
ABSTRACT
Routine childhood vaccination improves health and prevents morbidity and mortality from vaccine-preventable diseases. There are indications that the COVID-19 pandemic has negatively impacted immunization rates globally, but systematic studies on this are still lacking in Canada. This study aims to add knowledge on the pandemic’s effect on children’s immunization rates with pneumococcal vaccine using self-reported immunization data from CANImmunize. An interrupted time series analysis was conducted on aggregated monthly enrollment of children on the platform (2016–2021) and their pneumococcal immunization series completion rates (2016–2020). Predicted trends before and after the onset of the COVID19-related restriction (March 1, 2020) were compared by means of an Autoregressive Integrated Moving Average (ARIMA). The highest monthly enrollment was 3,474 new infant records observed in January 2020, and the lowest was 100 records in December 2021. The highest Self-reported pneumococcal immunization series completion rate was 78.89%, observed in February 2017, and the lowest was 6.94% in December 2021. Enrollment decreased by 1177.52 records (95% CI: −1865.47, −489.57), with a continued decrease of 80.84 records each month. Completion rates had an immediate increase of 14.57% (95% CI 4.64, 24.51), followed by a decrease of 3.54% each month. The onset of the COVID-19 related restrictions impacted the enrollment of children in the CANImmunize digital immunization platform and an overall decrease in self-reported pneumococcal immunization series completion rates. Our findings support efforts to increase catch-up immunization campaigns so that children who could not get scheduled immunization during the pandemic are not missed.
Background
Immunizing children against routine vaccine-preventable diseases (VPDs) has been among the most effective interventions in reducing childhood morbidity and mortality and indirectly saving the world a substantial economic loss.Citation1 Between 2000 and 2020, in developing countries, the use of routine childhood vaccines against measles, pneumonia, severe diarrhea, and meningitis has averted approximately 20 million deaths and saved around US$ 350 billion in the cost of illness.Citation2,Citation3 This achievement was possible because of the successful mobilization of beneficiaries, excellent planning, and execution of childhood immunization programs.Citation4
In the past two decades, routine childhood immunization has successfully cut pediatric deaths and placed Canada on the elimination journey for VPDs such as measles, rubella, and polio.Citation5 That was due to the equitable access to childhood vaccines achieved through the publicly funded immunization programs.Citation6 However, VPDs have been increasing in the last decade, with 20.7 cases per 100,000 population from 2013, with Invasive Pneumococcal Disease (IPD) accounting for more cases (44%) and mainly among children less than one year of age (92.4 cases per 100,000 population).Citation7 In collaboration with provinces and territories, the Canadian federal government has established a National Immunization Strategy for 2016–2025 to reach goals such as the 95% coverage for childhood vaccines.Citation8 Key actions were set to address vaccination uptake, which is mainly impeded by vaccination hesitance and refusal.Citation9
Unfortunately, in March 2020, the outbreak of the highly infectious and deadly Coronavirus disease of 2019 (COVID-19) emerged as an unprecedented challenge.Citation10 Countries governments across the world adopted the World Health Organization (WHO)’s public health and social measures to limit the spread of SARS-CoV-2 and mitigate its associated health loss.Citation11,Citation12 Those measures included face mask-wearing; restrictions on public and private gatherings; cautious opening and closure of schools and businesses; domestic movements as well as public transport restrictions, and stay-at-home orders; and international travel restrictions.Citation12 Two years into the pandemic, the world has already recorded more than 400 million cases, a death toll surpassing 6 million, and the disruption of many preventive interventions, such as routine immunization programs for children.Citation12,Citation13
Disruptions to the routine childhood vaccines started right after the onset of the pandemic, affecting vaccines’ supply and demand, their cold chain, and delivery.Citation4,Citation14 Consequently, 23 million children did not receive their scheduled vaccines,Citation15 the number of doses administered globally fell by 31.3%,Citation16 and vaccination coverage dropped by approximately 7.7%.Citation16 A drop in ordering vaccines was also noted in countries such as the USA, where a 50% reduction happened right after the onset of pandemic-related restrictions.Citation14
As observed in many countries, the effect of the COVID-19 restrictions on vaccination rates created an initial shock after the onset of restrictions or delayed recovery of the service after a few months of the pandemic. In some countries, such as Canada, such data on childhood vaccines is still lacking. There is a possibility that the national goal of achieving community protection against all VPDs by 2025 could have been disrupted by the onset of the pandemic-related restrictions,Citation8 as restrictions caused an approximately 80% drop in in-person doctor visits for children’s services, including vaccination during the first wave of infections.Citation17 Alternatively, the pandemic’s restrictions in Canada might not have significantly refrained the country’s overall immunization rates, as observed in the later data on infants’ immunization rates in Brazil and adolescents’ routine immunization with the human papillomavirus vaccine in the United States of America.Citation18,Citation19
The lack of knowledge on the possible effects of timely vaccination and the adoption of immunization tools hinders interventions aiming to recover vaccination uptake and may further increase the risk of VPDs, especially during this period when most restrictions have been eased. In this study, the impact of the pandemic on immunization efforts in Canada was studied. Changes in children’s enrollment on the pan-Canadian digital vaccination platform and self-reported pediatric pneumococcal immunization series completion rates were assessed to describe how the pandemic’s related restrictions affected previously observed trends. The availability of this knowledge provides insights into how the pandemic has affected immunization and will guide interventions that aim to control and prevent VPDs during the current stage of the pandemic, as all provinces are alleviating COVID-19 restrictions. We hypothesized that the onset of COVID-19-related restrictions in Canada would impact both outcomes in a step-change format, an assumption based on the interim reports from the World Health Organization (WHO) on the impact of the pandemic on universal immunization coverage.Citation13
Methods
Study design and settings
We conducted a quasi-experimental study to assess the impact of the COVID-19 pandemic restrictions on infant vaccination rates in Canada. COVID-19’s related restrictions, the interrupting variable, were considered a natural event affecting everyone in Canada, while vaccination rates in terms of enrollment of children on the CANImmunize platform and self-reported on-time pneumococcal immunization series completion rates were considered the population-level outcomes. We conducted a single cohort interrupted time series analysis to examine these questions.
Source of data
All data was collected from the CANImmunize database. CANImmunize is a pan-Canadian digital vaccination tool established in 2016 to support Canadians in managing their own immunization information.Citation20 Data extraction happened in February 2022 and the extracted dataset contained information about children’s date of birth, the date every child’s record was created, the number of pneumococcal doses recorded in every record, and the date each dose was reported by CANImmunize users (parents and guardians) using their unique accounts.
Immunization data in CANImmunize is self-reported. CANImmunize uses children’s information, such as age, sex, and jurisdiction, to create a custom immunization schedule for every record.Citation20 Most children’s records were created after the child was born and already started their immunization journey, which means that reporting immunization in CANImmunize was done retrospectively. Because of that, the date of vaccination for many children became older than when their record was created on CANImmunize.
This study included only CANImmunize records of children that contained at least one dose of any pediatric vaccine; however, records with incorrect entries of children’s date of birth were excluded from both enrollment and series completion analysis. For the analysis of enrollments, the plan was to include records created from 2016 to 2021; however, the earliest children’s records were created in September 2017. So, we included all records created from 2017 to 2021 that fulfilled all inclusion criteria.
On the other side, for a successful analysis of series completion before 13 months, every included child must have turned 13 months by the date this data was pulled. Consequently, only children born from January 2016 to December 2020 were included in the analysis.
The data management has been described in .
Figure 1. The data management flow.
Statistical analysis
Two outcomes were assessed; Enrollment of children on the CANImmunize platform, which was evaluated as the number of records created on CANImmunize from 2017 to 2021; and the on-time completion rate of self-reported immunization series for pneumococcal vaccine. The number of new records was counted monthly using the record’s unique identifiers on CANImmunize. On-time completion of the immunization series for the pneumococcal vaccine was defined as the reception of three doses of pneumococcal vaccine before the child turns 13 months of age.Citation21 It was calculated using the child’s date of birth, the date the child turned 13 months, and the number of doses of pneumococcal vaccines every child received in that period.
The count of children that were born every month during the observation period served as the denominator, while the count of children born in the same month and received all doses of pneumococcal vaccine before they turned 13 months served as the numerator to provide the monthly completion rate in percentage.
A total of 52 (from September 2017 to December 2021) and 60 (from January 2016 to December 2020) monthly time series were generated for enrollment and immunization series completion rates, respectively. The nadir of enrollment and completion rates during the Covid19 pandemic was 100 records and 6.94% completed series, all in December 2021, respectively.
The point estimate and the confidence interval for the impact of the pandemic on both outcomes were assessed using Autoregressive Integrated Moving Average (ARIMA) models.Citation22
Model identification
After examining the trend and patterns of both outcomes’ time series (see ), the ARIMA model was used to account for autocorrelation and seasonality bias. The Dickey-Fuller test was used to confirm the series’ stationarityCitation22 prior to fitting an ARIMA model. We used an automated algorithm, specifically auto.arima() in the forecast package for R, to identify the ARIMA model terms based on minimizing the information criteria (AIC, BIC).Citation22 The statistical R version 4.1.3 was used for all analyses, and both the P_value and the confidence interval were reported. The P_value less than 0.05 was considered statistically significant.
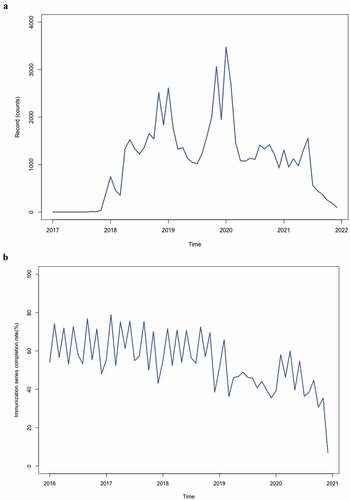
Figure 2. (a) shows the time series of monthly enrollment of children on CANImmunize from January 2016 to December 2021. (b) displays the time series of on-time completion rates of immunization series for the Pneumococcal vaccines from 2016 to 2020.
Ethical considerations
Data collection and handling were conducted according to the CANImmunize privacy policy.Citation23 Additionally, ethical approval to conduct this research has been obtained from the Ottawa Health Sciences Research Ethics Board (OHSN REB) prior to the start of all research activities.
Results
Overview of our data
A total of 63,833 pediatric records created in CANImmunize from 2017 to 2021 have met the study’s inclusion criteria. The highest enrollment of children occurred in January 2019, with 3374 records, as shows. The trend for enrollment displayed seasonality features, including a spike in the number of enrolled children toward the end of each year. However, there was a decrease in counts of enrolling children observed after the onset of COVID-19 restrictions, and the tall spikes observed in the pre-restriction period have not been repeated. Additionally, the post-restriction trend did not recover to reach the pre-restriction level; instead, it decreased further until the end of 2021.
The trend for pneumococcal immunization series completion rates has been decreasing since the end of 2018, and the recovery that happened in the early months of 2020 was not sustained.
ARIMA model
Enrollment series
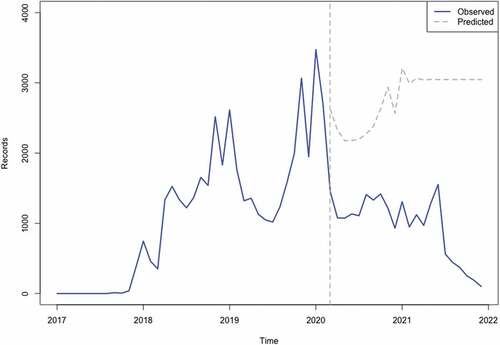
The model with the lowest information criteria selected by the algorithm was (1,1, 0) × (0, 0, 1) [12]. The estimated step change was −1177.52 records (95% CI: −1865.47, −489.57), while the estimated change in slope was −80.84 records per month (95% CI −227.03, 65.34). (See ) shows the values predicted by our ARIMA model in the absence of the intervention (counterfactual) compared with the observed values. This means that restrictions that were imposed to curb the impact of COVID-19 in March 2020 were associated with an abrupt and continued decline in enrollment by 1177.52, with a further decrease of 80.84 records each month during the study period. The p-value for the Ljung-Box test for white noise is 0.73 at 24 lags.
Figure 3. Shows both the observed and forecasted children’s enrollment on CANImmunize from 2016 to 2021 (The red-dash line represents the cut-off, the onset of COVID-19 related restrictions in Canada)Citation24.
Pneumococcal series completion rates
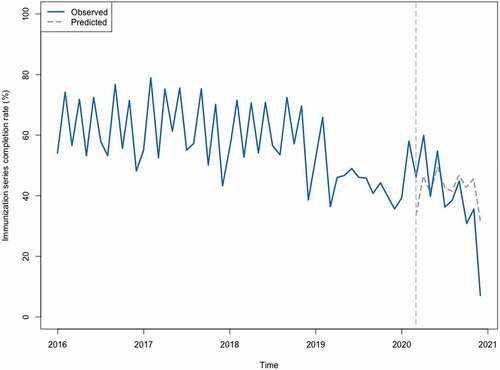
The model with the lowest information criteria selected by the algorithm was (3,0,0)(1,1,0) [12]. The estimated step change was 14.57% (95% CI 4.64, 24.51), while the estimated change in slope was −3.54% per month (95% CI −5.31, −1.76).
shows the values predicted by our ARIMA model in the absence of the intervention (counterfactual) compared with the observed values. This means that restrictions that followed the onset of COVID-19 restrictions in March 2020 were associated with an increase in self-reported completion of scheduled pneumococcal immunization series by 14.57%, followed by a decrease of 3.54% each month during the study period. The p-value for the Ljung-Box test for white noise is 0.98 at 24 lags.
Figure 4. Shows the predicted completion rates compared to observed rates from 2016 to 2020. The red-dash line represents the cut-off, the onset of COVID-19-related restrictions in CanadaCitation24.
Discussion
This study found that the onset of COVID-19 in Canada was associated with changes in immunization rates among users of the CANImmunize platform. The monthly enrollment of children on the platform has dropped by −1177.52 records (95% CI: −1865.47, −489.57), with a continued drop of 80.84 records each month. Pneumococcal immunization series completion had an initial increase of 14.57% (95% CI 4.64, 24.51); however, a sustained decrease of −3.54% each month that was spent in the pandemic has produced an estimated net effect of −20.83%.
These findings are consistent with results from early studies emerging on the impact of the COVID-19 pandemic on routine childhood vaccines globally. In North America, studies in the United States of America and the Dominican Republic have reported a decline of 5–18% and 10% in vaccination coverage, respectively.Citation25–29 In South America, studies in Columbia and Brazil have reported a drop in vaccination coverage of 14.4–20% and 10 to 20%, respectively.Citation30 European countries, in general, saw a 1% decrease in vaccination coverage, while the African region saw a 2–18% decrease.Citation31,Citation32 Middle eastern countries such as Jordan have reported a decrease in vaccination coverage of 11.1%,Citation33 while Lebanon reported a national level decrease of 31% in the utilization of immunization services during the pandemic.Citation34
The pandemic-related drop in the uptake of routine vaccines could not be generalized worldwide. For instance, the Brazilian immunization programs appeared to have challenges that were not necessarily furthered by the pandemic, as Alves J. G et al showed in their study. They didn’t find a significant impact of the pandemic on the already declining completion rates of routine pediatric immunization in Brazil;Citation18 therefore, catch-up programs targeting children that missed their scheduled doses due to the pandemic’s restrictions would not significantly improve the completion rate of the pediatric immunization programs. On the other side, unlike our findings on the adoption of CANImmunize during the pandemic, the initiation and uptake of the HPV immunization series among adolescents in the United States have not been affected by the Covid-19 pandemic,Citation19 highlighting the role of having schools open on the Canadian immunization program in relation to the USA’s.
Our findings did spot a slight increase in the completion rates during the first 3 months of 2020, including March, the first month of the pandemic. However, this was not a positive result of the pandemic. Rather, it was a seasonality feature of the data that is observed around the start of every year. It is influenced by the annual commencement of schools and daycares during that period. It is believed that a significant number of parents update their immunization records to fulfill school enrollment requirements in provinces such as Ontario.Citation35 Unfortunately, the same observation would not be possible in 2021, as many schools were closed as a measure to mitigate the Covid-19 pandemic’s effects.Citation36
To our knowledge, no studies assessed the impact of the pandemic-related restrictions on population engagement in digital tools for vaccination, such as CANImmunize, and the impact of the pandemic on pneumococcal vaccination in Canada. A key strength of our study is that we used a large dataset observed over a long period. It has allowed us to compare and understand changes in the trend of each outcome. Additionally, this research was the first to detect the effect of the COVID-19 pandemic on children’s immunization in Canada. It will serve as hypothesis-generating while other nationwide evaluations are conducted.
The findings of this study depict the extent to which the COVID-19 pandemic has affected the adoption of digital immunization platforms, as well as the completion of pediatric immunization series among adopters of such platforms. Digital platform use increased considerably during the pandemicCitation37,Citation38 and data from digital platforms can serve as an early indicator of trends in vaccination. Our observations in the CANImmunize database are consistent with data emerging from other sources. Together they speak to an emerging challenge that requires immediate attention from a public health perspective. The study also points to an opportunity to use digital platforms to inform public health decision-making.
This study had some limitations. Outcomes were assessed in a population that is actively utilizing a free digital tool for managing immunization records, which may not be representative of the general population. This study was also a single-group interrupted time series analysis, lacking a parallel comparison group. Furthermore, all data on vaccination was self-reported. However, vaccinations reported by parents are used by some provinces as the official source of data. Parents are required to register such information to public health for school entry under the Immunization of School Pupils Act in Ontario.Citation35
Additionally, disparities in the effect of the pandemic on immunization rates due to factors such as geographical location and socioeconomic status of the CANImmunize users have not been assessed. The company’s privacy policy limits access to the socioeconomic data of users and prohibits the collection of a complete user postal code. The combination of those roll blocks made it impossible for the analysis to utilize other datasets that could provide socioeconomic data, such as the Canada Revenue Agency’s publicly available data on household income tax per postal code. Additionally, geographical disparities were not assessed due to the difficulties in increasing the power of the analysis. As a result, the scope of the analysis was limited to the national level impact, given that all provinces and territories of Canada share similar federal immunization goals and strategies.Citation8 However, we agree that further research is recommended to test and elucidate the possibility of disparities in the effect of the pandemic on children’s immunization rates among all provinces and territories of Canada.
Conclusion
The COVID-19 pandemic has negatively affected enrollment in the CANImmunize app immediately and the whole time under pandemic restrictions. Pneumococcal immunization series completion rates had an initial increase but an overall estimated net effect of −20.83%. Further research is needed to assess the impact of the COVID-19 pandemic on pediatric vaccination rates in Canada. There is a strong need for the development and implementation of catch-up intervention programs to mitigate the effects of the pandemic on the 2025 Public Health Agency of Canada’s goals of achieving community protection against VPDs.
Supplemental Material
Download PDF (757.5 KB)Acknowledgment
We thank the team of supervisors from Karolinska Institutet for their guidance during the research proposal writing and data analysis.
Disclosure statement
BN is an employee of CANImmunize. KW and KA are co-founders of CANImmunize. KW is on the safety advisory boards for Medicago and Moderna.
Supplementary material
Supplemental data for this article can be accessed on the publisher’s website at https://doi.org/10.1080/21645515.2022.2158005
Additional information
Funding
References
- Greenwood B. The contribution of vaccination to global health: past, present and future. Philos Trans R Soc B Biol Sci [Internet]. 2014 Jun 19 [accessed 2021 Feb 21];369(1645):20130433. doi:10.1098/rstb.2013.0433.
- Ozawa S, Clark S, Portnoy A, Grewal S, Stack ML, Sinha A, Mirelman A, Franklin H, Friberg IK, Tam Y, et al. Estimated economic impact of vaccinations in 73 low- and middle-income countries, 2001–2020. Bull World Health Organ. 2017 Sep 1;95(9):629–8. doi:10.2471/BLT.16.178475.
- Lee LA, Franzel L, Atwell J, Datta SD, Friberg IK, Goldie SJ, Reef SE, Schwalbe N, Simons E, Strebel PM, et al. The estimated mortality impact of vaccinations forecast to be administered during 2011–2020 in 73 countries supported by the GAVI Alliance. Vaccine. 2013 Apr 18;31(SUPPL2):B61–72. doi:10.1016/j.vaccine.2012.11.035.
- The elements of a strong immunization programme - and why we need to invest in them. 2015;5.
- Saboui M, Hiebert J, Squires SG, Guay M, Barcellos P, Thom A, Li YA. Re-verifying the elimination of measles, rubella and congenital rubella syndrome in Canada, 2016–2020. Can Commun Dis Rep. 2021 Nov 10;47(11):476–78. doi:10.14745/ccdr.v47i11a06.
- Halperin SA, Pianosi K. Immunization in Canada: a 6-year update. J Can Chiropr Assoc. 2010 Jun;54(2):85–91.
- Canada PHA of. Vaccine preventable disease: surveillance report to December 31, 2017 [Internet]. aem. 2020 [accessed 2021 Jan 21]. https://www.canada.ca/en/public-health/services/publications/vaccines-immunization/vaccine-preventable-disease-surveillance-report-december-31-2017.html#introduction.
- Canada PHA of. Vaccination coverage goals and vaccine preventable disease reduction targets by 2025 [Internet]. aem. 2017 [accessed 2021 Feb 22]. https://www.canada.ca/en/public-health/services/immunization-vaccine-priorities/national-immunization-strategy/vaccination-coverage-goals-vaccine-preventable-diseases-reduction-targets-2025.html.
- Dubé E, Bettinger J, Fisher W, Naus M, Mahmud S, Hilderman T. Vaccine acceptance, hesitancy and refusal in Canada: challenges and potential approaches. Can Commun Dis Rep. 2016 Dec 1;42(12):246–51. doi:10.14745/ccdr.v42i12a02.
- WHO Coronavirus (COVID-19) dashboard [Internet]. [ accessed 2022 Oct 12]. https://covid19.who.int.
- Chu J. A statistical analysis of the novel coronavirus (COVID-19) in Italy and Spain. PLoS One. 2021 Mar 25;16(3):e0249037. doi:10.1371/journal.pone.0249037.
- Public health and social measures [Internet]. [accessed 2022 Oct 12]. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/phsm.
- Organization WH. Guiding principles for immunization activities during the COVID-19 pandemic: interim guidance, 26 March 2020. 2020 [accessed 2021 Jan 22]. https://apps.who.int/iris/handle/10665/331590.
- Santoli JM, Lindley MC, DeSilva MB, Kharbanda EO, Daley MF, Galloway L, Gee J, Glover M, Herring B, Kang Y, et al. Effects of the COVID-19 pandemic on routine pediatric vaccine ordering and administration — United States, 2020. MMWR Morb Mortal Wkly Rep [Internet]. 2020 [accessed 2021 Feb 2];69(19):591–93. doi:10.15585/mmwr.mm6919e2.
- COVID-19 pandemic leads to major backsliding on childhood vaccinations, new WHO, UNICEF data shows [Internet]. [accessed 2022 Mar 28]. https://www.who.int/news/item/15-07-2021-covid-19-pandemic-leads-to-major-backsliding-on-childhood-vaccinations-new-who-unicef-data-shows.
- Causey K, Fullman N, Sorensen RJD, Galles NC, Zheng P, Aravkin A, Danovaro-Holliday MC, Martinez-Piedra R, Sodha SV., et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: a modelling study. Lancet. 2021 Aug 7;398(10299):522–34. doi:10.1016/S0140-6736(21)01337-4.
- Piché-Renaud PP, Ji C, Farrar DS, Friedman JN, Science M, Kitai I, Burey S, Feldman M, Morris SK. Impact of the COVID-19 pandemic on the provision of routine childhood immunizations in Ontario, Canada. Vaccine. 2021 Jul 13;39(31):4373–82. doi:10.1016/j.vaccine.2021.05.094.
- Alves JG, Figueiroa JN, Urquia ML. Impact of COVID-19 on immunization of Brazilian infants. Int J Infect Dis IJID off Publ Int Soc Infect Dis. 2021 Jun;107:252–53. doi:10.1016/j.ijid.2021.04.089.
- Pingali C, Yankey D, Elam-Evans LD, Markowitz LE, Williams CL, Fredua B, McNamara LA, Stokley S, Singleton JA. National, regional, state, and selected local area vaccination coverage among adolescents aged 13–17 years — United States, 2020. Morb Mortal Wkly Rep. 2021 Sep 3;70(35):1183–90. doi:10.15585/mmwr.mm7035a1.
- World Health Organization. CANImmunize [Internet]. CANImmunize. 2020 [accessed 2021 Nov 3]. https://www.who.int/teams/regulation-prequalification/regulation-and-safety/pharmacovigilance/vaccine-safety-net/vsn-members/canimmunize.
- Childhood-vaccination-schedule-2021-eng (1).Pdf [Internet]. Google Docs. [accessed 2022 Apr 8]. https://drive.google.com/file/d/1j5pbTICu-DMuDAPiZK3vfsCIkhRnPtUC/view?usp=sharing&usp=embed_facebook.
- Schaffer AL, Dobbins TA, Pearson SA. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: a guide for evaluating large-scale health interventions. BMC Med Res Methodol. 2021 Mar 22;21(1):58. doi:10.1186/s12874-021-01235-8.
- CANImmunize privacy policy [Internet]. [accessed 2021 Jan 22]. https://www.canimmunize.ca/en/privacy-policy?canimm-inappbrowser=1.
- A timeline of events in Canada’s fight against COVID-19 [Internet]. CP24. 2020 [ accessed 2021 May 3]. https://www.cp24.com/news/a-timeline-of-events-in-canada-s-fight-against-covid-19-1.5231865?cache=%3FclipId%3D89750%3FclipId%3D89578%3FclipId%3D104062%3FclipId%3D89563.
- DeSilva MB, Haapala J, Vazquez-Benitez G, Daley MF, Nordin JD, Klein NP, Henninger ML, Williams JTB, Hambidge SJ, Jackson ML, et al. Association of the COVID-19 pandemic with routine childhood vaccination rates and proportion up to date with vaccinations across 8 US health systems in the vaccine safety datalink. JAMA Pediatr. 2022 Jan 1;176(1):68–77. doi:10.1001/jamapediatrics.2021.4251.
- Colomé-Hidalgo M, Campos JD, de Miguel Á G. Tracking the impact of the COVID-19 pandemic on routine infant vaccinations in the Dominican Republic. Hum Vaccines Immunother. 2022;18(1):1972708. doi:10.1080/21645515.2021.1972708.
- SeyedAlinaghi S, Karimi A, Mojdeganlou H, Alilou S, Mirghaderi SP, Noori T, Shamsabadi A, Dadras O, Vahedi F, Mohammadi P, et al. Impact of COVID -19 pandemic on routine vaccination coverage of children and adolescents: a systematic review. Health Sci Rep. 2022 Feb 18;5(2):e00516. doi:10.1002/hsr2.516.
- O’Leary ST, Trefren L, Roth H, Moss A, Severson R, Kempe A. Number of childhood and adolescent vaccinations administered before and after the COVID-19 outbreak in Colorado. JAMA Pediatr. 2021 Mar 1;175(3):305–07. doi:10.1001/jamapediatrics.2020.4733.
- Bramer CA. Decline in Child Vaccination Coverage During the COVID-19 Pandemic — Michigan Care Improvement Registry, May 2016–may 2020. MMWR Morb Mortal Wkly Rep [Internet]. 2020 [accessed 2021 May 3];69(20):630–31. doi:10.15585/mmwr.mm6920e1.
- Moreno-Montoya J, Ballesteros SM, Rojas Sotelo JC, Bocanegra Cervera CL, Barrera-López P, De la Hoz-Valle JA. Impact of the COVID-19 pandemic on routine childhood immunisation in Colombia. Arch Dis Child. 2022 Mar;107(3):e4. doi:10.1136/archdischild-2021-321792.
- COVID-19 widens routine immunization gaps in Africa [Internet]. WHO | Regional Office for Africa. [accessed 2022 Oct 12]. https://www.afro.who.int/news/covid-19-widens-routine-immunization-gaps-africa.
- Varied impact of COVID-19 on routine immunization in the European Region [Internet]. [accessed 2022 Oct 12]. https://www.who.int/europe/news/item/16-07-2021-varied-impact-of-covid-19-on-routine-immunization-in-the-european-region.
- Abu-Rish EY, Bustanji Y, Abusal K. Nationwide routine childhood vaccination coverage during the COVID-19 pandemic in Jordan: current situation, reasons, and predictors of vaccination. Int J Clin Pract. 2022 Mar 24;2022:e7918604. doi:10.1155/2022/7918604.
- Mansour Z, Arab J, Said R, Rady A, Hamadeh R, Gerbaka B, Bizri AR. Impact of COVID-19 pandemic on the utilization of routine immunization services in Lebanon. PLoS One. 2021 Feb 17;16(2):e0246951. doi:10.1371/journal.pone.0246951.
- Immunization of School Pupils Act (ISPA) [Internet]. Canadian Partnership Against Cancer. 1990 [accessed 2021 May 9]. https://www.partnershipagainstcancer.ca/preventionpoliciesdirectory/ppd2024/.
- El Jaouhari M, Edjoc R, Waddell L, Houston P, Atchessi N, Striha M, Bonti-Ankomah S. Impact of school closures and re-openings on COVID-19 transmission. Can Commun Dis Rep. 2021 Dec 9;47(12):515–23. doi:10.14745/ccdr.v47i12a02.
- Gostin LO, Cohen IG, Shaw J. Digital health passes in the age of COVID-19: are “vaccine passports” Lawful and Ethical?. JAMA. 2021 May 18;325(19):1933–34. doi:10.1001/jama.2021.5283.
- Golinelli D, Boetto E, Carullo G, Nuzzolese AG, Landini MP, Fantini MP. Adoption of digital technologies in health care during the COVID-19 pandemic: systematic review of early scientific literature. J Med Internet Res. 2020 Nov 6;22(11):e22280. doi:10.2196/22280.