
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Background: In low- and middle-income countries where vaccination rates are low, tetanus is still an important threat to public health. Although maternal and neonatal tetanus remains a major global health concern, its magnitude and determinates are not well studied. Therefore, this study aimed to assess the number of tetanus toxoid injections and associated factors among pregnant women in low- and middle-income countries.
Methods: Data from the most recent Demographic and Health Surveys, which covered 60 low- and middle-income countries from 2010 to 2022, was used for secondary data analysis. The study included a total of 118,704 pregnant women. A statistical software package, STATA 14, was used to analyze the data. A negative binomial regression of a cross-sectional study was carried out. Factors associated with the number of tetanus vaccinations were declared significant at a p-value of < 0.05. The incidence rate ratio and confidence interval were used to interpret the results. A model with the smallest Akaike Information Criterion and Bayesian Information Criterion values and the highest log likelihood was considered the best-fit model for this study.
Results: In low- and middle-income countries, 26.0% of pregnant women took at least two doses of the tetanus toxoid vaccine. Factors such as maternal education, primary (IRR = 1.22, 95% CI: 1.17, 1.26), secondary (IRR = 1.19, 95% CI: 1.15, 1.23), higher (IRR = 1.16, 95% CI: 1.12, 1.20), employment (IRR = 1.11, 95% CI: 1.09, 1.13), 1-3 ANC visits (IRR = 2.49, 95% CI: 2.41, 2.57), ≥4 visits (IRR = 2.94, 95% CI: 2.84, 3.03), wealth index (IRR = 1.06; 95% CI: 11.04, 1.08), ≥birth order (IRR = 1.04, 95% CI: 1.02, 1.27), distance to health facility (IRR = 1.02, 95% CI: 1.00, 1.03), and health insurance coverage (IRR = 1.08; 95% CI: 1.06, 1.10) had a significant association with the number of tetanus vaccinations among pregnant women.
Conclusions and recommendations: This study concludes that the number of tetanus toxoid vaccinations among pregnant women in low- and middle-income countries is low. In the negative binomial model, the frequency of tetanus vaccinations has a significant association with maternal employment, educational status, wealth index, antenatal care visits, birth order, distance from a health facility, and health insurance. Therefore, the ministries of health in low and middle-income countries should give attention to those women who had no antenatal care visits and women from poor wealth quantiles while designing policies and strategies.
Background
Tetanus is an acute infectious disease caused by spores of the bacterium Clostridium tetani.Citation1–3 Tetanus that develops during pregnancy or within six weeks after pregnancy termination (birth, miscarriage, or abortion) is referred to as maternal tetanus.Citation4 The use of vaccines is an appealing way of preventing infectious diseases such as tetanus, which mostly affects people in countries with low and middle incomes and is a highly fatal illness affecting the central nervous system.Citation5 Through the transfer of maternally-derived pathogen-specific antibodies through the placenta and breast milk, maternal immunization has become a viable technique to lower the morbidity and mortality of pregnant women and their very young babies during the critical early weeks of the infant’s life.Citation6,Citation7
Maternal immunization is a critical strategy to protect both mothers and their newborns from infectious diseases. During pregnancy, antibodies are naturally transferred from the mother to the fetus through the placenta, a process that intensifies in the last trimester. This transfer provides the infant with passive immunity against various pathogens that the mother has antibodies for. After birth, breastfeeding continues to supply the infant with important antibodies, especially immunoglobulin A (IgA), which plays a crucial role in mucosal immunity.Citation8,Citation9
The rationale behind maternal immunization is to boost the mother’s antibody levels against specific pathogens, which can then be passed on to the infant, offering protection during the early stages of life when the infant’s own immune system is still developing.Citation10,Citation11 Maternal immunization might also influence the infant’s immune system development and response to later vaccinations. However, the efficiency of antibody transfer and the duration of the resulting infant protection can vary based on several factors, including the type of antibody, the mother’s health, and the timing of the vaccination during pregnancy.Citation12,Citation13
Pregnant women should receive at least two doses of the tetanus vaccine, according to the dose intervals, to maintain antibody levels above the protective threshold in the event that vaccination proof is absent.Citation14 Although a vaccine that contains tetanus toxoid offers a reliable and secure defense against the disease, the high case-fatality rate of 80–100% among neonates from maternal and neonatal tetanus remains a serious public health concern, and it is an indicator of social inequality.Citation15,Citation16
For pregnant women who have never received tetanus vaccinations, a three-vaccination series containing tetanus and reduced diphtheria toxoids should be initiated. Tetanus toxoid vaccination provides protection against both maternal and neonatal tetanus. For this vaccination series, it is advised to provide tetanus toxoid vaccines at 0 weeks, 4 weeks, and 6–12 months.Citation17 A lack of vaccination during pregnancy is responsible for the majority of tetanus infections, and the tetanus vaccine is thought to be unavailable to 47 million women globally.Citation15 As a result, every year 15,000–30,000 maternal deaths occur due to tetanus infection.Citation18
Globally 38,000 people died due to tetanus in 2017.Citation18 In 2017, Sub-Saharan Africa and South Asia saw the greatest number of new cases of tetanus. Eighty-two percent of tetanus cases worldwide are concentrated in sub-Saharan Africa and South Asia. Similarly, South Asia and Sub-Saharan Africa account for 29,500 of all tetanus deaths, or 77% of total mortality. Sub-Saharan Africa continues to have a higher rate of tetanus cases than any other region in the world.Citation19,Citation20 Immunizing women before birth with at least two doses of tetanus toxoid immunization can reduce nearly 94% of neonatal mortality related to tetanus.Citation21 The World Health Organization recommends 5 consecutive doses of tetanus toxoid vaccination per schedule for lifelong protection against tetanus.Citation22
The studies carried out in different parts of the world revealed that maternal age,Citation21 maternal educational attainment,Citation23 marital status,Citation24 household wealth index,Citation25 distance to health facilities,Citation26 low antenatal care utilization, parity,Citation27 and type of place of residenceCitation28,Citation29 were significantly associated with tetanus immunization before birth.
While the World Health Organization (WHO) implemented maternal immunization, which started in 2016, it recommends systematic immunization of pregnant women and those in the reproductive age range (15–49 years) with a tetanus toxoid-containing vaccine. Additionally, the provision of at least 3 doses of tetanus toxoid to women of reproductive age who reside in areas classified as being at high risk through supplemental immunization activities for maternal and neonatal tetanus remains a public health problem in low and middle-income countries.Citation30,Citation31
Despite low and middle-income countries share the huge burden of global maternal and neonatal morbidity and mortality related to tetanus infection, as far as our search of the literature and knowledge is concerned, there has been no study conducted on the number of tetanus injections before birth and associated factors among pregnant women in low and middle-income countries. Therefore, the present study focuses on investigating the number of tetanus injections before birth and associated factors among pregnant women in low and middle-income countries using the recent Demographic and Health Survey by applying a negative binomial poisson regression model.
Methods
Study setting
Based on the World Bank, the low and middle-income countries are included in Africa (Eastern Africa, Middle Africa, Northern Africa, Southern Africa, and Western Africa), Asia (Central Asia, Eastern Asia, Southeast Asia, Southern Asia, and Western Asia), Europe (Eastern and southern Europe), Latin America and the Caribbean (Caribbean, central America, and south America), and Oceania (Melanesia, Micronesia, and Polynesia).Citation32 A country is considered low-income if its gross national productivity (GNI) per person is $1,135 or less in 2022. Countries with a GNI per capita falling between $1,136 and $4,465 are classified as having lower-middle income. The GNI per capita for upper-middle-income countries ranges from $4,466 to $13,845.Citation33 This study was conducted based on the recent DHS survey data from 60 low and middle income countries such as Afghanistan, Albania, Angola, Armenia, Bangladesh, Burkina Faso, Benin, Burundi, Congo Democratic Republic, Congo, Cote d’Ivoire, Cambodia, Cameroon, Chad, Colombia, Dominican Republic, Egypt, Ethiopia, Gabon, Ghana, Gambia, Guinea, Guatemala, Honduras, Haiti, India, Indonesia, Jordan, Kenya, Comoros, Kyrgyz Republic, Liberia, Lesotho, Madagascar, Mali, Malawi, Mauritania, Myanmar, Maldives, Mozambique, Nigeria, Niger, Namibia, Nepal, Papua New Guinea, Philippines, Pakistan, Rwanda, Sierra Leone, Senegal, Tajikistan, Tanzania, Timor-Leste, Togo, Turkey, Uganda, Yemen, South Africa, Zambia, Zimbabwe.
Study design and period
A negative binomial poisson regression of a cross-sectional study was carried out. A negative binomial regression analysis has been conducted using DHS data from 60 low- and middle-income countries that were surveyed between 2010 and 2022. As a component of the global Demographic and Health Survey, the Demographic and Health Survey (DHS) is a five-year national study that deploys organized, pretested, and validated tools. Twelve years of DHS data, beginning in 2010, were collected in order to obtain a representative sample of recent Demographic and Health Survey data from every region of low- and middle-income countries. The surveys have huge sample sizes, are population-based, and are nationally representative of all countries.
Population and eligibility criteria
All pregnant women who are 15–49 years old in low- and middle-income countries were the source population. The study population was all pregnant women in the selected enumeration areas, which were included in the analysis.
Data source
In order to investigate the number of tetanus injections before birth among pregnant women, the DHS surveys from 60 low- and middle-income countries were appended together. Each country’s survey involves various datasets, such as information on key health indicators like mortality, disease, family planning services, fertility, and maternal and child health services. The Demographic and Health Survey has Household Recode (HR), Individual Recode (IR), Male’s Recode (MR), Couple’s Recode (CR), Children’s Recode (KR), and Birth’s Recode (BR) datasets. For this study, we used the individual record dataset (IR file) to extract the dependent and independent variables for each country, and then we appended the data using STATA version 14. The number of tetanus injections before birth from the individual record (IR) dataset was used as an outcome variable ().
Table 1. Sample size for number of tetanus injections before birth and associated factors among pregnant women in low and middle income countries, DHS 2010–2022.
Sampling procedure
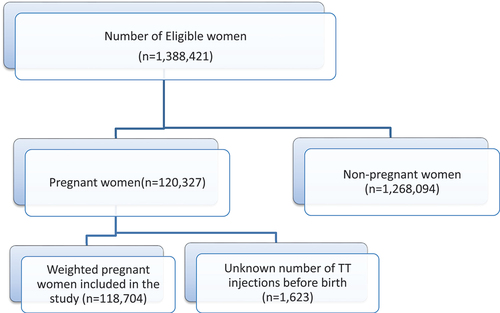
The Demographic and Health Surveys (DHS) program is a comprehensive survey that collects data on population, health, and nutrition in low- and middle-income countries. The DHS program uses a multistage cluster sampling technique to select a representative sample of households from the population of interest. The sampling procedure involves selecting clusters of households from a list of enumeration areas, then selecting households within each cluster using a random sampling technique. First, a proportional allocation of enumeration areas was selected randomly from each stratum, separated by place of residence (rural and urban). In the second phase, households were selected using a systematic sampling technique from the selected enumeration areas. We have used sample weights to adjust for the probability of selection and non-response, which allows for the estimation of population-level indicators. This study included 118,704 weighted pregnant women for analysis ().
Figure 1. Sampling procedure to number of tetanus toxoid injections before birth among pregnant women in low and middle income countries, DHS 2010–2022.
Study variables
Dependent variable: The outcome variable of this study was the number of tetanus toxoid injections before birth, measured as a count of 0.1, 2, 3…
Independent variables: Explanatory variables for this study were selected after a review of relevant literature.Citation34–41 The independent variables were: sex of household head (male, female), Maternal age,Citation15–38–Citation48 maternal educational status (no formal education, primary, secondary, higher), husband educational status (no formal education, primary, secondary, higher), marital status of the mother (unmarried, married, ever married), maternal employment (not working, working), number of antenatal care visits (no visit, 1–3, ≥4), parity (Nullipara, primipara, multipara), birth order (first birth order, second birth order, third or more birth order), wealth index (poor, middle, rich), perception of distance from the health facility (big problem, not big problem), household media exposure (no, yes), planning status of birth (wanted then, wanted later, no more wanted), health care decision making (self, husband, someone else), health insurance coverage (no, yes), facility type for antenatal care (public, private), use of internet (no, yes), residence (urban, rural).
These variables were described within the results into two subtypes: Nominal variables: Categories with no inherent order (e.g., sex of the household head, marital status of the mother, household media exposure). Ordinal variables: categories with a specific order (e.g., maternal age, maternal educational status, husband educational status, wealth index, perception of distance from the health facility, planning status of birth, health care decision-making, health insurance coverage, facility type for antenatal care, residence). Discrete Quantitative Variables: These variables take on specific, distinct values. Examples include the number of antenatal care visits, parity, birth order, and use of the internet.
Data processing and statistical analysis
The data were extracted from recent standard DHS datasets and cleaned, recorded, and analyzed with STATA version 14 statistical software. The data were weighted using sampling weight, primary sampling unit, and strata before any statistical analysis to restore the representativeness of the survey and take into account the sampling design when calculating standard errors to get reliable statistical estimates. We used the weighting variable (v005) as a relative weight normalized to make the analysis survey-specific, while for the pooled data, we denormalized the pregnant women’s individual standard weight variable by dividing the pregnant women’s individual standard weight by the sampling fraction of each country: (pregnant women adjusted weight= v005)× (total pregnant women aged 15–49 years in the country at the time of the survey)/(number of pregnant women aged 15–49 years in the survey).
The number of tetanus toxoid shots received before birth was measured as 0, 1, 2, 3… Which is the count data, and we used count regression models to analyze the data. The standard Poisson regression assumption is broken in our data since the variance is greater than the mean due to unobserved heterogeneity. Because of this, we have employed the most widely used extensions of Poisson regression, which have more parameters than the Poisson distribution for over-dispersed data, including zero-inflated Poisson regression, negative binomial zero-inflated Poisson regression, and negative binomial regression.
In order to account for the unobserved heterogeneity in the count data, the negative binomial model incorporates a dispersion parameter, which addresses the over-dispersion issue. The However, the negative binomial model cannot handle the over dispersion brought by excessive zeros; in this situation, Hurdle models and zero-inflated models are applicable. Over-dispersion is permitted in zero-inflated models because they account for a count component and a point mass at zero.Citation42 Finally, log likelihood ratio, Akaike Information Criterion (AIC), and Bayesian Information Criterion (BIC) were tested to compare the candidate models, so negative binomial regression with the smallest AIC and BIC values and the highest log likelihood was considered the best-fit model for this study. The variables used in the models were verified for multi-collinearity by measuring the variance inflation factors (VIF), with the findings falling within acceptable limits of 1 to 10.
Data management and model building
In order to make appropriate adjustments, the data were weighted using sample weight (v005), primary sampling unit (v023), and strata (v021) after being extracted using STATA/SE statistical software. Descriptive statistics like percentages, bar charts, and frequency tables were used to describe the data. The DHS data showed that women were nested within clusters, and it’s possible that these clusters included similar characteristics. The standard count regression model assumptions of equality of variance and mean were broken. Thus, the heterogeneity between mean and variance must be considered in advanced models. Negative binomial distribution is widely used to model count data when the poisson model does not fit well due to the over dispersion V(Y) > E(Y). Generalization to the domain of y* = 0, 1,…
Where
In this model k is not assumed to be integer-valued and must be estimated via maximum likelihood
Result
Among weighted pregnant women in low- and middle-income countries 38,942 (32.8%) had received two or more doses of tetanus toxoid before giving birth. 39316 (33.1%) of the women do not receive tetanus toxoid injections before birth. The mean and the variance of the number of tetanus toxoid injections before birth are 1.554064 and 1.758891, respectively () and ().
Figure 2. Number of tetanus toxoid injections before birth among pregnant women in low and middle income countries.
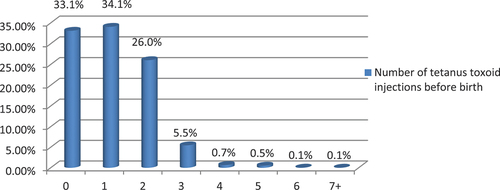
Table 2. Number of tetanus toxoid injections before birth and associated factors among pregnant women in low and middle income countries, DHS 2010–2022.
Model comparison
Poisson regression, negative binomial regression, zero-inflated Poisson regression, and zero-inflated negative binomial were tested to select a model for analysis. The negative binomial regression model has the highest log likelihood test (−74029.809) compared to Poisson regression, negative binomial regression, and zero-inflated negative binomial regression. The alpha test (<0.001) indicates that there is a statistical difference between Poisson regression and negative binomial regression. In addition, the minimum AIC and BIC values were observed for the negative binomial model, followed by Poisson regression, zero-inflated Poisson, and zero-inflated negative binomial models. Furthermore, the vuong test for zero-inflated Poisson regression is statistically insignificant, which indicates zip is an inappropriate model for this study ().
Table 3. Models comparison for number of tetanus injections before birth and associated factors among pregnant women in low and middle income countries, DHS 2010–2022.
A total of 118,704 pregnant women within five years of the survey were included. The median age of women was 26 years, with an interquartile range (IQR) of 21–32 years. Nearly one-third (32.8%) of the pregnant women were between the ages of 35 and 49. A quarter of pregnant women (25.9%) in low- and middle-income countries had no formal education. Nearly half (46.2%) of pregnant women were from poor households, and about 69.1% were from rural residences. About 43.3% of pregnant women perceived distance to health institutions as the biggest problem in accessing health care facilities ().
Table 4. Number of tetanus injections before birth and socio-demographic and economic characteristics of pregnant women in low and middle income countries, DHS 2010–2022.
Factors associated with the number of tetanus injections before birth among pregnant women in low and middle income countries
In the negative binomial model, maternal educational status, maternal employment, antenatal care visits, household wealth index, birth order, distance from a health facility, and health insurance coverage show a significant association with the frequency of tetanus injections before birth.
The number of tetanus injections before birth was 1.22 (IRR = 1.22, 95% CI: 1.17, 1.26), 1.19 (IRR = 1.19, 95% CI: 1.15, 1.23), and 1.16 (IRR = 1.16, 95% CI: 1.12, 1.20) times more among pregnant women with primary, secondary, and above educational levels than pregnant women who had no formal education, respectively. The number of tetanus injections before birth was 1.11 (IRR = 1.11, 95% CI: 1.09, 1.13) times higher among pregnant women who were employed compared to unemployed pregnant women. The number of tetanus injections before birth was 2.49 (IRR = 2.49, 95% CI: 2.41, 2.57) and 2.94 (IRR = 2.94, 95% CI: 2.84, 3.03) times higher among pregnant women who had one or more ANC follow-ups than women who had no ANC visits. Pregnant women with a rich household wealth index (IRR = 1.06; 95% CI: 11.04, 1.08) had a significantly high frequency of tetanus injections before birth. The frequency of tetanus injections before birth was 1.04 (IRR = 1.04, 95% CI: 1.02, 1.27) times higher among pregnant women whose birth orders were three and more compared to pregnant women who had only one birth order.
The number of tetanus injections before birth was 1.02 (IRR = 1.02, 95% CI: 1.00, 1.03) times more among pregnant women whose distance to health facilities is not a big problem compared to their counterparts. Pregnant women who had health insurance coverage (IRR = 1.08; 95% CI: 1.06, 1.10) had a higher number of tetanus toxoid vaccinations than pregnant women who did not have it ().
Table 5. Negative binomial fitted model for number of tetanus injections before birth and socio-demographic and economic characteristics of pregnant women in low and middle income countries, DHS 2010–2022.
Discussion
This study used negative binomial Poisson regression to determine the factors associated with the frequency of tetanus injections given before birth in low- and middle-income countries. During their current pregnancy, 26.0% of pregnant women in low- and middle-income countries receive tetanus toxoid injections at least twice. The finding is lower compared to the studies conducted in Sierra Leone, 82.1%,Citation38 Africa, 62%,Citation30 Turkey, 27.8%,Citation43 and Brazil, 59.2%.Citation44 This could be related to differences in healthcare delivery systems, access to vaccinations at healthcare facilities, levels of vaccination awareness and information, the prevalence of diseases that can be prevented by vaccination, the available political environment, and methodological variations in the assessment of vaccination status. This finding indicates that greater effort is needed in low- and middle-income countries to ensure that pregnant women receive at least two doses of the tetanus toxoid vaccine. The other explanation could be that vaccine hesitancy among pregnant women can be the cause of the lower tetanus toxoid vaccination. Belief in vaccine-induced harm: pregnant women who believe there is potential for vaccine-induced harm are less likely to get vaccinated. Vaccine hesitancy varies across demographic, political, age, geographical, and socioeconomic groups. Understanding these concerns is crucial for individualized approaches to patient education and vaccine promotion.Citation45–47
The number of tetanus injections before birth was 1.22, 1.19, and 1.16 times higher among pregnant women with primary, secondary, and higher educational levels than pregnant women with no formal education, respectively. This finding is in line with the studies conducted in Ethiopia,Citation36–48–Citation50 Ivory Coast,Citation39 Egypt,Citation51 Nigeria,Citation52 and Bangladesh.Citation53 This could be attributed to women with education having simple access to information and knowledge of the immunization program. Women’s independence will probably increase as a result of education, giving them more confidence and the capacity to make decisions about their own immunization during pregnancy.
The results of the study also showed a significant association between the women’s employment and their use of the tetanus toxoid vaccine. The number of tetanus injections before birth was 1.11 times higher among pregnant women who were employed compared to unemployed pregnant women. This finding is in line with the studies conducted in Ethiopia,Citation54 Kenya,Citation26 Nigeria,Citation52 Brazil,Citation55 and the United Kingdom.Citation56 The possible explanation could be that working women’s incomes could have given them the purchasing ability to pay for their health care, even if it wasn’t free at all or wasn’t covered by insurance, as well as for their transportation to the institution.Citation54 Furthermore, the majority of women in employment have positions that require them to interact socially with others in a certain way. Such communications could establish an environment for awareness and engagement in health-related discussions, especially when a woman is pregnant. Therefore, the workplace may serve as a place of social support and motivation, increasing the use of health care services.Citation26
The number of tetanus injections before birth was 2.49 and 2.94 times higher among pregnant women who had one and more ANC follow-ups than women who had no antenatal care visits, respectively. This was consistent with studies reported in Kenya,Citation26 Sierra Leone,Citation38 Ghana,Citation57 Mali,Citation58 Malawi,Citation59 Pakistan,Citation40 and Turkey.Citation60 This could be because regular contact with healthcare providers actively maintains and increases awareness of the advantages of using the complete tetanus toxoid vaccine. Attending antenatal care services increases the likelihood that women have received education regarding the value of the tetanus toxoid vaccine in preventing tetanus in both themselves and their unborn child. Additionally, as the tetanus toxoid vaccine is part of antenatal care services, healthcare providers make sure that pregnant women receive the immunization.Citation61,Citation62
In this study, the household wealth index and the use of the tetanus toxoid vaccination were significantly associated. Pregnant women who reside in rich household wealth indexes had a significantly higher frequency of tetanus vaccine utilization. This was consistent with studies reported in developing African and Asian countries,Citation63 Kenya,Citation26 South Africa,Citation64 Alexandra,Citation65 and India.Citation21 The explanation could be that pregnant women from affluent households would be able to afford the costs of health care, including those of preventive measures like getting a vaccination against tetanus.Citation49,Citation54,Citation66 The other explanation for this could be that women from lower-income families experienced disadvantages and found it challenging to acquire the tetanus toxoid vaccination due to the high expenses and time required to maintain their daily lives.
The frequency of tetanus injections before birth was 1.04 times higher among pregnant women whose birth orders were three and more compared to pregnant women who had only one birth order. This finding is contrary to the studies conducted in Zimbabwe,Citation67 Pakistan,Citation68 and Carolina University.Citation69 This may be because women with three or more birth orders are more likely to seek health care when necessary because they have more experience with pregnancy and childbirth; additionally, these women may have established relationships with healthcare providers that facilitate better interaction and more effective care.
The number of tetanus injections before birth was 1.02 times higher among pregnant women whose distance to health facilities is not a big problem compared to their counterparts. It is in line with study findings in Peshawar,Citation24 Zimbabwe,Citation70 Tanzania,Citation71 and Pakistan.Citation72 This can be the result of the time and money spent traveling to and from far-off immunization centers. In addition, women are typically preoccupied at home since they have a lot of responsibilities at home, including taking care of the elderly and children, in addition to other household responsibilities. As a result, women frequently hesitate to travel to immunization centers because they are quite far from their houses. Furthermore, if vaccination centers are located far from one another, the TT vaccination may cause fatigue in women and their children since it requires multiple trips to healthcare facilities for the complete immunization.Citation50
Health insurance coverage was significantly associated with the frequency of the tetanus toxoid vaccination. Pregnant women who had health insurance coverage had a higher number of tetanus injections before birth than pregnant women who did not. This finding is consistent with previous studies in Georgia.Citation73 Because women who have health insurance are probably going to have frequent antenatal care follow-ups, essentially, reducing the financial barriers to ANC is meant to boost the utilization of ANC follow-up.
The study’s strength was the utilization of recently conducted large-sample national demography and health surveys from 60 low- and middle-income countries. In addition, this study used negative binomial poisson regression to determine factors that could not be determined using classical poisson regression. However, the study was limited in its ability to include other variables that might have been associated with the outcome variables due to a lack of some important variables in the DHS dataset, such as maternal psychological factors.
Conclusions and recommendations
This study concludes that the number of tetanus toxoid vaccinations among pregnant women in low- and middle-income countries is low. In the negative binomial model, the frequency of tetanus vaccinations has a significant association with maternal employment, educational status, household wealth index, ANC visits, birth order, distance from a health facility, and health insurance coverage. Therefore, the ministries of health in low and middle-income countries should give attention to those women who had no ANC visits and women from poor wealth quantiles while designing policies and strategies targeting reducing stillbirth rates. By addressing these areas, health ministries can work toward increasing the number of tetanus toxoid vaccinations among pregnant women, which is crucial for reducing stillbirth rates related to tetanus and improving maternal and child health outcomes. Future researchers should conduct longitudinal studies to track the effectiveness of policies and interventions over time. Moreover, the upcoming researchers should conduct research to understand the barriers to vaccination for women with no ANC visits and those from poorer wealth quantiles.
Ethical approval and consent to participate
This study is a secondary analysis of the DHS data, so it does not require ethical approval. For conducting our study, we registered and requested the dataset from the DHS online archive and received approval to access and download the data files. According to the DHS report, all participant data was anonymized during the collection of the survey data. Visit http://www.dhsprogram.com. for more information about DHS data and ethical standards.
Author’s contributions
AFZ: involved in conceptualization, data curation, formal analysis, investigation, methodology, resources, software, supervision, validation, visualization, writing original draft
TTT and EGM: involved in data curation, project administration, and formal analysis
SST: involved in investigation, and methodology
MSA, ATG, and MAT: involved in conceptualization, data curation, formal
MW, ATK, MAA, YAW, BT: involved in data curation, writing original draft, review and editing
BSW: involved in conceptualization, data curation, and formal analysis.
Acknowledgments
We are grateful to the DHS programs for letting us use the relevant EDHS data in this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The most recent data from the Demographic and Health Survey were used in this study, and it is publicly available online at (https://www.dhsprogram.com).
Additional information
Funding
References
- World Health Organization (WHO) global health achievements 2023.
- WHO. Protecting all against tetanus: guide to sustaining maternal and neonatal tetanus elimination (MNTE) and broadening tetanus protection for all populations; 2019.
- Farnworth E, Roberts A, Rangaraj A, Minhas U, Holloway S, Harding K. Tetanus in patients with chronic wounds–are we aware? Int Wound J. 2012;9(1):93–11. doi:10.1111/j.1742-481X.2011.00850.x.
- Organization WH. Surveillance standards for vaccine-preventable diseases; 2018.
- Organization WH. Weekly epidemiological record: tetanus vaccines. Switzerland; 2017.
- Raya BA, Srugo I, Kessel A, Peterman M, Bader D, Peri R, Ashtamker N, Gonen R, Bamberger E. The induction of breast milk pertussis specific antibodies following gestational tetanus–diphtheria–acellular pertussis vaccination. Vaccine. 2014;32(43):5632–7. doi:10.1016/j.vaccine.2014.08.006.
- Halperin B, Morris A, Mackinnon-Cameron D, Mutch J, Langley J, McNeil S, MacDougall D, Halperin SA. Kinetics of the antibody response to tetanus-diphtheria-acellular pertussis vaccine in women of childbearing age and postpartum women. Clin Infect Dis. 2011;53(9):885–92. doi:10.1093/cid/cir538.
- Saso A, Kampmann B. Maternal immunization: nature meets nurture. Front Microbiol. 2020;11:531598. doi:10.3389/fmicb.2020.01499.
- Atyeo C, Alter G. The multifaceted roles of breast milk antibodies. Cell. 2021;184(6):1486–99. doi:10.1016/j.cell.2021.02.031.
- Erdogan RR, Dolatshahi S. Quantitative mechanistic model reveals key determinants of placental IgG transfer and informs prenatal immunization strategies. bioRxiv 2023;19(11):e1011109.
- Albrecht M, Arck PC. Vertically transferred immunity in neonates: mothers, mechanisms and mediators. Front Immunol. 2020;11:526432. doi:10.3389/fimmu.2020.00555.
- Coakley CM, Staszewski V, Herborn KA, Cunningham EJ. Factors affecting the levels of protection transferred from mother to offspring following immune challenge. Front Zool. 2014;11(1):1–11. doi:10.1186/1742-9994-11-46.
- Stelzer IA, Urbschat C, Schepanski S, Thiele K, Triviai I, Wieczorek A, Alawi M, Ohnezeit D, Kottlau J, Huang J. et al. Vertically transferred maternal immune cells promote neonatal immunity against early life infections. Nat Commun. 2021;12(1):4706. doi:10.1038/s41467-021-24719-z.
- Yusuf N, Steinglass R, Gasse F, Raza A, Ahmed B, Blanc DC, Yakubu A, Gregory C, Tohme RA. Sustaining Maternal and Neonatal Tetanus Elimination (MNTE) in countries that have been validated for elimination–progress and challenges. BMC Public Health. 2022;22(1):1–12. doi:10.1186/s12889-022-13110-2.
- Njuguna HN, Yusuf N, Raza AA, Ahmed B, Tohme RA. Progress toward maternal and neonatal tetanus elimination—worldwide, 2000–2018. MMWR Morb Mortal Wkly Rep. 2020;69(17):515. doi:10.15585/mmwr.mm6917a2.
- Moniz MH, Beigi RH. Maternal immunization: clinical experiences, challenges, and opportunities in vaccine acceptance. Hum Vaccines Immunother. 2014;10(9):2562–70. doi:10.4161/21645515.2014.970901.
- World Health Organization. (WHO)-maternal and neonatal tetanus elimination (Mnte)/the strategies. 2019. https://www.who.int/initiatives/maternal-and-neonatal-tetanus-elimination-%28mnte%29/the-strategies.
- WHO U. World Bank. State of the world’s vaccines and immunization. Geneva: World Health Organization; 2009. 2017.
- Akwataghibe NN, Ogunsola EA, Broerse JE, Popoola OA, Agbo AI, Dieleman MA. Exploring factors influencing immunization utilization in Nigeria—a mixed methods study. Front Public Health. 2019;7:392. doi:10.3389/fpubh.2019.00392.
- Mengesha MB, Weldegeorges DA, Assefa NE, Gebremeskel SG, Hidru HD, Teame H, Hailesilassie Y. Tetanus toxoid immunization status and associated factors among mothers in Hawzen, eastern zone of Tigray, Ethiopia, 2019. Open Public Health J. 2020;13(1):281–8. doi:10.2174/1874944502013010281.
- Khan REA, Raza MA. Maternal health-care in India: the case of tetanus toxoid vaccination. Asian Dev Policy Rev. 2013;1(1):1–14. doi:10.18488/journal.107.2013.11.1.14.
- Organization WH. Weekly Epidemiological Record, 1928, vol. 03, 126 [full issue]. Weekly Epidemiological Record = relevé épidémiologique hebdomadaire. Organi WH. Weekly Epidem Rec. 1928;3(126):1–5.
- Singh A, Pallikadavath S, Ogollah R, Stones W, Crowcroft NS. Maternal tetanus toxoid vaccination and neonatal mortality in rural north India. PLOS ONE. 2012;7(11):e48891. doi:10.1371/journal.pone.0048891.
- Naeem M, Khan M-U-I, Abbas SH, Adil M, Khan A, Naz SM, Khan MU. Coverage and factors associated with tetanus toxoid vaccination among married women of reproductive age: a cross sectional study in Peshawar. J Ayub Med Coll Abbottabad. 2010;22(3):136–40.
- Hashmi FK, Islam M, Khan TA, Tipu MK. Vaccination coverage of mothers during pregnancy with tetanus toxoid and infants after birth. Pakistan J Pharm. 2011;24:1–3.
- Haile ZT, Chertok IRA, Teweldeberhan AK. Determinants of utilization of sufficient tetanus toxoid immunization during pregnancy: evidence from the Kenya demographic and health survey, 2008–2009. J Community Health. 2013;38(3):492–9. doi:10.1007/s10900-012-9638-9.
- Masuno K, Xaysomphoo D, Phengsavanh A, Douangmala S, Kuroiwa C. Scaling up interventions to eliminate neonatal tetanus: factors associated with the coverage of tetanus toxoid and clean deliveries among women in Vientiane, Lao PDR. Vaccine. 2009;27(32):4284–8. doi:10.1016/j.vaccine.2009.05.024.
- Tesfahun F, Worku W, Mazengiya F, Kifle M. Knowledge, perception and utilization of postnatal care of mothers in Gondar Zuria District, Ethiopia: a cross-sectional study. Matern Child Health J. 2014;18(10):2341–51. doi:10.1007/s10995-014-1474-3.
- Abdella A. Maternal mortality trend in Ethiopia. Ethiop J Health Dev. 2010;24(1). doi:10.4314/ejhd.v24i1.62953.
- Messeret ES, Masresha B, Yakubu A, Daniel F, R M, Nshimirimana D, Okeibunor J, Akanmori B. Maternal and neonatal tetanus elimination (MNTE) in the WHO African region. J Immunological Sci. 2018;2(SI1):103. doi:10.29245/2578-3009/2018/si.1115.
- Giles M, Mantel C, Muñoz F, Moran A, Roos N, Yusuf N, Diaz T, Ahun M, Nic Lochlainn LM, Wootton E. et al. Vaccine implementation factors affecting maternal tetanus immunization in low- and middle-income countries: results of the maternal immunization and Antenatal Care Situational Analysis (MIACSA) project. Vaccine. 2020;38(33):5268–77. doi:10.1016/j.vaccine.2020.05.084.
- Hamadeh N, Van Rompaey C, Metreau E. World Bank Group country classifications by income level for FY24 (July 1, 2023–June 30, 2024). New Hampshire, United States: The World Bank Group; 2023.
- World Bank Country and Lending Groups. 2023. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
- Olaniyan A, Isiguzo C, Hawk M. The socioecological model as a framework for exploring factors influencing childhood immunization uptake in Lagos state, Nigeria. BMC Public Health. 2021;21(1):867. doi:10.1186/s12889-021-10922-6.
- Muluken Dubale Mamoro MDM, Lolemo Kelbiso Hanfore LKH. Tetanus toxoid immunization status and associated factors among mothers in Damboya Woreda, Kembata Tembaro Zone. Ethiopia: SNNP; 2018.
- Gebremedhin TS, Welay FT, Mengesha MB, Assefa NE, Werid WM. Tetanus toxoid vaccination uptake and associated factors among mothers who gave birth in the last 12 months in Errer District, Somali regional state, eastern Ethiopia. Biomed Res Int. 2020;2020:1–8. doi:10.1155/2020/4023031.
- Awosan K, Hassan M. Perception and utilization of tetanus toxoid immunization among pregnant women attending a tertiary centre in North-West Nigeria. J Drug Delivery Ther. 2018;8(6):119–24. doi:10.22270/jddt.v8i6.2032.
- Yaya S, Kota K, Buh A, Bishwajit G. Prevalence and predictors of taking tetanus toxoid vaccine in pregnancy: a cross-sectional study of 8,722 women in Sierra Leone. BMC Public Health. 2020;20(1):1–9. doi:10.1186/s12889-020-08985-y.
- Yaya S, Kota K, Buh A, Bishwajit G. Antenatal visits are positively associated with uptake of tetanus toxoid and intermittent preventive treatment in pregnancy in Ivory Coast. BMC Public Health. 2019;19(1):1–12. doi:10.1186/s12889-019-7847-1.
- Iqbal S, Ali I, Ekmekcioglu C, Kundi M. Increasing frequency of antenatal care visits may improve tetanus toxoid vaccination coverage in pregnant women in Pakistan. Hum Vaccines Immunother. 2020;16(7):1529–32. doi:10.1080/21645515.2019.1705693.
- Gabriel-Job N, Ide LY. Tetanus toxoid status and determinants of uptake among women in Etche local government area, Rivers State, Nigeria: a community based study. AJMAH. 2020;17(4):1–7. doi:10.9734/ajmah/2019/v17i430171.
- McCullagh P. Generalized linear models. New York: Routledge; 2019.
- Maral I, Baykan Z, Aksakal F, Kayikcioglu F, Bumin M. Tetanus immunization in pregnant women: evaluation of maternal tetanus vaccination status and factors affecting rate of vaccination coverage. Public Health. 2001;115(5):359–64. doi:10.1016/S0033-3506(01)00476-0.
- Faria APV, da Silva TPR, Vieira EWR, Lachtim SAF, Rezende EM, Matozinhos FP. Factors associated with tetanus vaccination in pregnant women living in Minas Gerais State, Brazil: a cross-sectional study. Public Health Pract (Oxf). 2021;2:100203. doi:10.1016/j.puhip.2021.100203.
- Kilich E, Dada S, Francis MR, Tazare J, Chico RM, Paterson P, Larson HJ. Factors that influence vaccination decision-making among pregnant women: a systematic review and meta-analysis. PLOS ONE. 2020;15(7):e0234827. doi:10.1371/journal.pone.0234827.
- Gianfredi V, Berti A, Stefanizzi P, D’Amico M, De Lorenzo V, Moscara L, Di Lorenzo A, Venerito V, Castaldi S. COVID-19 vaccine knowledge, attitude, acceptance and hesitancy among pregnancy and breastfeeding: systematic review of hospital-based studies. Nato Adv Sci Inst Se. 2023;11(11):1697. doi:10.3390/vaccines11111697.
- Hsu AL, Johnson T, Phillips L, Nelson TB. editors. Sources of vaccine hesitancy: pregnancy, infertility, minority concerns, and general skepticism. In Open forum infectious diseases. New York: Oxford University Press US; 2022.
- Fenta SM, Fenta HM. Magnitude of tetanus toxoid immunization and associated factors among pregnant women in Ethiopia. Open Public Health J. 2023;16(1). doi:10.2174/18749445-v16-e230111-2022-161.
- Dubale Mamoro M, Kelbiso Hanfore L. Tetanus toxoid immunization status and associated factors among mothers in Damboya Woreda, Kembata Tembaro zone, SNNP, Ethiopia. J Nutr Metab. 2018;2018:1–9. doi:10.1155/2018/2839579.
- Anatea MD, Mekonnen TH, Dachew BA. Determinants and perceptions of the utilization of tetanus toxoid immunization among reproductive-age women in Dukem Town, Eastern Ethiopia: a community-based cross-sectional study. BMC Int Health Hum Rights. 2018;18(1):1–0. doi:10.1186/s12914-018-0168-0.
- Hassan AM, Shoman AE, Abo-Elezz NF, Amer MM. Tetanus vaccination status and its associated factors among women attending a primary healthcare center in Cairo Governorate, Egypt. J Egypt Public Health Assoc. 2016;91(3):127–34. doi:10.1097/01.EPX.0000491267.30015.2a.
- Gabriel-Job N, Yaguo E, Ide L. Tetanus toxoid status and determinants of uptake among women in Etche local government area, Rivers State, Nigeria: a community based study. Asian J Med Health. 2020;17(4):1–7. doi:10.9734/ajmah/2019/v17i430171.
- Amin MB, Roy N, Meem AE, Hossain E, Aktarujjaman M, Antonello VS. Trends and determinants of taking tetanus toxoid vaccine among women during last pregnancy in Bangladesh: country representative survey from 2006–2019. PLOS ONE. 2022;17(10):e0276417. doi:10.1371/journal.pone.0276417.
- Liyew AM, Ayalew HG. Individual and community-level determinants of poor tetanus toxoid immunization among pregnant women in Ethiopia using data from 2016 Ethiopian demographic and health survey; multilevel analysis. Arch Belg. 2021;79(1):1–0. doi:10.1186/s13690-021-00622-3.
- Faria A, da Silva T, Duarte C, Mendes L, Santos F, Matozinhos F. Tetanus vaccination in pregnant women: a systematic review and meta-analysis of the global literature. Public Health. 2021;196:43–51. doi:10.1016/j.puhe.2021.04.019.
- Wilson RJ, Paterson P, Jarrett C, Larson HJ. Understanding factors influencing vaccination acceptance during pregnancy globally: a literature review. Vaccine. 2015;33(47):6420–9. doi:10.1016/j.vaccine.2015.08.046.
- Owusu-Boateng I, Anto F. Intermittent preventive treatment of malaria in pregnancy: a cross-sectional survey to assess uptake of the new sulfadoxine–pyrimethamine five dose policy in Ghana. Malar J. 2017;16(1):1–9. doi:10.1186/s12936-017-1969-7.
- Hill J, Kayentao K, Touré M, Diarwara S, Bruce J, Smedley J, Doumbo OK, ter Kuile FO, Webster J. Effectiveness of antenatal clinics to deliver intermittent preventive treatment and insecticide treated nets for the control of malaria in pregnancy in Mali: a household survey. PLOS ONE. 2014;9(3):e92102. doi:10.1371/journal.pone.0092102.
- Azizi SC, Chongwe G, Chipukuma H, Jacobs C, Zgambo J, Michelo C. Uptake of intermittent preventive treatment for malaria during pregnancy with sulphadoxine-pyrimethamine (IPTp-SP) among postpartum women in Zomba District, Malawi: a cross-sectional study. BMC Pregnancy Childbirth. 2018;18(1):1–13. doi:10.1186/s12884-018-1744-y.
- İnakçı Hİ, Şimsek Z, Koruk İ, Koruk ST. Coverage of tetanus vaccine after national tetanus vaccination campaign and basic determinants in Şanliurfa. Turk Silahli Kuvvetleri Koruyucu Hekim Bul. 2009;8(6).
- Barrow A, Barrow S, Jobe A. Differentials in prevalence and correlates on uptake of tetanus toxoid and intermittent preventive treatment with sulfadoxine-pyrimethamine during pregnancy: a community-based cross-sectional study in the Gambia. SAGE Open Med. 2022;10:20503121211065908. doi:10.1177/20503121211065908.
- Nigussie J, Girma B, Molla A, Mareg M. Tetanus toxoid vaccination coverage and associated factors among childbearing women in Ethiopia: a systematic review and meta-analysis. Biomed Res Int. 2021;2021:1–0. doi:10.1155/2021/5529315.
- Pathirana J, Nkambule J, Black S. Determinants of maternal immunization in developing countries. Vaccine. 2015;33(26):2971–7. doi:10.1016/j.vaccine.2015.04.070.
- van der Hoeven M, Kruger A, Greeff M. Differences in health care seeking behaviour between rural and urban communities in South Africa. Int J Equity Health. 2012;11(1):1–9. doi:10.1186/1475-9276-11-31.
- Mehanna A, Ali MH, Kharboush I. Knowledge and health beliefs of reproductive-age women in Alexandria about tetanus toxoid immunization. J Egypt Public Health Assoc. 2020;95(1):1–11. doi:10.1186/s42506-020-00049-8.
- Mohamed SOO, Ahmed EM. Prevalence and determinants of antenatal tetanus vaccination in Sudan: a cross-sectional analysis of the multiple indicator cluster survey. Trop Med Health. 2022;50(1):1–6. doi:10.1186/s41182-022-00398-4.
- Mukungwa T. Factors associated with full immunization coverage amongst children aged 12–23 months in Zimbabwe. African Population Studies. 2015;29(2). doi:10.11564/29-2-745.
- Hasnain S, Sheikh N. Causes of low tetanus toxoid vaccination coverage in pregnant women in Lahore district, Pakistan. EMHJ-Eastern Mediterranean Health Journal. 2007;13(5):1142–52. doi:10.26719/2007.13.5.1142.
- Hulsey TM, Laken M, Miller V, Ager J. The influence of attitudes about unintended pregnancy on use of prenatal and postpartum care. J Perinatol. 2000;20(8):513–9. doi:10.1038/sj.jp.7200455.
- Kachimba J. Factors contributing to low tetanus toxoid immunization coverage among women of child bearing age in Luanshya district; 2014.
- Asia Hemed K, Sweetness Naftal L, Perry M C, Zuhura L, Nateiya M Y, Neema Allen NA, Irene H, Blandina Theophil M, Agnes Cyril M. A qualitative study on perspectives of pregnant and postnatal mothers on accessing tetanus Toxoid vaccine in Hai District Kilimanjaro region Tanzania. J Gynecol Res Obstet. 2021;7(3):042–9. doi:10.17352/jgro.000104.
- Usman HR, Kristensen S, Rahbar MH, Vermund SH, Habib F, Chamot E. Determinants of third dose of diphtheria–tetanus–pertussis (DTP) completion among children who received DTP1 at rural immunization centres in Pakistan: a cohort study. Tropical Medicine & International Health: TM & IH. 2010;15(1):140. doi:10.1111/j.1365-3156.2009.02432.x.
- P-J L, O’Halloran A, Williams WW. Impact of health insurance status on vaccination coverage among adult populations. Am J Prev Med. 2015;48(6):647–61. doi:10.1016/j.amepre.2014.12.008.