
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Introduction: Susceptibility to amyotrophic lateral sclerosis (ALS) is associated with smoking in some studies, but it is not clear which aspect of smoking behavior is related. Using detailed records of lifetime smoking we investigated the relationship between smoking and ALS in a UK population. Methods: In this retrospective case-control study, smoking status was collected using environmental questionnaires from people diagnosed with ALS between 2008 and 2013 and from age, sex and geographically matched controls. Categorical measures of smoking behavior were: smoking at the time of survey and smoking initiation; continuous measures were intensity (cigarettes per day), duration (years from starting to stopping or time of survey), cigarette pack years, and comprehensive smoking index (CSI), a measure of lifetime smoking. We used logistic regression to assess the risk of ALS with different combinations of smoking variables adjusted for age at survey, gender, level of education, smoking status and alcohol initiation, selecting the best model using the Akaike Information Criterion. Results: There were 388 records with full smoking history. The best-fitting model used CSI and smoking status at the time of survey. We found a weak association between current smoking and risk of ALS, OR 3.63 (95% CI 1.02–13.9) p value 0.05. Increase in CSI score did not increase risk of ALS: OR 0.81 (95% CI 0.58–1.11) p value 0.2.Conclusion: There is weak evidence of a positive effect of current smoking on the risk of ALS which does not show dose-dependence with higher levels of lifetime smoking and maybe a false positive result.
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease characterized by progressive death of motor neurons leading to relentlessly worsening weakness and death, usually from respiratory failure due to involvement of the diaphragm, 2–3 years after diagnosis (Citation1,Citation2) Although there is an evident genetic component, heritability studies indicate that environmental (and probably stochastic) factors also contribute (Citation3–6).
There is evidence from multiple studies that smoking is associated with ALS, but no agreement over which aspect of smoking behavior is related to ALS (Citation7–14). Despite an evidence-based literature review that concluded that smoking can be considered a risk factor for ALS, it remains unclear if there is a dose-response effect, or what the biological mechanism might be (Citation15). In addition, confounding cannot be discounted, since ALS is also associated with military service, education and socioeconomic status, which are also associated with smoking status (Citation16,Citation17). It is biologically plausible that smoking could be a risk factor through oxidative stress or exposure to potentially neurotoxic chemicals, and so it remains an attractive candidate for studies of environmental etiology (Citation18,Citation19).
The comprehensive smoking index (CSI) estimates lifetime smoking by combining duration, intensity and time since cessation into a score allowing all factors to be considered while avoiding issues of multicollinearity between smoking exposure variables (Citation20). CSI has not previously been used to investigate the role of smoking in ALS risk.
We, therefore, analyzed retrospective case-control data to determine whether smoking is related to ALS in a UK population, investigating the relationship between different smoking variables including CSI and other regularly used measures, and risk of ALS.
Methods
Case-control study design
The data were obtained from the Motor Neurone Disease Association of England, Wales and Northern Ireland (MNDA) Collections collected as part of the MNDA Epidemiology Study, REC reference 07/MRE01/57. People diagnosed with definite, probable or possible ALS according to the El Escorial criteria between 2008 and 2013 were included (Citation21). Three tertiary centers in London, Sheffield, and Birmingham acted as data collection hubs but people with ALS were recruited at secondary centers such as district general hospitals, therefore these are incident cases representative of the ALS population. General practitioners from the general practice of the person with ALS were asked to invite 10 healthy controls to participate in the study via post. The research team matched people on age (within 5 years of the person with ALS) and gender in a 1:1 ratio. Four hundred and thirteen participants provided informed consent, 405 undertook a telephone interview about their lifestyle including smoking undertaken by a trained nurse. Three participants gave no information on smoking behavior.
Definition of smoking status
Categorical measures were: smoking at the time of survey (current, former, never), smoking initiation (ever, never).
To define former smokers we used logistic regression modeling to compare ALS risk between current smokers and ex-smokers, using never smokers as a reference. Few people had recently quit (n = 3 within one year of survey) so we grouped ex-smokers into 5-year time since cessation intervals up to 20 years which was aggregated to 20+. ALS risk reduced from an odds ratio of 2.02–0.79 for current smokers compared to people who had quit within 5 years so former smokers were defined as having given up at least a day before the survey.
Continuous measures included: intensity (cigarettes per day), duration of smoking (years from starting to stopping or time of survey), pack years (intensity × duration), and CSI. The CSI is a non-linear model of smoking exposure that combines duration of smoking, time since cessation and smoking intensity into a continuous score which can be used in a regression model representing lifetime smoking (Citation20). The model involves the simulation of tau and delta from the dataset. Delta, or half-life, reflects the exponential decay in the effect of smoking on health outcomes during a lifetime. Tau, or lag-time, reflects that smokers may be at a higher risk of disease immediately after quitting due to reverse causality. The equations for CSI are as follows:
tsc: time since cessation; δ: lag time; tss: time started smoking; dur: duration of smoking (calculated as age-tss for people currently smoking or [age-tsc]-tss for former smokers); τ: half-life; int: cigarettes per day.
Logistic regression
Data were analyzed using R (Citation22). Continuous demographic characteristics were compared by Student’s t-test or Mann-Whitney U test. Categorical variables were compared by chi-squared or Fisher’s exact test. The primary outcome, whether smoking increases the risk of ALS, was analyzed using logistic regression with maximum likelihood estimation. We generated eight models with combinations of one categorical and one continuous measure of smoking, comparing the Akaike Information Criterion (AIC) of the models to assess fit (Citation23). Odds ratios were adjusted for age, educational attainment, gender, and alcohol consumption.
Assuming an odds ratio of 1.8, a 20% smoking rate in the control population and alpha of 0.05, we had 71% power with a sample size of 400 cases and controls in a 1:1 ratio.
Results
There were 202 cases and 200 control records available for analysis. The two groups were similar except for educational attainment and alcohol status. The details are shown in .
Table 1 Unadjusted comparisons of demographics and behavior in ALS cases and controls.
The optimal CSI variables were tau = 2 and delta = 3.6. There were no differences between groups in unadjusted smoking behaviors, as shown in .
Table 2 Smoking variables and crude comparisons.
Three hundred eighty-eight records had full smoking history available for logistic regression analysis. gives the results of the best fitting logistic regression model which included the CSI and smoking status at time of survey with AIC 543.77. The highest AIC, representing the worst fitting model, was for smoking initiation and number of cigarettes per day at 553.23. An increase in the value of CSI did not increase the risk of ALS: OR 0.81 (95% CI 0.57–1.11) p value 0.2. Current smoking increased the risk of ALS, OR 3.62 (95% CI 1.02–13.9) p value = 0.05, a Bonferroni correction shows that this is likely a false positive result because of multiple testing.
Figure 1 (a) Density plot of CSI value by case control status. (b) Box plot of CSI value by smoking status at time of survey, points colored by case control status. Both graphs are in ever smokers only.
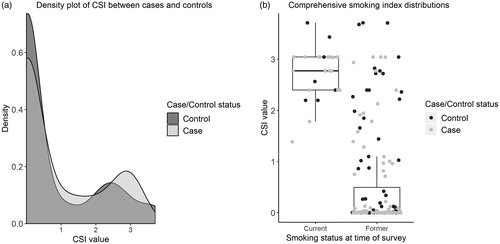
Table 3 Best fitting logistic regression model for smoking and risk of ALS.
Discussion
We found a weak association between current smoking and risk of ALS using traditional epidemiology methods to explore association. We report an uncorrected p-value of 0.05, and several models tested for fit, suggesting that this is, in fact, a false-positive result. We also found that using CSI to measure lifetime smoking exposure resulted in a better fitting model for our data than using cigarette pack years but we found no evidence of a dose-dependent response of ALS risk to smoking.
Our results are similar to those from a study conducted in the Netherlands which found current smoking to be associated with ALS in an incident cohort but no strong dose-dependent relationship (Citation9). The strength of the association between smoking and ALS was reported as weak in a meta-analysis of case-control and cohort studies, with a higher effect in women (Citation7). This weakness may be due to the reliance on prevalent and clinic cohorts which would under-represent smokers because their survival is shorter (Citation9).
A pooled analysis of prospective studies found that there was an increased risk of ALS in former and current smokers (Citation13). Two large prospective cohort studies included in the pooled analysis were originally set up as prospective studies into environmental exposures and cancer risk (Citation11,Citation14). People with ALS were identified from death certificates, which may over-represent people who smoke as their survival is shorter.
The CSI is more useful than cigarette pack years to investigate dose-dependency, as it formally considers the decreased risk of disease after smoking cessation. The CSI had a bimodal distribution of smoking exposure in both cases and controls, corresponding to smoking at the time of survey (). The mean CSI of current smokers is slightly higher in cases than controls and so dose-dependency in current smokers should be investigated further.
Median age of smoking initiation was around the late teens in both groups, and it has been reported that frontotemporal dementia, a behavioral change that occurs in some people with ALS is not associated with smoking behaviors, so the association is unlikely to reflect reverse causality (Citation24).
The strengths of this study are that we have detailed environmental data on incident cases of ALS and controls. A limitation is the sample size which means it is only powered to detect relatively large effect sizes with odds ratios of the order of 1.8 or higher. Retrospective case-control studies generally suffer from recall bias. This study may suffer the effect of two opposing sample biases: people in an environmental study of lifestyle may be more likely to smoke heavily, and some people in this ALS study attended specialist clinics so may be less likely to smoke. Additionally, we do not know how many controls who were contacted declined to participate, so the control population may be biased. There were no current smokers in the controls recruited in London, although a subgroup analysis in the other two areas shows that odds ratios for current smoking are consistent between the remaining areas.
We found that people with ALS were less likely to drink alcohol, but our survey responses do not support a protective relationship as ALS was cited as the reason for not drinking in most cases. Despite controlling for drinking and educational status, it is not possible to completely rule out the effects of confounding.
In this study of smoking and ALS, we do not find strong evidence to support smoking as a risk factor, even using lifetime smoking exposure as measured by the CSI.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Acknowledgment
We would like to thank people with MND and their families for their participation in this project. This is in part an EU Joint Program – Neurodegenerative Disease Research (JPND) project.
Additional information
Funding
References
- Brown RH, Al-Chalabi A. Amyotrophic lateral sclerosis. N Engl J Med. 2017;377:162–72.
- Westeneng H-J, Debray TPA, Visser AE, van Eijk RPA, Rooney JPK, Calvo A, et al. Prognosis for patients with amyotrophic lateral sclerosis: development and validation of a personalised prediction model. Lancet Neurol. 2018;17:423–33.
- Al-Chalabi A, Fang F, Hanby MF, Leigh PN, Shaw CE, Ye W, et al. An estimate of amyotrophic lateral sclerosis heritability using twin data. J Neurol Neurosurg Psychiatry. 2010;81:1324–6.
- Longinetti E, Fang F. Epidemiology of amyotrophic lateral sclerosis: an update of recent literature. Curr Opin Neurol. 2019;32:771–6.
- McLaughlin RL, Vajda A, Hardiman O. Heritability of amyotrophic lateral sclerosis: insights from disparate numbers. JAMA Neurol. 2015;72:857–8.
- Smith GD. Epidemiology, epigenetics and the ‘Gloomy Prospect’: embracing randomness in population health research and practice. Int J Epidemiol. 2011;40:537–62.
- Alonso A, Logroscino G, Hernán MA. Smoking and the risk of amyotrophic lateral sclerosis: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2010;81:1249–52.
- Alonso A, Logroscino G, Jick SS, Hernán MA. Association of smoking with amyotrophic lateral sclerosis risk and survival in men and women: a prospective study. BMC Neurol. 2010;10:6.
- de Jong SW, Huisman MHB, Sutedja NA, van der Kooi AJ, de Visser M, Schelhaas HJ, et al. Smoking, alcohol consumption, and the risk of amyotrophic lateral sclerosis: a population-based study. Am J Epidemiol. 2012;176:233–9.
- Fang F, Bellocco R, Hernán MA, Ye W. Smoking, snuff dipping and the risk of amyotrophic lateral sclerosis–a prospective cohort study. Neuroepidemiology 2006;27:217–21.
- Gallo V, Bueno-De-Mesquita HB, Vermeulen R, Andersen PM, Kyrozis A, Linseisen J, et al. Smoking and risk for amyotrophic lateral sclerosis: analysis of the EPIC cohort. Ann Neurol. 2009;65:378–85.
- Kamel F, Umbach DM, Munsat TL, Shefner JM, Sandler DP. Association of cigarette smoking with amyotrophic lateral sclerosis. Neuroepidemiology 1999;18:194–202.
- Wang H, O’Reilly ÉJ, Weisskopf MG, Logroscino G, McCullough ML, Thun M, et al. Smoking and risk of amyotrophic lateral sclerosis: a pooled analysis of five prospective cohorts. Arch Neurol. 2011;68:207–13.
- Weisskopf MG, McCullough ML, Calle EE, Thun MJ, Cudkowicz M, Ascherio A. Prospective study of cigarette smoking and amyotrophic lateral sclerosis. Am J Epidemiol. 2004;160:26–33.
- Armon C. Smoking may be considered an established risk factor for sporadic ALS. Neurology. 2009;73:1693–8.
- Beard JD, Kamel F. Military service, deployments, and exposures in relation to amyotrophic lateral sclerosis etiology and survival. Epidemiol Rev. 2015;37:55–70.
- Sutedja NA, Veldink JH, Fischer K, Kromhout H, Wokke JH, Huisman MH, et al. Lifetime occupation, education, smoking, and risk of ALS. Neurology. 2007;69:1508–14.
- D’Amico E, Factor-Litvak P, Santella RM, Mitsumoto H. Clinical perspective of oxidative stress in sporadic ALS. Free Radic Biol Med. 2013;65:509–27.
- Roberts AL, Johnson NJ, Cudkowicz ME, Eum K-D, Weisskopf MG. Job-related formaldehyde exposure and ALS mortality in the USA. J Neurol Neurosurg Psychiatry. 2016;87:786–8.
- Leffondre K, Abrahamowicz M, Xiao Y, Siemiatycki J. Modelling smoking history using a comprehensive smoking index: application to lung cancer. Statist Med. 2006;25:4132–46.
- Brooks BR. El Escorial World Federation of Neurology criteria for the diagnosis of amyotrophic lateral sclerosis. Subcommittee on motor neuron diseases/amyotrophic lateral sclerosis of the World Federation of Neurology Research Group on neuromuscular diseases and the El Escorial “Clinical limits of amyotrophic lateral sclerosis” workshop contributors. J Neurol Sci. 1994;124:96–107.
- R Foundation for Statistical Computing. R: a language and environment for statistical computing. Vienna, Austria; 2017. https://cran.r-project.org/doc/FAQ/R-FAQ.html#Citing-R
- Akaike H. Information theory and an extension of the maximum likelihood principle. In: Parzen E, Tanabe K, Kitagawa G, eds. Selected papers of Hirotugu Akaike. New York, NY: Springer New York; 1998:199–213.
- Tremolizzo L, Bianchi E, Susani E, Pupillo E, Messina P, Aliprandi A, et al. Voluptuary habits and risk of frontotemporal dementia: a case control retrospective study. J Alzheimers Dis. 2017;60:335–40.