
Abstract
Objective: Amyotrophic lateral sclerosis (ALS) is a mostly sporadic neurodegenerative disease. The role of environmental factors has been extensively investigated but associations remain controversial. Considering that a substantial proportion of adult life is spent at work, identifying occupations and work-related exposures is considered an effective way to detect factors that increase ALS risk. This process may be further facilitated in population isolates due to environmental and genetic homogeneity. Our study investigated occupations and occupational exposures potentially associated with ALS risk in the isolated island population of Malta, using a case-control study design. Methods: Patients with ALS and randomly identified matched controls (1:1) were recruited throughout a four-year window, from 2017 through 2020. Data on educational level, residence, main occupation, smoking, and alcohol history were collected. Results: We found that compared to controls (44.4%), a higher percentage (73.7%) of ALS patients reported a blue-collar job as their main occupation (OR 2.04, 95% CI 1.2–3.72; p = 0.0072). Through regression analysis, craft and related trades occupations such as carpentry and construction (ISCO-08 major group 7), were found to be positively associated with ALS, with patients in this occupational category found to be more prone to develop bulbar-onset ALS (p = 0.0297). Overall, patients with ALS reported a significantly higher exposure to work-related strenuous physical activity (OR 2.35, 95% CI 1.53–3.59; p = 0.0002). Conclusion: Our findings suggest that manual workers particularly those working in the carpentry and construction industries have an increased ALS risk, possibly due to a history of intense or sustained physical activity.
Introduction
Amyotrophic lateral sclerosis (ALS) is a rapidly progressing, neurodegenerative disease. Onset is typically accompanied by clinical signs of upper and/or lower motor neuron degeneration and patients usually present with weakness in the bulbar muscles, only the limbs, or both regions simultaneously (Citation1,Citation2). ALS typically starts in the fifth or sixth decade of life, although cases with a younger or older age of onset are apparent (Citation3). Advances in genetics have improved significantly our understanding of the genetic causes of ALS, leading to the explanation of up to two-thirds of familial cases (Citation4). Nevertheless, the majority of ALS cases occur sporadically, without a clear family history of the disease. Relationships between exposure to environmental factors and ALS have thus been extensively investigated but associations remain controversial. Considering that a significant percentage of human life is spent at work, evaluating the occurrence of sporadic ALS (sALS) within occupational categories is thought to be a straightforward and effective way to detect disease risk factors.
Occupational risks have long been addressed with a classical study, published more than 50 years ago, presenting evidence indicating a trend for ALS to occur among persons engaged in physical labor (Citation5). More recently, several studies are supportive of an increased ALS risk in professions associated with strenuous physical exertion and/or sustained physical activity (PA) including professional European and American football players (Citation6–9), elite long-distance cross-country skiers (Citation10), military personnel (Citation11–13), and manual workers comprising mechanics, painters, and employees in the agriculture and construction industry (Citation14–18). Small and large-scale case-control studies have further confirmed an association between risk of developing ALS and a history of PA in occupation-related activities (Citation19–21). Nonetheless, contradictory findings that are unsupportive of this link have also been reported in several studies (Citation22–26), and like many environmental factors the role of PA in ALS causation remains inconclusive.
In addition to reduced genetic diversity, population isolates experience environmental homogeneity, which facilitates the identification of environmental factors that increase ALS risk. To this end, due to its geographical and cultural isolation, the native population of Malta offers a unique opportunity to study ALS. Malta is one of the southernmost states of the European Union, situated between Sicily and Africa at a latitude of 35.9 and longitude of 14.4. Consisting of an archipelago of three inhabited islands (total area 316 km2), Malta has a population of 514,564, based on Malta’s National Statistics Office (NSO) data in 2019. Climatic conditions are typical of the Mediterranean zone with very mild winters and hot, dry summers. Mean yearly temperature is around 23 °C during the day and 16 °C at night with the country experiencing, on average, 12.1 hours of daylight. The incidence of ALS in Malta is 2.5 cases per year per 100,000 persons and is similar to the European median (Citation27). In this work, we sought to investigate occupational factors potentially associated with ALS risk in Malta, using a population-based case-control study design.
Materials and methods
Subjects
Subjects were recruited throughout a four-year window, from 2017 through 2020, during which the population of Malta increased from 475,701 to 514,564 based on NSO data. During the study period, 38 ALS cases were identified. These were defined as patients diagnosed with probable or definite ALS, and were referred by consultant neurologists, the national Motor Neuron Disease association, general practitioners and neurophysiology units. Alternatively, patients or their relatives made direct contact with our laboratory expressing willingness to participate in the study. Patient participants met the revised El Escorial criteria for ALS (Citation28,Citation29). Controls were randomly identified from community general practitioner’s databases, eliminating those with an active neurological diagnosis. Controls were ascertained in a roughly 1:1 case-control ratio, and matched patients for age (±5 years), sex and geographical region.
Data collection
A face-to-face interview based on a structured questionnaire was used to collect demographic characteristics of participants and data on their marital status, educational level, residence, main occupation, cigarette smoking, and alcohol history. In cognitively impaired patients or patients with a deteriorating condition (5.3%), the data were obtained from a relative. An ALS Functional Rating Scale-revised (ALSFRS-R) score was calculated for every participant. Since Malta is heavily urbanized, subjects’ residence was classified as urban and exurban, defined as having >500 and <500 inhabitants per km2, respectively. The particular town or village in which a subject spent the longest time in residence was chosen for analysis. The main occupation was defined as the longest occupation held during the subject’s lifetime and was coded using the latest International Standard Classification of Occupation (ISCO-08) developed by the United Nations’ International Labour Organisation (http://www.ilo.org). The ISCO-08 categorizes jobs into 10 major groups based on similarity in skill level and tasks performed during the occupation. Subjects with an occupation requiring manual labor were classified as “blue collar” whereas the remainder were categorized as “white collar”. To quantify occupation-associated PA objectively, occupations were given scores based on the 2011 Compendium of Physical Activities (Citation30). The Compendium links occupation-associated activities to the respective metabolic equivalent of task (MET), which is the ratio of the rate at which a person expends energy while performing a specific PA compared to the energy expended when sitting quietly (resting metabolic rate). A MET score of 1.0 is defined as 1 kcal/kg body weight/hour. Subjects with an occupation having an MET score <4 were classified as having been exposed to moderate work-related PA whereas those with an MET score ≥4 were categorized as having experienced strenuous work-related PA.
Statistical analysis
Continuous variables were described as median and range, whereas categorical variables were reported as number of subjects (percentages). An exception was made for occupation-related MET scores for which the mean ± S.E.M. was given. Comparisons between continuous variables were made with the unpaired, Mann–Whitney’s test or the unpaired, two-tailed Student’s t test whereas comparison between categorical variables was made with χ2 test. To test for association between ALS case-control status of participants and main occupation based on ISCO classification, univariate analysis was performed using logistic regression considering the small sample size and to account for the matching of cases and controls. Odds ratio (OR) and associated 95% confidence interval were estimated where appropriate. A p value <0.05 was considered significant. Statistical analysis was carried out with GraphPad Prism v9 software (La Jolla, CA).
Results
The study population included 38 cases and 45 controls. Baseline characteristics are detailed in . Majority of cases were men (sex ratio = 1.9). The onset of symptoms was spinal in 31 patients (81.6%), bulbar in six patients (15.8%), and generalized in one patient (2.6%). The median age at onset was 60.5 years (range 27–80) and the median disease duration at interview was 30 months (range 6–108). ALSFRS-R score was 30.8 (11.5–44) for ALS patients and 47.9 (47–48) for controls (p < 0.0001). As a result of matching, there was no difference between patients and controls for sex () and age (median: ALS = 65.5, controls = 68; p = 0.0640). Geographical distribution for cases largely overlapped that of controls (), with the majority of individuals residing in the center and southeast of mainland Malta, a reflection of a high population density in these regions. No difference was therefore observed between exurban and urban residence, with more than four-fifths of the subjects in either group residing in urban areas (). Marital status was similar among cases and controls. The level of education was also comparable between the two groups, with approximately half having high school education. There were no significant differences between ALS patients and controls for smoking or alcohol consumption ().
Figure 1 Geographical distribution of ALS cases and controls resident in the archipelago of Malta. Symbol map was generated by Datawrapper. Size of circles reflects size of sample.
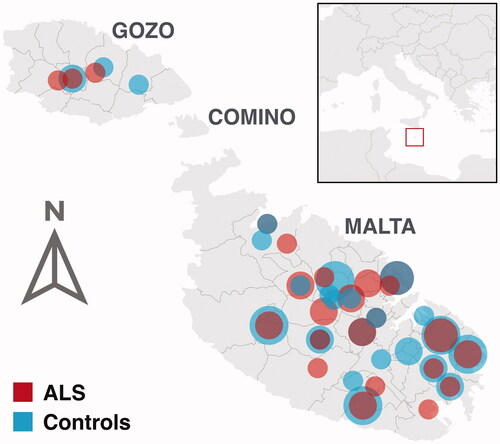
Table 1 Demographic characteristics of Maltese ALS patients and controls.
Type of main occupation was significantly different in cases and controls. Hence, compared to controls, a higher percentage of ALS patients reported a blue collar job as the main occupation during their entire career (). Blue collar workers were therefore twice as likely to develop ALS compared to controls. Considering the distribution of main occupations based on ISCO classification (), craft and related trades occupations, including carpentry and construction, were found to be associated with ALS (OR = 17.50, p = 0.0350). Bulbar-onset ALS was more prevalent in these workers compared to other occupations (42.9% vs. 9.7%; p = 0.0297). There was no statistically significant sex ratio between the two groups (2.5 vs. 2; p = 0.05873). Odds for elementary occupations including cleaners were also high but association did not reach statistical significance (; p = 0.0774). Compared to controls, patients with ALS had a significantly higher exposure to work-related strenuous PA (). Cases were thus more than twice as likely to experience intense PA occurring as part of their occupation and frequently described their occupation as sweat-inducing. In confirmation, mean occupation-associated MET scores for ALS patients were markedly higher than those of controls (p = 0.0010; ).
Figure 2 Average MET score in ALS patients and controls.
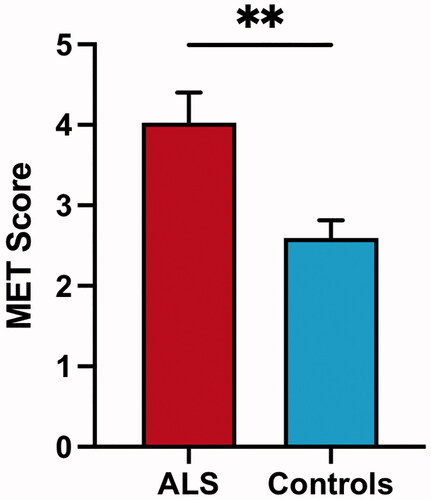
Table 2 Distribution of main occupations in ALS patients and controls.
Discussion
This case-control study based on an isolated island population suggests that manual workers, particularly those working in the carpentry and construction industries have an increased ALS risk, possibly associated with a history of physical exertion. We also found that in this occupational category, ALS patients were at a higher risk of developing the bulbar-onset type of the disease, which is associated with a worse prognosis. Our findings confirm early studies showing a significantly increased distribution of ALS cases among individuals engaged in heavy physical labor in both American and European populations (Citation5,Citation31,Citation32). More recently, a multi-population study, also corroborates our results. Thus, using population-based ALS registries from Italy, United Kingdom, and Ireland, Beghi et al. (Citation19) showed that in contrast to controls, a significant number of cases had blue-collar occupations and a higher percentage of patients with ALS reported strenuous PA at work. A positive association for individuals employed in construction was reported by three independent studies based on case-control cohorts derived from the populations of New England, Ohio, and Denmark (Citation15,Citation16,Citation33). Carpenters were also identified as an occupation with a significantly higher risk according to a case-control study in Turin, Italy (Citation34). Although various environmental risk factors can contribute to increasing ALS risk in this category of workers, intense or sustained PA is hypothesized to be a contributing factor.
A role for PA in ALS causation is supported by various reports that identified an association between occupation-related and/or leisure-related PA. In a Dutch cohort, ALS patients had significantly higher levels of leisure-time PA compared to controls (Citation23). In corroboration, Italian professional footballers were found to have a higher risk of developing ALS compared to the general population (Citation7,Citation9) and triathlon athletes were over-represented in Israeli patients with ALS (Citation35). Interestingly, both triathletes and footballers with ALS had a higher frequency of bulbar-onset ALS compared to other patients (Citation6,Citation35), a result that resonates with our findings. In a population within Northern England, ALS cases consistently reported higher PA in work and leisure-related activities (Citation21). Recently, in a study recruiting incident cases and controls from five population-based registers in The Netherlands, Ireland, and Italy, Visser et al. (Citation20) showed a linear association between ALS and PA in leisure time and occupational activities, and all activities combined. Although these findings including ours, favor intense or prolonged PA as an ALS risk factor, other studies do not support this role (Citation22,Citation25,Citation26). Numerous factors might contribute to such an inconsistent landscape including differences in study design. However, we hypothesize that geographic variations in environmental exposures in addition to differences in the genetic make-up may contribute significantly to the reported discrepancies.
Limitations of this study include a low sample size, which is however expected considering the rare frequency of ALS in the relatively small population (half a million inhabitants) living on the archipelago of Malta. Data regarding leisure-time PA were unfortunately not collected. However, we believe that this would have had a minimal impact on the study’s findings considering that due to various factors (Citation36), participation in sports amongst Maltese is exceedingly low (Citation37) with a recent study on global leisure PA levels reporting that close to two thirds of the adult population is physically inactive (Citation38).
PA has long been hypothesized as a risk factor for developing ALS ever since Lou Gehrig, the legendary 1930s baseball player also known as “The Iron Horse”, succumbed to the disease. Results of our case-control study in a unique population isolate provide support for this hypothesis. Taken in the context of other studies, our data suggest that potentially modifiable occupational exposures may be responsible for a substantial proportion of ALS cases. Despite limitations of sample size, the ability to detect an association in a small sample is either reflective of a homogeneous population or indicative of the significant effect of the exposure. Studies that unveil the mechanisms underpinning the role of PA on ALS are warranted, with animal models being best suited to identify molecular events that can be therapeutically targeted in ALS (Citation39). Work by Garbugino et al. (Citation40) showing that prolonged voluntary running induced shorter survival and poorer disease prognosis in a mild SOD1 mouse model is not only confirmatory but a promising line of work in the right direction.
Ethical approval
Ethical approval for the study was given by the Research Ethics Committee of the University of Malta. All participants gave written informed consent.
Acknowledgements
The authors are indebted to all participants of this study.
Declaration of interest
The authors declare that they have no conflict of interest. The authors alone are responsible for the content and writing of this article.
Data availability statement
Readers seeking access to the data should contact the corresponding author. Access will be granted to named individuals in accordance with ethical procedures governing the reuse of sensitive data.
Additional information
Funding
References
- Brown RH, Al-Chalabi A. Amyotrophic lateral sclerosis. N Engl J Med. 2017;377:162–72.
- van Es MA, Hardiman O, Chio A, Al-Chalabi A, Pasterkamp RJ, Veldink JH, et al. Amyotrophic lateral sclerosis. Lancet. 2017;390:2084–98.
- Swinnen B, Robberecht W. The phenotypic variability of amyotrophic lateral sclerosis. Nat Rev Neurol. 2014;10:661–70.
- Caballero-Hernandez D, Toscano MG, Cejudo-Guillen M, Garcia-Martin ML, Lopez S, Franco JM, et al. The 'Omics' of amyotrophic lateral sclerosis. Trends Mol Med. 2016;22:53–67.
- Breland AE, Jr., Currier RD. Multiple sclerosis and amyotrophic lateral sclerosis in Mississippi. Neurology. 1967;17:1011–6.
- Chio A, Calvo A, Dossena M, Ghiglione P, Mutani R, Mora G. ALS in Italian professional soccer players: the risk is still present and could be soccer-specific. Amyotroph Lateral Scler. 2009;10:205–9.
- Chio A, Benzi G, Dossena M, Mutani R, Mora G. Severely increased risk of amyotrophic lateral sclerosis among Italian professional football players. Brain. 2005;128:472–6.
- Lehman EJ, Hein MJ, Baron SL, Gersic CM. Neurodegenerative causes of death among retired National Football League players. Neurology. 2012;79:1970–4.
- Pupillo E, Bianchi E, Vanacore N, Montalto C, Ricca G, Robustelli Della Cuna FS, et al. Increased risk and early onset of ALS in professional players from Italian Soccer Teams. Amyotroph Lateral Scler Frontotemporal Degener. 2020;21:403–9.
- Fang F, Hallmarker U, James S, Ingre C, Michaelsson K, Ahlbom A, et al. Amyotrophic lateral sclerosis among cross-country skiers in Sweden. Eur J Epidemiol. 2016;31:247–53.
- McKay KA, Smith KA, Smertinaite L, Fang F, Ingre C, Taube F. Military service and related risk factors for amyotrophic lateral sclerosis. Acta Neurol Scand. 2021;143:39–50.
- Seals RM, Kioumourtzoglou MA, Hansen J, Gredal O, Weisskopf MG. Amyotrophic lateral sclerosis and the military: a population-based study in the Danish registries. Epidemiology. 2016;27:188–93.
- Sutedja NA, Veldink JH, Fischer K, Kromhout H, Heederik D, Huisman MH, et al. Exposure to chemicals and metals and risk of amyotrophic lateral sclerosis: a systematic review. Amyotroph Lateral Scler. 2009;10:302–9.
- Filippini T, Tesauro M, Fiore M, Malagoli C, Consonni M, Violi F, et al. Environmental and occupational risk factors of amyotrophic lateral sclerosis: a population-based case-control study. Int J Environ Res Public Health. 2020;17:2882.
- Andrew AS, Bradley WG, Peipert D, Butt T, Amoako K, Pioro EP, et al. Risk factors for amyotrophic lateral sclerosis: a regional United States case-control study. Muscle Nerve. 2020;63:52–9.
- Dickerson AS, Hansen J, Kioumourtzoglou MA, Specht AJ, Gredal O, Weisskopf MG. Study of occupation and amyotrophic lateral sclerosis in a Danish cohort. Occup Environ Med. 2018;75:630–8.
- Furby A, Beauvais K, Kolev I, Rivain JG, Sebille V. Rural environment and risk factors of amyotrophic lateral sclerosis: a case-control study. J Neurol. 2010;257:792–8.
- Govoni V, Granieri E, Fallica E, Casetta I. Amyotrophic lateral sclerosis, rural environment and agricultural work in the Local Health District of Ferrara, Italy, in the years 1964–1998. J Neurol. 2005;252:1322–7.
- Beghi E, Logroscino G, Chio A, Hardiman O, Millul A, Mitchell D, et al. Amyotrophic lateral sclerosis, physical exercise, trauma and sports: results of a population-based pilot case-control study. Amyotroph Lateral Scler. 2010;11:289–92.
- Visser AE, Rooney JPK, D’Ovidio F, Westeneng H-J, Vermeulen RCH, Beghi E, et al. Multicentre, cross-cultural, population-based, case-control study of physical activity as risk factor for amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2018;89:797–803.
- Harwood CA, Westgate K, Gunstone S, Brage S, Wareham NJ, McDermott CJ, et al. Long-term physical activity: an exogenous risk factor for sporadic amyotrophic lateral sclerosis? Amyotroph Lateral Scler Frontotemporal Degener. 2016;17:377–84.
- Pupillo E, Messina P, Giussani G, Logroscino G, Zoccolella S, Chio A, et al. Physical activity and amyotrophic lateral sclerosis: a European population-based case-control study. Ann Neurol. 2014;75:708–16.
- Huisman MH, Seelen M, de Jong SW, Dorresteijn KR, van Doormaal PT, van der Kooi AJ, et al. Lifetime physical activity and the risk of amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2013;84:976–81.
- Armon C, Kurland LT, Daube JR, O'Brien PC. Epidemiologic correlates of sporadic amyotrophic lateral sclerosis. Neurology. 1991;41:1077–84.
- Longstreth WT, McGuire V, Koepsell TD, Wang Y, van Belle G. Risk of amyotrophic lateral sclerosis and history of physical activity: a population-based case-control study. Arch Neurol. 1998;55:201–6.
- Gallo V, Vanacore N, Bueno-de-Mesquita HB, Vermeulen R, Brayne C, Pearce N, et al. Physical activity and risk of amyotrophic lateral sclerosis in a prospective cohort study. Eur J Epidemiol. 2016;31:255–66.
- Borg R, Farrugia Wismayer M, Bonavia K, Farrugia Wiswayer A, Vella M, van Vught JFA, et al. Genetic analysis of ALS cases in the isolated island population of Malta. Eur J Hum Genet. 2021. DOI: https://doi.org/10.1038/s41431-020-00767-9
- Brooks BR, Miller RG, Swash M, Munsat TL, World Federation of Neurology Research Group on Motor Neuron Diseases. El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord. 2000;1:293–9.
- Ludolph A, Drory V, Hardiman O, Nakano I, Ravits J, Robberecht W, et al. A revision of the El Escorial criteria – 2015. Amyotroph Lateral Scler Frontotemporal Degener. 2015;16:291–2.
- Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32:S498–S504.
- Bracco L, Antuono P, Amaducci L. Study of epidemiological and etiological factors of amyotrophic lateral sclerosis in the province of Florence, Italy. Acta Neurol Scand. 1979;60:112–24.
- Provinciali L, Giovagnoli AR. Antecedent events in amyotrophic lateral sclerosis: do they influence clinical onset and progression? Neuroepidemiology. 1990;9:255–62.
- Fang F, Quinlan P, Ye W, Barber MK, Umbach DM, Sandler DP, et al. Workplace exposures and the risk of amyotrophic lateral sclerosis. Environ Health Perspect. 2009;117:1387–92.
- Chio A, Meineri P, Tribolo A, Schiffer D. Risk factors in motor neuron disease: a case-control study. Neuroepidemiology. 1991;10:174–84.
- Gotkine M, Friedlander Y, Hochner H. Triathletes are over-represented in a population of patients with ALS. Amyotroph Lateral Scler Frontotemporal Degener. 2014;15:534–6.
- Cauchi D, Rutter H, Knai C. An obesogenic island in the Mediterranean: mapping potential drivers of obesity in Malta. Public Health Nutr. 2015;18:3211–23.
- EU. Special eurobarometer 472: sport and physical activity. Brussels: European Commission; 2017.
- Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380:247–57.
- Aquilina B, Cauchi RJ. Modelling motor neuron disease in fruit flies: lessons from spinal muscular atrophy. J Neurosci Methods. 2018;310:3–11.
- Garbugino L, Golini E, Giuliani A, Mandillo S. Prolonged voluntary running negatively affects survival and disease prognosis of male SOD1G93A low-copy transgenic mice. Front Behav Neurosci. 2018;12:275.