
ABSTRACT
The introduction of Expanded Program on Immunization (EPI) and the availability of vaccines have contributed to significant reduction in morbidity and mortality rate, particularly among infants and children under five years. The coronavirus pandemic has however interrupted vaccination systems, limiting access and coverage for children. This study assesses the effect of the coronavirus disease outbreak on the EPI activities. The study employed a cross-sectional study design. Purposive and convenience sampling methods were used to sample 510 health workers directly engaged in immunization activities from 15 health care facilities. Coverages for five selected antigens (Diphtheria, Tetanus, Pertussis, Poliomyelitis, Tuberculosis) and Measles in the year 2020 experienced an overall decline ranging from 38.8% for measles rubella vaccine to 53.1% for Penta vaccine. The year 2019 recorded coverages ranging from 69.1% for BCG vaccine to 78.4% for penta vaccine, relatively higher than 2020. EPI services patronization rose up after COVID-19 peaks periods for BCG vaccine 67.7% to 89.2% for penta vaccine. The COVID-19 pandemic disrupted the delivery of EPI services significantly. Healthcare stakeholders can envisage telehealth services in care delivery against pandemic outbreaks. This study contributes to empirical knowledge by recommending vital predictive factors during a pandemic outbreak.
Introduction
The health-related Sustainable Development Goals (SDGs), particularly SDG 3 for improving child survival, have gotten much attention and effort worldwide.Citation1 According to Legesse and Dechasa, the adoption of the Expanded Program on Immunization (EPI) is one of the most efficient and cost-effective public health interventions for lowering child morbidity, death, and disability linked with infectious illnesses.Citation2 Over the years, after introducing the EPI, enhancing access to and utilization of routine immunization services has been the best choice for preventing and controlling vaccine-preventable diseases (VPD).Citation3
The World Health Organization (WHO) began the EPI services in 1974 to make immunization accessible to all children globally. Ghana initiated the EPI in the year 1978. It made it countrywide in 1985, with the aim of expanding immunization coverage among children under the age of one (1) year from 6% to 80% against six diseases: tetanus, pertussis, tuberculosis, diphtheria, poliomyelitis, and measles (now measles rubella).Citation4 Since the EPI program’s inception, international endeavors have been made to spread the gains of immunizations to every country and population group. Inequalities in childhood immunizations remain an issue despite significant progress in many aspects of immunization programs.Citation5 Immunization is a critical health intervention that protects vulnerable people against Vaccine-Preventable Diseases (VPD), ensuring that individuals and communities are protected and that outbreaks of VPD are reduced. Preventing a VPD outbreak not only saves lives but also needs fewer resources than reacting to an attack, easing the stress on the healthcare system.Citation6 The works of Yawson et al., portrays that there are various challenges to reaching all children with a full complement of immunizations, including distance to facilities, maternal education, insufficient vaccines, poor service quality and poorly qualified and motivated human resources.Citation1 According to their findings, it is critical to recognize area-specific constraints and congestions affecting every child with life-saving vaccines to address stagnation and disparities at many levels of the health care system. In emergencies such as the COVID-19 pandemic, individuals are likely to become hesitant to seek immunization services due to the fear of contracting the pandemics and, at the same time, committing to sustaining immunization systems. WHO recommends that countries use approaches that respect the principle of do-no-harm and limit transmission of the pandemic (COVID-19) while providing immunization activities.Citation3,Citation4,Citation6 Immunization is regarded as a vital health service, it’s coverage is tracked as part of Sustainable Development Goal 3: ensuring healthy lives and promoting well-being for all ages.Citation5 However, the global COVID-19 pandemic has disrupted essential health and vaccination services. People could not access these services due to the agitation of contracting the virus. Similarly, vaccination campaigns and programs were deferred to ensure that social distancing measures were adhered to, and not intensifying the risk of disease outbreaks. This contributed to a decrease in routine immunization coverage, which put some communities at risk of epidemics of highly contagious diseases like measles.Citation5 A continuous reduction in regular immunization coverage will mean that numerous children will be under-vaccinated or unvaccinated, exposing them to the risk of preventable vaccine-related diseases.Citation6 On the other hand, studies have shown that immunization visits can also be utilized as an opportunity to circulate messages to encourage individuals to decrease the transmission risk of the pandemic virus, to recognize signs and symptoms of pandemic disease, and issue guidance on what to do if symptoms emerge.Citation6,Citation7 Therefore, this study seeks to identify the effect of the COVID-19 pandemic on the Expanded Program on Immunization activities in the Weija Gbawe Municipality and suggest measures to improve coverage amidst pandemics (COVID-19) outbreaks to prevent future vaccine-preventable disease outbreaks.
Routine immunization coverage
EPI administrative coverages are usually high, while routine children immunization is low. Most children do not receive the recommended seven vaccines in 15 doses before their first birthday.Citation4 Enhancing immunization coverage is critical to promoting child health and decreasing childhood diseases and deaths. Even though routine immunization has remained a significant public health intervention for national development after the latter part of the 1970s, Ghana’s immunization coverage is still low.Citation8 Meanwhile, immunization coverage levels and trends are vital for monitoring the general performance of immunization services locally, nationally and internationally. According to the studies of Sally and Kenu, high vaccination coverage is a prerequisite to control, eliminate and eradicate VPDs successfully.Citation9 Even though most mothers thought immunization was inevitable for their children, they had inadequate knowledge about EPI diseases their wards are vaccinated against and the program schedule. The majority of them knew not up to three VPD or overstated the protective benefits of immunization.Citation9 The district’s health education program should emphasize the EPI targeted diseases and schedule, the eligible age for vaccination, and the relevancy of continued attendance to Child Welfare Clinic when the mother travels.Citation8 National immunization campaigns ought to emphasize women and children in informal settlements in urban areas and higher socioeconomic households, utilizing community participation and mobilization to improve immunization services in these areas. For instance, school vaccination programs could be expanded and intensified to enhance immunization coverage in urban areas in Ghana.Citation10–12
Materials and methods
Study site description and participants
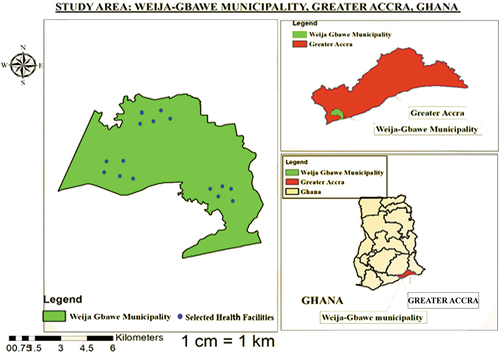
The Weija-Gbawe Municipal has Weija as its capital and is one of the Twenty-six (26) Metropolitan, Municipal, and District Assemblies in the Greater Accra Region of Ghana. The population of the Weija-Gbawe municipality is 213,674 with 108,764 females and 104,910 males, according to the 2021 Ghana Population and Housing Census (PHC) report. The municipality’s population growth rate is 4.1%, higher in the Greater Accra region. The Weija-Gbawe Municipality is situated in the South-Western part of Accra. It can be located within Latitudes 5°47‘30“N and 5°27’30“N and Longitudes 0°31‘30“W and 0°16’30“W. The Weija-Gbawe Municipality shares boundaries with Ga South to the north, Ga Central Municipal Assembly to the east, and Ablekuma North Assembly to the South-East. The Municipality also shares border again with Ga-South to the South-West and the Gulf of Guinea to the South. It occupies a land area of approximately 502.31 sq.km with about 120 settlements. The Municipality has 29 health facilities distributed among the three sub-municipals, namely Mallam, Oblogo and Weija. The graphical distributions of the health centers in the Weija-Gbawe are shown in
Figure 1. Shows the graphical distributions of the health centers in the Weija-Gbawe municipality.
Study design and sampling
Approval for this study was sought from the Weija Gbawe Municipal Health Directorate Ethical Review Committee. The study employed a descriptive cross-sectional design. This design sought to evaluate the effect of the coronavirus disease outbreak on EPI activities in the Weija-Gbawe municipality between March 2019 and January 2022. This design was preferred because it is an appropriate design for collecting information in a large quantity and drawing a quick snapshot of data on the variables of interest to the study.Citation13–15
A purposive and convenience sampling technique was used to select 15 facilities. This sampling technique is normally used when respondents drawn from large population characteristics are based on suitability and accessibility to the researcher. The facilities were selected based on the human resource capacity, availability of EPI services provided, and availability of EPI data. Data was received from management members of the selected 15 facilities that provide EPI services. Relevant data were also retrieved from the District Health Information Management System (DHIMS). Two data collection instruments were used to collect data on the effect of the COVID-19 pandemic on EPI activities.Citation13–15 Firstly, a checklist was used to retrieve selected antigens from DHIMS from 2019 to 2021. Secondly, a structured questionnaire was used to collect data on coverage, accessibility of EPI service providers, and accessibility and provision of EPI activities during the COVID-19 outbreak from the management staff of the selected facilities. The respondents were limited to a list of options from which they were required to choose a chance to answer each item in the questionnaire.
Data on the total number of vaccines administered from 2019 to 2021 was extracted from DHIMS and recorded on the checklist. Primary data was collected through the administration of questionnaires.Citation13–15 An informed consent form was given to the management staff of the selected facilities. Those who gave their consent were required to answer a series of questions with limited options on the questionnaire. A password-protected soft copy of data was collected onto the researcher’s computer. Additionally, due to the Coronavirus disease (COVID-19) pandemic, all COVID-19 protocols were observed to protect the data collection officers and the respondents.
Study population and sample size
A total of 600 questionnaires were distributed to the Management and Staff of the various health facilities. 582 responses were received, 72 were incomplete and not utilized in the study analysis. The study population finally included 510 management staff and health workers who had worked for at least two years and were engaged directly in providing an Expanded Program on Immunization services in the selected 15 facilities within the Weija-Gbawe Municipality. Staff who do not offer assistance on Expanded Program were not included in the study. Expanded Program on Immunization data between 2019 and 2021 was also retrieved and used for the analysis. The sample of 510 of healthcare workers, representing about 70% of the total population (729), was studied. The sample size selection for the study was not based on a priori determination by statistical power and/or effect size calculations. It was dependent on the proportion of the population used by most of the researchers in the fields of organizational health and safety.Citation16–18 This is because calculating effect sizes apriori is based on the assumption that sample distribution is normal.Citation16 However, in the current study, power and effect sizes were also not calculated apriori since the normality could not be determined before data collection.Citation18 Besides, 70% of the sample chosen was deemed adequate in the organizational study.Citation17,Citation19 Furthermore, this sample of 510 appropriately represents the population, and thus making the results of the study more accurate and reliable.Citation20
Data analysis and results
Data were analyzed using SPSS version 23.Citation21,Citation22 Data cleaning was also carried out before analysis was done. The checklist and the questionnaires were examined for completeness, accuracy and consistency of responses to detect and eliminate errors. Descriptive statistics were calculated with frequency distribution, and results were presented in tables and charts.
indicates that out of the 15 facilities engaged in this study, 40% did not record any staff absenteeism, while 53.3% and 6.7% recorded less than 10% and 10 to 20% levels of absenteeism, respectively. Even though immunization services were not disrupted in all 15 facilities, 9 (60%) made changes in the management of health care providers to contain the outbreak.
Table 1. Availability and access to EPI service at the Weija Gbawe municipality.
From , 34.6% of health workers were on maternity leave. During the period of the research, all pregnant women and lactating mothers were categorized into the maternity leave group since they are all maternity-related. Fear of contracting the disease (11.5%) and having been infected with the disease (19.2%) were reasons why staff were absent from work to receive counseling and treatment, respectively. The lockdown imposed by the government also prevented 3.8% of health workers from going to work due to limited transportation.
In reference to ; 53.3% of staff were reassigned to different units to work. In comparison, 6.7% were assigned to other facilities within the district to temporarily support discharging varying duties during the pandemic period to help contain the situation. Working hours were also increased among permanent staff (33.3%) and temporary staff (6.7%).
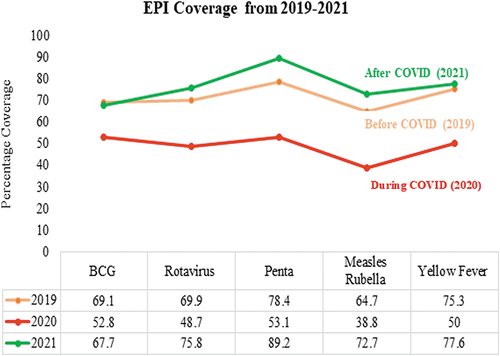
shows the coverage comparison between 2019, 2020 and 2021 for five selected antigens. It could be observed that 2020 being the pandemic year, experienced an overall decline in antigen coverages ranging from a coverage rate of 38.8% recorded for measles-rubella to 53.1% for Penta. 2019 recorded coverages ranging from 69.1% to 78.4%, which were relatively higher than 2020. After the intrusion of COVID-19 in 2021, coverages recorded were ranged from 67.7% for BCG to 89.2% for Penta.
Figure 2. Coverages of selected antigens for 2019, 2020 and 2021.
Discussion
Availability of EPI service providers
Early implementation of pandemic vaccines to frontline workers and other health service providers involved in regular immunizations are assured care should untoward incidents happen during disease outbreaks in the country. Besides, the health system faces logistical challenges, particularly in rural northern Ghana, which restricts the impact of immunization programs. In most remote locations, EPI outreach plans may not coincide with the exact moment a child is scheduled for a particular antigen.Citation23,Citation24 To keep their potency, most vaccinations must be kept at low temperatures. The antigen may have lost its effectiveness by the time it is administered to a child if the cold chain is interrupted due to a lack of infrastructure to maintain a resilient cold chain system.Citation23,Citation24
Socio-demographic/economic factors of mothers, socio-cultural factors, and health facility/system factors significantly hampers the successful implementation of immunization coverage in poor resource countries like Ghana.Citation25 According to referencesCitation25,Citation26 children delivered by traditional birth attendants (TBAs) outside the healthcare sector are more likely to miss immunization because their mothers become hesitant to immunize their children. Other factors, including spending long hours, communication gaps between healthcare givers and mothers (particularly regarding safety and efficacy information of the vaccination offered), and poor conduct of some health care providers, discourage mothers from bringing their wards for immunization services.Citation25,Citation26 Given all these known challenges, the COVID-19 pandemic has also contributed to the declined EPI coverages. Vacation, family commitments, sick leave – unrelated to COVID-19, sick leave – related to COVID-19, maternity leave, limited transportation due to lockdown, fear related to COVID-19, and fear related to violence targeting health workers were all cited as reasons for absenteeism in the Weija Gbawe Municipality (see figure ). The study results divulge that majority (34.6%) of health workers were asked to proceed on maternity leave during the pandemic following the president’s directive to protect the highly vulnerable population. Fear of contracting the disease (11.5%) and having been infected with the disease (19.2%) were reasons cited by staff for absenting themselves from work to receive counseling and treatment, respectively (see ). The government also imposed a lockdown restricting movement, preventing about 3.8% of health workers from delivering immunization services. These contributed to a massive decline in the staff strength to provide immunization services within the period. These findings are consistent with results from other studies to assess the impact of COVID-19 on routine immunization conducted in South-East Asia and the Western Pacific, which indicated that the highest-ranked reasons for disruption in the delivery of immunization services were fear of infection, movement/travel restrictions, and limited healthcare access.Citation27,Citation28
Availability and provision of EPI services
According to the World Health Organization (WHO), about half of all children in Sub-Saharan Africa (SSA) receive primary vaccination. Only one out of every twenty children in low- and middle-income countries (LMICs) has access to immunization.Citation29 Every year, more than 10 million children in low- and middle-income countries die due to a lack of access to effective therapies such as immunization to combat common and avoidable childhood illnesses.Citation30 Contrary to this, in Africa, children in urban areas are also more likely to be fully vaccinated than children in rural regions.Citation31,Citation32
This study’s results indicate that EPI coverages in the Weija Gbawe Municipality were affected by the COVID-19 pandemic. Immunization services were disrupted in all 15 selected health facilities, as indicated in . As a result, 60.0% absenteeism was recorded across the selected health facilities within the municipality for varying reasons. Although the Management of 9 facilities made changes such as reassigning staff on temporary secondment to a different facility, increasing over-time hours among entire time/part-time staff and reassigning staff to various units in the facility. The other six facilities Management could not make any changes to take care of the human resource deficit and hence operated under capacity.
Utilization for all five selected antigens in 2020 compared to 2019 experienced an overall decline in the year 2020 ranging from 38.8% recorded for measles rubella to 53.1% for Penta vaccine, which was during the COVID-19 pandemic period in Ghana (see ). This general decrease is attributed to the human resource deficit (absenteeism) created due to the COVID-19 pandemic as seen in . 2019 recorded coverages ranging from 69.1% to 78.4%, which were relatively higher than that of 2020, as shown in . This is in line with the findings of referenceCitation32 which demonstrate a negative difference in the monthly number of delivered doses between the current and prior year throughout the study period, alternatively, 2021 recorded higher coverages ranging from 67.7% for BCG to 89.2% for Penta.
According to referenceCitation33 deficient community awareness and fallacies that vaccines cause disease and doubts about vaccine effectiveness and safety have been identified as critical factors that hinder immunization uptake.Citation33 To improve access and utilization of immunization services, mass education in populations with low literacy levels, mainly women, a robust surveillance network, targeted community awareness programs, and involvement of dominant religious entities can help eliminate misbeliefs. Immunization services are primarily provided through costly outreaches and face logistic issues with a lack of details in micro-plans. It also has weak monitoring and supervision; and deficient human, operational, and other resources.Citation34 In Ghana, access and utilization of vaccination services are generally good, with complete vaccination coverage of 77% according to reference.Citation9 Access to the antigens is mainly through outreach programs, particularly in remote areas, and regular child clinic sessions at health care facilities.Citation23,Citation35
Study limitations
There was recall bias since respondents were asked to respond to past events.
Conclusion and recommendations
The results of this study divulge a substantial disruption in the provision of immunization services in the Weija Gbawe Municipality as a result of the COVID-19 pandemic. There was also a marginal decline in the administration of the various antigens, especially for measles and ROTA, in March 2020 when the outbreak began in Ghana and BCG in May 2020, two months after the outbreak. Even though there was continuous delivery of immunization services, most health workers were absent from work for several reasons. Notable among them were mandatory maternity leave, fear of contracting the disease, isolation and quarantine for those who had contracted the disease and limited access to transportation due to lockdown imposed by the government. The results of this study have informed the researchers to make the following recommendations to the stakeholders of health before and during a pandemic era:
Firstly, detailed micro-planning, partnership building, social mobilization, logistic support, and monitoring should be encouraged to improve the utilization of EPI services during disease outbreaks. Secondly, an adequate supply of Personal Protective Equipment (PPE’s) and other logistics should be made available to health workers to boost their confidence to deliver service amidst disease outbreaks. Again, special arrangements should be put in place to transport health workers to work during disease outbreaks to reduce absenteeism as a result of lack of access to transportation. Lastly, accurate up-to-date education and advice about vaccine efficacy should be communicated to healthcare workers using more user-friendly approaches, for example, via social media, given the importance of proper online messaging during the pandemic to deal with fear and anxiety resulting from misconception.
Authors’ contributions
Conceptualization, JK; formal analysis, investigation, and data curation, JK, KD, and VAA.; formal data analysis and results interpretation, JK, EO, KD and VAA.; writing, original draft preparation, JK and KD; writing, review and editing, JOM, and JNLL. All authors have read and agreed to the published version of the manuscript.
Consent for publication
All authors have provided their consent for the manuscript to be submitted for review and publication
Acknowledgements
We wish to render our sincere gratitude to the Management and Staff of the selected hospitals in the Weija Gbawe Municipality for their resources, time and contributions during the period of this research.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Yawson AE, Bonsu G, Senaya LK, Yawson AO, Eleeza JB, Banskota HK. Regional disparities in immunization services in Ghana through a bottleneck analysis approach: implications for sustaining national gains in immunization. Arch Public Health. 2017:1–7. doi:10.1186/s13690-017-0179-7.
- Legesse E, Dechasa W. An assessment of child immunization coverage and its determinants in Sinana District, Southeast Ethiopia. BMC Pediatr. 2015;15(1):1–14. doi:10.1186/s12887-015-0345-4.
- Meleko A, Geremew M, Birhanu F. Assessment of child immunization coverage and associated factors with full vaccination among children aged 12 – 23 months at Mizan Aman town. Bench Maji Zone, Southwest Ethiopia; 2017.
- Adokiya MN, Baguune B, Ndago JA. Evaluation of immunization coverage and its associated factors among children 12 – 23 months of age in Techiman Municipality, Ghana. Arch Public Health. 2017;75(1):1–10. doi:10.1186/s13690-017-0196-6.
- Brearley L, Eggers R, Steinglass R, Vandelaer J. Applying an equity lens in the decade of vaccines. Vaccine. 2013;31:B103–B107. doi:10.1016/j.vaccine.2012.11.088.
- WHO. Immunization in the context of COVID-19 pandemic. World Health Organization; 2020 [accessed 2022 March 4]. who.int/health-topics/immunization.
- Anderson VL. Promoting childhood immunizations. TJNP: J Nurse Pract. 2017;11(1):1–10. doi:10.1016/j.nurpra.2014.10.016.
- Bosu WK, Ahelegbe D, Edum-Fotwe E, Bainson KA, Turkson PK. Factors influencing attendance to immunization sessions for children in a rural district of Ghana. Acta Trop. 1997;68:259–67. doi:10.1016/s0001-706x(97)00094-6.
- Sally ET, Kenu E. Evaluation of access and utilization of EPI services amongst children 12-23 months in Kwahu Afram Plains, Eastern region, Ghana. Pan Afr Med J. 2017;28:238. doi:10.11604/pamj.2017.28.238.11538.
- Asuman D, Ackah CG, Enemark U. Inequalities in child immunization coverage in Ghana: evidence from a decomposition analysis. Health Econ Rev. 2018;8. doi:10.1186/s13561-018-0193-7.
- Adongo PB, Phillips JF, Aikins M, Arhin DA, Schmitt M, Nwameme AU, et al. Does the design and implementation of proven innovations for delivering basic primary health care services in rural communities fit the urban setting: the case of Ghana’s community-based health planning and services (CHPS). Health Res Policy Syst. 2014;12(1):1–10.
- Ghana Health Service. Annual report. Accra: Ghana Health Service; 2016:
- Creswell JW. Qualitative inquiry and research design: choosing among five approaches. 2nd. Thousand Oaks, CA: SAGE; 2007.
- Venkatesh V. Bridging the qualitative-quantitative divide: guidelines for conducting mixed methods research in information systems. MIS. 2013;37:21–54.
- Fornell C, Larcker F. Evaluating structural equation models with unobservable variables and measurement error. J Marketing Res. 1981;18:39–50.
- Selya AS, Rose JS, Dierker LC, Hedeker D, Mermelstein RJ. A practical guide to calculating Cohen’s f2, a measure of local effect size, from PROC MIXED. Educ Psychol Meas. 2012;3:1–6.
- Dollard MF, Bakker AB. Psychosocial safety climate as a precursor to conducive work environments, psychological health problems, and employee engagement. J Occup Organ Psychol. 2010; 83:579–99.
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Erlbaum; 1988.
- Idris MA, Dollard MF, Coward J, Dormann C. Psychosocial safety climate: conceptual distinctiveness and effect on job demands and worker psychological health. Saf Sci. 2012;50:19–28.
- Araujo P, Froyland L. Statistical power and analytical quantification. J Chromatogr. 2007;847:305–08.
- Arbuckle JL. IBM SPSS Amos 20 user’s guide. Amos Development Corporation, SPSS Inc. 2011;226–229.
- Pence B. Immunization status and child survival in rural Ghana immunization status and child survival in rural Ghana. 2001;147.
- Amugsi DA, Mittelmark MB, Lartey A. An analysis of socio-demographic patterns in child malnutrition trends using Ghana demographic and health survey data in the period 1993–2008. BMC Public Health. 2013;13:1–16.
- Lu G, Seyi S, Augustinus A, Alexander M, Maureen O, Zelee H, Samuel D, et al. Socio-Economic determinants and inequities in coverage and timeliness of early childhood immunisation in rural Ghana; 2014. doi:10.1111/tmi.12324.
- Edward KA, Yusuf OK, Bright OA, Abdul-Aziz S, Sanni Y. Decomposing the rural–urban gap in factors associated with childhood immunisation in sub-Saharan Africa: evidence from surveys in 23 countries. BMJ Com. 2021;6(1):e003773.
- Harris RC, Chen Y, Côte P, Ardillon A, Nievera MC, Ong-Lim A, Aiyamperumal S, Chong CP, Kandasamy KV, Mahenthiran K, et al. Impact of COVID-19 on routine immunisation in South-East Asia and Western Pacific, disruptions and solutions. Lancet Reg Health West Pac. 2021;10:100140. doi:10.1016/j.lanwpc.2021.100140.
- Shet A, Carr K, Danovaro-Holliday MC, Sodha SV, Prosperi C, Wunderlich J, Wonodi C, Reynolds HW, Mirza I, Gacic-Dobo M, et al. Impact of the SARS-CoV-2 pandemic on routine immunisation services: evidence of disruption and recovery from 170 countries and territories. Lancet Glob Health. 2021;10:e186–e194. doi:10.1016/S2214-109X(21)00512-X.
- WHO. Progress and Challenges with Achieving Universal Immunization Coverage: 2015 Estimates of Immunization Coverage. who.Int [assessed 2022 March 4].
- WHO. 2014. Immunization coverage. World Health Organization. [assessed 2022 March 4]. https://www.who.int›Newsroom›Factsheets›Detail.
- Budu E, Kofuor E, Darteh M, Ahinkorah BO, Seidu A, Dickson KS. Trend and determinants of complete vaccination coverage among children aged 12-23 months in Ghana: analysis of data from the 1998 to 2014. Ghana Demographic Health Surveys. 2020:1–12. doi:10.1371/journal.pone.0239754.
- Nthombenhle JN, Prakash MJ, Shabir AM, Barry DS, Anthony H, Muki SS, Gregory DH. Advances in childhood immunisation in South Africa. BMC Public Health Biomedcentral. 2012. doi:10.1186/1471-2458-12-578.
- Mukungwa T. Factors Associated with full Immunization coverage amongst children aged 12 – 23 months in Zimbabwe. Afr Popul Stud. 29(2): 2015.
- Mansour Z, Id JA, Id RS, Rady A, Hamadeh R, Gerbaka B, Bizri AR. Impact of COVID-19 pandemic on the utilization of routine immunization services; 2021. doi:10.1371/journal.pone.0246951.
- Tasneem SB. Implementation of the expanded program on immunization (EPI): understanding the enablers and barriers in a health system. Immunization-Vaccine Adjuvant Delivery Syst Strategies. 2018. doi:10.5772/intechopen.78676.
- Ota MO, Badur S, Romano-Mazzotti L, Friedland LR. Impact of COVID-19 pandemic on routine immunization. Ann Med. 2021;53:2286–97.