
ABSTRACT
To probe the understanding of healthcare providers regarding occupational exposure to human papillomavirus and their knowledge about human papillomavirus vaccination in relation to the American Society for Colposcopy and Cervical Pathology (ASCCP) recommendations. In this cross-sectional study, the healthcare providers at Mayo Clinic Arizona, Florida, and Minnesota were delivered an electronic survey. The survey was completed by 349 healthcare providers, with one respondent excluded for inconsistent entry. The mean age of respondents was 42.7 ± 10.9, and of those, 68% were female and 32% were male. Of the unvaccinated respondents, 43.3% were ≤ 45 y of age (eligible for vaccination), while those vaccinated formed 41% of the respondents. Healthcare providers are highly concerned about their cancer safety, as shown by their awareness of occupational human papillomavirus hazards and broad knowledge about vaccine efficacy. The use of personal protective equipment varied widely, including eyewear, double gloving, procedural face mask, N95 face mask, and/or nothing. Human papillomavirus and cancer risk was clearly perceived by healthcare providers. For professions, pairwise comparisons revealed that nurse practitioners, physician assistants, certified registered nurse anesthetists, and allied healthcare providers had lower scores than medical doctors. Despite the high level of understanding among healthcare providers of occupational human papillomavirus exposure, only a few of them knew of the recommendations of the ASCPP for vaccination of healthcare providers treating human papillomavirus-related diseases. In such cases, most of those surveyed embraced vaccination, which was considered 100% safe by medical doctors and allied health professionals.
Introduction
The human papillomavirus (HPV) is the most prevalent sexually transmitted virus infection in the United States. HPV is a small deoxyribonucleic acid (DNA) virus that targets the squamous epithelium of the human body. It is the main culprit behind squamous cancers in different organs, including the cervix, vulva, vagina, penis, anus, and oropharynx.Citation1 Low-risk HPV genotypes, mainly HPV type-6 and type-11, are liable for anogenital warts and oropharyngeal papillomatosis.Citation2
Cervical cancer is the fourth most common cancer in women globally. Global Cancer Observatory 2020 data estimated approximately 600,000 new cases of cervical cancer and 350,000 deaths from cervical cancer annually are expected.Citation3 The incidence of HPV-related head and neck cancers primarily associated with HPV type-16 overtook HPV-related cervical cancers in 2018 in the United States.Citation4 High-risk HPV, especially HPV type-16, is accountable for almost all anal cancers, and about 60% of vulvar-vaginal and penile cancers.Citation1,Citation5
HPV-related cancers are preventable by prophylactic recombinant DNA vaccines targeting the major L1 capsid protein of high-risk HPVs, such as HPV type-16 and type-18.Citation6,Citation7 The current FDA-approved HPV vaccine (Gardasil-9) supplies extended spectrum protection against high-risk HPV types 31, 33, 45, 52, and 58 and is approved for adults up to age 45 y since 2018.Citation1,Citation6,Citation8 HPV vaccination for healthcare providers who are occupationally exposed to the virus is recommended by the American Society for Colposcopy and Cervical Pathology (ASCCP) and the American College of Obstetricians and Gynecologists (ACOG).Citation7,Citation9
The treatment of HPV-related diseases consists of electrocautery, cryotherapy, loop electrical excision, and laser treatments, which providers widely use in daily practice to treat benign and preinvasive diseases. HPV-DNA has been proven to be distinctly isolatable from the surgical fumes produced during these treatments, indicating that healthcare professionals are passively exposed to HPVs during procedures to treat afflicted patients by particles found in the ambient air.Citation2,Citation10 Moreover, it has been found that the viral particles containing HPV-DNAisolated from the surgical fumes are capable of infecting HPV-negative cervical cancer cell lines.Citation10 It becomes then imperative that healthcare providers in positions vulnerable to exposure to such surgical fumes, and thus HPV-DNA molecules, mitigate their risk of susceptibility to becoming infected by a type of HPV.Citation2,Citation11
This study aims to survey the awareness of healthcare providers in the context of occupational exposure to HPV and their knowledge of HPV vaccination in parallel with the ASCCP recommendations
Methods
After being determined to be exempt from the requirement for IRB approval by the local Institutional Review Board (23-002111), an electronic survey delivered to healthcare providers at Mayo Clinic (AZ, FL, MN) between April 2023 and July 2023 focused on four main themes: the awareness of occupational exposure to HPV, the knowledge of HPV vaccination, precautions for HPV exposure, and the understanding of the relationship of HPV with cancer. The generated data from the survey was captured and stored by Research Electronic Data Capture (REDCap) software.Citation12
The demographic characteristics of healthcare providers were explored, including age, gender, HPV vaccination status, profession, and affiliated department. Additionally, healthcare providers replied to mainly four main themes within the query in which a dichotomous scale was used for each scale: (1) a 3-question scale questioning the awareness of occupational exposure to HPV (), (2) a 3-question scale questioning healthcare providers’ knowledge about HPV vaccination recommendations (), (3) and a 4-item scale questioning healthcare providers’ precautions for HPV exposure, (4) an 8-item scale questioning healthcare providers’ understanding about the relationship of HPV with cancer that included two reversal items to tackle with response bias (). The complete survey questionnaire from the REDCap database in PDF format was provided as a supplementary file.
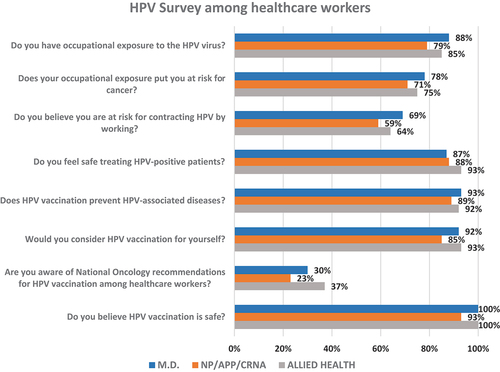
Graph 1. The responses to the HPV survey based on profession.
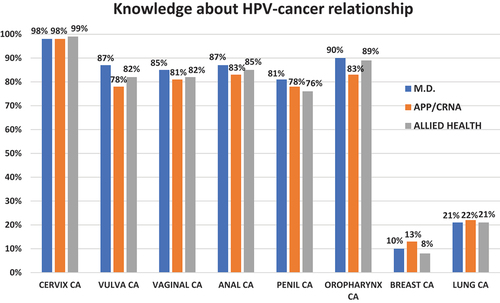
Graph 2. Knowledge about HPV-related cancers by profession.
Statistical analysis
The study’s statistical analysis was performed with open-source Jamovi statistical software (Version 2.3.21). The scale reliability of the survey was assessed with Cronbach’s alpha. The awareness of occupational HPV exposure, precautions for HPV exposure, HPV vaccine knowledge, and understanding of the relationship of HPV with cancer were compared based on age, gender, HPV vaccination status, profession, and department by non-parametric one-way analysis of variance, namely Kruskal-Wallis and pairwise comparisons were made with the Dwass-Steel-Critchlow-Fligner test. A p-value < .05 was considered statistically significant.
Results
The survey was completed by 349 healthcare providers, with one respondent excluded for inconsistent entry. Although 84% (n = 292) of respondents are well-informed about occupational human papillomavirus exposure and risk, most are unaware of the ASCCP recommendations for HPV vaccination among healthcare providers (n = 243, 70%). The majority of respondents (n = 313, 90%) were willing to get vaccinated if provided with the vaccine ().
The mean age of respondents was 42.7 ± 10.9 and of those, 68% (n = 229) female, and 32% (n = 109) male. Of the unvaccinated respondents, 43.3% (n = 87) were ≤45 y of age (eligible for vaccination approved by FDA in 2018), while those vaccinated formed 41% (n = 140) of the respondents. The demographic features of the respondents are summarized in . The value for Cronbach’s alpha for the survey was α = 0.72.
Table 1. The respondents’ demographic features (n = 348).
Awareness of occupational human papillomavirus exposure & knowledge of human papillomavirus vaccination
Providers are highly concerned about their cancer safety, as shown by their responses to three yes or no questions related to occupational HPV hazards (M.D.:2.30 ± 1.06, NP/PA/CRNA:2.18 ± 1.12 and Allied Health 2.24 ± 1.10) and broad knowledge about vaccine efficacy, as shown by their responses to three yes or no questions related to HPV-vaccine (M.D.:2.84 ± 0.41, NP/PA/CRNA:2.67 ± 0.66 and Allied Health 2.71 ± 0.59). No statistical difference was detected based on gender, vaccination status, profession, and department, respectively (p = .365; p = .082, p = .411; p = .160, p = .716; p = .081, and p = .936; p = .771) ().
Table 2. Awareness of occupational exposure to HPV and HPV-vaccination by profession.
Precautions for occupational human papillomavirus exposure
The use of personal protective equipment varied widely, including eyewear (n = 209, 60%), double gloving (n = 83, 24%), procedural face mask (n = 187, 54%), N95 face mask (n = 141, 41%), and/or nothing (n = 40, 11%). No statistical difference was detected based on gender, vaccination status, profession, and department for personal protective equipment, respectively (p = .679, p = .161, p = .294, and p = .771) ().
Table 3. Precautions for HPV exposure and knowledge about the relationship of HPV with cancers by profession.
Understanding the relationship between human papillomavirus and cancer
HPV and cancer risk was clearly perceived by healthcare providers. No statistical difference was detected based on vaccination status and department, respectively (p = .959 and p = .936). For profession (p = .002), pairwise comparisons revealed that NP/PAC/CRNAs and allied health professionals had lower scores than medical doctors, respectively (p = .038 and p = .002). Moreover, there was less knowledge about HPV-cancer relation among males (p < .001) ().
Healthcare providers had a broad knowledge of HPV-related cancers; as described previously, two reversal items were included to detect response bias, and these were breast (10%) and lung cancer (21%) ().
Discussion
This survey highlights that the awareness of occupational HPV exposure is 84% among healthcare providers, and unvaccinated respondents comprise 59% of the survey, of whom 43.3% were ≤45 y, and could be protected against occupational HPV exposure if vaccinated. However, only 30% of respondents knew of the ASCCP recommendation for vaccinating healthcare providers treating HPV-related diseases. In such cases, most respondents welcomed vaccination, which was believed to be 100% safe by medical doctors and allied health professionals.
Emerging evidence from recent studies indicates that exposure to surgical smoke during procedures on HPV-related lesions may result in nasal and oropharyngeal HPV infection. For healthcare workers specializing in gynecology, dermatology, otolaryngology, urology, and proctology, understanding the role of surgical smoke in relation to HPV-associated lesions is critical for their practice. A growing body of research suggests a possible association between performing such procedures that involve HPV-associated lesions and generating surgical smoke and a handful of cases of HPV-related upper respiratory tract disease in medical workers with suspected occupational origins.Citation10–15 This information could inspire healthcare providers to protect themselves from surgical smoke. In parallel with this, the awareness of occupational exposure to HPV among healthcare providers in this survey is remarkable. The National Institute for Occupational Safety and Health (NIOSH) recommends using high-efficiency local smoke evacuators in addition to general room ventilation, which must contain a high-efficiency particulate air (HEPA) filter or equivalent.Citation13 Smoke evacuation has been considered an effective and beneficial method for reducing surgical smoke. It has been proven to be the most effective way to lower the potentially hazardous effects of electrosurgical and laser plumes.Citation11,Citation16 Despite the lack of guidelines regarding respirator usage during surgical procedures, it is clear that NIOSH-approved respirators or N95 masks offer the most significant protection against surgical plumes generated by electrocautery, lasers, or ultrasonic scalpels.Citation17 Survey data showed that healthcare providers underestimated N95 face masks (n = 141, 41%) as a protective measure against surgical plumes, considered carriers for HPV-DNA. To develop behavior-changing interventions, it’s imperative to perform a root cause analysis that uncovers the underlying attitudes and beliefs influencing their actions.
It has been estimated that nearly half a million of healthcare providers are exposed to surgical smoke annually by the American Occupational Safety and Health Administration. This estimation signifies that occupational exposure to HPV is a growing concern for governing bodies and providers in healthcare.Citation17,Citation18 In reaction to this warning, the ASCCP recommended HPV vaccinations for healthcare providers treating HPV-related lesions; however, only 30% of healthcare providers in this survey were aware of that recommendation.Citation7,Citation9 The consumption of health-related videos on social media in the United States has been on the rise.Citation19 Developing effective social media strategies is crucial in spreading awareness of national oncology recommendations on HPV exposure and vaccination among healthcare providers.
Surprisingly, even if it was believed that the human papillomavirus vaccine was safe, it was unveiled in this survey that 59% of the healthcare providers were unvaccinated, of whom 43.3% were ≤45 y. Although ACOG announced HPV vaccine is safe and effective, vaccine hesitancy varies across countries and healthcare providers.Citation20,Citation21 The worldwide acceptance and uptake of HPV vaccines have been impacted by a multitude of factors.Citation22 This might stem from the lack of knowledge about the vaccine and its safety, which could be overcome through vocational education.Citation23 The Health Belief Model (HBM) theory has been used to explore the dynamics of human behavior in regards to vaccination.Citation24 Recent studies have revealed that the perception of susceptibility, severity, benefit, self-efficacy, and behavioral intention plays a crucial role in determining the uptake of HPV vaccination. Prioritizing the elements of the HBM might effectively increase HPV vaccination rates among healthcare workers.Citation22,Citation25 All in the healthcare system should be vaccinated, especially those ≤45 y. Employers are responsible for advocating for their staff and making the vaccine readily available. It was revealed in this survey analysis that most employees would welcome this if vaccination was provided. One of the main barriers to HPV vaccination is the high cost of the three-dose vaccine series, which has negatively impacted the elements of the HBM.Citation22 The three dose vaccine series should be covered without financial burden to the employee at risk.
Strengths and limitations
The greatest strength of our survey was pinpointing a neglected subject with well-crafted questions. To the best of our knowledge, our survey is the first to reveal awareness among healthcare providers regarding occupational exposure to HPV, as well as their understanding and attitudes toward vaccination.
The response rate in our survey was 26%, which could have affected the results due to an increased sampling bias. Furthermore, the survey analysis is also prone to both recall and selection bias due to its nature (respondents were contacted by e-mail). The acquiescence bias for our survey was 10% and 21%. The cross-sectional design of the survey provides a fourth-level grade of scientific evidence.
Author contributions (in credit format)
Author 1: Investigation, methodology, project administration, resources, software, validation, visualization, writing – original draft, review, and editing; Author 2: Data curation, formal analysis, investigation, methodology, project administration, writing – original draft, review, and editing; Author 3: Data curation, formal analysis, investigation, methodology, project administration, writing – original draft, review, and editing; Author 4: Resources, validation, visualization, writing – original draft, review, and editing; Author 5: Formal analysis, resources, writing – review and editing; Author 6: conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, validation, visualization, writing – original draft, review, and editing.
Ethics
This survey study was conducted in conformity with the principles of the Declaration of Helsinki after being determined to be exempt from the requirement for IRB approval by the local Institutional Review Board [23–002111). As protected health information is not being requested from subjects, Health Insurance Portability and Accountability Act authorization is not required in accordance with 45 CFR 160.103.
Informed consent statement
Informed consent was obtained from all participants of the study.
Supplementary file HPV Survey Questionnaire.pdf
Download PDF (779.6 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed on the publisher’s website at https://doi.org/10.1080/21645515.2024.2342622.
Additional information
Funding
References
- Harden ME, Munger K. Human papillomavirus molecular biology. Mutat Res Rev Mutat Res. 2017;772:3–6. doi:10.1016/j.mrrev.2016.07.002.
- Palma S, Gnambs T, Crevenna R, Jordakieva G. Airborne human papillomavirus (HPV) transmission risk during ablation procedures: a systematic review and meta-analysis. Environ Res. 2021;192:110437. doi:10.1016/j.envres.2020.110437.
- Singh D, Vignat J, Lorenzoni V, Eslahi M, Ginsburg O, Lauby-Secretan B, Arbyn M, Basu P, Bray F, Vaccarella S, et al. Global estimates of incidence and mortality of cervical cancer in 2020: a baseline analysis of the WHO global cervical cancer elimination initiative. Lancet Glob Health. 2023;11(2):197–206. doi:10.1016/S2214-109X(22)00501-0.
- Subbarayan RS, Shew M, Enders J, Bur AM, Thomas SM. Occupational exposure of oropharyngeal human papillomavirus amongst otolaryngologists. Laryngoscope. 2020;130(10):2366–2371. doi:10.1002/lary.28383.
- Szymonowicz KA, Chen J. Biological and clinical aspects of HPV-related cancers. Cancer Biol Med. 2020;17(4):864–878. doi:10.20892/j.issn.2095-3941.2020.0370.
- Dilley S, Miller KM, Huh WK. Human papillomavirus vaccination: ongoing challenges and future directions. Gynecol Oncol. 2020;156(2):498–502. doi:10.1016/j.ygyno.2019.10.018.
- Harrison R, Huh W. Occupational exposure to human papillomavirus and vaccination for health care workers. Obstet Gynecol. 2020;136(4):663–665. doi:10.1097/AOG.0000000000004021.
- U.S. Food & Drug Administration. Approval letter of Gardasil 9; 2018 Feb 9. https://www.fda.gov/media/110875/download?attachment.
- American Society for Colposcopy and Cervical Pathology. American Society for Colposcopy and Cervical Pathology recommends HPV vaccination for providers. https://www.asccp.org/hpv-vaccination.
- Yan L, Liu Y, Zhang J, Chen X, Li J, Zhu X. In vivo and in vitro study of the potential hazards of surgical smoke during cervical cancer treatment with an ultrasonic scalpel. Gynecol Oncol. 2022;164(3):587–595. doi:10.1016/j.ygyno.2022.01.006.
- Liu Y, Song Y, Hu X, Yan L, Zhu X. Awareness of surgical smoke hazards and enhancement of surgical smoke prevention among the gynecologists. J Cancer. 2019;10(12):2788–2799. doi:10.7150/jca.31464.
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010.
- The National Institute for Occupational Safety and Health Control of Smoke from Laser/Electric surgical procedures. Department of health and human services; 1996. p. 96–128. https://www.cdc.gov/niosh/docs/hazardcontrol/hc11.html.
- Manson LT, Damrose EJ. Does exposure to laser plume place the surgeon at high risk for acquiring clinical human papillomavirus infection? Laryngoscope. 2013;123(6):1319–1320. doi:10.1002/lary.23642.
- Shemtob L, Asanati K, Jayasekera P. Should healthcare workers with occupational exposure to HPV be vaccinated? Occup Med (Lond). 2023;73(3):115–116. doi:10.1093/occmed/kqad005.
- Takahashi H, Hirota M, Takahashi T, Yamasaki M, Miyazaki Y, Makino T, Kurokawa Y, Takiguchi S, Mori M, Doki Y, et al. Simultaneous automatic insufflation and smoke-evacuation system in flexible gastrointestinal endoscopy. Endoscopy. 2016;48(6):579–583. doi:10.1055/s-0042-102782.
- Edwards BE, Reiman RE. Comparison of current and past surgical smoke control practices. AORN J. 2012 Mar;95(3):337–350. doi:10.1016/j.aorn.2011.07.019.
- Fox-Lewis A, Allum C, Vokes D, Roberts S. Human papillomavirus and surgical smoke: a systematic review. Occup Environ Med. 2020;77(12):809–817. doi:10.1136/oemed-2019-106333.
- Garg A, Nyitray AG, Roberts JR, Shungu N, Ruggiero KJ, Chandler J, Damgacioglu H, Zhu Y, Brownstein NC, Sterba KR, et al. Consumption of health-related videos and human papillomavirus awareness: cross-sectional analyses of a US national survey and YouTube from the urban-rural context. J Med Internet Res. 2024;26:e49749. doi:10.2196/49749.
- Young JL, Bernheim RG, Korte JE, Stoler MH, Guterbock TM, Rice LW. Human papillomavirus vaccination recommendation may be linked to reimbursement: virginia family practitioners and gynecologists survey. J Ped Adolesc Gynecol. 2011;24(6):380–385. doi:10.1016/j.jpag.2011.06.016.
- Lin C, Mullen J, Smith D, Kotarba M, Kaplan SJ, Tu P. Healthcare providers’ vaccine perceptions, hesitancy, and recommendation to patients: a systematic review. Vaccines. 2021;9(7):713. doi:10.3390/vaccines9070713.
- Shao X, Lu X, Zhou W, Huang W, Lu Y. HPV vaccination behavior, vaccine preference, and health beliefs in Chinese female health care workers: a nationwide cross-sectional study. Vaccines. 2023 Aug 15;11(8):1367. doi:10.3390/vaccines11081367.
- Tubaş F, Dulkadir R, Taplak AŞ, Ünlü E. Knowledge and attitudes of physicians and nurses in Turkey regarding human papillomavirus vaccination of their children. J Community Health. 2023;48(1):99–103. doi:10.1007/s10900-022-01141-0.
- Jose R, Narendran M, Bindu A, Beevi N, Manju L, Benny PV. Public perception and preparedness for the pandemic COVID 19: a health belief model approach. Clin Epidemiol Glob Health. 2021;9:41–46. doi:10.1016/j.cegh.2020.06.009.
- Wang Z, Fang Y, Chan PS, Chidgey A, Fong F, Ip M, Lau JTF. Effectiveness of a community-based organization-private clinic service model in promoting human papillomavirus vaccination among Chinese men who have sex with men. Vaccines. 2021;9(11):1218. doi:10.3390/vaccines9111218.