
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objectives: High-intensity physical activity and sports prone to repetitive injuries of the cervical spine and head (when associated with vigorous practice) have been suggested as possible risk factors for amyotrophic lateral sclerosis (ALS). Our objective was to evaluate the relationship between the practice of contact sports (boxing, hockey, football, rugby) and ALS. Methods: The study included 2247 individuals, 1326 patients and 921 controls from several European countries. Analysis of the effect of contact sports on ALS was conducted in male participants only, as very few women practiced contact sports. Logistic regression models were used with the response variable as the presence or absence of ALS, with α = 0.05 significance level. Results: A relationship between the practice of contact sports and ALS was found, with those practicing contact sports having 76% higher odds of an ALS diagnosis (OR = 1.76, p = 0.001). In addition, univariate analyses for age (higher risk for older people, p < 0.001), smoking status (higher risk for ex-smokers, p = 0.022) and tobacco exposure (higher risk for more exposure, p = 0.038) also indicated that these variables are risk factors for ALS. In multivariate models, in addition to age, the interaction term between practice of contact sports and tobacco exposure was still significant (p = 0.03). Conclusions: This is one of the largest studies on the role of contact sport in ALS development. Our results support the existence of a relationship between the practice of sports with repetitive trauma at the level of the cervical spine and head, and ALS. This risk appears to be enhanced by tobacco exposure.
Introduction
Amyotrophic lateral sclerosis (ALS) is a rapidly progressive neurodegenerative disease, involving mainly the motor system, currently without a cure. Approximately 50% of ALS patients die within 30 months of onset of symptoms, often due to respiratory failure and its complications, while about 10% of patients can survive for more than a decade (Citation1).
ALS patients present with lower and/or upper limb weakness (spinal-onset ALS), or with bulbar weakness (bulbar onset ALS), but other less frequent presentations are observed, such as respiratory or generalized-onset (Citation1,Citation2). Most patients present with a negative family history, but in 5–10% there are one or more family members affected, familial ALS. More than 30 genes have been associated with ALS, mainly in familial cases, whereas gene mutations can be found only in about 10% of sporadic patients (Citation3).
Aging, gender and smoking are well-established risk factors for ALS, while a role of additional factors such as intense physical activity has been less clearly established (Citation4). Despite the existence of multiple studies (Citation2), data are still controversial, and more in-depth epidemiological investigation is critical.
Sports involving repetitive head and cervical spine trauma, such as football, are referred by some as a potential risk factor for the onset of ALS, especially when practiced vigorously (Citation5). Here we address this issue by evaluating the relationship between the practice of contact sports, such as boxing, rugby, martial arts, hockey and football (Citation5), and the occurrence of ALS. Moreover, we also investigated the interaction between contact sports and smoking as risk-factor in ALS, which to our knowledge has not been analyzed before.
Methods
Data
The data analyzed here were collected as part of the JPND ONWebDUALS (ONTology-based Web Database for Understanding Amyotrophic Lateral Sclerosis) project, which is a collective effort involving a consortium of partners from several European countries (Germany, Poland, Portugal and Turkey). The data set consists of answers to a standardized questionnaire by patients with ALS and controls, regarding demographic, lifestyle (including smoking), family history of ALS (or other neurodegenerative diseases), and practice of sports. This questionnaire was developed based on an international survey of specialists (Citation6). In general, the questionnaire was applied at initial consultation following diagnosis, and the patients were regularly followed in the participating centers. The questions, including smoking status, referred to the time before disease onset/diagnosis. Controls were spouses, family members and caregivers of the patients, as well as patients with mimicking disorders with initial suspicion of ALS (for example, benign fasciculations, motor neuropathies, myopathies and other neuromuscular disorders).
The study was approved by each of the local Ethics Committees. All patients and controls signed an informed consent before inclusion in the study.
Sports and contact sports
The questionnaire includes information on the practice of 21 different sports (e.g. volleyball, running, soccer, boxing, golf, tennis, …) and the intensity of this practice was graded into high (>150 minutes/week of vigorous physical activity, >1 year), moderate (>75 minutes/week of vigorous physical activity, >1 year) or low (regular but of lower intensity, >1 year) (Citation6). The present study focuses on sports that involve contact and increased risk of cervical and head trauma (Citation7). Following the work of Blecher et al. (Citation5), we defined a study participant as a practitioner of a contact sport, if (s)he practiced boxing, hockey, soccer or rugby at a moderate or high level of intensity. All others were considered to not practice a contact sport of interest for this study, including practitioners of these modalities at low intensity, practitioners of other sports regardless of intensity and those that did not practice any sport. Regular sports activity was defined as continuous practice for a minimum duration of one year.
Smoking
Participants responded whether they were regular smokers (>5 cigarettes/day, >1 year) or not, whether they had stopped or not, for how long they smoked regularly, and how much. Based on these responses, participants were grouped into three categories: smokers, nonsmokers, and ex-smokers. We also calculated a variable for tobacco exposure (TE) as “packs smoked per day” times “years smoked” (Citation8).
Data analysis
We present standard descriptive statistics of the main variable relevant to our study, including means, standard deviations and frequencies. Patients and controls were compared using the chi-square test for categorical variables and Student’s t-test for continuous variables. Within the group of patients, males and females were also compared by the same tests. We calculated the ALS Function Rating Score-revised decay rate (ALSFRS-R decay) as
where ALSFRS-R1st is the functional score at the first medical visit and Δt is the time in months between the first symptoms and the first medical visit for diagnosis.
Logistic regression models were used to study associations between the presence of ALS and the explanatory variables of interest. The response variable was binary, presence or absence of ALS. As independent variables, we considered: regular practice of contact sports (our main variable), age and tobacco exposure (TE). For the continuous variables age and tobacco exposure, the assumption of logit linearity was assessed. Multivariable models were constructed using a backward selection method. To assess the association between the presence of ALS and contact sports, only men were considered (both for patients and controls), because there were too few women who practiced contact sports.
We considered the significance level α = 0.05. Statistical analyses were performed using R with the interface RStudio Version 1.1.463 (Core Team, Vienna Austria) (Citation9).
Results
Participants’ characteristics
The study included 2247 participants, with 1326 patients (58% male) and 921 controls (47% male). There was a significantly larger fraction of male patients than male controls (p < 0.001). Other demographic and clinical characteristics of the participants are shown in . Patients were slightly older than controls, although this difference was more marked in females than in males (; ). More males than females smoked, and tobacco exposure was also heavier in males. For the latter, the average tobacco exposure for patients was 14.1 and for controls it was 12.4 (; ).
Figure 1 (A) Age of contact sports practitioners by gender (controls vs patients); (B) Age of non-practitioners of contact sports by gender (patients vs controls).
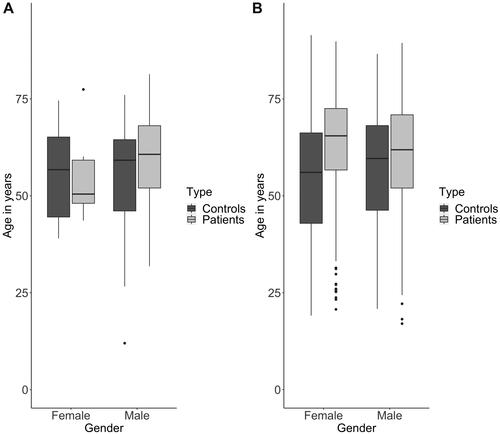
Figure 2 Tobacco exposure for male study participants. Tobacco exposure was higher for the practitioners of contact sports, especially in patients compared to controls. Note that this difference is not observed in those participants that did not practice contact sports. (Several outliers with TE up to 175 “packs per day” times “years smoked” are not shown.)
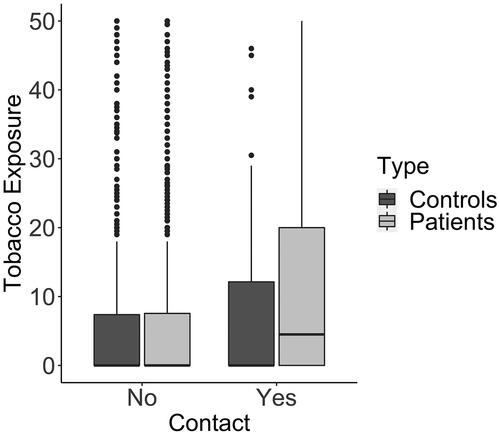
Table 1 Demographic and clinical characteristics of the participants.Table Footnotea
Most patients had spinal-onset ALS (76% for males, and 63% for females). The age of disease onset was slightly higher in females (61.3 years) vs. males (58.1 years). The initial decay rate in function (ALSFRS-R decay) was faster in women ().
Practice of sports
Our database lists 21 different sports practiced by the participants. Of the 2247 participants, 1016 (45.2%) reported regular sports activities. The three most common were cycling (n = 245, or 24.1% of sports practicing participants), soccer (n = 183, 18.0%), and fitness (n = 176, 17.3%). There were 221 (21.8%) participants who practiced contact sports with moderate to high levels of intensity, distributed as n = 173 soccer (78.3% of the participants who practice contact sports), n = 11 rugby (5.0%), n = 32 boxing (14.5%), and n = 13 hockey (5.9%), with some people reporting practice of more than one sport. Of these practitioners of contact sports, 196 were male and only 25 were female. Thus, there were too few females to analyze the impact of contact sports on their development of ALS. In what follows, we focus on the male participants only.
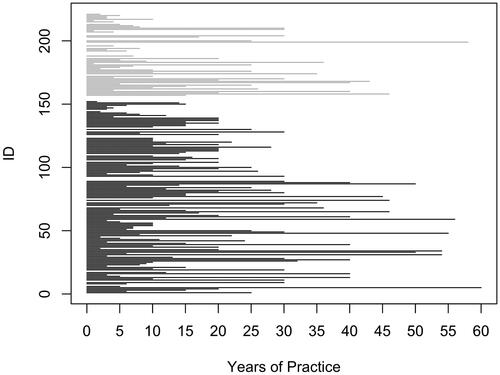
Although we did not consider in detail how long people practiced the sport of interest, because this information was not available for all participants, we did not find a difference in the years of practice between patients and controls, for whom this information was available (). However, a simple homogeneity test (chi-square test) showed a significant imbalance in the proportion of participants that practice contact sports in the patient group when compared to the same proportion in the control group (p = 0.002), considering only the male participants. This result points toward the existence of association between contact sports and ALS, which we explored in more detail next.
Figure 3 Years of practice of contact sports (black – controls; grey – patients) There is no significant difference in the duration of this practice (p = 0.24). (Of the 221 participants who practiced contact sports, this information was available for 190, and the y-axis is just an index for participant.).
Relationship between practice of contact sports and ALS diagnosis
The result of the chi-square analysis is confirmed by a univariate logistic regression model for ALS diagnosis and contact sport as an explanatory variably (p = 0.001, OR = 1.76, 95% CI 1.26–2.51). This analysis shows that people who practice contact sports (at a moderate or high intensity level) have 76% higher chance of being diagnosed with ALS than those who do not engage in those activities. In addition, univariate analyses for age, smoking status and tobacco exposure also indicate that these variables are risk factors for ALS (). The risk of ALS increases by 3% per year of age and by 0.5% per unit of tobacco exposure (packs smoked per day times years smoking). Ex-smokers have a 26% higher risk of ALS when compared with people who never smoked (p = 0.022; OR = 1.26, 95% CI 1.04–1.53) ().
Table 2 Results of univariate logistic models for the outcome ALS.
We next considered a multivariable logistic model including all these variables, since they were all significant in the univariate models; as well as all the possible interactions. We then removed interactions and variables in a backward stepwise approach, according to their lower contribution and non-significance in the model. The final model obtained in this analysis is shown in .
Table 3 Final multivariate logistic model for outcome ALS.
In the final model, age, practice of contact sports and the interaction of tobacco exposure with contact sport are all associated with ALS. For each year of increase in age, the chance of developing the disease is 1.02 times higher, and practicing contact sports increases the chance of ALS by 35%. This effect is further increased by tobacco exposure, that is, those who practiced contact sports have an approximately 3% increase in the odds of ALS per unit of tobacco exposure (packs smoked per day times years smoking), in comparison with those who do not practice contact sports and have the same tobacco exposure (p = 0.03). In this multivariable model, the interaction between age and practice of contact sports was not significant, and did not make it into the final model.
We conducted a sensitivity analyses, also for internal validation, for the potential effect of cycling (chosen because it is the sport with the largest number of practitioners) on ALS. We did not find a significant relationship between ALS and cycling either in an univariate model or in multivariate models with age and tobacco exposure. This indicates that practice of a vigorous sport per se is not associated with an ALS diagnosis.
Discussion and conclusion
In this study, we found an association between the practice of high intensity contact sport modalities and ALS. The results are aligned with the systematic review by Blecher et al. (Citation5) of 16 previous studies, which concludes that intense activity and sports associated with successive head and neck trauma increase the risk of developing ALS. Their outcome was the incidence of ALS or mortality associated with ALS, and exposure to any organized competitive sport, professional or nonprofessional, defined a priori as the sports with the greatest exposure of players to repetitive trauma to the head and back or cervical spine: American football, soccer, hockey, boxing, rugby. They found an overall pooled rate ratio of 1.80 (95%CI 1.13–2.88, heterogeneity degree I2 = 83%) for increased risk of ALS with practice of organized competitive sports. Compared to the 16 reviewed studies (Citation5), ours is one of the largest in terms of sample size, including more participants than 11 of those studies. We found a relationship between the practice of contact sports and the risk of developing ALS. Considering only the practice of contact sports, the odds of developing the disease is 1.76 times higher in practitioners, compared to non-practitioners. These sports also involve very vigorous physical activity, which has been recently proposed as a risk factor (Citation10), because strenuous exercise induces altered expression in genes enriched with known ALS risk genes. Thus, we cannot exclude this alternative explanation for our observed association between practice of contact sports and ALS, although we did not find this relationship for the practice of cycling, a strenuous exercise without contact.
The relationship between physical activity and sports-related trauma has received some attention in ALS (Citation5). Most studies found an association between intense leisure time activities (Citation11,Citation12), hard physical work (Citation11), organized sports in high school (Citation13), varsity sports (Citation14), specific sport activities like football (Citation15,Citation16), professional basketball playing (Citation16), professional road cycling (Citation16), and triathlon (Citation17) with ALS risk. This could be related to a higher risk of trauma in the head, back and cervical regions (Citation11) but the combination of both, sports and trauma, may be needed (Citation18). This combination could explain why ALS risk has been found increased in military personnel (Citation19), particularly in Gulf War veterans (Citation20), at least for a decade after deployment (Citation21), as confirmed in a recent meta-analysis (Citation22). In spite of this evidence, some studies were negative regarding the association between physical activity and ALS (Citation23). A recent meta-analysis (Citation5) concluded for a higher risk in professional athletes practicing sports with repetitive concussive head and cervical spinal trauma. The link we have found between the practice of contact sports and risk of ALS is supported by the known association between repetitive head trauma and widespread TDP-43 proteinopathy in several brain regions, in particular affecting the frontal and temporal cortices, brainstem, and sometimes associated with spinal cord involvement (Citation24). Moreover, head injury associated with contact sports can cause dysfunction of the brain pathways compensating for the loss of motor neurons in the frontal cortex, in particular by cerebellar activation, as documented in imaging studies (Citation25).
Smoking has been recognized as a risk factor for ALS (Citation26,Citation27) and can shorten survival of ALS patients (Citation28). This association was supported by one meta-analysis (Citation29), but again this is not fully accepted, as another meta-analysis provided a negative result (Citation30). Although we normally do not associate athletes with smoking habits, approximately 50% of contact practitioners in our study stated that they were or had been smokers. This allowed us to study simultaneously the impact of contact sports and smoking. We found an increased chance of ALS in those who practiced contact sports and smoked, a relationship not yet described in the literature, as far as we know.
One of the limitations of our study was the small number of women practicing contact sports, leading us to focus only the male study participants. Clearly, studies involving larger numbers of women are necessary to assess the impact of contact sports in the development of ALS in this population. A second limitation is that we did not have consistent information for all the participants on the duration of their practice of contact sports, thus we could not use this variable as a predictor in our model. Another study limitation is that the participants included were not systematically investigated for genetic mutations, thus the possible impact of these on our results could not be considered.
This is one of the largest studies in the ALS field and the data collected is very complete. Moreover, we followed a longitudinal study design and the data was systematically recorded using a standardized questionnaire applied in the different centers involved. Our results support the existence of a relationship between the practice of sports with repetitive trauma at the level of the cervical spine and head and ALS, a risk that is enhanced by tobacco exposure. Further research in this area is needed and more studies will be essential to draw the attention of athletes and sport federations to this problem.
Ethics statement
The study was approved by each of the local Ethics Committees. All patients and controls signed informed consent before inclusion in the study.
Declaration of interest
The authors report there are no competing interests to declare.
Data availability statement
The data that support the findings of this study are available from the authors, upon reasonable request.
Additional information
Funding
References
- National Institute of Neurological Disorders and Stroke. Amyotrophic lateral sclerosis fact sheet. National Institutes of Health. https://www.ninds.nih.gov/amyotrophic-lateral-sclerosis-als-fact-sheet.
- Longinetti E, Fang F. Epidemiology of amyotrophic lateral sclerosis: an update of recent literature. Curr Opin Neurol. 2019;32:771–6.
- Ungaro C, Sprovieri T, Morello G, Perrone B, Spampinato AG, Simone IL, et al. Genetic investigation of amyotrophic lateral sclerosis patients in south Italy: a two-decade analysis. Neurobiol Aging. 2021;99:99.e7–99.e14.
- Masrori P, Van Damme P. Amyotrophic lateral sclerosis: a clinical review. Eur J Neurol. 2020;27:1918–29.
- Blecher R, Elliott MA, Yilmaz E, Dettori JR, Oskouian RJ, Patel A, et al. Contact sports as a risk factor for amyotrophic lateral sclerosis: a systematic review. Glob Spine J. 2019;9:104–18.
- De Carvalho M, Ryczkowski A, Andersen P, Gromicho M, Grosskreutz J, Kuźma-Kozakiewicz M, et al. International survey of ALS experts about critical questions for assessing patients with ALS. Amyotroph Lateral Scler Front Degener. 2017;18:505–10.
- Tommasone BA, McLeod TCV. Contact sport concussion incidence. J Athl Train 2006;4:470–2.
- Nance R, Delaney J, McEvoy JW, Blaha MJ, Burke GL, Navas-Acien A, et al. Smoking intensity (pack/day) is a better measure than pack-years or smoking status for modeling cardiovascular disease outcomes. J Clin Epidemiol. 2017;81:111–9.
- R Core Team. R: A language and environment for statistical computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing; 2020. Available from: https://www.R-project.org/
- Julian TH, Glascow N, Barry ADF, Moll T, Harvey C, Klimentidis YC, et al. Physical exercise is a risk factor for amyotrophic lateral sclerosis: convergent evidence from Mendelian randomisation, transcriptomics and risk genotypes. EBioMedicine 2021;68:103397.
- Strickland D, Smith SA, Dolliff G, Goldman L, Roelofs RI. Physical activity, trauma, and ALS: a case-control study. Acta Neurol Scand. 1996;94:45–50.
- Huisman MHB, Seelen M, de Jong SW, Dorresteijn KRIS, van Doormaal PTC, van der Kooi AJ, et al. Lifetime physical activity and the risk of amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2013;84:976–81.
- Longstreth WT, McGuire V, Koepsell TD, Wang Y, Belle G. v. Risk of amyotrophic lateral sclerosis and history of physical activity: a population-based case-control study. Arch Neurol. 1998;55:201.
- Scarmeas N, Shih T, Stern Y, Ottman R, Rowland LP. Premorbid weight, body mass, and varsity athletics in ALS. Neurology 2002;59:773–5.
- Belli S, Vanacore N. Proportionate mortality of Italian soccer players: is amyotrophic lateral sclerosis an occupational disease? Eur J Epidemiol. 2005;20:237–42.
- Chiò A, Calvo A, Dossena M, Ghiglione P, Mutani R, Mora G. ALS in Italian professional soccer players: the risk is still present and could be soccer-specific. Amyotroph Lateral Scler. 2009;10:205–9.
- Gotkine M, Friedlander Y, Hochner H. Triathletes are over-represented in a population of patients with ALS. Amyotroph Lateral Scler Front Degener. 2014;15:534–6.
- Valenti M, Pontieri FE, Conti F, Altobelli E, Manzoni T, Frati L. Amyotrophic lateral sclerosis and sports: a case-control study. Eur J Neurol. 2005;12:223–5.
- Weisskopf MG, Cudkowicz ME, Johnson N. Military service and amyotrophic lateral sclerosis in a population-based cohort. Epidemiology 2015;26:831–8.
- Horner RD, Kamins KG, Feussner JR, Grambow SC, Hoff-Lindquist J, Harati Y, et al. Occurrence of amyotrophic lateral sclerosis among Gulf War veterans. Neurology 2003;61:742–9.
- Horner RD, Grambow SC, Coffman CJ, Lindquist JH, Oddone EZ, Allen KD, et al. Amyotrophic lateral sclerosis among 1991 Gulf War veterans: evidence for a time-limited outbreak. Neuroepidemiology 2008;31:28–32.
- Tai H, Cui L, Shen D, Li D, Cui B, Fang J. Military service and the risk of amyotrophic lateral sclerosis: a meta-analysis. J Clin Neurosci. 2017;45:337–42.
- Pupillo E, Messina P, Giussani G, Logroscino G, Zoccolella S, Chiò A, et al. Physical activity and amyotrophic lateral sclerosis: a European population-based case-control study: physical activity in ALS. Ann Neurol. 2014;75:708–16.
- McKee AC, Gavett BE, Stern RA, Nowinski CJ, Cantu RC, Kowall NW, et al. TDP-43 proteinopathy and motor neuron disease in chronic traumatic encephalopathy. J Neuropathol Exp Neurol. 2010;69:918–29.
- Canosa A, D'Ovidio F, Calvo A, Moglia C, Manera U, Torrieri MC, et al. Lifetime sport practice and brain metabolism in amyotrophic lateral sclerosis. Neuroimage Clin. 2020;27:102312.
- Sutedja NA, Veldink JH, Fischer K, Kromhout H, Wokke JHJ, Huisman MHB, et al. Lifetime occupation, education, smoking, and risk of ALS. Neurology 2007;69:1508–14.
- Wang H, O’Reilly ÉJ, Weisskopf MG, Logroscino G, McCullough ML, Thun MJ, et al. Smoking and risk of amyotrophic lateral sclerosis: a pooled analysis of 5 prospective cohorts. Arch Neurol. 2011;68:207–13.
- Calvo A, Canosa A, Bertuzzo D, Cugnasco P, Solero L, Clerico M, et al. Influence of cigarette smoking on ALS outcome: a population-based study. J Neurol Neurosurg Psychiatry. 2016;87:1229–33.
- Armon C. Smoking may be considered an established risk factor for sporadic ALS. Neurology 2009;73:1693–8.
- Alonso A, Logroscino G, Hernan MA. Smoking and the risk of amyotrophic lateral sclerosis: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2010;81:1249–52.