?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Nigeria has one of the highest measles burdens in the world. While measles-containing vaccine is proven to be effective in reducing measles cases, empirical studies on the correlation between measles incidence and measles vaccine coverage in Nigeria has been limited. The aim of this study was to conduct a detailed analysis on measles incidence, measles vaccine coverage, and their correlation between 2012 and 2021. A retrospective observational study was conducted based on the Integrated Disease Surveillance and Response (IDSR) data for the measles incidence in each Nigerian state over time, District Health Information System, V.2 (DHIS2) and Nigeria Demographic and Health Survey (DHS) for the coverage of the first dose of measles containing vaccine (MCV1) over time (2012–2021). We observed the trend of measles incidence and measles vaccine coverage, as well as their correlation. Out of the study period from 2012 to 2021, we found that the majority of measles outbreaks occurred in the northeastern states in recent years after 2019, especially in Borno state, where Boko Haram insurgency has negatively impacted health service delivery, including routine vaccination. We observed a significant negative correlation between measles incidence and measles vaccine coverage across Nigerian states. However, there was no sudden drop in measles vaccine coverage before the recent outbreak in Borno state in 2019, which could be due to various factors other than the overall vaccine coverage.
KEYWORDS:
Introduction
Measles is a highly contagious infectious disease caused by the Measles virus. It is an RNA virus belonging to the genus Morbillivirus and family Paramyxoviridae. Out of 10 people without protection against measles in a room, nine of them will contract the virus.Citation1 The basic reproduction number, defined as the average number of secondary cases of an infectious disease arising from a typical case in a totally susceptible population, for measles is 12 to 18, which is quite high.Citation2
Prior to the introduction of measles vaccines, over 2 million people died annually due to measles infection. After the introduction of the measles vaccine, the number of deaths due to measles decreased substantially to about 100,000, which is only 5% of the total deaths before the vaccine introduction.Citation3
However, there still were over 870,000 measles cases and over 200,000 deaths due to measles worldwide in 2019.Citation4 Despite initial progress and impact, recent measles vaccine miscommunication has resulted in vaccine hesitancy and rejection which has translated into measles incidence increasing from 2016 to 2019 by 50% globally.Citation4 Meanwhile, world coverage of measles vaccine has been stagnant for the past 5 years at around 85%.Citation5
Nigeria has one of the highest measles burdens in the world. In 2021, Nigeria had the world’s largest number of measles cases in any country: over 10,000 cases based on data from the Integrated Disease Surveillance and Response (IDSR) were recorded. However, measles vaccination coverage remains suboptimal and stagnant since 1990, 53% in 1990 to 54% in 2018.Citation6
There has been a limited number of studies conducted on the measles incidence and its link with measles vaccination coverage in Nigeria. Ibrahim et al. (2019) studied the trend of measles incidence and fatality rate from 2012 to 2016 in Nigeria and found a high measles burden especially in the northern region of the country.Citation7 They emphasized the importance of routine immunization, yet they did not show the empirical evidence on the correlation between measles incidence and vaccination coverage.
Baptiste et al. (2021) studied the trend of measles incidence between 2008 and 2018, as well as measles vaccine coverage.Citation8 Consistent with Ibrahim et al. (2019), Baptiste et al. (2021) also found the high burden of measles in the northern part of Nigeria. Furthermore, they studied the trend of measles vaccine coverage over years and revealed that it was suboptimal. Nevertheless, they did not investigate the correlation between the measles incidence and vaccination coverage.
In this study, we conducted detailed analysis on the measles incidence, measles vaccine coverage, and investigated their correlation between 2012 and 2021. In particular, we identified the geographical zones within Nigeria that have the largest burden of measles incidence and evaluated the correlation between measles incidence and measles vaccine coverage using two different datasets on the coverage.
Methods
Setting
Nigeria is comprised of 36 states and 1 Federal Capital Territory (FCT), which belong to one of 6 zones: North Central zone (NCZ), North East zone (NEZ), North West zone (NWZ), South East zone (SEZ), South South zone (SSZ), and South West zone (SWZ).
Data
We used four datasets for the analysis.
Integrated disease surveillance and response (IDSR)
We used IDSR to track the monthly aggregate measles cases in each state between 2012 and 2021, as well as the monthly aggregate measles cases in each local government areas (LGA) in all the states between 2014 and 2021. The IDSR data is routinely collected across the country by the Nigeria Center for Disease Control (NCDC) in collaboration with the 36 State Ministries of Health and FCT department of health, and the organization provided access to this data. IDSR tracks 41 diseases of public health significance using immediate case-based notification (IDSR001), weekly notification (IDSR002) and monthly notification forms (IDSR003).Citation9,Citation10 Data used in this study was retrieved from the NCDC and contained aggregate measles incidence data compiled on a monthly basis between 2012 and 2021.
District health information system, V.2 (DHIS2)
We used DHIS2 to track the monthly measles vaccination coverage in each state. In this study, we focused on the first dose of measles vaccine (MCV1). We also used this dataset to examine the monthly vaccination coverage in all the LGAs in Borno state. The coverage information in DHIS2 is based on the data reported from each health facility. Each health facility has a target population to reach for the measles vaccination coverage, and this target population is compared with the actual number of vaccines administered within the catchment area of each health facility. Thus, it is possible for the coverage to exceed 100% as the target population is based on the census data, which might not necessarily reflect the accurate population as the last census was conducted in 2006. Also, if the estimated number of the target population is inaccurate, the vaccination coverage might not necessarily reflect the actual coverage.
DHIS2, a platform developed by the University of Oslo and in use in more than 60 countries, is the platform used to manage the country’s routine health information system, generally known as the national health management information system (NHMIS).Citation11 The NHMIS collects data from all health facilities across the country monthly, including number of measles immunizations completed.
Nigeria demographic and health survey (DHS)
We used the 2013 and 2018 Nigeria DHS data to estimate the measles vaccination coverage in each state. The DHS is a nationally representative household survey, conducted every 5 years in developing countries. The first edition of the study in Nigeria was in 1990.
Unlike DHIS2 data, the DHS data on the coverage was based on the household visits of nationally representative sample. While these data might closely reflect the actual vaccination coverage, this DHS data has two data points: one in 2013 and another in 2018, while DHIS2 data has monthly data points.
Population data
The population data were based on 2006 population census data as well as projected populations in 2016 calculated by the National Bureau of Statistics. The data are available publicly online.Citation12,Citation13 We projected the population between 2012 and 2021 in each state under the assumption that the population grows at the same growth rate per year in each state.
Main variables
One of the main variables on which we focused in this study was the measles incidence: the number of measles cases per 1 million population. Measles incidence, calculated as the monthly aggregated data on measles cases obtained from IDSR divided by the population estimate in each state in each year.
Another main variable was the coverage of the first dose of measles containing vaccine (MCV1). We used DHIS2 data for observing the pattern of coverage in each state over time, while we used both DHIS2 data and DHS data for evaluating the correlation between the measles incidence and measles vaccination coverage. In Nigeria, it is recommended that children receive MCV1 at the age of 9 months.
Cost required to reach 80% of measles vaccine coverage in each state was also assessed. For the unit cost of delivering the measles vaccine per dose, the existing literature gathered at Immunization Cost Action Network (ICAN) cost catalog as well as the United Nations International Children’s Emergency Fund (UNICEF) vaccine price data.Citation14 The delivering cost of measles vaccination per dose is estimated to be $0.638.
Estimation strategy
To estimate the correlation between measles vaccination coverage and the measles incidence, the simple Ordinary least-squares (OLS) regression was employed. The correlation was estimated in the following equation:
where is the measles incidence per 1 million population in zone i at time t,
is the coverage in zone i at time t-1 (previous time). By using the lagged variable of the vaccination coverage and its correlation with the measles incidence, we mitigate the risk of reversal causality. We also controlled for any unobservable characteristics in each year and in each zone by including dummy variables. For the measles vaccine coverage, we used two different datasets separately: one was DHIS2 data for the monthly information, and another was DHS data for the coverage information for year 2013 and for year 2018. For the coverage based on the DHS data, we predicted the yearly vaccination coverage for other years besides 2013 and 2018, assuming the same annual growth of the coverage. We analyzed the correlation using these two datasets separately for the robustness check.
Finally, we also estimated the cost required for each state to reach 80% of the measles vaccination coverage. To estimate it, we used the DHS data for the baseline measles vaccination coverage, the current total population, and the unit of delivering the measles vaccine per dose.
Results
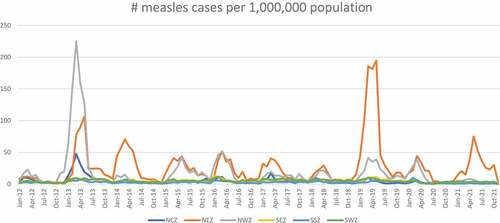
During the period studied a clear seasonal pattern was observed from January to July, when measles cases surged (). Measles cases were dominantly concentrated in northeast and northwest zones. In the last 10 years, there were two large measles outbreaks in Nigeria—one in 2013 and another in 2019. In 2013, the largest surge was in northwest zone (over 200 cases per 1 million population), while in 2019, it was in northeast. Indeed, in the last 3 years, the surge has been concentrated in northeast zone (almost 200 cases per 1 million population).
Figure 1. Measles cases per 1 million population by zone.
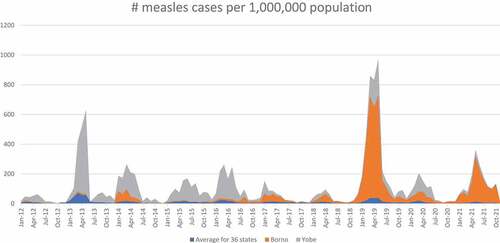
Several states have had a surge almost yearly (). Yobe state (grey) has been having a surge almost every year since 2012 with the peak in 2013 at more than 500 cases per 1 million population. On the other hand, Borno state (orange) has had large surges in the last 3 years (since 2019) with the peak in 2019 at almost 700 cases per 1 million population. Both Yobe and Borno states are in northeast zone.
Figure 2. Measles cases per 1 million population by state.
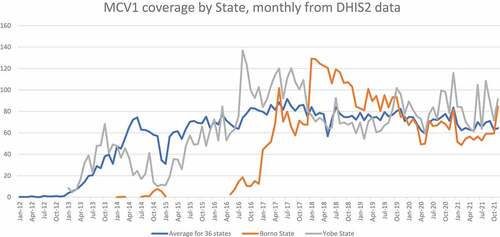
presents the trend of the measles vaccination coverage by state over time. Because of the high volume of measles cases per 1 million population in Yobe and Borno states over time, these two states were highlighted in . Borno state has had one of the lowest levels of the vaccination coverage until 2016. The highest coverage observed in Borno state until 2016 was 18.5% in 2016. Although the coverage rate improved in 2018 for Borno state, it has again assumed a downward trend since then: it dropped from over 100% in 2018 to less than 50% in 2020. Yobe state also has had consistently low level of vaccination coverage throughout, except in 2016 and 2017 when the state reached over 100%, as compared to other states.
Figure 3. Measles vaccination (MCV1) coverage by state.
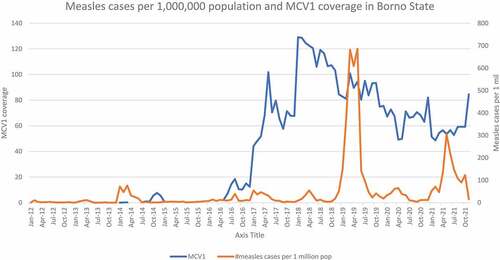
Because Borno state had the largest measles cases over the past several years, presents the trend of measles cases per 1 million population and MCV1 coverage only in Borno state over time. We did not observe a clear relationship between the measles cases and MCV1 coverage in Borno state. The MCV coverage improved substantially from less than 20% to 100% in the mid-2016, while we still observed the surges in the measles cases every year. From 2018, the MCV1 coverage started to decline from 100% to 50% in 2020 but still kept the high level of coverage around the beginning of 2019 when the largest surge occurred in the past 10 years: 700 cases per 1 million population.
Figure 4. Measles incidence and measles vaccination (MCV1) coverage in Borno State.
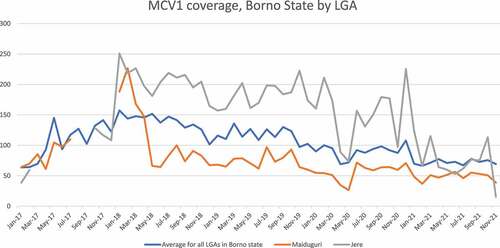
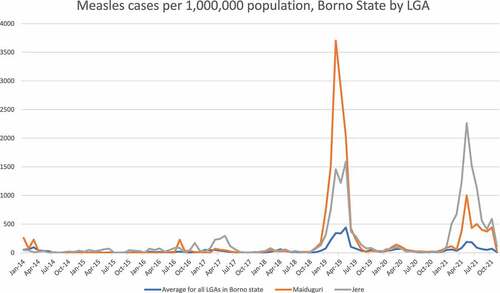
Appendix A presents the trend of measles cases only in Borno state. As observed in , the large surges in measles cases in Borno state occurred from 2019 to 2022. In 2019, the majority of cases were concentrated in Maiduguri local government area (LGA) (dark gray) which observed more than 3500 cases per 1 million population in 2019. The most recent outbreak occurred in 2021 and was concentrated in Jere LGA (blue): over 2000 cases per 1 million. Maiduguri is where the state capital is located and Jere is the neighboring LGA to Maiduguri LGA. Both LGAs have large concentrations of internally displaced person camps.
Appendix B presents the trend of measles vaccination coverage in Borno state. Because we observed high number of measles outbreaks in Maiduguri and Jere LGA, we assessed the MCV1 coverage in these 2 LGAs. Maiduguri LGA consistently presented low level of MCV1 coverage over time as compared to other LGAs, although the coverage reached almost 100% around the time of the largest outbreak in 2019. Jere LGA seemed to have performed better than Maiduguri LGA over the years: the MCV1 coverage exceeds 100% in most years. However, in recent years, the coverage in Jere LGA has been low.
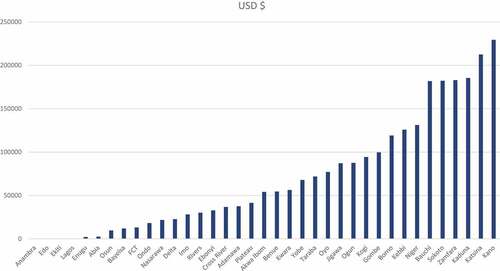
presents a cost assessment for each state in order to reach 80% of MCV1 coverage. The result depended on the combination of the population of children eligible for vaccination and the baseline coverage of MCV1. The costs required to achieve 80% coverage for many of the southern states were low because of the lower population as well as the higher vaccination coverage. Four states (Anambra, Edo, Ekiti, and Lagos states), all of which are in the south, did not require any additional budget to reach 80% of MCV1 coverage as they have already reached the level. Similarly, many northern states required higher costs due to the higher population and the current low vaccination coverage status. Four states that needed the highest budget were all in the north: Zamfara, Kaduna, Katsina, and Kano. They require the budget of USD183,000 to 229,000 to reach 80% of MCV1 coverage.
Figure 5. Cost required to reach 80% of MCV2 coverage in each state.
presents the results for the regression analysis on the relationship between measles vaccination coverage in the previous year and the number of measles cases per 1 million population, according to yearly and monthly data (Panel A and Panel B), respectively. We found that the higher measles vaccination coverage of the previous year and month was significantly and negatively correlated with the measles cases in the present year and month.
Table 1. Correlation between MCV coverage and measles cases (DHS data for MCV1, yearly).
Discussion
This paper demonstrated the pattern of measles incidence, measles vaccination coverage, and their correlation across Nigerian states in the 10 years between 2012 and 2021. Overall, our study was, to our knowledge, the first to evaluate in depth, the measles incidence and its correlation with measles vaccine coverage in Nigeria.
We found that Nigeria experienced measles outbreaks every year from January for about 6 months with peak incidence around April each year. Two largest outbreaks in Nigeria occurred in 2013 and in 2019. Measles outbreaks were predominantly concentrated in the northern region of the country. Since 2019, however, most measles outbreaks occurred in the northeastern states, especially in Borno state. Based on the monthly aggregate measles data, the biggest measles outbreak in the past 10 years was the one in 2019 with an incidence exceeding 600 new cases per million population only in Borno state monthly from March to May 2019, while the second-largest outbreak occurred in Yobe state, another northeastern state, with about 250 cases per 1 million population as of April 2019. The average monthly incidence in Nigeria during this period was about 40 cases per 1 million population. Our findings around the measles incidence were consistent with the previous study.Citation8
In 2011, African Region of the World Health Organization, including Nigeria, endorsed the 2020 elimination goal which targets to reach the vaccine coverage of 95% at national and district level, as well as to reduce the annual measles incidence to less than 1 case per 1 million population.Citation15 The current measles incidence is unfortunately much higher than this target.
Although Borno state had low level of measles vaccination coverage until 2017, the coverage improved substantially during 2018. However, the coverage has been decreasing since then. The measles outbreak of 2019 in Borno state occurred when the vaccination coverage was not as low as before 2017 but it was decreasing.
We found that there was a significant correlation between the measles vaccination coverage at month (year) t and measles incidence in the following month (year) t +1. The lower the vaccination coverage was, the higher the measles incidence that was observed. This finding is consistent with other studies.Citation16
The budget required to achieve 80% of measles vaccination coverage in each state differed substantially by state. Generally, the northern states needed much more budget than the southern states per year, due to the higher unvaccinated population. Kano and Katsina states, both in NWZ, are the two states that required the largest budget – over 200,000 USD. In our analysis, we did not differentiate the unit cost for vaccine delivery according to geography due to the lack of data availability. However, the landmass of the states is usually much larger among northern states than southern states. This difference might cause the differential unit cost of vaccine delivery according to the geography to be further widened between northern and southern states. Future work should incorporate the differential unit cost to estimate the budget more accurately.
Overall, although we found the negative correlation between measles vaccination coverage and measles incidence, we did not observe the substantial/sudden drop in the measles vaccination coverage in Borno state that could have explained one of the largest measles outbreaks in the past decade in Nigeria, which occurred in 2019. This result implies the difficulty of predicting the measles outbreaks from the monthly measles vaccination coverage and population density at the state and LGA level, or it could as well be due to the poor availability of routine data.
Other factors might contribute to the sudden measles outbreaks. For example, the requirement for herd immunity is not only due to the population-wide vaccine coverage, but also due to the relatively-homogeneous vaccine-protected population. If a particular part of Borno state has an extremely low vaccine coverage, for example, this place could then serve as foci of outbreaks.
Another reason for this inconsistency could be that the vaccination coverage data available for this study were administrative rather than survey and might have been subject to reporting bias. Furthermore, the compliance with disease surveillance reporting has been observed to be poor across private health facilities across Nigeria, despite catering to a larger proportion of the population.Citation10 Additionally, the measles prevalence data reported the cases, regardless of the age group. The transmission of the measles might have been different by the age group. However, the lack of data prevented us from conducting this analysis.
One thing to note, however, is that one of the main contributing states for the high measles incidence in Nigeria, Borno state, has been heavily impacted by the Boko Haram insurgency which is trying to establish an Islamic Caliphate in the Sahel region. Armed conflicts due to the violent activities of Boko Haram led to the reduction of the vaccination uptake.Citation17 The negative impact on vaccination is noted to have contributed to the reemergence of the wild polio virus in the state in 2016.Citation18 Such armed conflicts also forced people to move out of their home to camps where there is significant clustering of people. In the state capital of Borno state, Maiduguri Municipal Council, as well as in the neighboring area including Jere LGA, many people temporarily settled in internally displaced person camps due to the insecurity in their usual domicile. From our analysis, we observed a high measles incidence in these local government areas. On many occasions, it is challenging to maintain the high level of vaccination status in such camps, and this situation might have contributed to the consistent and high level of measles outbreaks in Borno state, especially around Maiduguri metropolis.
Yobe state shares much similarity with Borno state: low vaccination coverage, high measles prevalence, and been heavily affected by the Boko Haram insurgency. While our discussion is dominantly around the situation in Borno state, general statements we made here on Borno state can be applied to Yobe state.
Conclusion
Consistent with the previous study by Baptiste et al. in 2021, we found that northern states, especially Borno state in the NEZ, bore the largest burden of measles in Nigeria, in terms of measles incidence. We also confirmed the significant and negative correlation between the measles vaccine coverage and measles incidence, although we did not observe any drop in vaccine coverage right before the surges in measles incidence. While the NEZ has the largest measles incidence, many states in the NWZ might require more finance to reach the 80% of vaccination coverage, due to the low baseline coverage and larger population to cover. Borno state might have been observing the surges in measles outbreaks due to the Boko Haram insurgences which led many people to settle temporarily in the camps, which makes it difficult to maintain the up-to-date measles vaccine status among them.
Acknowledgments
We would like to thank the Nigeria Center for Disease Control (NCDC) team who facilitated access to the IDSR data on measles for the country. This includes the Director General, Dr Ifedayo Adetifa, the Director, Prevention Programs & Knowledge Management, Dr Chinwe Ochu and Dr Grace Esebanmen. We thank other knowledge experts from the NCDC, Dr Clement Daam and Dr Bola Lawal. We also appreciate the Demographic and Health Survey (DHS) which provided access to the DHS surveys in Nigeria on request.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- CDC Global. 2022. Global measles outbreaks. Cent Dis Control Prev [Internet]. [accessed 2022 Aug 3]. https://www.cdc.gov/globalhealth/measles/data/global-measles-outbreaks.html
- Guerra FM, Bolotin S, Lim G, Heffernan J, Deeks SL, Li Y, Crowcroft NS. The basic reproduction number (R0) of measles: a systematic review. Lancet Infect Dis. 2017;17(12):1–8. doi:10.1016/S1473-3099(17)30307-9.
- Moss WJ. Measles. Lancet. 2017;390(10111):2490–2502. doi:10.1016/S0140-6736(17)31463-0.
- Tanne JH. Measles cases and deaths are increasing worldwide, warn health agencies. Bmj. 2020;371:m4450. doi:10.1136/bmj.m4450.
- WHO, UNICEF. 2021. Immunization, measles (% of children ages 12-23 months). Data [Internet]. [accessed 2022 Aug 15]. https://data.worldbank.org/indicator/SH.IMM.MEAS
- ICF International, Maryland USA. STATcompiler. [Internet]. [accessed 2022 Aug 15]. https://www.statcompiler.com/en/
- Ibrahim BS, Usman R, Mohammed Y, Datti Z, Okunromade O, Abubakar AA, Nguku PM. Burden of measles in Nigeria: a five-year review of casebased surveillance data, 2012-2016. Pan Afr Med J. 2019;32(Suppl 1):5. doi:10.11604/pamj.supp.2019.32.1.13564.
- Jean Baptiste AE, Masresha B, Wagai J, Luce R, Oteri J, Dieng B, Bawa S, Ikeonu OC, Chukwuji M, Braka F, et al. Trends in measles incidence and measles vaccination coverage in Nigeria, 2008–2018. Vaccine. 2021;39:C89–C95. doi:10.1016/j.vaccine.2021.03.095.
- Isere EE, Fatiregun AA Measles case-based surveillance and outbreak response in Nigeria; an update for clinicians and public health professionals. Ann Ib Postgrad Med. 2014;12:15–21.
- Makinde OA, Odimegwu CO. Compliance with disease surveillance and notification by private health providers in South-West Nigeria. Pan Afr Med J. 2020; 35(114). [Internet][accessed 2020 Apr 13. doi:10.11604/pamj.35.114.21188
- Meribole EC, Makinde OA, Oyemakinde A, Oyediran KA, Atobatele A, Fadeyibi FA, Azeez A, Ogbokor D, Adebayo O, Adebayo W, et al. The Nigerian health information system policy review of 2014 : the need, content, expectations and progress. Health Inf Libr J. 2018;35(4):285–297. doi:10.1111/hir.12240.
- National Bureau of Statistics. 2006. National results: population by state and by sex [Internet]. [accessed 2022 Feb 21]. https://web.archive.org/web/20110519235026/http:/www.population.gov.ng/files/nationafinal.pdf
- National Bureau of StatisticsDemographic statistics nulletin. 2018.
- Immunization Cost Action Network (ICAN). Cost Catalogue. ImmunizationEconomics.org. [Internet]. [accessed 2022 Aug 15]. https://immunizationeconomics.org/ican-idcc
- WHO Regional Committee for Africa. Sixty-First session of the WHO Regional Committee for Africa. WHO Reg Off Afr [Internet]. [accessed 2022 Jan 31]. https://www.afro.who.int/about-us/governance/sessions/sixty-first-session-who-regional-committee-africa
- Wang R, Jing W, Liu M, Liu J. Trends of the global, regional, and national incidence of measles, vaccine coverage, and risk factors in 204 countries from 1990 to 2019. Front Med. 2022;8:798031. doi:10.3389/fmed.2021.798031.
- Sato R. Effect of armed conflict on vaccination: Evidence from the Boko haram insurgency in northeastern Nigeria. Confl Health. 2019;13(1):49. doi:10.1186/s13031-019-0235-8.
- Zoakah AI, Adebiyi AO, Ashikeni M, Makinde OA; . Epidemiological Society of Nigeria (EPiSON)Wild poliovirus in Nigeria. Lancet Infect Dis. 2016;16(11):1224. doi:10.1016/S1473-3099(16)30391-7.
Appendix Appendix A.
Measles cases in Borno State
Appendix B.
MCV coverage in Borno State