimates were explored at only one time point and could not reflect long-term exposure to various factors. Further epidemiological and longitudinal investigations are essential not only to extrapolate findings to other regions of China but also to better understand the causal relationship between factors and WTP of booster doses of COVID-19 vaccines. Fifth, there are many types of COVID-19 vaccines in China and people were randomly vaccinated one type. It is difficult to control the impact of different vaccines in this study, so we could not estimate the WTP for different vaccines. Finally, we did not exact understand whether HCWs would accept a booster dose—only whether they would pay for a booster dose, that is, we did not determine how many subjects wanted a COVID-19 booster but also wanted the government (or hospital) to pay for the booster dose. Since 97% of the HCWs were vaccinated with a primary series, presumably a high proportion will want a booster dose, too. A proportion (probably a large proportion) of HCWs who were unwilling to pay for a booster would be willing to receive a booster dose if they did not need to pay.
Conclusions
This study found that about half of health-care workers were willing to pay for booster dose of inactivated SARS-CoV-2 vaccines in Taizhou, China, and most of them are willing to pay less than 100 CHY. Health-care workers’ willingness to pay for booster dose of COVID-19 vaccines were related to sex, education level, whether they had adverse effect to COVID-19 vaccines. To improve the WTP for booster dose of COVID-19 vaccines, the publicity and education of the benefits of vaccination should be strengthened among men and those with low education levels.
Acknowledgements
The authors gratefully acknowledge the supervisors and all employees who participated in this study for their assistance as well as all the experts and members of our group for their help and advice.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Majumder J, Minko T. Recent developments on therapeutic and diagnostic approaches for COVID-19. Aaps J. 2021;23(1):14. doi:10.1208/s12248-020-00532-2.
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, Perez JL, Pérez Marc G, Moreira ED, Zerbini C, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383:2603–5. doi:10.1056/NEJMoa2034577.
- Russell FM, Greenwood B. Who should be prioritised for COVID-19 vaccination? Hum Vaccin Immunother. 2021;17(5):1317–21. doi:10.1080/21645515.2020.1827882.
- Committee on Infectious Diseases. Universal hepatitis B immunization. Pedi-Atrics. 1992;4:795–800. doi:10.1542/peds.89.4.795.
- Gay NJ. The theory of measles elimination:implications for the design of elimination strategies. J Infect Dis. 2004;189(suppl 1):S27–35. doi:10.1086/381592.
- Naaber P, Tserel L, Kangro K, Sepp E, Jürjenson V, Adamson A, Haljasmägi L, Rumm AP, Maruste R, Kärner J, et al. Dynamics of antibody response to BNT162b2 vaccine after six months: a longitudinal prospective study. Lancet Reg Health Eur. 2021 ;10:100208. Epub 2021 Sep 6. PMID: 34514454; PMCID:PMC8418937. doi:10.1016/j.lanepe.2021.100208.
- Sabetian G, Moghadami M, Hashemizadeh Fard Haghighi L, Shahriarirad R, Fallahi MJ, Asmarian N, Moeini YS. COVID-19 infection among healthcare workers: a cross-sectional study in southwest Iran. Virol J. 2021;18(1):58. PMID: 33731169. doi:10.1186/s12985-021-01532-0.
- Euronews: at least 90,000 healthcare workers infected by COVID-19’, says nursing group. [accessed 8 July]. https://www.euronews.com/2020/05/06/at-least90-000-healthcare-workers-infected-by-covid-19-says-nursing-group
- Zheng L, Wang X, Zhou C, Liu Q, Li S, Sun Q, Wang M, Zhou Q, Wang W. Analysis of the infection status of the health care workers in Wuhan during the COVID-19 outbreak: a cross-sectional study. Clin Infect Dis. 2020;71:2109–13. doi:10.1093/cid/ciaa588.
- Harapan H, Wagner AL, Yufika A, Winardi W, Anwar S, Gan AK, Setiawan AM, Rajamoorthy Y, Sofyan H, Vo TQ, et al. Willingness-To-Pay for a COVID-19 vaccine and its associated determinants in Indonesia. Hum Vaccin Immunother. 2020 ;16(12):3074–80. Epub 2020 Sep 29.PMID: 32991230. doi:10.1080/21645515.2020.1819741.
- Wong LP, Alias H, Wong PF, Lee HY, AbuBakar S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum Vaccin Immunother. 2020;16(9):2204–14. Epub 2020 Jul 30. PMID 32730103. doi:10.1080/21645515.2020.1790279.
- Wang J, Lyu Y, Zhang H, Jing R, Lai X, Feng H, Knoll MD, Fang H. Willingness to pay and financing preferences for COVID-19 vaccination in China. Vaccine. 2021 ;39(14):1968–76. Epub 2021 Feb 27.PMID: 33714653. doi:10.1016/j.vaccine.2021.02.060.
- Cerda AA, García LY. Willingness to pay for a COVID-19 vaccine. Appl Health Econ Health Policy. 2021;19(3):343–51. Epub 2021 Feb 23. PMID: 33619688. doi:10.1007/s40258-021-00644-6.
- Kabir R, Mahmud I, Chowdhury MTH, Vinnakota D, Jahan SS, Siddika N, Isha SN, Nath SK, Hoque Apu E. COVID-19 vaccination intent and willingness to pay in Bangladesh: a cross-sectional study. Vaccines (Basel). 2021;9(5):416. PMID:33919254. doi:10.3390/vaccines9050416.
- Han K, Francis MR, Zhang R, Wang Q, Xia A, Lu L, Yang B, Hou Z. Confidence, acceptance and willingness to pay for the COVID-19 vaccine among migrants in Shanghai, China: a cross-sectional study. Vaccines (Basel). 2021;9(5):443. PMID:34063182. doi:10.3390/vaccines9050443.
- Adigwe OP. COVID-19 vaccine hesitancy and willingness to pay: Emergent factors from a cross-sectional study in Nigeria. Vaccine X. 2021;9:100112. doi:10.1016/j.jvacx.2021.100112. Epub 2021 Sep 3.PMID: 34494000.
- Qin W, Wang E, Ni Z. Chinese consumers’ willingness to get a COVID-19 vaccine and willingness to pay for it. PLoS One. 2021 May 4;16(5):e0250112. eCollection 2021.PMID: 33945544. doi:10.1371/journal.pone.0250112.
- Hao F, Wang B, Tan W, Husain SF, McIntyre RS, Tang X, Zhang L, Han X, Jiang L, Chew NWS, et al. Attitudes toward COVID-19 vaccination and willingness to pay: comparison of people with and without mental disorders in China. Bjpsych Open. 2021 Aug 11;7(5):e146. eCollection 2021 Sep. DOI:10.1192/bjo.2021.979. PMID: 34422295. doi:10.1192/bjo.2021.979.
- Shitu K, Wolde M, Handebo S, Kassie A. Acceptance and willingness to pay for COVID-19 vaccine among school teachers in Gondar City, Northwest Ethiopia. Trop Med Health. 2021 ;49(1):63. PMID: 34372943. doi:10.1186/s41182-021-00337-9.
- Banik R, Islam MS, Pranta MUR, Rahman QM, Rahman M, Pardhan S, Driscoll R, Hossain S, Sikder MT. Understanding the determinants of COVID-19 vaccination intention and willingness to pay: findings from a population-based survey in Bangladesh. BMC Infect Dis. 2021;21(1):892. PMID: 34465297. doi:10.1186/s12879-021-06406-y.
- Arshad MS, Hussain I, Mahmood T, Hayat K, Majeed A, Imran I, Saeed H, Iqbal MO, Uzair M, Rehman AU, et al. A national survey to assess the COVID-19 vaccine-related conspiracy beliefs, acceptability, preference, and willingness to pay among the general population of Pakistan. Vaccines (Basel). 2021;9(7):720. PMID:34358136. doi:10.3390/vaccines9070720.
- Campbell ZA, Otieno L, Shirima GM, Marsh TL, Palmer GH. Using contingent valuation method to estimate adults’ willingness to pay for a future coronavirus 2019 vaccination. Value Health Reg Issues. 2021;24:240–46. PMID:30478006. doi:10.1016/j.vaccine.2018.11.058.
- Munro APS, Janani L, Cornelius V, Aley PK, Babbage G, Baxter D, Bula M, Cathie K, Chatterjee K, Dodd K, et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdox1 nCov-19 or BNT162b2 in the UK (COV-BOOST): a blinded, multicentre, randomised, controlled, phase 2 trial. Lancet. 2021;398(10318):2258–76. Epub 2021 Dec 2. PMID: 34863358 Free PMC article. Clinical Trial. doi:10.1016/S0140-6736(21)02717-3.