
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Herpes Zoster is a viral infection that occurs due to reactivation of the Varicella Zoster virus. A vaccine has been approved for adults aged 50 and above for the prevention of Herpes Zoster and its complications. This study aims to assess the at-risk population’s awareness of the disease and its vaccine, and attitudes and practices toward the vaccine. A quantitative, observational, cross-sectional study was conducted among 420 adults above the age of 50. Non-probability, convenience sampling was used to select participants from public venues. SPSS-25 was used to analyze the data. 64.3% (n = 270) of participants heard of Herpes Zoster. 78.3% (n = 329) did not recognize the link between chickenpox and Herpes Zoster. Multiple linear regression showed that being female, Arab expatriate, or healthcare professional were the only positive predictors of Herpes Zoster knowledge. 14.8% (n = 62) heard of Herpes Zoster vaccine but 96.7% (n = 406) had not taken it. Participants with chronic diseases were 2.064 times more likely to hear about the vaccine than healthy participants (p = 0.026). Multiple linear regression showed that being a healthcare professional was the only significant predictor of Herpes Zoster vaccine knowledge. 28.1% (n = 118) were not willing to take optional vaccines. Those reluctant to take optional vaccines were 26.023 times more likely to take them if recommended by a healthcare professional (p < 0.001). Attitudes toward Herpes Zoster vaccine were generally positive; however, due to lack of knowledge, poor practices were observed. Nationwide campaigns aimed toward at-risk groups can raise awareness on Herpes Zoster and its vaccine, subsequently improving Herpes Zoster vaccination rate.
Introduction
Varicella zoster virus (VZV) is a highly contagious virus that typically infects school-age children during late winter, resulting in chickenpox infection.Citation1 Following primary infection with VZV, the virus remains dormant in the cranial nerves and sensory dorsal root ganglia. Reactivation of the latent virus and its subsequent spread along the sensory nerve to the corresponding dermatomes results in shingles or Herpes Zoster (HZ).Citation2 Henceforth, HZ exclusively affects those with a history of chickenpox infection.Citation3 HZ commonly presents as a vesicular dermatological rash that does not cross the midline that crusts within 10 days.Citation2 The pain associated with the rash can be highly variable; patients might experience hypersensitivity, tingling, aching, or burning pain.Citation2,Citation4 A recent study that evaluated the healthcare economic burden of skin disease has shown that herpes (including HZ) is one of the top 10 most costly causes of skin conditions.Citation5
The incidence of HZ in the general population is estimated to be 4.47 cases per 1000 people in the United States (US) annually and rises to 10.46 per 1000 in those aged above 60.Citation6 Multiple predisposing factors have been linked to developing HZ, including diabetes mellitus, malignancy, immunosuppressive medications, HIV infection, radiotherapy, and TB.Citation7 Additionally, around 95% of immunocompetent individuals above the age of 50 are seropositive for VZV, henceforth are at a higher risk of developing HZ.Citation8 Over the years, there has been a worldwide shift toward an aging population. Bearing in mind that the incidence of HZ increases with age, a greater impact of HZ can be expected.Citation9 Adults over 50 years of age, due to immunosenescence associated with advancing age, are at an increased risk for developing HZ. However, individuals of any age can be at risk, especially those with reduced cell-mediated immunity due to any medication or disease.Citation10
HZ, if not prevented or treated, could add to the elderly patients’ co-morbidities, hence negatively affecting their quality of life.Citation11,Citation12 The most common complication of HZ is postherpetic neuralgia (PHN), which is characterized by the persistence of HZ pain for at least 3 months after the rash outbreak, or the persistence of pain beyond the rash resolution. Other complications include HZ encephalitis, meningitis, and ophthalmic complications, which can be sight-threatening.Citation13,Citation14 Vaccines have helped to reduce morbidity and mortality of multiple diseases across different age groups.Citation15 They have also played a role in the eradication of smallpox and majorly reduced the prevalence of poliovirus.Citation16,Citation17 As such Shringrix, a two-dose recombinant HZ vaccine, was introduced in 2017 aiming to prevent HZ and PHN as well as reduce the severity of the disease in case of breakthrough.Citation18 Shingrix can be administered to the general population as well as immunocompromised patients and is effective up to 90%.Citation19 In the absence of HZ vaccine, it is estimated that around 20 to 30% of the population and about 50% of those living to the age of 85 will develop HZ.Citation20
To our knowledge, no previous study has explored the public’s understanding of HZ and its vaccine in the United Arab Emirates (UAE). Additionally, there is an overall gap in the literature on HZ in the Middle East and North Africa region. With the scarcity of research conducted on this topic in Middle Eastern communities and the emergence of a vaccine with high effectiveness profile in 2017, we aimed to explore the knowledge, attitudes, and practices (KAP) regarding HZ virus and its vaccine in the UAE community among the at-risk group.
Materials and methods
Research design and sampling method
A quantitative, observational, cross-sectional study was conducted to assess the KAP of the UAE population regarding HZ virus and its vaccine. A non-probability, convenience sample of English or Arabic-speaking adults above 50 years of age was selected. The inclusion criteria consisted of UAE citizens and residents aged 50 and above, who spoke either English or Arabic. Visitors to the UAE were excluded from the study. A minimum sample size of 385 was calculated based on 5% marginal error and 50% prevalence, using the following formula: where n = sample size, p = expected prevalence, and SE = sampling error.Citation21 The study was approved by the Research Ethics Committee of the Medical Colleges, at the University of Sharjah (REC-18-12-05-02-S).
Data collection tools and process
A close-ended structured questionnaire was adapted from a similar study conducted in Hong Kong.Citation22 It consisted of 36 close-ended questions split into four sections: demographics (10 questions), knowledge of HZ and its vaccine (15 questions), attitudes (8 questions), and practices regarding the HZ vaccine (3 questions). It consisted of true and false, multiple choice, and Likert scale questions. The questionnaire was developed in English and then translated to Arabic. It was then sent to a language specialist, and feedback was used to fix grammatical mistakes and ensure that the Arabic translation of the questionnaire was accurate. Furthermore, a biostatistician was consulted to ensure content’s reliability and face validity. Both versions (Arabic and English) of the questionnaire were piloted on 20 randomly selected individuals from public venues, who met the inclusion criteria. Following the pilot, the questionnaire was discussed with the pilot group to compare what they understood versus and what the question was trying to inquire. Questions that were ambiguous were clarified to the participants and a clearer structure was subsequently evaluated. Amendments were then made based on the pilot’s feedback, which entailed clarification of a few medical jargons. Data obtained from the pilot was not included in the data analysis. Standardization sessions were held among the researchers to ensure that the participants’ questions were answered in a similar manner and to minimize interviewer bias.
A total of 420 individuals were interviewed by utilizing convenience sampling in public venues (shopping malls, parks, beaches) encompassing Dubai, Sharjah, and the Northern Emirates from February to April 2019. Those who met the inclusion criteria were asked to sign a consent form and were then interviewed using the developed questionnaire. To assure confidentiality, no participant identifying information was collected. Additionally, the collected data were stored in a safe place and disposed of appropriately upon completion of the study. The participants were informed that they can withdraw at any point and their answers would then be discarded immediately.
Statistical analysis
The collected data was entered and coded, then cleaned, and analyzed using IBM Statistical Package for the Social Sciences for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). Frequency analyses were then run for each variable. Inferential statistics tests, including Chi-square, ANOVA, and Student’s t-test were carried out. A knowledge score was also computed, awarding a point when a participant affirmed a true statement or disagreed with a false one. As such, scoring ≥80% was considered as “high”, ≥60% as “intermediate”, ≥40% as “moderate”, ≥20% as “low”, and <20% as “unsatisfactory”. A similar scoring method was used for HZ vaccine knowledge. Five-item Likert scales were collapsed into a three-item scale and awarded 1, 2, or 3 points accordingly when analyzing the participants’ attitudes towards HZ and its vaccine. A multiple linear regression (MLR) was adopted to analyze data after the results of ANOVA and Student’s t-test were statistically significant. MLR was utilized to calculate regression coefficients to compare the relationship between the variables in the outcome variables: knowledge of HZ and its vaccine. The MLR model with entry method was applied to determine which of the demographic variables had the most effect on the knowledge scores. Categorical variables were transformed into dummy variables. Bar graphs, tables, and pie charts were also used to present the study’s findings. A p-value <0.05 was considered to be statistically significant.
Results
Demographics
While 486 adults were approached, only 420 agreed to take part in the study, yielding a response rate of 86.4%. Time constraint was the most reported reason for declining to partake in the study. 54.8% (n = 230) of the participants were male, 61.0% (n = 256) were between the age of 50–55, 58.5% (n = 245) had a bachelor’s degree, and 73.4% (n = 306) had medical insurance. 66.3% (n = 277) of participants reported a history of chronic disease. 52.7% (n = 221) of the respondents stated that they contracted chickenpox. The participants’ demographic characteristics are presented in .
Table 1. Knowledge and attitudes of the participants toward HZ and its vaccine per demographic characteristics.
Knowledge of HZ
The mean HZ virus knowledge was 39.3%. While 64.3% (n = 270) claimed to be aware of HZ, only 1.9% (n = 8) had a knowledge score of 80% and above (). When asked about HZ virus, 48.2% (n = 202) were unaware of its predisposing factors. 35.5% (n = 149) of the participants recognized immunodeficiency as a predisposing factor for HZ. 78.3% (n = 329) of the participants were unable to recognize the link between chickenpox and HZ. Only 18% (n = 39) recognized that having chronic illnesses, advanced age (32.7%, n = 71), and stress (41.9%, n = 91) were predisposing factors for HZ. Only 26.7% (n = 111) recognized that HZ is not transmitted through direct contact. 58.7% (n = 246) of the participants correctly identified rash as a clinical feature of HZ. However, other symptoms such as blisters (29.1%, n = 122) and neuropathic pain (16.5%, n = 69) were not recognized by the majority of participants while fever (25.3%, n = 106) was incorrectly reported as a clinical feature of HZ by some. 39.0% (n = 164) thought that HZ is curable. Participants who had heard of HZ did so through friends and family (50.0%, n = 135), knew someone who had HZ (38.1%, n = 103), or through the internet and social media (14.8%, n = 40). Postgraduates, with an average knowledge score of 41.8%, were found to be more knowledgeable regarding HZ disease compared to other educational groups (p = 0.002). MLR showed that being female, an Arab expatriate, or healthcare professional (HCP) were the only positive predictors of HZ knowledge while being unaware of their history of chickenpox was a negative predictor ().
Table 2. Multiple linear regression analysis of the factors influencing knowledge of HZ and its vaccine.
Knowledge of HZ vaccine
The average HZ vaccine knowledge level was 19.6%. While 14.8% (n = 62) of the participants had heard of HZ vaccine, only 2 participants were able to answer all knowledge questions correctly. Furthermore, 71.2% (n = 299) achieved a score of less than or equal to 20%. Participants who had heard of the HZ vaccine did so through friends and family (40.3%, n = 25), healthcare professionals (30.6%, n = 19), and the internet or social media (22.6%, n = 14).
Only 20.0% (n = 84) were able to recognize that HZ vaccine is a preventive measure and not a treatment for HZ infection. 63.4% (n = 266) did not recognize that the HZ vaccine can dramatically reduce the incidence of the disease. 89.5% (n = 372) were not aware that those infected with HZ can still get vaccinated. Additionally, 80.3% (n = 335) did not know that those infected with chickenpox as children need to be vaccinated for HZ. Only 13.3% (n = 56) correctly recognized that adults aged 50 and above should receive the HZ vaccine. Participants with chronic diseases were 2.064 times (95% CI: 1.078–3.953) more likely to hear about HZ vaccine than healthy participants (p = 0.026). MLR showed that being a healthcare professional was the only significant predictor of HZ vaccine knowledge ().
Attitudes and practice of HZ vaccination
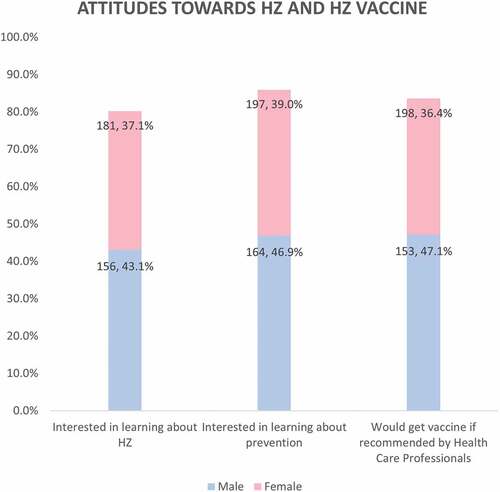
The majority of the participants (96.7%, n = 406) have not received the HZ vaccine. However, 86.2% (n = 361) were willing to learn more about methods of HZ prevention. In addition, 83.6% (n = 351) of the participants would get the HZ vaccine if recommended by an HCP (). Only 23.9% (n = 100) were concerned about the cost of HZ vaccine. Those who had medical insurance were 1.257 times (95% CI: 1.012–1.562) more likely not to worry about the cost (p = 0.024).
Figure 1. Participants’ attitudes toward HZ and its vaccine.
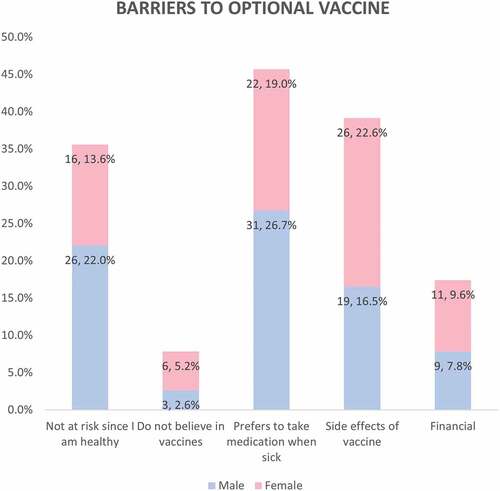
Only 28.1% (n = 118) of participants were generally not willing to take optional vaccines. When exploring the main barriers among those who were vaccine hesitant, 45.7% (n = 53) preferred taking medications instead of vaccines (). Those reluctant to take optional vaccines were 26.023 times (95% CI: 8.911–77.049) more likely to take optional vaccines if recommended by an HCP (p < 0.001).
Figure 2. Barriers to optional vaccination in participants who are vaccine hesitant.
Discussion
In the Middle East and North Africa region, the topic of HZ has not been explored comprehensively. While multiple international studies have explored the effects of HZ vaccine on the at-risk population and the reduction in economic burden secondary to vaccine administration, limited research has explored the willingness of the population to take the vaccine as well as the barriers to vaccination.
There was an overall lack in knowledge of the UAE population regarding HZ. Just over 60% were aware of HZ, whereas HZ vaccine knowledge was limited with just under 15% aware of the vaccine. This contrasts with a study conducted in South Korea where more than 80% and almost half of the subjects were knowledgeable regarding HZ and HZ vaccine, respectively.Citation23 Additionally, a study conducted in the US found that gaining a better understanding of HZ and its vaccine was a leading factor in participants’ willingness to take the vaccine.Citation24 Hence, public health awareness campaigns that underscore the importance of vaccination as well as HZ vaccine recommendations, while underlining the HZ associated sequalae, could essentially improve the willingness to take the HZ vaccine.
While many claimed to be aware of HZ, less than 2% were able to answer most of the questions correctly. Additionally, about 80% of the participants were unable to recognize the link between chickenpox and HZ. This could be related to the fact that more than 60% of the participants heard of HZ through either friends and family or the internet, which are not the most reliable sources of information. Furthermore, postgraduates were more knowledgeable regarding HZ than others, which is in accordance with a Hong Kong study, where higher level of education was associated with better HZ knowledge.Citation22 This elucidates the importance of education, as well as providing the public with primary resources of information to minimize the spread of distorted facts and falsity.
Interestingly, participants with chronic diseases were twice more likely to have heard about HZ vaccine than healthy participants, which is in line with the Hong Kong study.Citation22 This could be secondary to increased interaction with HCPs leading to discussions about immunocompromised state and diseases associated with it, such as HZ. It might also be due to picking up interest in learning about other chronic diseases from health forums and support group blogs. Seeking information regarding HZ ultimately leads to learning about methods of prevention including vaccination.
The vaccination rates for HZ are extremely low across multiple geographical regions as demonstrated by multiple studies. In the UAE and Hong Kong, only around 3% have received the HZ vaccine and only around 8% in the US.Citation22,Citation25 In our study, the overwhelming majority were not aware that the vaccine is in fact recommended for individuals above 50 years of age. This coupled with the fact that more than 80% of the participants showed positive attitudes and were willing to take the vaccine if recommended by an HCP, provides a possible framework to encourage the at-risk individuals to take the vaccine.
While a South Korean study illustrated that the cost of HZ vaccine was a major barrier to vaccination,Citation23 we found that cost was not a barrier in the UAE. On the other hand, we found that just under half of our participants preferred to take medications over being vaccinated to resolve HZ. Upheaving the overall knowledge of the population regarding HZ would emphasize the importance of the Shingrix vaccine in HZ prevention. We also found that about 60% of the participants were willing to take optional vaccines especially when recommended by an HCP. With the current state of the world and in light of the COVID-19 pandemic, we expect better awareness regarding the importance of vaccines and an increased willingness to take some optional vaccines, such as influenza.Citation26,Citation27
Limitations
Convenience sampling was used to recruit participants, which might affect the generalizability of the results. Recall bias is another limitation of this study. Participants were asked to self-report about previous history of chickenpox infection. Although interviews took place all over the seven Emirates, they were not represented equally nor were they stratified according to the population distribution. However, we do not expect this to affect the validity of the results as the UAE is a metropolitan country with majority of the participants being from the largest Emirates, which are the commercial and cultural hubs of the UAE.
Conclusion
Although the participants’ awareness of HZ and its vaccine were substandard, the observed attitudes were positive as participants were willing to protect themselves from HZ via a vaccine if recommended by an HCP. Nationwide campaigns addressing the disease, its complications and the importance of the HZ vaccine, could encourage the target population to improve their willingness to take the vaccine. More importantly, HCPs should be encouraged to recommend the HZ vaccine to those above 50 years of age.
Author contributions
All authors collected and curated the data, performed the formal analysis and data visualization. H.J.B. supervised the project and critically reviewed the process. All authors reviewed the manuscript prior to submission.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Blair RJ. Varicella Zoster virus. Pediatr Rev. 2019;40:375–7. doi:10.1542/pir.2017-0242.
- Cohen JI. Clinical practice: Herpes zoster. N Engl J Med. 2013;369:255–63. doi:10.1056/NEJMcp1302674.
- Freer G, Pistello M. Varicella-Zoster virus infection: natural history, clinical manifestations, immunity and current and future vaccination strategies. New Microbiologica. 2018;41(2):95–105.
- Schmader K. Herpes Zoster. Clin Geriatr Med. 2016;32:539–53. doi:10.1016/j.cger.2016.02.011.
- Lim HW, Collins SAB, Resneck JS, Bolognia JL, Hodge JA, Rohrer TA, Van Beek MJ, Margolis DJ, Sober AJ, Weinstock MA, et al. The burden of skin disease in the United States. J Am Acad Dermatol. 2017;76:958–72.e2. doi:10.1016/j.jaad.2016.12.043.
- Johnson BH, Palmer L, Gatwood J, Lenhart G, Kawai K, Acosta CJ. Annual incidence rates of herpes zoster among an immunocompetent population in the United States. BMC Infect Dis. 2015;15:1–5. doi:10.1186/s12879-015-1262-8.
- Babamahmoodi F, Alikhani A, Ahangarkani F, Delavarian L, Barani H, Babamahmoodi A. Clinical manifestations of herpes zoster, its comorbidities, and its complications in North of Iran from 2007 to 2013. Neurol Res Int. 2015;2015:10–13. doi:10.1155/2015/896098.
- Johnson RW, Alvarez-Pasquin M-J, Bijl M, Franco E, Gaillat J, Clara JG, Labetoulle M, Michel J-P, Naldi L, Sanmarti LS, et al. Herpes zoster epidemiology, management, and disease and economic burden in Europe: a multidisciplinary perspective. Ther Adv Vaccines. 2015;3:109–20. doi:10.1177/2051013615599151.
- Wolfson LJ, Daniels VJ, Altland A, Black W, Huang W, Ou W. The impact of varicella vaccination on the incidence of varicella and Herpes Zoster in the United States: updated evidence from observational databases, 1991-2016. Clin Infect Dis. 2020;70:995–1002. doi:10.1093/cid/ciz305.
- Lal H, Cunningham AL, Godeaux O, Chlibek R, Diez-Domingo J, Hwang S-J, Levin MJ, McElhaney JE, Poder A, Puig-Barberà J, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older Adults. N Engl J Med. 2015;372:2087–96. doi:10.1056/nejmoa1501184.
- Pickering G, Gavazzi G, Gaillat J, Paccalin M, Bloch K, Bouhassira D. Is herpes zoster an additional complication in old age alongside comorbidity and multiple medications? Results of the post hoc analysis of the 12-month longitudinal prospective observational ARIZONA cohort study. BMJ Open. 2016;6:1–8. doi:10.1136/bmjopen-2015-009689.
- Curran D, Oostvogels L, Heineman T, Matthews S, McElhaney J, McNeil S, Diez-Domingo J, Lal H, Andrews C, Athan E, et al. Quality of life impact of an adjuvanted recombinant zoster vaccine in adults aged 50 years and older. Journals Gerontol - Ser a Biol Sci Med Sci. 2019;74:1231–38. doi:10.1093/gerona/gly150.
- Koshy E, Mengting L, Kumar H, Jianbo W. Epidemiology, treatment and prevention of herpes zoster: a comprehensive review. Indian J Dermatol Venereol Leprol. 2018;84:251–62. doi:10.4103/ijdvl.IJDVL_1021_16.
- Stein AN, Britt H, Harrison C, Conway EL, Cunningham A, MacIntyre CR. Herpes zoster burden of illness and health care resource utilisation in the Australian population aged 50 years and older. Vaccine. 2009;27:520–29. doi:10.1016/j.vaccine.2008.11.012.
- Ciabattini A, Nardini C, Santoro F, Garagnani P, Franceschi C, Medaglini D. Vaccination in the elderly: the challenge of immune changes with aging. Semin Immunol. 2018;40:83–94. doi:10.1016/j.smim.2018.10.010.
- Koff WC, Schenkelberg T. The future of vaccine development. Vaccine. 2020;38:4485–86. doi:10.1016/j.vaccine.2019.07.101.
- Martinez M, Shukla H, Nikulin J, Mbaeyi C, Jorba J, Ehrhardt D. Progress toward poliomyelitis eradication — Afghanistan, January 2018–may 2019. MMWR Morb Mortal Wkly Rep. 2019;68:729–33. doi:10.15585/mmwr.mm6833a4.
- Rosamilia LL. Herpes Zoster presentation, management, and prevention: a modern case-based review. Am J Clin Dermatol. 2020;21:97–107. doi:10.1007/s40257-019-00483-1.
- James SF, Chahine EB, Sucher AJ, Hanna CS. The new adjuvanted recombinant Herpes Zoster vaccine. Ann Pharmacother. 2018;52:673–80. doi:10.1177/1060028018758431.
- John AR, Canaday DH. Herpes Zoster in the older adult. Infect Dis Clin North Am. 2017;31:811–26. doi:10.1016/j.idc.2017.07.016.
- Macfarlane SBJ. Conducting a descriptive survey: 2. choosing a sampling strategy. Trop Doct. 1997;27:14–21. doi:10.1177/004947559702700108.
- Lam ACY, Chan MY, Chou HY, Ho SY, Li HL, Lo CY, Shek KF, To SY, Yam KK, Yeung I. A cross-sectional study of the knowledge, attitude, and practice of patients aged 50 years or above towards herpes zoster in an out-patient setting. Hong Kong Med J. 2017;23:365–73. doi:10.12809/hkmj165043.
- Yang TU, Cheong HJ, Song JY, Noh JY, Kim WJ. Survey on public awareness, attitudes, and barriers for herpes zoster vaccination in South Korea. Hum Vaccines Immunother. 2015;11:719–26. doi:10.1080/21645515.2015.1008885.
- Baalbaki NA, Fava JP, Ng M, Okorafor E, Nawaz A, Chiu W, Salim A, Cha R, Kilgore PE. A community-based survey to assess knowledge, attitudes, beliefs and practices regarding Herpes Zoster in an urban setting. Infect Dis Ther. 2019;8:687–94. doi:10.1007/s40121-019-00269-2.
- Lee TJ, Hayes S, Cummings DM, Cao Q, Carpenter K, Heim L, Edwards H. Herpes zoster knowledge, prevalence, vaccination rate by race. J Am Board Fam Med. 2013;26:45–51. doi:10.3122/jabfm.2013.01.120154.
- Record flu vaccines in 2020 to protect Australians | health portfolio ministers. [Accessed 2021 July 12]. https://www.health.gov.au/ministers/the-hon-greg-hunt-mp/media/record-flu-vaccines-in-2020-to-protect-australians.
- Bachtiger P, Adamson A, Chow JJ, Sisodia R, Quint JK, Peters NS. The impact of the COVID-19 pandemic on the uptake of influenza vaccine: UK-wide observational study. JMIR Public Heal Surveill. 2021:7. doi:10.2196/26734.