
ABSTRACT
COVID-19 vaccination in the Democratic Republic of the Congo (DRC) began in April 2021. A month later, most COVID-19 vaccine doses were reallocated to other African countries, due to low vaccine uptake and the realization that the doses would expire before use. Based on data available on 13 August 2022, 2.76% of the DRC population had been fully vaccinated with last dose of primary series of COVID-19 vaccine, placing the country second to last in Africa and in the last five in global COVID-19 vaccination coverage. The DRC’s reliance on vaccine donations requires continuous adaptation of the vaccine deployment plan to match incoming COVID-19 vaccines shipments. Challenges in planning vaccine deployments, vaccinating priority populations, coordinating, and implementing the communications plan, disbursing funds, and conducting supervision of vaccination activities have contributed to low COVID-19 vaccine coverage. In addition, the spread of rumors through social media and by various community and religious leaders resulted in high levels of vaccine hesitancy. A strong risk communication and community engagement plan, coupled with innovative efforts to target the highest-risk populations are critical to increase vaccine uptake during the next phase of COVID-19 vaccine introduction.
Introduction
It has been more than 2 years since the World Health Organization (WHO) declared the COVID-19 outbreak to be a Public Health Emergency of International Concern (PHEIC) on 30 January 2020.Citation1 Since then, public health and social measures (PHSMs) have been put in place globally, with COVID-19 vaccination starting in December 2020 in certain countries.
COVID-19 vaccine access for low- and middle-income countries has been facilitated by the COVID-19 Vaccines Global Access (COVAX), the vaccines pillar of the Access to COVID-19 tools (ACT) accelerator.Citation2 The objective of COVAX is to ensure equitable access to COVID-19 vaccines in these countries and to mitigate the public health and economic impact of the pandemic. COVAX is dedicated to ensuring enough vaccine doses are available for countries to reach the WHO target to vaccinate 70% of the population in every country with the primary vaccination series by mid-2022.Citation3,Citation4 As of 13 August 2022, 67.4% of the world’s population has received at least one dose of a COVID-19 vaccine, whereas only 20.7% of people in low-income countries have received at least one dose.Citation5
The Democratic Republic of the Congo (DRC) has an estimated population of 107 million with a fragile health system that continues to experience recurrent epidemics of Ebola, measles, polio, yellow fever, and cholera, as well as endemic diseases, such as malaria and typhoid fever.Citation6 Despite multiple waves of COVID-19, overall reported cases and deaths have remained relatively low, with 92.542 COVID-19 cases and 1.393 deaths reported as of 13 August 2022.Citation7,Citation8 However, gaps in COVID-19 surveillance and limited testing capacity nationwide have largely hindered the development and implementation of a strong COVID-19 response in DRC, and the true disease burden is unknown.Citation9
In March 2021, 1.8 million doses of COVID-19 vaccines were received in DRC and COVID-19 vaccination officially began on 19 April 202.Citation10 After only reaching 0.15% of the population with one dose during the first phase (April through July 2021), the country planned to strengthen vaccination efforts during the second phase (beginning September 2021, ). By 13 August 2021, 2.8% of the DRC adult population had been fully vaccinated.Citation7,Citation8 Here, we report on the COVID-19 vaccine introduction and the challenges encountered during the first phase of vaccination in DRC, focusing on the COVID-19 vaccine ChAdOx1-S [recombinant] (AstraZeneca®/Covishield).
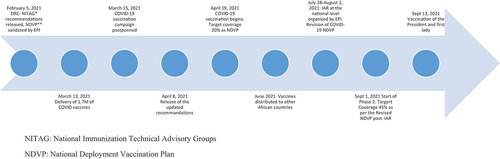
Figure 1. Timeline of COVID-19 vaccine introduction events in the Democratic Republic of the Congo, 2021.
COVID-19 vaccination in DRC
In February 2021, the DRC’s National Immunization Technical Advisory Group (NITAG) issued recommendations for the use of COVID-19 vaccines in DRC.Citation11 The NITAG also recommended vaccination strategies and priority target populations for vaccination, following recommendations of the Strategic Advisory Group of Experts (SAGE) on immunization,Citation12 as well as strong risk communication and community engagement (RCCE) efforts around vaccination. Following these recommendations and WHO guidance, a National Vaccine Deployment Plan (NVDP) was developed to define priority groups per scenarios of vaccine scarcity (phases of vaccination), strategies, and timeframe to reach out to them (). The three priority target groups for phase 1, estimated to represent 20% of the population, were healthcare workers (HCWs) and social workers, people over 55 years of age, and people with comorbidities. The DRC government had planned two sub-phases for phase 1 and were defined according to the country’s expected vaccine allocations. Sub-phase 1a was planned to cover 3% of the population and 1b would cover 17% in order to reach 20% vaccination coverage of the most at-risk population.
On 2 March 2021, 1,760,000 doses of ChAdOx1-S [recombinant] (Covishield®), given as a two dose regimen, were received through COVAX, with an additional 50,000 doses donated by the Indian Government.Citation10 This delivery was the first in a series of shipments to cover 3% of the population (sub-phase 1a) (8, 13) (). Nine days later, Denmark, followed by over a dozen other European countries, paused vaccination with ChAdOx1-S [recombinant] pending a safety investigation of thrombosis events reported in multiple vaccinated persons.Citation13 To strengthen capacity for vaccine safety investigations, the DRC Ministry of Health postponed the rollout on 14 March 2021, the day before the launch. On 8 April 2021, the DRC NITAG issued an updated set of guidelines re-recommending ChAdOx1-S [recombinant] and vaccinations began on 19 April 202.Citation14,Citation15 Early vaccine uptake was slow, and within weeks it was clear that most of the 1.7 million doses would reach their June and July expiration dates before they could be administered. To avoid wasting doses, 1.44 million doses were redeployed to other African countries. In addition, the recommended age group was expanded to include adults ages 18 and older.
By July 2021, vaccination was expanded from 5 provinces to 13 out of 26 provinces, with the selection of provinces based on disease rates, risk of further spread, and readiness to distribute the vaccines. By 10 July 2021, 82151 people (0.15% of the total adult population) had received their first dose and 4,260 (0.01% of the adult population) received their second, and approximately 182,000 doses expired according to the DRC, the Expanded Programme on Immunization (EPI). Vaccination resumed after receipt of 51,000 doses of ChAdOx1-S [recombinant] donated by the United Kingdom (UK on 13 August 2021).Citation16 These doses were reserved for persons needing their second dose.
Operational challenges with COVID-19 vaccine rollout
Successful vaccine introduction is highly dependent on robust operational microplanning, that is creating a detailed roadmap for the implementation of the vaccination program.Citation17 Implementation of COVID-19 vaccination should align with the country’s national deployment and vaccination plan (NDVP) and identification of priority populations, the need to tailor strategies for delivery, demand and uptake; and implementation planning will need to be regularly updated as the vaccine availability increases.Citation17 In February 2021, the DRC EPI hosted a workshop with provincial health authorities to plan human resource allocation; vaccines supply logistics, service delivery, demand generation and community engagement. Planning was challenged by the difficulties quantifying priority populations, as there is no reliable list of HCWs and no accurate estimates of the number of people over the age of 65 or the number with high-risk comorbidities. Estimates of the total population are based on extrapolations from 1984, when the last national census occurred. Without accurate population data, planning service delivery, and accurately quantifying vaccine needs was challenging and did not allow for the implementation of the relevant strategies proposed to reach all target populations, including the most vulnerable.
The lack of sufficient resources hindered the implementation of vaccination activities. According to the officials from the DRC Ministry of Health, a detailed budget was developed by the EPI to cover vaccination activities and 100% financing was to be provided by the World Bank in January 2021, with 50% considered as a loan that required repayment. However, the negotiation process took close to one year, thus at the start of phase 1, less than half of the planned resources had been disbursed.
Moreover, there were significant challenges securely and efficiently moving funds to subnational levels. According to the DRC EPI, financial documentation submitted by provincial authorities (Division Provincial de la Santé, DPS) to the national level was regularly delayed. These funding gaps hindered vaccination activities and prevented the recruitment of adequate numbers of vaccinators, adequate training of staff, and the payment of salaries. Subsequently, many planned sites never opened or had reduced or inconsistent hours of operation. Strikes among public sector healthcare workers in multiple provinces lasting 3 weeks to 6 months added to the difficulties in maintaining immunization services.Citation18 The lack of payment and training also affected data management staff, which led to reporting delays. According to the DRC EPI, funding gaps also contributed to limited national level supportive supervision, hindering the detection and response to gaps in training and motivation.
According to the DRC EPI, not all sites targeted the same priority groups or provided vaccination cards, and some sites charged service fees or insisted on conducting and charging for clinical examinations prior to vaccination. With the low demand and few people coming to sites each day, vaccine wastage was reported up to 50%. At other sites, vaccine vials remained unopened if the number of people requesting vaccination in a day was insufficient and persons were turned away unvaccinated. This lack of national-level supervision likely prevented timely correction of other operational issues, such as having and using thermometers or vaccine vial monitors (VVMs) to monitor vaccine storage conditions, or using adequate waste management protocols.
Introduction of COVID-19 vaccine has been further complicated by outbreaks of other vaccine-preventable diseases in different provinces and other natural disasters. Since the pandemic started, there have been outbreaks of meningitis in Tshopo, typhoid fever in Kwango, cholera in South-Kivu, Ebola virus disease in North-Kivu and Equateur, and measles throughout the country.Citation19 In May 2021, the Nyiragongo volcano erupted near the city of Goma, displacing more than 500,000 people, further disrupting immunization activities in North Kivu.Citation20
COVID-19 response and perceived risk
After the first confirmed case of COVID-19 in DRC, the government responded swiftly, announcing PHSMs to prevent COVID-19 transmission.Citation19 These PHSMs included lockdowns and curfews, closing of restaurants and nightclubs, closing of schools and universities, prohibiting mass gatherings, and banning domestic and international flights. However, these PHSMs had a negative economic impact on the community, affecting the most vulnerable households, and increasing the risks for women and young girls now unable to work, go to school, or leave the house.Citation21 The country’s economy declined in the first quarter of 2020, leading to a reduction in employment (especially in the sector without government regulation), and a decline in household income.Citation22 Exacerbating the situation for families that lost income was a rise in food prices in DRC by 10.9% between February 2020 and July 2021.Citation23
Perceived effectiveness of a government response to COVID-19 has been shown to be a key factor in building public confidence,Citation24 with willingness to accept a COVID-19 vaccine generally being higher among people who felt the response was well-handled.Citation25 According to a survey, satisfaction with the government’s response to the pandemic fell from 79% to 66% between February and December 2021.Citation26 Satisfaction with the government’s response to the pandemic has been shown to be a relevant determinant contributing to adherence of population to PHSMs.Citation27 In DRC, perceived risk of COVID-19 in the general population was found to be low.Citation26 For example, at a vaccination site, a man was asked about COVID-19 vaccination by media journalist and the man responded: “we don’t like vaccines here and I’m not afraid of COVID-19: we have remedies, homemade herbal teas.”Citation28 Several COVID-19 response leaders, as well as political figures remained unvaccinated and continued to make comments undermining the safety of the vaccines and further reinforcing the idea that COVID-19 was not a serious threat.Citation26
Communication and community engagement
Though a well-designed communication and community engagement plan was developed, the plan was never implemented, partially due to challenges with funding distribution to the local levels according to DRC Ministry of Health officials. Community engagement activities, including outreach mobilization, and the incorporation of community influencers (including parliamentarians, religious and community leaders) were rarely used and failed to create the necessary trust and increase vaccine demand.Citation29 According to the DRC EPI, media briefings through the radio or the television, print based materials, posters, advertisements, and social messaging conveying the importance of COVID-19 vaccination were not widely available. Many vaccination sites were not clearly identified and lacked posters or banners and hours of operation. Eligible community members reported not knowing where to get vaccinated.Citation30
Vaccine hesitancy, rumors, and misinformation
Prior to the start of the pandemic, WHO identified vaccine hesitancy as one of the ten main threats to global health.Citation31–33 A survey among 15 African countries conducted between August and December 2020 found that 41% of Congolese adults, aged 18 years and above indicated they would not take the vaccine, compared to 20% from all other countries.Citation34 Vaccine hesitancy was also reportedly high among HCWs and the lack of training and sensitization on COVID-19 vaccines led to low uptake in HCWs.Citation26 For example, the director of a public hospital in Kinshasa said he delayed receiving his vaccination due to fears of being judged by the facility’s staff.Citation35 By 7 July 2021, only 0.01% of HCWs had received one dose of COVID-19 vaccine.Citation36 HCWs knowledge and attitudes about vaccines are important determinants of their own vaccine acceptance and their intention to recommend the vaccine to their patients.Citation37 High vaccine uptake among HCWs has been found to be associated with higher uptake in the community and their reluctance to be vaccinated likely resulted in reduced uptake in the community.Citation38,Citation39 A key lesson learned from this phase was to recognize the importance of HCWs and their critical role promoting vaccine confidence and uptake among patients and across the larger community. A renewed focus on increasing HCW uptake could lead to increased uptake in the community overall.
In DRC, the circulation of misinformation and rumors through social and traditional media and by various community and religious leaders may have contributed to low COVID-19 vaccine uptake.Citation40 Confidence likely declined after a controversial discussion between two French experts broadcast on television at the start of the pandemic. It was hypothesized that BCG (bacille Calmette-Guerin) vaccine might help to combat COVID-19, experts suggested that trials of BCG vaccine to prevent COVID-19 could be more easily done in Africa because care and treatment, and prevention, were all lacking.Citation41 This video clip spread rapidly in DRC, with many accusing Europeans of wanting to test experimental COVID-19 vaccines on Africans.Citation40 Throughout social media channels several other rumors circulated: that the Congolese were the “experimental mice” for untested COVID vaccines; SARS-CoV-2 was created in a European laboratory; COVID-19 vaccines were being used to sterilize women and to exterminate Africans.Citation42 For example, in February 2021, a rumor that students would receive COVID-19 vaccines in schools in Bukavu, South-Kivu Province and Lubumbashi, Haut-Katanga Province without parental consent created panic among parents.Citation43 False information continued to circulate about vaccine safety, including that the COVID-19 vaccines were manufactured too quickly and that the vaccines were dangerous and might lead to COVID-19 or death.Citation44 In July, when efforts to revitalize the vaccination campaign were ongoing, one politician tweeted that his brother had died the day after receiving the first dose of COVID-19 vaccine.Citation45 The President of the Republic expressed concerns about ChAdOx1-S [recombinant] vaccine and refused to take the vaccine, declaring on national television: “I believe I was right not to be vaccinated [with this vaccine]. I asked the opinions of some and others, but (they) were divided, some reassured me that there was no danger, but I have my own doubts. There are other vaccines coming and you will see me get vaccinated.”Citation46 Religious and community leaders continued to advise followers not to accept COVID-19 vaccines before political leaders accepted to be publicly vaccinated.Citation47
Limited attempts were made to dispel rumors and improve RCCE. Efforts included increasing capacity to report science among select journalists, sensitizing religious leaders (Protestants, Catholics, Muslims, Orthodox, Salvation Army and born-again churches), and increasing information on vaccination site availability through telecom companies. As DRC attempts to rebuild their COVID-19 vaccination plan, engagement of community and religious leaders will be important. Further, focusing on real time dispelling of rumors may increase acceptance and demand.
Discussion
In the early phases of the COVID-19 vaccine introduction, many African countries relied heavily on doses delivered by COVAX and faced similar challenges in terms of the supply, ultra-cold chain management, planning ofvaccine deployment, vaccinating priority populations, insufficient funds, vaccine hesitancy, and a slow uptake.Citation48 Furthermore, ChAdOx1-S [recombinant] was initially widely distributed due to less restrictive storage conditions, but the safety concerns amplified rumors and led to lower uptake.Citation49 Hence, only eight African countries managed to use their received COVAX doses, nine nations administered less than a quarter of their doses, and 15 nations administered less than half of the received COVID-19 doses, according to WHO.
A few countries, such as Angola (country bordering DRC its southwestern part) drew on its existing systems and experience, basing its COVID-19 immunization campaign on the systems put in place to address a deadly yellow fever outbreak in 2017.Citation50 Covid-19 vaccination in Angola started on 10 March 2021, and in two weeks over 70, 000 people from priority groups across the country were vaccinated with one dose, including over 35, 000 health workers.Citation48,Citation50 The electronic pre-registration system, use of SMS messages, e-mail confirmations, and QR codes for on-site verification have been useful in preparing the administration of second doses, as well as in collecting data to monitor vaccine safety.Citation50
Likewise, in Ghana, political leadership was found to be the key in addressing the Covid-19 vaccine hesitancy. Actually, the Ghana’s President received country’s first COVID-19 vaccine live on national television on 1 March 2021 and was followed by several other political and religious leaders as well as prominent Ghanaian figures.Citation48 Innovation has played a pivotal role in Ghana’s successful rollout (use of electronic register for all vaccines, virtual platforms for training, various Apps to enhance work etc.).Citation51
Conclusion
At the end of phase 1 on 10 July 2021, a total of 4,260 people were fully vaccinated in DRC with two doses of COVID-19 vaccine.Citation52 COVID-19 vaccine uptake was the among the lowest in the world, most doses were redeployed to other countries, and wastage rates were high.Citation53 Operational challenges with NDVP implementation, and financial constraints, particularly the delay in the disbursement of funds, have contributed to low COVID-19 vaccine uptake in DRC. Gaps in training of healthcare providers, limited supervision of immunization sites, and limited implementation of communications activities contributed to misinformation, rumors, and conspiracy theories about COVID-19 vaccines potentially contributing to poor demand and acceptance for vaccination.
Recommendations
At the end of July 2021, a national Intra Action Review (IAR) to evaluate the first phase of vaccination was held with all relevant consultants. Priority recommendations included 1) incorporating the updated NDVP into the 2022 EPI Action Plan, 2) improved and detailed microplanning to better estimate immunization needs, 3) conducting a mass two-week vaccination campaign to kickoff phase 2 and incorporation of COVID-19 vaccination into the routine immunization system and 3) improving communications. The NDVP was updated based on these key findings and recommendations. Since July, subsequent sub-national (provincial level) IARs have been implemented or plan to be implemented to identify and improve provincial level responses.
Implementation of recommendations from the IARs could faciliate success in subsequent phases of COVID-19 vaccination with a focus on using evidence-based COVID-19 risk communication strategies with innovative efforts to target a population with low acceptance. Effective and regular communication, such as regular press briefings on radio and television, distribution of educational materials with specific site information, and incorporation of community and religious leaders may also lead to increased demand for the vaccine.
The next phase of vaccination began in September 2021, with the arrival of Moderna mRNA-1273 (Spikevax®, 250.000 doses, enough to vaccinate 125,000 persons) through COVAX.Citation54 The President of the Republic was publicly vaccinated on 12 September 2021 and invited the entire population to also get vaccinated. Several other shipments of various COVID-19 vaccines, through either COVAX, through bilateral donations, or through the Africa Vaccine Acquisition Task Team (AVATT) have been received with more than 5.8 million received to date. The DRC EPI is committed to revising their vaccination plan to better protect the population against COVID-19. According to EPI, Moderna mRNA-1273 is the first two-dose regimen COVID-19 vaccine administered across DRC as primary series of vaccination since the start in September 2021. As of 8 August 2022, 188,788 have been fully vaccinated with Moderna mRNA-1273.
Disclaimer
The findings and conclusions of this paper are those of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
Acknowledgement
The authors are grateful to the following staffs and managers of the DRC Expanded programme on immunization of DRC for their collaboration, support and advice during the writing of this commentary paper: Crispin Kazadi, Christophe Luhata, David Olela, Arsène Kabwaya, Lora Bertin, and Donat Shungu.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Sohrabi C, Alsafi Z, O'Neill N, Khan M, Kerwan A, Al-Jabir K, Losifidis C, Agha R. Wolrd Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID19). Int J surg; 2020 apr; 76: 71-76. doi:10.1016/j.ijsu.2020.02.034. Epub2020 Feb 26. Erratum in: Int J Surg. 2020 May; 77: 217.
- Mark E, Upton H. International collaboration to ensure equitable access to vaccines for COVID‐19: the ACT‐Accelerator and the COVAX facility. Milbank Q. 2021;99(2):1–7. doi:10.1111/1468-0009.12503.
- World Health Organization. Strategy to achieve global COVID-19 vaccination by mid-2022. Geneva (Switzerland): World Health Organization; 2021 Jun 10 [accessed 2022 Jan 2022]. https://cdn.who.int/media/docs/default-source/immunization/covid-19/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022.pdf.
- Dzinamarira T, Nachipo B, Phiri B, Musuka G. COVID-19 vaccine roll-out in South Africa and Zimbabwe: urgent need to address community preparedness, fears and hesitancy. Vaccines. 2021;9(3):250. doi:10.3390/vaccines9030250.
- Our World in Data. Coronavirus (COVID-19) vaccinations. Oxford (United Kingdom): Oxford Martin School, University of Oxford; 2022 Aug 14 [accessed 2022 Aug 14]. https://ourworldindata.org/covid-vaccinations.
- Ministère du Plan de la République Démocratique du Congo (RDC). Annuaire statistique RDC 2020. Kinshasa (RDC): Programme de Nations Unies pour le Développement; 2021 Oct 18 [accessed 2021 Nov 20]. https://www.cd.undp.org/content/rdc/fr/home/library/annuaire-statistique-2020.html.
- Our World in Data. Coronavirus (COVID-19) vaccinations. Oxford (United Kingdom): Oxford Martin School, University of Oxford; 2022 Jan 22 [accessed 2022 Jan 22].
- World Health Organization (WHO). WHO health emergency dashoard. Geneva (Switzerland): World Health Organization; 2022 Aug 13 [accessed 2022 Aug 13]. https://covid19.who.int/region/afro/country/cd.
- Ditekemena JD, Nkamba DM, Muhindo HM, Siewe JNF, Luhata C, Van den Bergh R, Tshefu Kitoto A, Van Damme W, Muyembe JJ, Colebunders R. Factors associated with adherence to COVID-19 prevention measures in the Democratic Republic of the Congo (DRC): results of an online survey. BMJ Open. 2021;11(1):e043356. doi:10.1136/bmjopen-2020-043356.
- The United Nations International Children Emergency funds (UNICEF) pour enfants en République Démocratique du Congo (RDC). Arrivée de plus de 1,7 million de doses de vaccin contre la COVID-19 en RDC. Kinshasa (RDC): UNICEF RDC; 2021 Mar 3 [accessed 2021 May 28]. https://www.unicef.org/drcongo/communiqu%C3%A9s-de-presse/arriv%C3%A9e-de-plus-de-17-million-de-doses-de-vaccin-contre-la-covid-19-en-rdc.
- OCHA Services. SITREP COVID_N87+VACC. Kinshasa (DRC): OICHA Services; 2021 Mar 28. [accessed 2021 Jul 30]. https://www.humanitarianresponse.info/fr/operations/democratic-republic-congo/document/sitrep-covidn87.
- World Health Organization (WHO) Emergencies Preparedness, Strategic Advisory Group of Experts on Immunization (SAGE). WHO SAGE values framework for the allocation and prioritization of COVID-19 vaccination. Geneva (Switzerland): World Health Organization; 2020 Sep 13 [accessed 2021 Apr 15]. https://www.who.int/publications/i/item/who-sage-values-framework-for-the-allocation-and-prioritization-of-covid-19-vaccination.
- Hunter PR. Thrombosis after covid-19 vaccination. BMJ. 2021;373:n958. doi:10.1136/bmj.n958.
- World Bank. Project paper on a proposed additional grant in the amount of US$ 69.3 million (US $100 million equivalent) and a proposed additional credit in the amount of US $100 million and a proposed restructuring to the Democratic Republic of Congo for the report no: pad4410 DRC COVID-19 strategic preparedness and response project. Washington (DC): World Bank; 2021 Jun 15. [accessed 2021 Aug 02]. https://documents1.worldbank.org/curated/en/602061625277685570/pdf/Congo-Democratic-Republic-of-COVID-19-Strategic-Preparedness-and-Response-Project-Additional-Financing-and-Restructuring.pdf.
- Wise J. Covid-19: European countries suspend use of Oxford-AstraZeneca vaccine after reports of blood clots. BMJ. 2021;372:n699. doi:10.1136/bmj.n699.
- The United Nations International Children Emergency funds (UNICEF) for every child in the Democratic Republic of the Congo (DRC). UK donates new doses of COVID-19 vaccine to DRC. Kinshasa: UNICEF DRC; 2021 Aug 13 [accessed 2022 Jun 7]. https://www.unicef.org/drcongo/en/node/3106.
- World Bank. The World Bank additional financing DRC COVID-19 strategic preparedness and response project (P176215). Washington (DC): World Bank; 2021 Jun 13 [accessed 2022 Jan 17]. https://documents1.worldbank.org/curated/en/289671623622272291/pdf/Project-Information-Document-Additional-Financing-DRC-COVID-19-Strategic-Preparedness-and-Response-Project-P176215.pdf.
- Nyemba B Congo health workers reduce coronavirus services in pay protest. Kinshasa (DRC): Reuters; 2020 Jul 7 [accessed 2021 Sep 22]. https://www.reuters.com/article/us-health-coronavirus-congo-strike-idUSKBN24823F.
- World Health Organization (WHO). Rapport de deux (02) ans d’appui de l’oms au Gouvernement de la République Démocratique du Congo dans la réponse à la COVID-19 (10 mars 2020 au 10 mars 2022). Kinshasa (DRC): OCHA Services; 2022 Mar 21 [accessed 2022 Jun 5]. https://reliefweb.int/report/democratic-republic-congo/rapport-de-deux-02-ans-d-appui-de-l-oms-au-gouvernement-de-la-r.
- Coulborn RM, Nackers F, Bachy C, Porten K, Vochten H, Ndele E, Van Herp M, Bibala-Faray E, Cohuet S, Panunzi I. Field challenges to measles elimination in the Democratic Republic of Congo. Field challenges to measles elimination in the Democratic Republic of the Congo. Vaccine. 2020 Mar 17;38(13):2800–07. doi:10.1016/j.vaccine.2020.02.029.
- Juma CA, Mushabaa NK, Abdu Salam F, Ahmadi A, Lucero-Prisno DE. COVID-19: the current situation in the Democratic Republic of Congo. Am J Trop Med Hyg. 2020 Dec;103(6):2168–70. doi:10.4269/ajtmh.20-1169.
- Gouvernement de la République Démocratique du Congo (RDC). Impacts sanitaires et socio-économiques de la Covid-19 en RDC, analyse prospective et orientation de la réponse multisectorielle. Kinshasa (RDC): Bureau d’études Congo Challenges; 2020 May [accessed 2021 Feb 21]. https://www.undp.org/content/dam/rba/docs/COVID-19-CO-Response/UNDP-rba-Covid-RDC-DRC_2020.pdf.
- World Vision. Price shocks, how COVID-19 is triggering a pandemic of child malnutrition and what is needed to prevent this from happening. Kinshasa (DRC): World Vision; 2021 Sep 23 [accessed 2022 Jan 17]. https://www.wvi.org/sites/default/files/2021-09/9022_Price_Shocks_Report_Final.pdf.
- Lazarus JV, Ratzan S, Palayew A, Billari FC, Binagwaho A, Kimball S, Larson HJ, Melegaro A, Rabin K, White TM, et al. COVID-SCORE: a global survey to assess public perceptions of government responses to COVID-19 (COVID-SCORE-10). PLoS One. 2020 Oct 6;15(10):e0240011. doi:10.1371/journal.pone.0240011.
- Wouters OJ, Shadlen KC, Salcher-Konrad M, Pollard AJ, Larson HJ, Teerawattananon Y, Jit M. Challenges in ensuring global access to COVID-19 vaccines: production, affordability, allocation, and deployment. Lancet. 2021 Mar 13;397(10278):1023–34. doi:10.1016/S0140-6736(21)00306-8.
- Partnership for Evidences-based Covid-19 (PERC). Responding to Covid-19 in Africa finding the balance (Part IV) and calls to Action. Addis Ababa: Africa CDC; 2021 Dec 19 [accessed 2022 Jan 26]. https://africacdc.org/download/responding-to-covid-19-in-africa-finding-the-balance-part-iv-and-calls-to-action/.
- Siegrist M, Luchsinger L, Bearth A. The impact of trust and risk perception on the acceptance of measures to reduce COVID-19 cases. Risk Anal. 2021 May;41(5):787–800. doi:10.1111/risa.13675. Epub 2021 Jan 12. PMID: 33438218; PMCID: PMC8014821.
- BBC News Afrique. Covid-19: pourquoi la vaccination contre le coronavirus en RDC est-elle si lente? Dakar (Senegal); 2021 May 1 [accessed 2022 Mar 10]. https://www.bbc.com/afrique/region-56933366.
- Ashworth HC, Dada S, Buggy C, Lees S. The importance of developing rigorous social science methods for community engagement and behavior change during outbreak response. Disaster Med Public Health Prep. 2021 Dec;15(6):685–90. doi:10.1017/dmp.2020.163.
- Bergson Kakule, Eugene Muhindo, Emily Janoch et Allison Prathe. Au dernier kilomètre: les vaccins COVID-19 en RDC. Geneva (Switzerland): OCHA Services, CARE; [accessed 2022 Jun 6]. https://careevaluations.org/wp-content/uploads/Etude-de-cas-RDC-FR-Avril-27.pdf.
- Wiysonge CS, Ndwandwe D, Ryan J, Jaca A, Batouré O, Anya BM, Cooper S. Vaccine hesitancy in the era of COVID-19: could lessons from the past help in divining the future?. Hum Vaccin Immunother. 2022 Dec 31;18(1):1–3. doi:10.1080/21645515.2021.1893062.
- Larson HJ, Jarrett C, Eckersberger E, Smith DM, Paterson P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007–2012. Vaccine. 2014;32(19):2150–59. doi:10.1016/j.vaccine.2014.01.081.
- Dubé E, Vivion M, Macdonald NE. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: influence, impact and implications. Expert Rev Vaccines. 2015 Jan;14(1):99–117. doi:10.1586/14760584.2015.964212.
- Africa Centres Disease Control and Prevention (CDC Africa) and the London School of Hygiene & Tropical Medicine (LSHTM). Majority of Africans would take a safe and effective COVID-19 vaccine. Addis-Ababa: Africa CDC; 2020 Dec 17 [accessed 2021 Jan 12]. https://africacdc.org/news-item/majority-of-africans-would-take-a-safe-and-effective-covid-19-vaccine/.
- All Africa. Congo-Kinshasa: Panel d’échanges sur la vaccination contre le Covid-19/ex. Mama Yemo - Dr. Jean Jacques Muyembe appelle le personnel à se faire vacciner pour servir d’exemple à la population. Kinshasa (RDC): La prospérité; 2021 Dec 24 [accessed 2021 Dec 24]. https://fr.allafrica.com/stories/202112240478.html.
- Kakule B, Lubukayi N, Muhindo E, Janoch E, Prather A. At the last mile: COVID-19 vaccines in DRC. Kinshasa (DRC): CARE; 2022 Apr 23 [accessed 2022 Aug 1]. https://careevaluations.org/wp-content/uploads/COVID-19-vaccines-in-Democratic-Republic-of-the-Congo-April-2022.pdf.
- Wiley KE, Massey PD, Cooper SC, Wood N, Quinn HE, Leask J. Pregnant women’s intention to take up a post-partum pertussis vaccine, and their willingness to take up the vaccine while pregnant: a cross sectional survey. Vaccine. 2013;31(37):3972–78. doi:10.1016/j.vaccine.2013.06.015.
- Vinck P, Pham PN, Bindu KK, Bedford J, Nilles EJ. Institutional trust and misinformation in the response to the 2018-19 Ebola outbreak in North Kivu, DR Congo: a population-based survey. Lancet Infect Dis. 2019 May;19(5):529–36. doi:10.1016/S1473-3099(19)30063-5.
- Tafuri S, Gallone MS, Cappelli MG, Martinelli D, Prato R, Germinario C. Addressing the anti-vaccination movement and the role of HCWs. Vaccine. 2014 Aug 27;32(38):4860–65. doi:10.1016/j.vaccine.2013.11.006.
- Agence d’information d’Afrique centrale. Vaccin Covid19 en Afrique?: undefined colère des internautes africains. Brazzaville (République du Congo): Yvette Nzeba; 2020 Apr 6 [accessed 2022 Feb 16]. https://www.adiac-congo.com/content/vaccin-covid19-en-afrique-la-colere-des-internautes-africains-115075.
- Le Parisien. Vaccins contre le coronavirus « à tester en Afrique » : undefined CSA met en garde LCI. Paris (France): BalanceTonMedia; 2020 Apr 02 [accessed 2021 Oct 9]. https://www.leparisien.fr/culture-loisirs/tv/vaccins-contre-le-coronavirus-a-tester-en-afrique-le-csa-met-en-garde-lci-14-04-2020-8299440.php.
- James MV, Lees SS. “Are you sure it’s not the Corona vaccine?” An Ebola vaccine trial during COVID-19 in DRC. Med Anthropol. 2022;41(5):503–17. doi:10.1080/01459740.2022.2097908.
- La Libre Afrique. RDC: une rumeur de vaccination perturbe les activités scolaires dans deux villes. Bruxelles (Belgique): Agence France Presse (AFP); 2021 Feb 25 [accessed 2021 Oct 11]. https://afrique.lalibre.be/58613/rdc-une-rumeur-de-vaccination-perturbe-les-activites-scolaires-dans-deux-villes/.
- RTBF. Non, les vaccins contre le Covid-19 ne créent pas des variants comme l’affirme un ancien prix Nobel. Bruxelles (Belgique): Johanne Montay et Grégoire Ryckmans; 2021 May 19 [accessed 2022 Feb 24]. https://www.rtbf.be/article/non-les-vaccins-contre-le-covid-19-ne-creent-pas-des-variants-comme-laffirme-un-ancien-prix-nobel-10764833.
- Kalombo F Jeanpi Bolakisa n’est plus. A la justice de faire son travail. Kinshasa (RDC): Francis Kalombo; 2021 Jul 5 [accessed 2021 Aug 23]. https://twitter.com/franciskalombos/status/1412017311435923456?lang=en.
- Mediacongo. Décès d’un Congolais suite à sa vaccination avec AstraZeneca: undefined ministre de la Santé ouvre une enquête. Kinshasa (RDC): Allo Docteurs/MCP; 2021 Jul 8 [accessed 2021 Sep 23]. https://www.mediacongo.net/article-actualite-89823_deces_d_un_congolais_suite_a_sa_vaccination_avec_astrazeneca_le_ministre_de_la_sante_ouvre_une_enquete.html.
- Habari RDC. RDC: AstraZeneca, un vaccin apocalyptique pour des pentecôtistes 2021. Kinshasa (RDC): Mike Lubandisha; 2021 Oct 9 [accessed 2022 Feb 24]. https://habarirdc.net/rdc-astrazeneca-un-vaccin-apocalyptique-pour-des-pentecotistes/.
- World Health Organization Africa (WHO Africa). Risks and challenges in Africa’s COVID-19 vaccine rollout. Brazzaville (Congo Republique): World Health Organization Africa (WHO Africa); 2021 May 14 [accessed 2022 Aug 17]. https://www.afro.who.int/news/risks-and-challenges-africas-covid-19-vaccine-rollout.
- Petersen MB, Jørgensen F, Lindholt MF. Did the European suspension of the AstraZeneca vaccine decrease vaccine acceptance during the COVID-19 pandemic? Vaccine. 2022 Jan 28;40(4):558–61. doi:10.1016/j.vaccine.2021.12.026. Epub 2021 Dec 21. PMID: 34952752; PMCID: PMC8693776.
- World Health Organization Africa (WHO Africa). Emerging lessons from Africa’s COVID-19 vaccine rollout. Brazzaville (Congo Republique): World Health Organization Africa (WHO Africa); 2021 Apr 27 [accessed 2022 Aug 16]. https://www.afro.who.int/news/emerging-lessons-africas-covid-19-vaccine-rollout.
- World Health Organization Africa (WHO Africa). Ghana shares success story in COVID-19 vaccine rollout with Cote d’Ivoire. Brazzaville (Congo Republique): World Health Organization Africa (WHO Africa); 2021 Jun 1 [accessed 2022 Aug 17]. https://www.afro.who.int/news/ghana-shares-success-story-covid-19-vaccine-rollout-cote-divoire.
- Ministère de la Santé publique, Hygiène et prévention de la République Démocratique du Congo (RDC). Rapport de situation N° 243/2021 du 31/08/2021. Kinshasa (RDC): Direction de la Surveillance de la Maladie; 2021 Aug 31 [accessed 2022 Mar 5]. https://fscluster.org/sites/default/files/documents/sitrep_covid-19_in_drc_243_20210831.pdf.
- Kakule B, Lubukayi N, Muhindo E, Janoch E, Prather A At the last mile: cOVID-19 vaccines in DRC. Kinshasa (DRC): Reliefweb, OCHA Services, CARE; 2022 Apr 27 [accessed Aug 19]. https://reliefweb.int/report/democratic-republic-congo/last-mile-covid-19-vaccines-drc.
- Zoomeco. RDC: Covid-19, 250 000 doses de vaccin Moderna réceptionnées à Kinshasa. Kinshasa (RDC): Mitterrand Masamuna; 2021 Sep 7 [accessed 2022 May 20]. https://zoom-eco.net/a-la-une/rdc-covid-19-250-000-doses-de-vaccin-moderna-receptionnees-a-kinshasa/.