
ABSTRACT
Neighborhood social cohesion is a prominent psychosocial factor during the pandemic, and trust in neighbors is critical for implementing health prevention-related behaviors with public health messages. We planned to specifically explore the association between neighborhood social cohesion and vaccine acceptability among older adults (≥60 years) in China. Using a random stratified sampling method, an anonymous cross-sectional online survey was conducted in mainland China via a professional scientific data platform from May 25 to June 8, 2022. A revised Social Cohesion Scale was applied to evaluate the level of neighborhood social cohesion. Of the 3,321 recruited respondents aged 60 and above, 82.8% (95% CI: 81.5–84.1) reported their willingness to be vaccinated. With all significant covariates adjusted, older adults with moderate (aOR = 1.77, 95% CI: 1.04–3.04) and high level of social cohesion (aOR = 2.21, 95% CI: 1.29–3.77) were more likely to receive the booster dose. Our findings remained robust in a series of models after controlling for different covariates. Uncertainty about contraindications (38.3%), underestimation of their vulnerability (33.1%), and concerns about vaccine safety (32.0%) were the three main reasons for vaccine hesitancy. Therefore, building a harmonious community environment, strengthening neighborhood communication and exchange, and making good use of peer education among neighbors may become a breakthrough to promote herd immunity, especially for vulnerable older adults with limited social networks.
Introduction
Coronavirus disease 2019 (COVID-19), a prominent infectious disease with profound health implications, has directly infected nearly 621.46 million people as of 10 October 2022, with approximately 6.56 million deaths.Citation1 As a result of the continual adaptive evolution of SARS-CoV-2, it is the Omicron variant that is now prevalent worldwide and has been recognized to be more contagious, insidious, and atypical than the wild strain and previous variants.Citation2–4 The elderly population is at high risk of SARS-CoV-2 infection, severe illness, and death, most notably due to their low immunity and preexisting diseases that tend to cause complications or exacerbate their poor conditions.Citation5–8 Vaccination is well recognized as the most cost-effective public health intervention to control infectious diseases and protect people’s lives and property.Citation9 However, the elderly population remained vulnerable in breakthrough infection after initial vaccination, as the protection derived from vaccines decreased over time.Citation10 Vaccine hesitancy was defined as one of the top ten threats to global health in 2019, especially for older adults who have more concerns or underestimate the poor prognosis of COVID-19.Citation11 As of 8 October 2022, only 32.3% of the global population had received a booster dose of COVID-19,Citation12 and 32.8% of older adults (≥60 years) in China still had not received the booster dose as of 29 September 2022Citation8. Given the current more infectious variant, decreased vaccine-induced antibody titers, and the special social status of elderly individuals, the Chinese government has continued to encourage older people to get vaccinated, especially for the booster shots.Citation8,Citation13 Communities have also launched a series of campaigns to increase vaccination rates among older people.Citation8,Citation13,Citation14
Community characteristics influenced a range of health behaviors and outcomes of residents, but previous studies mainly focused on the negative effects, such as violence, noise, poor air quality, and vandalism.Citation15–20 Health-enhancing effects caused by positive neighborhood characteristics such as neighborhood social cohesion were neglected. Neighborhood social cohesion is defined as the degree of perceived connection between neighbors and the willingness of people to intervene for shared benefits.Citation21 To some extent, neighbors served as a source of support for adults, and older adults with limited social circles were even more pronounced in this regard.Citation15 Recently, the role of neighborhood social cohesion has gained significant attention in the field of public health. Studies have shown that higher social cohesion and trust in others were associated with various health outcomes, including self-reported health status, frailty, depression, cardiovascular disease, etc.Citation15–20 However, the mechanisms underlying the association between neighborhood social cohesion and behaviors on disease prevention are still unclear. One possible explanation is the increased dissemination of information about effective preventive services, social and psychological support, collective ability to advocate for resources, and maintenance of health norms through informal social control.Citation15
To date, no studies have specifically investigated whether there is an association between neighborhood social cohesion and vaccine acceptability, which may become a breakthrough to promote the process of achieving herd immunity, especially for vulnerable older adults with limited social networks. Therefore, we conducted an online anonymous survey in China to assess the extent to which neighborhood social cohesion in this specific group (≥60 years old) influenced their willingness to receive the booster shots.
Methods
Study design and participants
This cross-sectional online survey was conducted in mainland China via a professional and paid scientific data platform called Wen Juan Xing (Changsha Ranxing Information Technology Co., Ltd., Hunan, China). Electronic questionnaires were randomly distributed over the Internet to potential study subjects who were included in this large, diverse, and intelligent sample bank. The recruitment criteria were as follows: (1) understanding the study purpose and being willing to fill in the questionnaire carefully; (2) ≥60 years old; and (3) completed the survey from May 25 to 8 June 2022. The purpose and data use of this survey were clearly stated in the preface of each questionnaire. By completing the questionnaire, the respondents consented to the researcher’s subsequent academic use of the anonymized data.
Based on the vaccine acceptance findings of previous studies, in PASS software 15.0 (NCSS LLC., Kaysville, U.T., USA) was used to calculate the minimum sample size with acceptance rate as 89%,Citation22,Citation23 α as 0.05 and the confidence interval width as 0.1p (0.089). Participants from all 31 provinces in mainland China were collected in a stratified and random way regarding the proportion of older adults (≥60 years old) reported in the Seventh National Census. After quality control and manual check procedures, a total of 3,321 eligible respondents were ultimately included in our analysis (Table S1).
Neighborhood social cohesion
Originally developed by Buckner, the Neighborhood Cohesion Instrument was modified by Fone et al in 2007, and has been derived into the Social Cohesion Scale and Neighborhood Belonging Scale.Citation24–26 We used an adapted Social Cohesion Scale, which has been used cross-culturally with good validity and internal consistency (Cronbach’s α: 0.84–0.95),Citation16,Citation25 to evaluate the neighborhood social cohesion of Chinese senior citizens. Social Cohesion Scale is a five-point Likert scale with eight questions in total (Table S2). Each item is assigned a score ranging from 1 to 5, which indicates an increasing approval from “the most disagreement (1 score)” to “the most agreement (5 scores).” All items were pooled with equal weighting, resulting in a total social cohesion score ranging from 8 to 40Citation24. For statistical analysis, all eligible respondents were divided equally into three groups according to the analytical method of Fone et al: Low (8–18 scores), Moderate (19–29 scores) and High (30–40 scores).
Willingness to receive the booster dose of COVID-19 vaccines
We set the question “would you be willing to receive the booster dose of the COVID-19 vaccine if available?” to determine participants’ vaccination intentions. Acceptance rate was defined as the proportion of participants who answered “Yes” among all respondents. For participants who answered “No” or “Not sure,” the specific reasons for the reluctance were further asked.
Covariates
Individual characteristics, including region, age, sex, marital status, education level, monthly household income per capita (RMB), principal source of income, and history of chronic diseases (diabetes mellitus, hypertension, dyslipidemia, cardiovascular diseases, etc.) were administered. Respondents were also required to recall the average amount of time per day they spent on social media acquiring information about vaccines and the main type of social media in use (official social media, professional social media, public social media, or others). Knowledge about the COVID-19 and COVID-19 vaccines may also influence older adults’ attitudes toward the booster shots.Citation27 Therefore, a total of 10 items (23 points) were set to evaluate the knowledge level of participants. The sources of infection, transmission routes, high-risk groups, prevention and control measures, vaccine effectiveness, and other important precautions were all included in this section. Each correct answer that matched the pre-set option was assigned with 1 point, and the total score was equally divided into three levels.Citation28,Citation29 Finally, those who scored 0–7, 8–15 and 16–23 were assigned to the “Low,” “Moderate” and “High” groups, respectively.
Data analysis
All variates, consisting of the primary variates (level of neighborhood social cohesion and vaccine acceptance) and covariates mentioned above, were reported with frequencies and percentages, and the chi-square test was used to compare the group differences. Multivariable logistic regression analyses were used to explore the associations between people’s neighborhood social cohesion and acceptance rate. Adjusted odds ratios (aORs) with 95% CIs were calculated to evaluate the effect size. To examine the robustness of the estimations, a series of potential confounding factors were adjusted in different models. Model 1 was unadjusted. Then, we added sociodemographic factors (age, education, monthly household income per capita, and principal source of income) in Model 2. The knowledge scores and the abovementioned sociodemographic factors were adjusted In Model 3. The source of vaccine information was additionally added into Model 4. Then, time for social media to acquire information on COVID-19 and COVID-19 vaccines was finally controlled in Model 5 on the basis of Model 4. All statistical analyses were conducted by SPSS 26.0 (IBM SPSS Inc., New York, USA), and a two-sided P value <0.05 indicated statistical significance.
Results
Basic characteristics of the study population
Of the 3,321 recruited respondents aged 60 and above, 52.1% were female, 69.0% lived with their spouses, and 40.2% had at least a high school degree (). Among them, 2750 (82.8%) were struggling in at least one chronic disease, and surprisingly, more than half had a relatively adequate understanding of COVID-19 and the vaccines. Only 74 (2.2%) of these participants experienced a low level of neighborhood social cohesion. shows the characteristics of the subjects stratified into three groups by Social Cohesion Scale scores. People with a higher level of neighborhood social cohesion were clustered with older age, higher education level, lower family income, shorter time on social media, and higher scores for COVID-19 knowledge. Older adults with different regions, genders, marital status, and chronic medical history were evenly distributed among the three groups of neighborhood social cohesion.
Table 1. Characteristics and vaccine acceptance toward the booster dose of 3,321 older people in China.
Table 2. Characteristics of the study population according to level of neighborhood social cohesion.
Willingness to be vaccinated
For 3,321 eligible respondents, 82.8% reported their willingness to be vaccinated, which increased with age, education level, time spent on social media, and knowledge scores (all P trend <0.05) (). People who lived with their spouses (84.8%) and used the money of themselves or their spouses (84.8%) were more likely to accept the booster dose. Participants with high neighborhood social cohesion exhibited a higher willingness than the other two groups (P trend <0.001). There was no significant difference in inoculation intention among people grouped by region, gender, household income, and chronic disease history.
Relationship between neighborhood social cohesion and the willingness to receive the booster dose of COVID-19 vaccination
As shown in , the neighborhood social cohesion of the older population was positively associated with their acceptance rate toward the booster dose of COVID-19 vaccines in the unadjusted model (moderate: cOR = 1.75, 95% CI: 1.04–2.93; high: cOR = 2.35, 95% CI: 1.40–3.92). After further multivariable adjustment for sociodemographic factors in Model 2, older adults with moderate (aOR = 1.83, 95% CI: 1.08–3.11) and high social cohesion (aOR = 2.41, 95% CI: 1.43–4.08) were still more likely to be vaccinated. Similar results were also observed in Model 3 and Model 4 by sequentially adding knowledge scores and sources of vaccine-related information while retaining the original covariates. With all significant covariates controlled in Model 5, neighborhood social cohesion was still positively associated with the inoculation intention among the older Chinese population (moderate: aOR = 1.77, 95% CI: 1.04–3.04; high: aOR = 2.21, 95% CI: 1.29–3.77). And as it was shown in Table S3, the abovementioned association was not modified by all covariates that were unevenly distributed in different cohesion groups. (all P for interaction >0.05). Additionally, age, primary income source, knowledge related to COVID-19, and source of COVID-19 vaccine information also affected older adults’ vaccination willingness (Table S4).
Table 3. OR (95%CI) for the acceptance toward the booster dose of COVID-19 vaccines according to neighborhood social cohesion.
Reasons for vaccination hesitancy
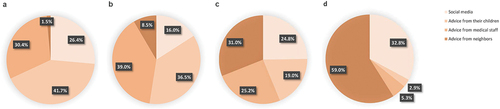
Among the 571 participants who were reluctant (56.4%) or refused (43.6%) to receive the booster dose, 33.1% believed that the initial dose was already sufficient, 32.0% worried about the safety of the COVID-19 vaccine, and 38.3% hesitated because of their susceptibility to vaccination (). Concerns about their serious illnesses or contraindications to vaccination were the most common reason why older adults refused to get vaccinated, while overestimation of the effectiveness of the initial dose or underestimation of the infectivity of the virus was the main reason for reluctance. For people aged 60 and above, only 1.5% and 8.5% of 3,321 participants placed advice from neighbors in the top 2 factors they considered most important in influencing their vaccination (). Advice from social media, children and professional staff were the more important factors self-reported by these older adults ().
Figure 1. Reasons for responding “No” or “Not sure” toward the COVID-19 vaccine booster shots (n = 571).
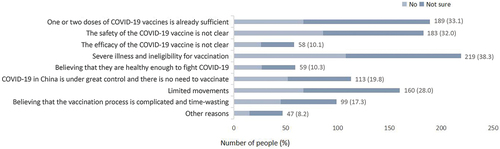
Figure 2. Ranking of the influence degree of four factors on the willingness of the elderly to booster vaccination. (a) the most important; (b) the second important (c) the third important (d) the least important.
Discussion
To our knowledge, this is the first study to specifically explore the association between neighborhood social cohesion and the acceptance rate toward the booster dose of the COVID-19 vaccines. We found that 2750 (82.8%) of all participants reported their positive inoculation intention. Concerns about contraindications, vaccine safety, and underestimation of the infectivity of COVID-19 were the main reasons causing hesitancy. With all significant covariates adjusted in Model 5, the vaccine acceptance rate of the booster dose was closely associated with a higher level of neighborhood social cohesion, and the results remained robust in a series of models after controlling for different covariates. Thus, a good neighborhood relation and cohesion may become a sally port with practical and theoretical implications to promote the vaccination coverage of booster doses among older populations.
Neighborhood social cohesion is a prominent psychosocial factor during this pandemic, and trust in neighbors is critical for social cohesion and for implementing health prevention-related behaviors with public health messages.Citation30,Citation31 According to our results, the neighborhood social cohesion of older adults was significantly and positively associated with their vaccination acceptance toward the booster dose of COVID-19 vaccines. A growing number of studies have reported the important role of harmonious, supportive, and communicative neighborhoods in the field of public health and disease prevention.Citation15–20 Higher social cohesion was correlated with better health outcomes, including self-rated health status, frailty, depression, and cardiovascular disease, etc.Citation32–35 Eric et al. showed that each standard deviation increase in neighborhood social cohesion was associated with a higher likelihood of people receiving flu vaccinations (aOR = 1.09, 95% CI: 1.04–1.15) or cholesterol testing (aOR = 1.10, 95% CI: 1.02–1.19), and women were more likely to undergo mammography (aOR = 1.10, 95% CI: 1.01–1.19) or Pap smear (aOR = 1.08, 95% CI: 1.00–1.17).Citation15 However, the mechanisms underlying the association between neighborhood social cohesion and such health behaviors remain inconclusive. One of the more discussed explanations is that perceived neighborhood social cohesion, particularly with neighbors, can be characterized as a form of social support that may influence health outcomes and well-being by facilitating access to health-related information and services.Citation15,Citation25 There is a consensus on the role of social support in maintaining the health of older adults in the community. People in vulnerable groups often share a strong sense of collective consciousness.Citation36,Citation37 Practically, many older adults were not aware of the importance of neighbors’ advice in influencing their health-related behaviors, and this may be a breakthrough for community workers to advance vaccine coverage among the older population.
In this study, 82.8% of 3,321 respondents exhibited a higher willingness toward the booster dose. In Taizhou, China, only 10.3% of adults aged 40 years and older hesitated to receive booster shots, and in another national study, the acceptance of the booster vaccination was as high as 89.44% in the subgroup of older adults (>60 years).Citation22,Citation23 And this level of behavioral intention is also comparable to that of the factory workers in China (84.0%) and to that of healthcare providers in the United States (83.6%) and medical students in Japan (90.7%).Citation38–40 However, our results differed from those of the Jordanian and Bangladeshi studies, where Chinese elderly were significantly more receptive to the booster dose than those two countries.Citation41,Citation42 As of 8 October 2022, only 32 out of every 100 people in the world had received booster shots, and nearly 35% of people aged 60 years and older were still not vaccinated with booster shots in China.Citation8,Citation12 Although the results of our study showed a high overall acceptance of the booster dose of COVID-19 vaccines among the elderly in China, more efforts are still needed to advance the process of herd immunization given the large population base and the special characteristics of elderly individuals. In addition, a trigger is also needed to promote intentions to real-world actions. Community-dwelling older adults aged 65 years or above in Hong Kong reported a lower uptake of COVID-19 vaccine booster dose than their younger counterparts.Citation43 Existing COVID-19 booster dose health promotional materials might not adequately address older adults’ main concerns.Citation43 Except for neighborhood social cohesion, the focus on older citizens, strengthening community dissemination of COVID-19 and vaccine-related knowledge, and standardizing the content of medical professional social media are also effective measures to increase vaccine coverage, especially among the elderly population.
According to our results, more than half of the 571 (17.2%) who self-reported that they were not currently willing to receive a booster vaccination answered “Not sure,” implying that these participants’ attitudes toward the booster dose were ambiguous. Three main reasons for their hesitation were underestimation of the perceived infectiousness of the variants and lack of understanding of the weakened immunity induced by vaccine, perceived contraindications, and limited movements. Clearly, it is imperative to enhance knowledge dissemination among this population so that they can understand their vulnerability in the context of a pandemic.Citation5,Citation6 Additionally, community and primary health care facilities ought to consider their limited mobility and the difficulty in handling a range of preparedness on smart devices. Timely, appropriate, and special care is necessary for those old adults. Moreover, for all seniors who refused or hesitated to be vaccinated, there was a high percentage of concerns about safety and uncertainty about whether they met the vaccination requirements. Elderly individuals may subjectively and arbitrarily judge their contraindications to inoculation, and patients with chronic diseases that are well controlled by medication are usually not contraindicated for vaccines.Citation44 Therefore, in addition to popularizing the safety and effectiveness of vaccines, medical professionals are supposed to have insight into the real physical conditions of the elderly and make a scientific judgment on whether they can be vaccinated at present.Citation44
As an online survey based on a professional data science company, some quality control measures were set directly in the backend, including the uniqueness of IP addresses, compulsory questions, logical jumps, etc. It reduced the waste of resources for all parties. Second, the results of this study were relevant and applicable. Our findings could be directly used to guide the improvement of vaccination coverage in the elderly population, and they also provide promotional ideas for other possible vaccination plans in the future, such as vaccines against the Omicron variant or other infectious diseases. Inevitably, there are some limitations to this study. First, it was a cross-sectional study, and the association between neighborhood social cohesion and vaccine acceptance could only serve as a hint of a potential causal link. Second, the accessibility of the target population has always been one of the major limitations of online surveys since questionnaires were answered only by Internet users. The usage of smartphone/Internet may be limited among older adults in China, especially among those who are older and living in less developed areas. In addition, older people who registered might be more educated than other general older populations. Although this sample may be limited in representation, we have done our best to compensate with a large sample size. Several studies have shown that people who were older, poorly educated and those living in rural or less developed areas were less likely to be vaccinated.Citation22,Citation43,Citation45 Therefore, there is a certain selection bias in our study. The vaccination acceptance rate and the positive association between vaccination willingness and neighborhood social cohesion may be overestimated to some extent. Further large-scale offline surveys with more participants are supposed to be implemented to verify the association between vaccination intentions and specific aspects of neighborhood social cohesion among the general population, and to reasonably include more covariates that are unevenly distributed between groups for adjustments.
Conclusions
In total, 82.8% of older people (≥60 years old) in China exhibited a high willingness toward the booster dose of COVID-19 vaccines. The neighborhood social cohesion among the older population was positively associated with the vaccination acceptance rate. Therefore, building a harmonious community environment, strengthening neighborhood communication and exchange, and making good use of peer education among neighbors may become a breakthrough to promote herd immunity, especially for vulnerable older adults with limited social networks.
Author contributions
Conceptualization, C.Q., and J.L.; methodology and analysis, C.Q., and J.L.; visualization, C.Q., and W.Y.; writing-original draft preparation, C.Q.; review and editing, L.T., M.D., Y.W., and Q.L.; supervision, M.L., and J.L. All authors have read and agreed to the published version of the manuscript.
Institutional review board statement
This study met the requirements of the Declaration of Helsinki and was approved by the Ethics Committee of Peking University (IRB00001052-21126).
Supplemental Material
Download PDF (200.6 KB)Acknowledgments
We would like to express our sincere gratitude to all the participants who enrolled in this study.
Data availability statement
All data in the study are available from the corresponding author by request.
Disclosure statement
No potential conflict of interest was reported by the author(s)
Supplementary material
Supplemental data for this article can be accessed on the publisher’s website at https://doi.org/10.1080/21645515.2022.2140530
Additional information
Funding
References
- University JH. COVID-19 Dashboard; 2022 Oct 10 [accessed 2022 Oct 10]. https://coronavirus.jhu.edu/map.html
- Organization WH. Tracking SARS-CoV-2 variants; 2022 Aug 31 [accessed 2022 Aug 31]. https://www.who.int/activities/tracking-SARS-CoV-2-variants.
- Araf Y, Akter F, Tang YD, Fatemi R, Parvez MSA, Zheng C, Hossain MG. Omicron variant of SARS-CoV-2: genomics, transmissibility, and responses to current COVID-19 vaccines. J Med Virol. 2022;94(5):1–8. doi:10.1002/jmv.27588.
- Chen J, Wang R, Gilby NB, Wei G-W. Omicron variant (B.1.1.529): infectivity, vaccine breakthrough, and antibody resistance. J Chem Inf Model. 2022;62(2):412–22. doi:10.1021/acs.jcim.1c01451.
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. Jama. 2020;323(13):1239–42. doi:10.1001/jama.2020.2648.
- Ramasamy MN, Minassian AM, Ewer KJ, Flaxman AL, Folegatti PM, Owens DR, Voysey M, Aley PK, Angus B, Babbage G, et al. Safety and immunogenicity of ChAdox1 nCov-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): a single-blind, randomised, controlled, phase 2/3 trial. Lancet. 2021;396(10267):1979–93. doi:10.1016/s0140-6736(20)32466-1.
- O’Driscoll M, Ribeiro Dos Santos G, Wang L, Cummings DA, Azman AS, Paireau J, Fontanet A, Cauchemez S, Salje H. Age-specific mortality and immunity patterns of SARS-CoV-2. Nature. 2021;590(7844):140–45. doi:10.1038/s41586-020-2918-0.
- Joint prevention and control mechanism of the state council (September29,2022); 2022 Sep 29 [accessed 2022 Oct 8]. http://www.gov.cn/xinwen/gwylflkjz208/index.htm
- Rauch S, Jasny E, Schmidt KE, Petsch B. New vaccine technologies to combat outbreak situations. Front Immunol. 2018;9:1963. doi:10.3389/fimmu.2018.01963.
- Feikin DR, Higdon MM, Abu-Raddad LJ, Andrews N, Araos R, Goldberg Y, Groome MJ, Huppert A, O’Brien KL, Smith PG, et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: results of a systematic review and meta-regression. Lancet. 2022;399(10328):924–44. doi:10.1016/s0140-6736(22)00152-0.
- Organization WH. Ten Threats to global health in 2019; 2021.
- Data OWI. COVID-19 vaccine boosters administered; 2022 Oct 8 [accessed 2022 Oct 10]. https://ourworldindata.org/covid-vaccinations
- Council tJPaCMotS. Effective Prevention of severe illness: china continues to encourage the elderly to get vaccinated; 2022April 7 [accessed 2022 Oct 8]. http://www.gov.cn/xinwen/2022-04/07/content_5683922.htm
- Council tJPaCMotS. Heartwarming measures to encourage elderly people to get vaccinated against COVID-19; 2022May 7 [accessed 2022 Aug 10]. http://www.gov.cn/xinwen/2022-05/07/content_5689000.htm
- Kim ES, Kawachi I. Perceived neighborhood social cohesion and preventive healthcare use. Am J Prev Med. 2017;53(2):e35–40. doi:10.1016/j.amepre.2017.01.007.
- Kim ES, Hawes AM, Smith J. Perceived neighbourhood social cohesion and myocardial infarction. J Epidemiol Community Health. 2014;68(11):1020–26. doi:10.1136/jech-2014-204009.
- Lochner KA, Kawachi I, Brennan RT, Buka SL. Social capital and neighborhood mortality rates in Chicago. Social Sci Med. 2003;56(8):1797–805. doi:10.1016/S0277-9536(02)00177-6.
- Inoue S, Yorifuji T, Takao S, Doi H, Kawachi I. Social cohesion and mortality: a survival analysis of older adults in Japan. Am J Public Health. 2013;103(12):e60–6. doi:10.2105/ajph.2013.301311.
- de Leon CF M, Cagney KA, Bienias JL, Barnes LL, Skarupski KA, Scherr PA, Evans DA. Neighborhood social cohesion and disorder in relation to walking in community-dwelling older adults: a multilevel analysis. J Aging Health. 2009;21(1):155–71. doi:10.1177/0898264308328650.
- Echeverría S, Diez-Roux AV, Shea S, Borrell LN, Jackson S. Associations of neighborhood problems and neighborhood social cohesion with mental health and health behaviors: the multi-ethnic study of atherosclerosis. Health Place. 2008;14(4):853–65. doi:10.1016/j.healthplace.2008.01.004.
- Kawachi I, Subramanian SV. Neighbourhood influences on health. J Epidemiol Community Health. 2007;61(1):3–4. doi:10.1136/jech.2005.045203.
- Wu J, Li Q, Silver Tarimo C, Wang M, Gu J, Wei W, Ma M, Zhao L, Mu Z, Miao Y. COVID-19 vaccine hesitancy among Chinese population: a large-scale national study. Front Immunol. 2021;12:781161. doi:10.3389/fimmu.2021.781161.
- Tung TH, Lin XQ, Chen Y, Zhang M-X, Zhu J-S. Willingness to receive a booster dose of inactivated coronavirus disease 2019 vaccine in Taizhou, China. Expert Rev Vaccines. 2022;21(2):261–67. doi:10.1080/14760584.2022.2016401.
- Fone D, Dunstan F, Lloyd K, Williams G, Watkins J, Palmer S. Does social cohesion modify the association between area income deprivation and mental health? A multilevel analysis. Int J Epidemiol. 2007;36(2):338–45. doi:10.1093/ije/dym004.
- Yu R, Cheung O, Leung J, Tong C, Lau K, Cheung J, Woo J. Is neighbourhood social cohesion associated with subjective well-being for older Chinese people? The neighbourhood social cohesion study. BMJ Open. 2019;9(5):e023332. doi:10.1136/bmjopen-2018-023332.
- Buckner JC. The development of an instrument to measure neighborhood cohesion. Am J Community Psychol. 1988;16(6):771–91. doi:10.1007/BF00930892.
- Wang R, Qin C, Du M, Liu Q, Tao L, Liu J. The association between social media use and hesitancy toward COVID-19 vaccine booster shots in China: a web-based cross-sectional survey. Hum Vaccin Immunother. 2022;18(5):2065167. doi:10.1080/21645515.2022.2065167.
- Tao L, Wang R, Liu J. Comparison of vaccine acceptance between COVID-19 and seasonal influenza among women in China: a national online survey based on health belief model. Front Med (Lausanne). 2021;8:679520. doi:10.3389/fmed.2021.679520.
- Tao L, Wang R, Han N, Liu J, Yuan C, Deng L, Han C, Sun F, Liu M, Liu J. Acceptance of a COVID-19 vaccine and associated factors among pregnant women in China: a multi-center cross-sectional study based on health belief model. Hum Vaccin Immunother. 2021;17(8):2378–88. doi:10.1080/21645515.2021.1892432.
- Stephen G, Siobhán H, Muldoon OT, Whittaker AC. Social cohesion and loneliness are associated with the antibody response to COVID-19 vaccination. Brain Behav Immun. 2022;103:179–85. doi:10.1016/j.bbi.2022.04.017.
- Muldoon OT, Bradshaw D, Jay S, Kinsella EL, Maher P, Murphy R, Taaffe C, O’Donnell P. Vaccination roll-out: a time to develop and maintain trust in science and health care. Br J Gen Pract. 2021;71(712):518–19. doi:10.3399/bjgp21X717629.
- Chuang YC, Chuang KY, Yang TH. Social cohesion matters in health. Int J Equity Health. 2013;12(1):87. doi:10.1186/1475-9276-12-87.
- Feng Z, Vlachantoni A, Liu X, Jones K. Social trust, interpersonal trust and self-rated health in China: a multi-level study. Int J Equity Health. 2016;15(1):180. doi:10.1186/s12939-016-0469-7.
- Miller HN, Thornton CP, Rodney T, Thorpe RJ, Allen J. Social cohesion in health: a concept analysis. ANS Adv Nurs Sci. 2020;43(4):375–90. doi:10.1097/ans.0000000000000327.
- Williams AJ, Maguire K, Morrissey K, Taylor T, Wyatt K. Social cohesion, mental wellbeing and health-related quality of life among a cohort of social housing residents in Cornwall: a cross sectional study. BMC Public Health. 2020;20(1):985. doi:10.1186/s12889-020-09078-6.
- Walker RB, Hiller JE. Places and health: a qualitative study to explore how older women living alone perceive the social and physical dimensions of their neighbourhoods. Social Sci Med. 2007;65(6):1154–65. doi:10.1016/j.socscimed.2007.04.031.
- Gardner PJ. Natural neighborhood networks — Important social networks in the lives of older adults aging in place. J Aging Stud. 2011;25(3):263–71. doi:10.1016/j.jaging.2011.03.007.
- Zhang K, Fang Y, Chan PS, Cao H, Chen H, Hu T, Chen Y, Zhou X, Wang Z. Behavioral intention to get a booster dose of COVID-19 vaccine among Chinese factory workers. Int J Environ Res Public Health. 2022;19(9):5245. doi:10.3390/ijerph19095245.
- Pal S, Shekhar R, Kottewar S, Upadhyay S, Singh M, Pathak D, Kapuria D, Barrett E, Sheikh AB. COVID-19 vaccine hesitancy and attitude toward booster doses among us healthcare workers. Vaccines (Basel). 2021;9(11):1358. doi:10.3390/vaccines9111358.
- Kanyike AM, Olum R, Kajjimu J, Ojilong D, Akech GM, Nassozi DR, Agira D, Wamala NK, Asiimwe A, Matovu D, et al. Acceptance of the coronavirus disease-2019 vaccine among medical students in Uganda. Trop Med Health. 2021;49(1):37. doi:10.1186/s41182-021-00331-1.
- Hossain MB, Alam MZ, Islam MS, Sultan S, Faysal MM, Rima S, Hossain MA, Mamun AA. COVID-19 vaccine hesitancy among the adult population in Bangladesh: a nationwide cross-sectional survey. Plos One. 2021;16(12):e0260821. doi:10.1371/journal.pone.0260821.
- Rababa’h AM, Abedalqader NN, Ababneh M. Jordanians’ willingness to receive heterologous prime-boost COVID-19 vaccination and vaccine boosters. Eur Rev Med Pharmacol Sci. 2021;25(23):7516–25. doi:10.26355/eurrev_202112_27452.
- Wang Z, Fang Y, Yu FY, Chan PSF, Chen S, Sun F. Facilitators and barriers to take up a COVID-19 vaccine booster dose among community-dwelling older adults in Hong Kong: a population-based random telephone survey. Vaccines (Basel). 2022;10(6):966. doi:10.3390/vaccines10060966.
- COVID-19 Vaccines Technical Guidence (Version 1); 2021 March 3 [accessed 2022 Aug 31]. http://www.nhc.gov.cn/xcs/yqfkdt/202103/c2febfd04fc5498f916b1be080905771.shtml
- Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, Kimball S, El-Mohandes A. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2021;27(2):225–28. doi:10.1038/s41591-020-1124-9.