
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Tetanus is still a major problem in sub-Saharan African countries. This study aims to evaluate tetanus disease and vaccine awareness among healthcare workers in Mogadishu. This descriptive, cross-sectional study was scheduled for January 2–7, 2022. A questionnaire consisting of 28 questions was applied in a face-to-face manner to 418 healthcare workers. Only health workers aged≥18 living in Mogadishu were included. Questions about sociodemographic characteristics, tetanus disease, and vaccines were developed. 71.1% of the participants were female, 72% were ˂25 years old, 42.6% were nursing students, and 63.2% had a university education. It was observed that 46.9% of the volunteers had an income level of <$250, and 60.8% resided in the city center. 50.5% of the participants received a tetanus vaccine in their childhood. Questions to determine participants’ level of knowledge about tetanus and the tetanus vaccine were responded to with an accuracy of between 44 and 77%. Although 38.5% of the participants reported that they were exposed to trauma at least once a day, the rate of those who had three or more doses of the vaccine was only 10.8%. On the other hand, 51.4% reported that they had received training about tetanus and vaccination. There was a significant difference (p < .001) in terms of knowledge level among sociodemographic characteristics. The fear of side effects was the most important reason for not being vaccinated. Healthcare workers in Mogadishu have little awareness of tetanus disease and vaccines. Efforts to improve education and other factors will be sufficient to eliminate the disadvantage brought about by the socio-demographic structure.
Introduction
A protein neurotoxin generated by the bacterium Clostridium tetani causes the severe but preventable disease known as tetanus.Citation1 Especially unvaccinated young adults, advanced age groups, and those on immunosuppressives are risk groups for tetanus.Citation2 The tetanus mortality rate is high in sub-Saharan African countries: reports have shown a mortality rate of 64% in Nigeria, 47% in Uganda, 43.1% in Tanzania, and 48.5% in Cameroon.Citation3 More than 1,000 newborn tetanus fatalities per 100,000 people were recorded in Somalia, South Sudan, Afghanistan, and Kenya, the countries with the highest prevalence of the disease. The countries with the greatest rates of post-neonatal tetanus mortality (greater than five fatalities per 100,000 people) were Somalia, South Sudan, and Kenya.Citation4 There are no data on the tetanus vaccination status in Somalian healthcare workers (HCWs). However, a study was conducted on the tetanus vaccine status in the African community covering 12 countries. It was determined that none of the women of reproductive age in these countries were protected by two or more doses of the tetanus vaccine. As of December 2020, the expected target has not been achieved in Afghanistan, Angola, Central African Republic, Guinea, Mali, Nigeria, Pakistan, Papua New Guinea, Somalia, South Sudan, Sudan, or Yemen.Citation5 The final decisions of the World Health Assembly recommended that at least 80% of pregnant women should be vaccinated with at least two doses of tetanus toxoid-containing vaccines and that at least 80% of women of reproductive age in high-risk areas should be vaccinated with at least three rounds of tetanus toxoid-containing vaccine. In Somalia, this rate remained at 58% as of 2019.Citation6 Income level directly affects the vaccination rate. Eight of the 12 countries investigated in 2019 were low-income countries, and the remaining four were lower-middle-income countries.Citation7 Maternal education, living in the city center, and being born to wealthy families increase the likelihood of children being protected against tetanus at birth.Citation8,Citation9 Considering that healthcare professionals are role models in vaccination, their views of vaccination and vaccination rates are very important.Citation10–12 This study aims to evaluate tetanus disease and tetanus vaccine awareness in healthcare workers (HCWs) living in Mogadishu, Somalia.
Materials and methods
Study design and data collection
This descriptive cross-sectional study was planned to be conducted with the students of the Faculty of Health Sciences at Recep Tayyip Erdogan Training and Research Hospital. Somalian HCWs and students receiving health education at the faculty were included in the study. The study was planned to be conducted between 2 and 7 January 2022. A questionnaire consisting of 28 questions was created. The questionnaire was applied to the participants in a face-to-face manner. Participation in the study was voluntary. The participants consisted of specialist doctors, assistant doctors, internship doctors, nurses, nursing students, and paramedics. Those who were <18 years old, Turkish HCWs, and those that were not HCWs were excluded from the study. In addition, participants who did not respond to all the items in the questionnaire form were excluded. The minimum number of participants was determined using the Raosoft calculator.Citation13 The calculation was made as follows:
where n: sample size, E: margin of error, N: population size, r: fraction of answers, and Z (c/100) c: critical value for confidence level.
A total of 950 healthcare workers work in our hospital. Moreover, 570 students are actively studying in the Faculty of Health Sciences. Thus, there are a total of 1,520 HCWs. So far, no similar study has been conducted in Somalia. 5% margin of error and 95% confidence interval were accepted. It was determined that there should be at least 307 participants using a 50% precautionary forecast rate. A number above the minimum number was reached by including 418 participants in the study. The data were collected at randomly distributed locations.
Ethical consideration
An application was made to the Ethics Committee of Somalia Mogadishu Turkey Recep Tayyip Erdogan Training and Research Hospital (Approval no: MSTH/12753). During the application of the survey, personal information such as name, surname, or identification number was not requested from the participants.
Questionnaire design and evaluation
The questionnaire was developed and validated with support from three similar studies.Citation14–16 The questionnaire was composed of three parts. The first part had seven questions about sociodemographic characteristics (age, gender, profession, education, income, experience, and region). The second part contained 12 multiple-choice questions about tetanus disease and tetanus vaccine (yes, no, and I don’t know). Finally, the last part included nine multiple-choice questions about the vaccination history of the HCWs, their approach to the vaccine, and the difficulties experienced in reaching the vaccine. The questionnaire items were prepared in English, as the majority of Somalian HCWs speak advanced English. Nevertheless, a Somalian health worker, one of the researchers, explained the whole questionnaire to the participants in the Somali language. Thus, there was no language problem. The survey data was first entered into the Excel Program. Then, the answers to the questions were listed as 1, 2, 3, etc. A number was added to each survey. The sum of knowledge scores was calculated in a separate column. Then, 70% of the total score was accepted as the limit, and the participants were divided into two groups: “those with good knowledge” and “those with poor knowledge.” Then, the data were entered into the SPSS program. The frequency data of all answers were determined in the analysis. In addition, the responses in the second part were scored to evaluate participants’ levels of knowledge about tetanus and the tetanus vaccine. In this part consisting of 12 questions, 1 point was given to the correct answer and 0 points to the wrong answer or the answer “I don’t know.” Thus, participants’ knowledge levels were evaluated based on a total of 12 points. Those who scored 8.4 and above (≥70%) were included in the “those with good knowledge” group, while those who scored lower were included in the “those with poor knowledge” group.Citation13
Statistical analysis
All data were entered into IBM SPSS Statistics 26.0 (IBM Corporation). Frequencies and percentages were calculated for categorical variables, and means (standard deviation) and medians (interquartile range; IQR) were calculated for continuous variables. While the normal distribution of the data was evaluated using Kolmogorov-Smirnov and histogram tests, homogeneity evaluation was done with Levene’s test. Since the number of participants was>50, the Kolmogorov-Smirnov test was used instead of the Shapiro-Wilk test. The chi-square test, Fisher’s exact test, and Bonferroni test were used to compare categorical data. In addition, the level of significance of the subgroups over the total knowledge score was determined by the Kruskall Wallis test and the Mann-Whitney U test. A p-value of<.05 was considered statistically significant.
Results
Demographic data
A total of 418 Somalian HCWs were included in the study. The sociodemographic characteristics of the participants are given in as frequencies and percentages. The majority of the participants were female (71.1%). It was observed that 72% of the participants were ˂25 years old. Nursing students (42.6%) constituted the largest group among the professional groups. When participants’ educational background was examined, it was determined that the majority of the participants (63.2%) received a university education. The income level of 46.9% of the volunteers was <$250. It was seen that 57.7% of the participants had no field experience. When their region of residence was examined, it was seen that 60.8% of them resided in the city center.
Table 1. Sociodemographic parameters, numbers, percentages.
Participants’ level of knowledge about tetanus disease and vaccine
The second part of the questionnaire included 12 multi-choice questions to determine participants’ level of knowledge about tetanus disease and vaccination. The frequency and percentages of the responses are given in . The rate of correct answers was 75.8% for the first question, 69.1% for the second question, 76.1% for the third question, 77.3% for the fourth question, 61% for the fifth question, 44.7% for the seventh question, 49.8% for the eighth question, 49% for the ninth question, 46.7% for the tenth question, 50% for the eleventh question, and 45.7% for the twelfth question. On the other hand, 50.5% reported that they had been vaccinated in their childhood.
Table 2. Knowledge of tetanus and vaccine.
Tetanus vaccine status of healthcare workers
The last part of the questionnaire aimed to determine the vaccination background of the participants, the reason for the problems in the supply of the vaccine, and their general attitudes toward the vaccine. A total of nine multiple-choice questions were included. The frequency and percentages of the responses are given in . Due to the civil war in Somalia, exposure to trauma is high because of frequent explosions and injuries. Although 38.5% of the participants reported that they were exposed to trauma at least once a day, it was seen that 31.6% of them did not receive the tetanus vaccine in childhood and 15.8% of them did not know whether or not they received it. It was determined that 39% received the booster dose. In general, the rate of those who had three or more doses of the vaccine was only 10.8%. On the other hand, 23.2% of the participants stated that they could access the vaccine for a fee. Although the tetanus vaccine was administered free of charge to all HCWs in the vaccination nursing unit of our hospital, it was understood that 20.8% of the participants were not aware of it. It was understood that 20.8% of the unvaccinated or insufficiently vaccinated participants did not have it because they were afraid of the side effects of the vaccine. 38.5% of the participants reported that it was compulsory to be vaccinated in the institution where they work or where they receive an education. About half (51.4%) reported that they had received training on the tetanus vaccine.
Table 3. Tetanus vaccine status of healthcare workers.
Evaluation of knowledge levels with the chi-square (χ2) test
Twelve questions were prepared to evaluate participants’ knowledge levels about the tetanus disease and vaccine. Each correct answer was worth 1 point (0–12 points). Participants with ≥8.4 points (≥70%) were categorized as “having good knowledge,” while those with <8.4 points (<70%) were categorized as “having poor knowledge.” When sociodemographic variables and knowledge levels were compared in the chi-square test, it was determined that there was a significant difference between all parameters in terms of knowledge levels (p < .001). In addition, the Kruskall Wallis test and Mann-Whitney U test were applied to evaluate the level of significance among subgroups over the total knowledge score. In the 25–35 age group, the knowledge score was statistically significantly higher than in the other age groups (p < .001). Similar significance was found in men compared to women, in doctors compared to other occupational groups, and in nurses compared to nursing students and paramedics (p < .001). Knowledge scores were statistically significantly higher in laborants than in paramedics, in those with Bachelor’s degrees and Master’s degrees than in university students, in those with an income of >$500 than in those with less income, in groups with professional work experience than in groups with no work experience, and in those living in the city center than in those living in rural areas (p < .001) ().
Table 4. Comparison of sociodemographic characteristics and level of knowledge about tetanus and vaccine (χ2).
Evaluation of none-vaccination by the chi-square (χ2) test according to sociodemographic characteristics
Participants who were not vaccinated or who had a missing dose were asked a question about the missing dose or the reasons for not being vaccinated. Their responses were analyzed with the chi-square (χ2) test and Bonferroni test according to sociodemographic characteristics (). When the answers were evaluated, the fear of side effects emerged as the most important reason. Difficulties in accessing the vaccine and lack of time were other important reasons. There was a significant difference in terms of the reasons for the lack of vaccination among gender (p < .008), age (p < .001), profession (p < .001), education (p < .001), experience (p < .001), income (p < .001), and region (p < .002) subgroups.
Table 5. Evaluation of none-vaccination according to sociodemographic characteristics (χ2).
Discussion
Although the risk of exposure to trauma is very high in Mogadishu, where civil war and explosions are experienced intensely, there is no study exploring the tetanus vaccine status in HCWs. In our study, a serious insufficiency was found in full-dose vaccination. The main reasons for this in Somalia are the fear of side effects, cultural and religious factors such as social opposition to vaccination, and financial inadequacy. Most of the participants are not aware of the fact that free vaccines can be obtained from our institution. Living in rural areas is another important disadvantage. According to World Health Organization data, 26–70% of the Somali population is poor. 2.6 million people have been displaced by terrorism. Vaccine insufficiency is inevitable in these people, who have difficulties in accessing even basic health services.Citation17
A meta-analysis searched PubMed/MEDLINE online, ScienceDirect, Hinari, Hinari, Google and Google Scholar databases and reviewed 199 published studies on tetanus toxoid vaccine in Ethiopia, Somalia’s neighbor. 14 studies were included. The rate of those who received at least two doses of the tetanus vaccine was found to be 52.2% (95% CI: 42.47–61.93). Antenatal treatment (OR = 7.8 (95% CI: 3.2, 19.2)), difficulty in accessing healthcare facilities (OR = 2.64 (95% CI: 1.1, 6.6)), women’s educational background (OR = 4.7 (95% CI: 2.07, 9.56)), and their husbands’ educational background (OR = 2.995 (95% CI: 1.194, 7.512)) were significantly associated with getting at least two doses of the tetanus vaccine.Citation18 Maternal tetanus and neonatal tetanus still occur in nine sub-Saharan African countries. There are many factors that affect access to vaccines. In a study conducted with women of childbearing age in rural areas in Nigeria, three groups of women were given financial aid to encourage vaccination. The probability of being vaccinated was found to be higher in the two groups with more financial aid than in the group with less money. Transportation costs were reported as one of the major barriers to accessing the vaccine.Citation19 In a review examining the efforts to develop vaccine strategies in sub-Saharan African countries, it was reported that factors such as low birth age, relatively good welfare level, employment of women, and frequency of prenatal follow-ups contributed positively to the efforts in Kenya. In Ethiopia, factors such as the large unvaccinated population, deficiencies in reporting, the fragility of the health system, and resource limitations were emphasized. In Nigeria, shortcomings in notifications, the lack of information on the vaccination schedule, deficiencies in the registration system, and the necessity of referral to a doctor for vaccination were reported as the disadvantages. The lack of community involvement was also found to be an important limiting factor. Emphasis was placed on raising awareness as a society to change or influence women’s attitudes and beliefs toward vaccination. It was also concluded that improving vaccine accessibility, affordability, availability, and accommodation would increase vaccination rates.Citation20 In another review that analyzed studies on vaccine distribution systems in Nigeria, Benin, and Mozambique, it was shown that outsourcing vaccine logistics to the private sector contributed to the improvement in vaccine distribution costs and backup in vaccine warehouses.Citation21
Even in developed countries, tetanus vaccine awareness among HCWs is lower than we expected. In a survey study with 197 HCWs in China, only 21.3% of physicians had a booster dose. In addition, only 28.9% reported that they had received training on vaccination. Only 14.2% of respondents confirmed that the tetanus vaccine was available at their institution. As a result, in this study conducted with emergency physicians, it was understood that patients were not vaccinated sufficiently because the physicians did not have enough knowledge. It was also determined that even physicians did not receive sufficient doses of vaccination.Citation14 In a survey study conducted with a volunteer group of 336 people consisting of doctors, nurses, and support staff in Turkey, the participants did not have enough information about the vaccination of women between the ages of 15 and 49 and the need for a booster tetanus vaccine every 10 years. In addition, it was understood that the nurses had a significant lack of knowledge about booster doses.Citation22 There are different data on the vaccination attitude, knowledge level, and vaccination rate of HCWs in survey studies conducted with HCWs in different countries.Citation23–26
In our study, it was determined that sociodemographic characteristics affected knowledge levels (p < .001). Tetanus and vaccine knowledge scores were higher in the middle-aged group, males, those living in the city center, and those with more work experience. These results indicate the effect of vocational education quality and the undeniable impact of financial means. When our study and similar studies are evaluated, the main factors related to inadequate vaccination in African countries are shown in under nine titles.
Figure 1. Factors affecting vaccination in Sub-Saharan Africa.
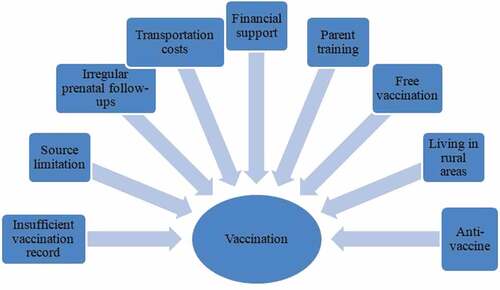
The development of plans for the solution of these problems by the health units of the countries, especially Somalia, will contribute greatly to vaccination.
The study has some limitations. First, the survey questions were developed using similar publications instead of an internationally valid scale. Second, the sample consisted mostly of participants living in Mogadishu. Therefore, the results may fail to reflect the whole country. Third, the majority of the respondents are female. This is because most of the students at the Faculty of Health Sciences are female. Hence, the study sample may fail to represent the general population. Future studies could be done with more favorable ratios of male and female participants. Fourth, the inclusion of allied HCWs and students without work experience may have affected homogeneity. To reduce the risk of bias in responding, the questionnaire was administered without collecting participants’ personal information. In addition, necessary explanations regarding confidentiality were made to the participants.
Conclusion
HCWs should be role models for other society members about vaccination. Yet, it was determined that vaccination awareness and vaccination rates were quite low among the HCWs in Mogadishu. It was understood that the sociodemographic structure of the HCWs in Mogadishu significantly affected the awareness of the vaccine. It was also seen that there was a serious need for planning training programs on vaccines. Besides, the lack of knowledge about vaccine availability among many HCWs was noticed. Somalia has difficult living conditions due to its geography and lack of income sources. However, a high rate of tetanus vaccination is possible, especially in HCWs, with simple measures such as reevaluation of education programs and free availability of the vaccine. In our study, the main factors affecting vaccination were revealed. The development of plans for the solution of these problems by health and education institutions will significantly contribute to increasing the rate of vaccination. Since this survey study was only applied to HCWs, large-scale studies including other segments of society would provide more precise data.
Acknowledgments
We would like to thank the staff of the Faculty of Health Sciences and infection control committee nurses for their support in the application of the survey.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Megighian A, Pirazzini M, Fabris F, Rossetto O, Montecucco C. Tetanus and tetanus neurotoxin: from peripheral uptake to central nervous tissue targets. J Neurochem. 2021 Sep;158(6):1–8. doi:10.1111/jnc.15330.
- Chrdle A, BalejovÁ M. Tetanus stále aktuální [Tetanus Still Current]. Acta Chir Orthop Traumatol Cech. 2020;87(4):292–6. Czech.
- Sangwe Clovis N, Palle JN, Linwa EMM, Ndung Ako F, Tabe Benem-Orock V, Chichom Mefire A. Factors associated with mortality in patients with tetanus in Cameroon. Sci Prog. 2023 Jan-Mar;106(1):368504221148933. doi:10.1177/00368504221148933.
- Kyu HH, Mumford JE, Stanaway JD, Barber RM, Hancock JR, Vos T, Murray CJL, Naghavi M. Mortality from tetanus between 1990 and 2015: findings from the global burden of disease study 2015. BMC Public Health. 2017;17:179. doi:10.1186/s12889-017-4111-4.
- Yusuf N, Raza AA, Chang-Blanc D, Ahmed B, Hailegebriel T, Luce RR, Tanifum P, Masresha B, Faton M, Omer MD, et al. Progress and barriers towards maternal and neonatal tetanus elimination in the remaining 12 countries: a systematic review. Lancet Glob Health. 2021 Nov;9(11):e1610–17. doi:10.1016/S2214-109X(21)00338-7. Erratum in: Lancet Glob Health. 2022 Feb;10(2):e185.
- WHO. Protecting all against tetanus: guide to sustaining maternal and neonatal tetanus elimination (MNTE) and broadening tetanus protection for all populations. Geneva: World Health Organization; 2019.
- World Bank. World Bank Country and Lending Group—country classification.
- https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groupsTheDHS Program. Demographic and Health Surveys
- https://www.dhsprogram.com/Countries/UNICEF. Multiple indicator cluster surveys (MICS). https://mics.unicef.org/surveys.
- Lee HY, Oh J, Heo J, Abraha A, Perkins JM, Lee JK, Tran TGH, Subramanian SV. Association between maternal literacy and child vaccination in Ethiopia and southeastern India and the moderating role of health workers: a multilevel regression analysis of the young lives study. Glob Health Action. 2019;12(1):1581467. doi:10.1080/16549716.2019.1581467.
- Ahmed S, Chase LE, Wagnild J, Akhter N, Sturridge S, Clarke A, Chowdhary P, Mukami D, Kasim A, Hampshire K. Community health workers and health equity in low- and middle-income countries: systematic review and recommendations for policy and practice. Int J Equity Health. 2022 Apr 11;21(1):49. doi:10.1186/s12939-021-01615-y.
- Masquillier C, Cosaert T. Community health workers: a sustainable health system innovation or just an emergency response? Front Pub Heal. 2022 Dec 6;10:1040539. doi:10.3389/fpubh.2022.1040539.
- Sahin TK, Erul E, Aksun MS, Sonmezer MC, Unal S, Akova M. Knowledge and attitudes of Turkish physicians towards human monkeypox disease and related vaccination: a cross-sectional study. Vaccines. 2022;11:19. doi:10.3390/vaccines11010019.
- Liu Y, Mo X, Yu X, Wang J, Tian J, Kuang J, Peng J. Insufficient knowledge and inappropriate practices of emergency doctors towards tetanus prevention in trauma patients: a pilot survey. Hum Vaccines Immunother. 2020;16(2):349–57. doi:10.1080/21645515.2019.1653745. Epub 2019 Oct 18.
- Gebremedhin TS, Welay FT, Mengesha MB, Assefa NE, Werid WM. Tetanus toxoid vaccination uptake and associated factors among mothers who gave birth in the last 12 months in Errer District, Somali Regional State, Eastern Ethiopia. Biomed Res Int. 2020 May 7;2020:4023031. doi:10.1155/2020/4023031.
- Seyman D, Keskin AS, Küçükateş E, Ceylan MR, Kul G, Tosun S, Oğuzöncül AF, Gazel ÖZ, Uzar H, Uysal S, et al. Healthcare personnel’s attitude and coverage about tetanus vaccination in Turkey: a multicenter study. Hum Vaccines Immunother. 2022 Dec 31;18(1):2014732. doi:10.1080/21645515.2021.2014732. Epub 2022 Feb 16.
- WHO. 2020 Sept 15. https://www.who.int/news-room/feature-stories/detail/somalia-building-a-stronger-primary-health-care-system.
- Nigussie J, Girma B, Molla A, Mareg M. Tetanus toxoid vaccination coverage and associated factors among childbearing women in Ethiopia: a systematic review and meta-analysis. Biomed Res Int. 2021 Nov 8;2021:5529315. doi:10.1155/2021/5529315.
- Sato R, Fintan B. Effect of cash incentives on tetanus toxoid vaccination among rural Nigerian women: a randomized controlled trial. Hum Vaccin Immunother. 2020;16(5):1181–8. doi:10.1080/21645515.2019.1672493.
- Vouking MZ, Tadenfok CN, Ekani JME. Strategies to increase immunization coverage of tetanus vaccine among women in Sub Saharan Africa: a systematic review. Pan Afr Med J. 2017 Jun 22;27(Suppl 3):25. doi:10.11604/pamj.supp.2017.27.3.11535.
- Vouking MZ, Mengue CMA, Yauba S, Edengue JM, Dicko M, Dicko HM, Wiysonge CS. Interventions to increase the distribution of vaccines in Sub-Saharan Africa: a scoping review. Pan Afr Med J. 2019 Jan 9;32:14. doi:10.11604/pamj.2019.32.14.17225.
- Sayar MS, Akca MÖ, Asan A, Gümüş A, Göktaş SY, Necati İ, Dağlı Ö, Öztürk Ç. Tetanus immunization among healthcare professionals: cross-sectional study in Turkey. J Infect Dev Ctries. 2022;16(10):1596–601. doi:10.3855/jidc.16787.
- Mukhtar AF, Abdul Kadir A, Mohd Noor N, Mohammad AH. Knowledge and attitude on childhood vaccination among healthcare workers in hospital universiti Sains Malaysia. Vaccines. 2022;10(7):1017. doi:10.3390/vaccines10071017.
- Savage EJ, Nash S, McGuinness A, Crowcroft NS. Audit of tetanus prevention knowledge and practices in accident and emergency departments in England. Emerg Med J. 2007 Jun;24(6):417–21. doi:10.1136/emj.2007.047399.
- Toska A, Saridi M, Rekleiti M, Wozniak G, Souliotis K, Apostolopoulou E. Tetanus vaccination coverage among nurses in Greece. Am J Infect Control. 2011;3:532 533. doi:10.1016/j.ajic.2010.09.014.
- Esteve M, Carreras R, Casas I, Pena P, Guixeras A, Torrecillas S, Bretau F, Subirats P, Alonso A, Soldevila N, et al. The immune status against tetanus and diphtheria in healthcare workers in Catalonia. Vaccine. 2020;38:2646–50. doi:10.1016/j.vaccine.2020.01.076.