
ABSTRACT
Today, neonatal tetanus accounts for a significant portion of newborn and under−5 mortality – 40% and 57%, respectively – and is the most prevalent cause of neonatal mortality and morbidity, particularly in developing nations. As a result, more study on birth protection against neonatal tetanus is required because it is such a terrible condition with such a high death rate and there is a need for more recent evidence on it. From April 1 to 30, 2022, a community-based cross-sectional survey was carried out in the Gozamn district of Northwest Ethiopia. A two-stage stratified sampling procedure was applied, with an overall sample size of 831. The data were gathered using a pre-tested, structured questionnaire. It was then checked, cleaned, and entered into Epidata software version 4.6 before being exported to Stata version 14 for analysis. The proportions of birth protected against neonatal tetanus were 58.57% (95% CI (55.15–61.89%) in the study. Mother who had radio (AOR = 3.09,95%CI: 2.09, 4.56), mother who travel less than one hour to reach nearest health facility (AOR = 1.96,95%CI: 1.23,3.10), mother who gave birth of their last child in the health institution (AOR = 4.17,95%CI:2.39,7.28), mothers who had information from health professional (AOR = 2.56,95%CI:1.56,4.19) and > 4 ANC visit (AOR = 2.57,95%CI:1.55,4.26) were positive predictors of birth protected against neonatal tetanus. Low levels of maternal protection against neonatal tetanus were seen in this study location. To enhance the percentage of births protected against neonatal tetanus, professional-based guidance regarding the TT vaccine are essential.
Background
Tetanus, sometimes known as “lockjaw,” is an acute deadly disease brought on by a toxin-producing bacterium called Clostridium tetani. It is one of the diseases that can be prevented by vaccination.Citation1 Globally, an estimated 3.3 million neonatal deaths occur each year and about 9,000 babies who were within the first 28 days of life die each day. From this death, neonatal tetanus shares a high number and constitutes 40% of under 5 mortality and 57% of infant mortality.Citation1,Citation2 According to Ethiopian demographic health survey, neonatal mortality increases by 1% from 2016 to 2019 (from 29 to 30), from those death, 9% were due to tetanus, which are 4.5 from 1000 live birth.Citation3,Citation4
World health organization recommends that all child-bearing aged women should receive five dose of tetanus vaccine for the prevention of tetanusCitation5,Citation6 and vaccinating pregnant mother with at least two dose during pregnancy can decrease neonatal tetanus by 94%.Citation7,Citation8 The first dose of tetanus vaccine can be given at any time within the age of 15 to 45 years; the second dose given at 4 week apart after first dose and the third dose can be given 6–12 months apart after second dose; the fourth and fifth doses can be given after one year apart of three and four doses; after fifth dose of tetanus vaccine, the protective antibody may last for 20 years.Citation7 Nowadays, the majority of the nation adds tetanus vaccination to their routine immunization regimen in order to protect the newborn.Citation9
Although the World Health Organization launched the maternal and neonatal tetanus elimination program (MNTE), which can be accomplished through the ANC (Antenatal Care) immunization of pregnant mothers, 14 countries in three regions were still unable to complete this initiative in 2018.Citation10 In addition, in spite of Ethiopia was validated for the MNTE initiative, there are still at least one neonatal tetanus death per 1000 live births in a single district each year, and the disease has a high virulence rate.Citation10,Citation11 This indicated that no enough mother were vaccinated to protect against neonatal tetanus.Citation1,Citation12 According to the 2016 Ethiopian demographic health survey, only 49% of mothers received a protective dose of tetanus immunization against neonatal tetanus.Citation11
The possible factor related to immunization against neonatal tetanus that were identified in different literature were women accessibility for information from media, the presence or absence of ANC (Antenatal care) contact.Citation13–15
The studies conducted in southern Ethiopian Demboya and Duguna Fango and Dukem, Ethiopia showed 72.5%, 69.3% and 39.2% of births were protected against neonatal tetanus, respectively.Citation16,Citation17 The study done in western Ethiopia, Ilu Aba Bora, showed that only 310, or around 39.8%, of women were protected at birth against neonatal tetanus.Citation18 The study conducted in Tigray, Ethiopia shows 40.2% of mothers were protected against neonatal tetanus during their last pregnancyCitation13 and a cross-sectional institutional study carried out in the University of Gondar comprehensive hospital revealed that 69.8% of mothers had received a protective dose of tetanus vaccine.Citation19
Studies related to birth protected were conducted but some studies focused on mothers who gave births before one year, which could lead to recall bias, and another study relied on secondary data, making it difficult to account for all important factors. Finally, another study focused only on urban residents, making it difficult to generalize to rural residents.Citation15,Citation20,Citation21
Therefore, this research aimed to assess birth protected for protection of neonatal tetanus in Gozamn district.
Methods
Study design, area and period
A community-based cross-sectional study was conducted from April 1 to 30, 2022, in Gozamn district, Northwest Amhara region. Gozamn district is one of the four most populous districts in the east Gojjam zone, it covered a total area of 1271.8 square Kms. Based on the 2007 National Census conducted by the Central Statistical Agency of Ethiopia (CSAE) and Gozamn district administration office report, this district in 2020 has an estimated 161,952 population, of whom 81,138 are females, and the total female reproductive age groups are 37,896. Within a year, around 6000 women are expected to give birth. It has 24 rural and 2 urban kebeles. Gozamn district is located 265 km from Bahir Dar and 299 km from Addis Ababa. This district has 6 health centers, 6 maternity waiting homes, 4 private primary clinics, 27 health posts, and Gozamn district has 206 technical, 95 administrative, 35 health extension workers, and 21 midwife staff. All governmental health facilities have immunization services, and all those facilities can provide tetanus vaccine immunization services. The source of population for this study was all mothers who gave birth in the past 6 months in Gozamn district, Northwest Ethiopia and the study population for this study was all mothers who gave birth in the last 6 months in the selected kebele during the data collection period. The inclusion criteria for this study were all mothers who gave birth within the past 6 months in Gozamn district and who had resided for at least 6 months in Gozamn district. Mothers who gave birth in Gozamn district but whose ANC follow-up was outside of Gozamn district were excluded.
Sample size determination
Sample sizes were calculated using manual methods for single populations proportions formula including the following assumption.
(A) For single population proportion, the following parameters were considered:
P = Proportion of mothers who have been immunized with TT protective dose was 56.2%Citation21
d = margin of error = 0.05 with 95% confidence interval
z = 1.96 (level of significance)
n = (zα/2)2p (1 − p)/d2 = (1.96) 2.562 (1–0.562)/(0.05) 2 = 3.8416(0.526×0.438)/0.0025 = 378
Design effect 2 and 10% non-respondent rate were added to the single population proportion formula mentioned above and the final sample size was 831.
Sampling procedure and technique
The study employed a two-stage stratified sampling method. The district’s 26 kebele were divided into urban and rural kebele. 24 rural kebele and 2 urban kebele are present. Then, simple random selection approach was used to choose 1 urban and 8 rural kebele. Before the actual data collection in all the selected kebele, moms who had given birth within the previous six months were registered using a family folder, a delivery registration book, and a vaccination chart at each health post level. Their household arrangement was used to determine the registration order in order to make data collection easier. After that, the whole sample size was proportionally distributed to the chosen kebele, and the study subjects were drawn using a simple random sampling technique from the registration list.
Study variables
Birth protected against neonatal tetanus was the Dependent Variable and the Independent variables includes Sociodemographic characteristics (age, marital status, religion, educational status of the mother, educational status of husband, mother occupation, husband occupation, use of mass media, place of residence, and making a joint decision with husband for a health issue, household wealth status), Reproductive factors (parity and pregnancy plan), Awareness and knowledge related factors (knowledge, attitude) and Health service-related factors (accessibility of ambulance service and getting information for TT vaccination from health professionals, ANC visit, and use of modern family planning method).
Operational definitions
Protected at birth (PAB) agianst neonatal tetanus
If the mother had received documented or not, two or more doses during last pregnancy or at least two TT doses prior to the last pregnancy of which the last dose was <3 years before the birth; or three doses within the 5 years before the last pregnancy; or four doses with the last dose <10 years before the pregnancy or receiving five doses or more before the last pregnancy.Citation11,Citation16
Knowledge
It was measured that if respondents correctly answered > 5 out of 9 knowledge questions about tetanus toxoid vaccination, which means 60% or above, they were considered to have good knowledge and below that, poor knowledge.Citation22
Attitude
Assessed through a 5-point Likert scale (i.e. strongly disagree; disagree; neutral; agree; and strongly agree), and a score of 1 for strong disagree, 2 for disagree, 3 for neutral,4 for agree and 5 for strongly agree then it was dichotomiz by mean score as favorable vs unfavorable attitudes.Citation23
Household wealth status
Derived using principal components analysis with the five categories (lowest, second, middle, fourth, and highest).Citation16,Citation20
Data collection procedures
The data were collected by unemployed deploma midwives. They were trained for two days by the principal investigator on the study instrument, consent form, and data collection procedure. The principal investigator supervised all the procedures of the data collection.
Data quality control management
To maintain data quality, the questionnaire (English version) was translated into Amharic and translated back to English by two different people. The data collectors received two days of training on the study’s objective, relevance, and confidentiality of information, as well as the respondents’ right to informed consent. A week before data collection, the questionnaire was pre-tested in the LUMAME district on 10% (83) of the final sample by the principal investigator. The goal of the pre-testing was to guarantee that respondents could understand the questions and to rationally examine the phrasing, logic, and skip patterns of the questions. Amendments were made as a result of the pre-testing. The supervisor was required to examine the data collection procedure on a regular basis to ensure the accuracy and consistency of the data collected, and any problems discovered during the process were repaired.
Data analysis
After data collection, the data were checked, cleaned, and entered into Epidata software version 4.6 and then exported to Stata Version 14 for analysis. Descriptive statistics were used to summarize the data. To find potential variables for a multivariable logistic regression analysis, a bivariable logistic regression analysis was carried out. All explanatory variables with a p value of less than 0.2 in bivariable logistic regression analysis were included in multivariable logistic regression analysis to identify independent predictors. Then, crude and adjusted odds ratios together with their corresponding 95% confidence intervals were computed. In this study, a p value of 0.05 was considered statistically significant.
Result
Sociodemographic factors
From a total of 831 study participants required for the study, 823 mothers who had given birth in the past 6 months prior to the study participated, giving a total response of about 99%. About eight participants refused to participate in the study and 346 (42.04%) of the respondents age falls in the range of 30–34 years. About 99.6% of the respondents were Orthodox in religion.
Regarding to marital status, majority of them 791 (96.11%) were married and about 700 (85.05%) of the respondents were resides to rural area. Of the 823 respondent 592 (71.93%) mothers and 590 (74.59) husbands had no formal education and majority of respondent about 745 (90.52%) were house wife and most of husbands about 645 (81.54) were farmer.
Concerning media exposure around 386 (46.9%) of respondent have radio and around 122 (14.82%) of the respondent have television and around 254 (30.86%) of the respondent can making joint decision with husband about the health issue ().
Table 1. Socio-demographic characteristics of respondents in assessment of birth protected against neonatal tetanus and associated factor in Gozamn district, 2022.
Immunization status
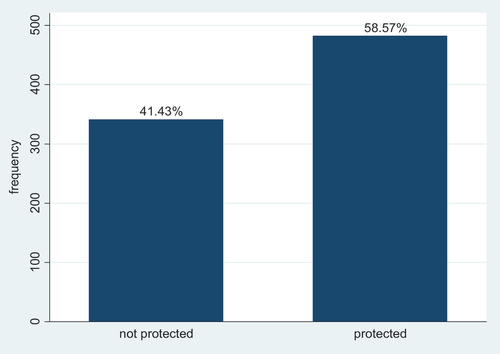
Related to birth protected against neonatal tetanus around 482 (58.57%) (95% CI(55.15–61.89%) of last birth with 6 month were protected. Among 823 respondents, around 102 (12.39%) of the respondents did not take TT vaccine throughout their life. As mothers were asked for the reasons why they do not started tetanus toxoid vaccination, the response was not aware about TT vaccine (22, 21.57%), no body advice about TT vaccine (15, 14.71%), service area to far (26, 25.49%), fear of side effect (10, 9.80%), and no problem experienced (29, 28.43%) were main reasons for not starting TT vaccination (). Among those 721 who took TT vaccine, around 233 (32.32%) took TT1, 238 (33.01%) took TT2, 198 (27.46%) took TT3, 31 (4.30%) took TT4, and around 21 respondents who is 2.91% took last dose (TT5) throughout their life ().
Figure 1. Pie chart for reason of respondent being not vaccinated throughout their life at Gozamn district, Ethiopia, 2022.
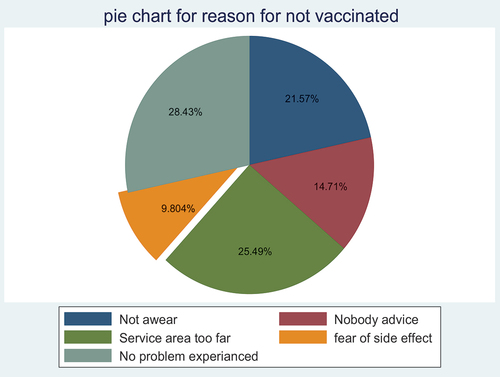
Figure 2. Births protected against neonatal tetanus in Gozman district, Northwest Ethiopia, 2022.
Reproductive related factor
Out of 823 respondents, majority of the respondents around 471 (57.23%) gave birth of 2–4 children in their life and 512 (62.21%) of women had plan for the last pregnancy and around 746 (90.64%) of women have future fertility plan. ()
Table 2. Frequency of some reproductive related factors related to birth protected against neonatal tetanus among mothers in Gozamn district, 2022.
Awareness and knowledge related Factors
Related to knowledge around 443 (53.83%) had poor knowledge () and around 613 (74.48%) of women had favorable attitude with a mean score of 11.6 (±3.24).
Table 3. Frequency of knowledge response of mothers on tetanus and TT vaccine in Gozamn district, Northwest Ethiopia, 2022.
Health service related factor
Related to health service availability around 175 (21.26%) of women have to walk on foot greater than 1 h to reach to health facility to gate service and around 190 (23.09%) of women had no access for ambulance service and majority of women which is 601 (73.03%) had no information obtained from health profession, almost 737 (89.55%) of women had visited by health extension package worker at home and majority of women which is 379 (46.05%) had greater than four ANC visit in the last pregnancy and 291 (35.36%) of women had no ANC visit in the last pregnancy and around 675 (82.02%) of women had history of family planning use throughout her life and 213 (25.88%) of women gave birth of last pregnancy at home ().
Table 4. Frequency of selected health service-related factors in Gozamn district, Northwest, Ethiopia, 2022.
Factors associated with birth protected against neonatal tetanus
The results of the bi-variable analysis showed that variables: residence, mother education, mother occupation, having radio, having television, joint decision with husbanded about health issue, wealth index, plan for last pregnancy, knowledge of respondent, attitude of respondent, distance from home to health facility, accessibility of ambulance, getting information from health professional, visited by health extension package worker at home, number of ANC visit, family planning use, place of delivery of last child were associated with birth protected against neonatal tetanus at 20% of level of significance.
The final multivariable logistic regression model showed that variables such as having radio, distance from home to health facility, getting information from health professional, number of ANC visit, and place of delivery of last child were independent predictors of birth protected against neonatal tetanus with p value < 0.05 (). The model fitness also cheeked using Hosmer-Lemeshow goodness-of-fit test and it fields a p value of 0.088.
Table 5. Factor associated with birth protected against neonatal tetanus among mothers who gave birth in the past six month in Gozamn district, Northwest Ethiopia, 2022.
Discussion
This study showed that the proportion of birth protected against neonatal tetanus among mothers who gave birth within six month found to be 58.57% which is in line with study done in Peshawar district Pakistan and Northern Ethiopia about 55.6% and 56.2%, respectively,Citation21,Citation24 and it is somewhat higher than the study conducted in different communities of Nigeria (24%)Citation14 and study conducted in 2016 Ethiopian demographic health survey (EDHS), Eastern Ethiopia Dukem Town and Errer District, Somali Regional State (49%), (39.2%), and (51.8%), respectively,Citation3,Citation15,Citation22 and study conducted in Tigray Ethiopia (40.2%).Citation13 The reason for the difference might be the difference in sample size, the time variation when the study conducted, cultural variation of study participant on health sacking behavior and technological improvement throughout time as a source of information.
On the other hand, this study finding is lower than study conducted in Lahore district Pakistan, Sierra Leone, Kenya and southern Ethiopia (Demboya) range from 72 to 91%.Citation16,Citation25–27 This discrepancy might be due to difference of healthcare coverage of different countries and lack of similar implementation of TT vaccine schedule in deferent area of our country.
The finding of this study showed that Getting information from health professional were an independent predictor of birth protected against neonatal tetanus, mothers who had information from health professional were 2.56 times more likely to be protected against neonatal tetanus as compared with its counterpart. This finding is consistent with the study conducted in southern part of Ethiopia.Citation17 This is because providing information to mothers during an ANC visit or during birth can improve their awareness and practice of the tetanus vaccine. And also systematic review conducted in different literature related to vaccine acceptance during pregnancy also stated that information and recommendation that was given from health professional was a good predictor of service utilization of mother;Citation28 therefore, those health professionals take their time while advising on the TT vaccine in the study area.
Another factor that was found to be an independent predictor of birth protected against neonatal tetanus was the number of ANC visits, with women who had four or more ANC visits being 2.57 times more likely to be protected against neonatal tetanus than mothers who did not have any ANC visits. This finding also congruent with the study conducted in east Africa, Ivory Coast and southern Ethiopia.Citation16,Citation17,Citation29,Citation30 This could be because mothers who have had multiple ANC visits have a better understanding of the TT vaccine and neonatal tetanus, and also TT vaccine is one of the components of ANC care, so those mothers who have had multiple ANC visits are more likely to be vaccinated for neonatal tetanus prevention. Additionally, going to an ANC appointment can enhance contact with a healthcare practitioner, increasing the likelihood of learning more about vaccinations.
In terms of media exposure, this study showed that those respondents who had radio were 3.09 times more likely to be protected against neonatal tetanus than those who did not, which is in agreement with study conducted in Ethiopia.Citation18,Citation20 This conclusion might be explained by the fact that crucial health information was broadcasted over the radio, so it raises people’s awareness of the TT vaccine and neonatal tetanus. Additionally, information conveyed via radio has the power to alter individual behavior and vaccination-related perceptions.
Place of delivery was another determinant of birth protected against neonatal tetanus. Those mothers who gave birth to their last child in a health institute were 4.17 times more likely to be protected against neonatal tetanus than their counterparts; this finding is congruent with the studies conducted in East Africa and Ethiopia.Citation16,Citation17,Citation29,Citation31 This may be true because moms who gave birth in a health facility are more likely than mothers who gave birth at home to seek information and learn useful information. These mothers may also have positive attitudes toward frequent ANC follow-up and the practise of seeking out medical care. Therefore, institutional delivery is vital to increase births protected against neonatal tetanus in the study area.
In this study, the distance between home and health facility was a favorable predictor of birth protected against neonatal tetanus. Mothers who travel less than 1 h to reach nearest health facility were 1.96 more likely to be protected against neonatal tetanus as compared with mother who travel more than 1 h. This finding is consistent with study done in Pakistan, East Africa, Southern and Eastern Ethiopia, and Errer district Somalia Ethiopia,Citation15,Citation16,Citation22,Citation24,Citation29 this might be due to when the distance from home to health facility increases, they might be reluctant to go to health facility whether for ANC follow-up or others health service, the health and wellness center in India can provide a comprehension primary care for the entire population; so it has to be practice in low-income countryCitation32 and also involvement of civil society and community-based organization is crucial for the universal coverage of healthcare services.Citation33 So increasing accessibility of health institution in the study area also another vital to increase birth protected against neonatal tetanus.
Limitation
Even if the duration was reduced to six months, recall bias still exists. To reduce recall bias, the card and registration book were not reviewed. Those are limitation of this study.
Conclusion and recommendation
Finally, in this study area, those mothers who protected against neonatal tetanus are low. And also having radio, distance from home to nearest health facility, place of delivery of last child, getting information from health professional and number of ANC visit were predictors of birth protected against neonatal tetanus.
To increase the number of births protected against neonatal tetanus, policymakers and others need to work on how to interlink and strengthen various healthcare services such as ANC visit and delivery services, and also need to enhance professional advice instead of increasing awareness of the community in the study area related to vaccination and neonatal tetanus. It is good to concentrate on raising awareness through other techniques, including media exposure and work on how to increase accessibility to healthcare services. The health professional need to adopt the habit of counseling, and it is preferable to link the various healthcare services in order to increase the number of mothers who are protected against neonatal tetanus. Other research in this area is good to conduct with the purpose of determining the proportion of mothers who are protected against neonatal tetanus by antibody testing in order to identify the absolute proportion of mothers who are protected from tetanus at birth.
Authors’ contributions
AG designed the study, was involved in data collection, analysis, and interpretation of the result and drafted the paper, and participated in preparing all versions of the manuscript. AT, MH, EA, AZ, MA, MD, SK,YA, TG, DY and AA assisted in the design and the proposal development, monitored data collection, assisted during analysis, and revised subsequent drafts of the paper. All authors read and approved the final manuscript.
Ethical approval and consent to participate
The ethical approval was obtained from the University of Gondar’s School of Midwifery’s ethical review committee with reference number (MIDW/23/2014), A letter of permission was written to the Gozamn district health office from the school of midwifery, University of Gondar. The letter of cooperation was written by the Gozamn district health office for each kebele. Following an explanation of the purpose of the study, written informed consent was obtained from participants. For those who cannot write and read the consent form was read in front of witness (their friends, relatives and independent body of research team) and the witness also signed and provided written informed consent, so for those minor participants the informed written consent was taken from their parents. Also, affirmation was made that they are free to withdraw consent and discontinue participation without any form of prejudice. All participants were assured confidentiality of information and privacy of their personal information. To preserve confidentiality, the data was not exposed to any third party except the investigators. All necessary methods were carried out in accordance with the guidelines of institutional and declaration of Helsinki.
List of abbreviations
EDHS Ethiopia Demographic and Health SurveyMNTE Maternal and Neonatal Tetanus Eliminization ProgramPAB Protected At BirthTT Tetanus Toxoid
Acknowledgments
First and foremost, we would like to express our gratitude to all of the participants in the study as well as the data collectors. We would also like to express our gratitude to all of the Gozamn district’s health extension workers. Last but not least, we would like to thank the staff at the Gozamn District Health Office for their cooperation and permission to collect data.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to preserving participant anonymity but are available from the corresponding author on reasonable request(Anteneh Gashaw, [email protected]) https://orcid.org/0009-0002-8396-2186.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Khan R, Vandelaer J, Yakubu A, Raza AA, Zulu F. Maternal and neonatal tetanus elimination: from protecting women and newborns to protecting all. Int J Women’s Health. 2015:171–80. doi:10.2147/IJWH.S50539.
- Lives SN. State of the world’s newborns. Washington (DC): Save the Children; 2001.
- EDHS I. Ethiopia demographic and health survey 2016. Addis Ababa (Ethiopia) and Rockville (MD): CSA and ICF; 2016.
- Maru M, Getahun A, Hosana S. A house-to-house survey of neonatal tetanus in urban and rural areas in the Gondar region, Ethiopia. Trop Geogr Med. 1988;40:233–8.
- Maternal W. Neonatal tetanus (MNT) elimination. 2012.
- Organization WH. Maternal and neonatal tetanus elimination by 2005: strategies for achieving and maintaining elimination. Maternal and neonatal tetanus elimination by 2005: strategies for achieving and maintaining elimination. 2000.
- Blencowe H, Lawn J, Vandelaer J, Roper M, Cousens S. Tetanus toxoid immunization to reduce mortality from neonatal tetanus. Int J Epidemiol. 2010;39(suppl_1):i102–i9. doi:10.1093/ije/dyq027.
- Vandelaer J, Birmingham M, Gasse F, Kurian M, Shaw C, Garnier S. Tetanus in developing countries: an update on the maternal and neonatal tetanus elimination initiative. Vaccine. 2003;21(24):3442–5. doi:10.1016/S0264-410X(03)00347-5.
- Prevension cfdca. Vaccine and preventable disease division of bacterial diseases. 2020 Jan 22.
- Organization WH. Protecting all against tetanus: guide to sustaining maternal and neonatal tetanus elimination (MNTE) and broadening tetanus protection for all populations. 2019.
- ICF CSACEa. Ethiopia demographic and health survey 2016. 2016.
- Esen B, Kurtoglu D, Coplu N, Gozalan A, Miyamura K, Ishida S, Akin L. Tetanus immunization status among women of childbearing age in Turkey. Jpn J Infect Dis. 2007;60:92.
- Mengesha MB, Weldegeorges DA, Assefa NE, Gebremeskel SG, Hidru HD, Teame H, Hailesilassie Y. Tetanus toxoid immunization status and associated factors among mothers in Hawzen, Eastern zone of Tigray, Ethiopia, 2019. Open Public Health J. 2020;13(1):281–8. doi:10.2174/1874944502013010281.
- Mohammed A, Usman R, Difa A, Danimoh A, Envuladu E. Determinants of uptake of tetanus toxoid vaccine among women of reproductive age in a selected community in Funakaye LGA, Gombe State, Nigeria. Age. 2019;15(24):25–34.
- Anatea MD, Mekonnen TH, Dachew BA. Determinants and perceptions of the utilization of tetanus toxoid immunization among reproductive-age women in Dukem town, Eastern Ethiopia: a community-based cross-sectional study. BMC Int Health Hum Rights. 2018;18(1):1–0. doi:10.1186/s12914-018-0168-0.
- Dubale Mamoro M, Kelbiso Hanfore L. Tetanus toxoid immunization status and associated factors among mothers in Damboya Woreda, Kembata Tembaro zone, SNNP, Ethiopia. J Nutr Metab. 2018;2018:1–9. doi:10.1155/2018/2839579.
- Facha W, Yohannes B, Duressa G. Tetanus toxoid vaccination coverage and associated factors among pregnant women in Duguna Fango district, southern Ethiopia. Int J Health Res. 2018;8:148–54.
- Kenea A, Oljira D, Tesfa B, Abamecha A. Assessment of protection at birth of tetanus toxoid immunization and associated risk factors in Ilu Aba Bora zone Southwest, Ethiopia. Int J Vaccines Immun. 2016;2(3):2–7.
- Gessesse DN, Yismaw AE, Yismaw YE, Workneh TW. Coverage and determinants of protective dose tetanus toxoid vaccine among postnatal women delivered at university of Gondar comprehensive specialized hospital, northwest Ethiopia, 2019. Clin Epidemiol Glob Health. 2021;12:100814. doi:10.1016/j.cegh.2021.100814.
- Teshale AB, Tesema GA, Das JK. Determinants of births protected against neonatal tetanus in Ethiopia: a multilevel analysis using EDHS 2016 data. PLos One. 2020;15(12):e0243071. doi:10.1371/journal.pone.0243071.
- Mihret MS, Limenih MA, Gudayu TW. The role of timely initiation of antenatal care on protective dose tetanus toxoid immunization: the case of northern Ethiopia post natal mothers. BMC Pregnancy Childbirth. 2018;18(1):1–0. doi:10.1186/s12884-018-1878-y.
- Gebremedhin TS, Welay FT, Mengesha MB, Assefa NE, Werid WM. Tetanus toxoid vaccination uptake and associated factors among mothers who gave birth in the last 12 months in Errer district, Somali regional state, Eastern Ethiopia. Biomed Res Int. 2020;2020:1–8. doi:10.1155/2020/4023031.
- Klett-Tammen CJ, Krause G, Seefeld L, Ott JJ. Determinants of tetanus, pneumococcal and influenza vaccination in the elderly: a representative cross-sectional study on knowledge, attitude and practice (KAP). BMC Public Health. 2015;16(1):1–9. doi:10.1186/s12889-016-2784-8.
- Naeem M, Khan M-U-I, Abbas SH, Adil M, Khan A, Naz SM. Coverage and factors associated with tetanus toxoid vaccination among married women of reproductive age: a cross sectional study in Peshawar. J Ayub Med Coll Abbottabad. 2010;22(3):136–40.
- Hasnain S, Sheikh N. Causes of low tetanus toxoid vaccination coverage in pregnant women in Lahore district, Pakistan. East Mediterr Health J. 2007;13(5):1142–52. doi:10.26719/2007.13.5.1142.
- Yaya S, Kota K, Buh A, Bishwajit G. Prevalence and predictors of taking tetanus toxoid vaccine in pregnancy: a cross-sectional study of 8,722 women in Sierra Leone. BMC Public Health. 2020;20(1):1–9. doi:10.1186/s12889-020-08985-y.
- Hashmi FK, Islam M, Khan TA, Tipu MK. Vaccination coverage of mothers during pregnancy with tetanus toxoid and infants after birth. Pak J Pharm. 2011;24:1–3.
- Wilson RJ, Paterson P, Jarrett C, Larson HJ. Understanding factors influencing vaccination acceptance during pregnancy globally: a literature review. Vaccine. 2015;33(47):6420–9. doi:10.1016/j.vaccine.2015.08.046.
- Belay AT, Fenta SM, Agegn SB, Muluneh MW, Ortega JA. Prevalence and risk factors associated with rural women’s protected against tetanus in east Africa: evidence from demographic and health surveys of ten east African countries. PLos One. 2022;17(3):e0265906. doi:10.1371/journal.pone.0265906.
- Yaya S, Kota K, Buh A, Bishwajit G. Antenatal visits are positively associated with uptake of tetanus toxoid and intermittent preventive treatment in pregnancy in Ivory coast. BMC Public Health. 2019;19(1):1–12. doi:10.1186/s12889-019-7847-1.
- Kalayu G, Fisseha G, Shamie R, Berhe A, Embaye K. Factors associated with protection of last live birth against neonatal tetanus among mother age 15-49 in Ethiopia: a multilevel analysis using EDHS 2016. 2021.
- Lahariya C. Health & wellness centers to strengthen primary health care in India: concept, progress and ways forward. Indian J Pediatr. 2020;87(11):916–29. doi:10.1007/s12098-020-03359-z.
- Lahariya C, Roy B, Shukla A, Chatterjee M, De Graeve H, Jhalani M, Bekedam H. Community action for health in India: evolution, lessons learnt and ways forward to achieve universal health coverage. WHO South East Asia J Public Health. 2020;9(1):82–91. doi:10.4103/2224-3151.283002.