
Abstract
Objective
This study set out to investigate, using qualitative methodology, the experiences of spouses of people with Amyotrophic Lateral Sclerosis (ALS) during the coronavirus pandemic, with particular focus on spouse distress and cognitive and behavioral change in people with ALS (pwALS).
Methods
Qualitative semi-structured interviews of nine spouses of pwALS living in England were conducted between 11/09/2020 and 20/04/2021, focusing on spouses’ perspectives of how their lives and the lives of pwALS were affected by the pandemic and related lockdowns. Interviews were subject to thematic analysis.
Results
Four superordinate themes were identified from the spouses’ interviews: (i) pandemic behaviors, which encompassed accounts of cautious behavior, relaxation of cautious behavior, and other people’s attitudes to shielding the person with ALS; (ii) changes to daily life caused by the pandemic and progression of ALS; (iii) distress in spouses, which included anxiety, depression, and burden; and (iv) ALS-related behavioral impairment. Spouses also provided mixed accounts of telehealth care, pointing out its convenience but some felt that face-to-face appointments were preferable.
Conclusions
While many reactions to the pandemic reported by spouses of pwALS may have been similar to those of the general population or other vulnerable groups, interviews indicated the potential for the pandemic to have made more apparent certain aspects of behavioral change in pwALS with which carers may require support. Clinicians need to acknowledge spouses’ concerns about the potential limitations of remote clinical consultations, enquire about cognitive and behavioral change, and consider how input should be best provided in such limiting circumstances.
Introduction
The impact of pandemic (SARS-CoV-2) lockdowns on pwALS and their carers has attracted international research attention (Citation1, Citation2).
The quality of life (QoL) of pwALS has been negatively affected by pandemic lockdowns (Citation3, Citation4), potentially due to decreased social and environmental interactions (Citation5). Pandemic-related isolation of pwALS is not always found to be problematic, however, because having ALS already leads to isolation (Citation1).
In pwALS, feeling forgotten by clinicians or changed relationships with neurologists is associated with anxiety (Citation6). Fear of being denied treatment in general has also been reported by pwALS (Citation7). During the pandemic efforts were made by many clinics to continue to provide care remotely (e.g. via telephone or videoconferencing) to prevent disease complications, improve QoL for caregivers and limit pandemic-specific anxiety and depression (Citation8).
However, healthcare for pwALS during the pandemic was considered sub-optimal by pwALS and healthcare professionals (Citation9); this dissatisfaction reflected cancelations and delayed in-person appointments as well as replacement of in-person appointments with remote appointments. There were mixed views as to whether in-person appointments or a hybrid model of in-person and remote appointments was preferable (Citation9).
Concern over the completeness of remote clinical assessments has been raised (Citation4, Citation7) particularly over the provision of gastrostomy, respiratory function testing and noninvasive ventilation (Citation7, Citation10). Nonetheless, pwALS report that telehealthcare reduces travel, costs, fatigue, and anxiety linked with COVID-19 infection (Citation2).
Psychosocially, a study of pwALS and their caregivers found that caregivers report an increase in caregiving duties and related burden (Citation1). A deterioration in the mental health of caregivers of pwALS and people with dementia (not including ALS-Frontotemporal Dementia; ALS-FTD) during the pandemic has been reported, with anxiety levels increasing (Citation6, Citation11). Behavioral alteration in pwALS is one of the variables most strongly associated with caregiver burden (Citation6).
National lockdowns (Citation12) have resulted in ALS caregivers reporting feelings of isolation, loneliness, and helplessness, among other negative emotions; the greatest difficulty for caregivers of pwALS is the loss of support from healthcare professionals, increasing feelings of helplessness (Citation12).
Between March 2020–March 2021, three national lockdowns were imposed in England by the government in response to the global COVID-19 pandemic (Citation13). Given the impact of lockdowns on QoL, we set out to investigate, using qualitative methodology, (i) the experience of spouses of pwALS of lockdown in England in terms of methods of protecting themselves and how daily life changed; (ii) the impact of the coronavirus pandemic on spouses of pwALS in terms of spouse distress (anxiety, depression and burden); and (iii) the perceived impact of the coronavirus pandemic on pwALS in terms of progression of the disease, cognitive and behavioral changes and whether these made caregiving more difficult.
Methods
Participants
Spouses of pwALS who were aged at least 18 years old, and able to give informed consent were approached for this study. They had recently participated in other research by the authors estimating behavioral change in pwALS (and where the pwALS had themselves participated in a study on cognitive change in ALS). They were approached to minimize the likelihood of distress when contacting spouses of pwALS who were deceased. Participants were, therefore, known to the interviewer. Details about the interviewer (LD) are provided in Supplementary Information 1.
It was expected that 10–21 participants would be needed for this study before saturation of themes was reached, given that a purposive sampling method (Supplementary Information 2) was used and the scope of the measured phenomenon was small (Citation14–16). Twenty-two spouses of pwALS were invited to participate (10 initially, with more being approached as others declined or were unavailable, until saturation of themes was reached); five people did not reply, and six declined the invitation. A total sample of 11 spouses of pwALS was recruited. However, due to technical issues only nine interviews could be transcribed and analyzed. Informal assessment during data collection indicated that saturation of themes had been reached.
Data collection
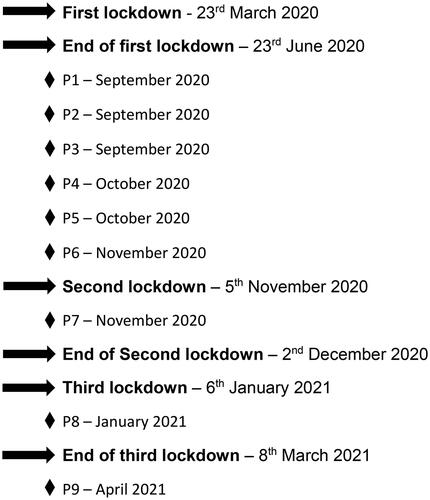
Data collection occurred between 11/09/2020 and 20/04/2021 (). Interviews were conducted online by LD during one session (50–80 min) using videoconferencing methods with participants who were at home. Semi-structured interviews were conducted using a topic guide. Only audio was recorded using screen recording software (AnyCap Screen Recorder V1.0.6.47 (Citation17)). Further details about the conduct of the interviews are given in Supplementary Information 2.
Figure 1. Timeline of interviews and coronavirus pandemic lockdowns in England.
Topic guide and interview structure
The topic guide (Supplementary Information 3), developed by LD and LG, addressed the experience of lockdown from the perspective of spouses of pwALS and the impact of the coronavirus pandemic on pwALS and their spouses. If interviews occurred after the second and third lockdown in England, participants were asked to reflect on the first lockdown when answering questions.
Spouses were asked about the methods they and the person with ALS employed to avoid contracting COVID-19; how the pandemic affected the person with ALS in terms of daily routines, medical appointments and community support; and, to highlight potential unexpected benefits from lockdowns, what elements of daily life remained the same or improved over the lockdown period. Spouses were asked whether and how their caring duties, and levels of anxiety, depression and burden changed. Questions to spouses about how the pandemic affected the person with ALS were specifically related to physical symptom progression and cognitive and behavioral changes noticed because of the pandemic, and whether any identified cognitive or behavioral changes, if present, made dealing with the pandemic more difficult.
Questions were phrased to be open-ended, to avoiding leading questions. There was a focus on balance by asking for positive, as well as negative, effects of the pandemic. Probing techniques were used to cue participants to develop their answers; examples and anecdotes were encouraged. See Supplementary Information 2 for methods on guiding the interview.
Data analysis
Thematic analysis was used to assess the interview data as it was the most suitable method for representing the views, opinions and experiences of spouses of pwALS. Supplementary Information 2 offers further justification for method choice and details of the analysis.
Results
Demographic information of participants
Participants were aged between 50–80. Six (66.7%) were female. All participants had known the person with ALS for over 10 years and had no other dependents. Seven participants (77.8%) did not report performing any caregiving duties for their spouse with ALS. Disease duration of the pwALS is shown in .
Table 1. Demographic information of participating spouses.
For the spouse sample whose interviews were analyzed, the status of pwALS in terms of cognitive and behavioral impairment was varied ().
Table 2. Summary of cognitive and behavioral impairment in the associated pwALS according to various screening tools.
Themes and subthemes
Four superordinate themes were identified: (i) pandemic behaviors; (ii) changes to daily life caused by the coronavirus pandemic and progression of ALS; (iii) spouse distress; (iv) ALS behavioral change.
Summaries of subthemes and codes within these subthemes that apply to pwALS specifically are presented in , alongside example quotations from interviews. Quotations demonstrating other subthemes that might have been expected in the general population or other high-risk groups, might have been expected in caregivers of other groups, or might have been expected in pwALS had the pandemic not occurred, are presented in tables in Supplementary Information 4. Example quotations and results for the superordinate theme, pandemic behaviors, can also be found in Supplementary Information 4.
Table 3. Summary of identified subthemes and codes related to changes to daily life caused by the COVID-19 pandemic with illustrative quotations.
Table 4. Summary of identified subthemes and codes related to distress in spouses as a result of the coronavirus pandemic with illustrative quotations.
Table 5. Summary of identified subthemes and codes related to ALS behavioral change with illustrative quotations.
Changes due to ALS or due to the pandemic
Three subthemes were identified: changes due to progression of ALS; changes due to the coronavirus pandemic; and changes caused by an interaction between ALS and the pandemic. Example quotations for changes due simply to the progression of ALS are presented in Supplementary Information 4.
Changes due to the coronavirus pandemic. This theme was formed of three codes: change in caregiving duties (Supplementary Information 4); changes to social interaction (Supplementary Information 4); and changes to medical appointments (). Most spouses had observed digital appointments with clinicians for the person with ALS and some experienced delays and cancelations of appointments with neurologists. The benefits of remote appointments included not visiting the hospital, which saved time and money; less formality; and the person with ALS did not need to use public transport which was helpful in preventing COVID-19. Four participants felt there was no difference between in-person and digital appointments and this gave them more options. However, five participants doubted the ability of clinicians to make accurate assessments of pwALS via videoconferencing, particularly assessments that traditionally involve clinicians touching their patient.
Of note, one spouse expressed concern that in-person appointments were canceled at short notice and poor aftercare was provided following a remote ALS diagnosis. They felt that the subsequent digital appointments were more organized but left little time for reassurance from clinicians and this affected the mental health of the person with ALS (quote 3.1.1.3, ).
Changes caused by an interaction between ALS and the pandemic. Participants often spoke about the challenges of separating the pandemic from the progression of ALS when trying to describe what had caused their lives to change. Disease progression and pandemic restrictions seemed to interact. Pandemic-related restrictions prevented pwALS from undertaking their hobbies or traveling. Over the pandemic period, their physical condition had deteriorated to the extent that, when pandemic restrictions were lifted, they would no longer be physically able to pursue these. Five participants felt that the period of time over which the pandemic had occurred had been the last chance for the person with ALS to have emotionally valuable experiences and this time had now been lost (quote 3.2.1.3, ).
Two participants struggled to think how their lives had changed during the pandemic because of the restricted way in which they lived to accommodate symptoms of ALS. One participant described ALS itself as a lockdown (quote 3.2.2.2, ). No spouses perceived an increase in the progression of ALS symptoms due to the pandemic. However, one participant spoke about the pandemic preventing the person with ALS, who was dysarthric, from being able to talk frequently with others which damaged their confidence and led them to avoid social interactions.
Distress in spouses
Anxiety. Anxiety was experienced by most participants and was predominantly about the person with ALS contracting COVID-19 (), the spouse contracting COVID-19, or being in crowds. Some reported no anxiety (Supplementary Information 4).
Depression. Spouses primarily reported a loss of interest in doing things and sleep disturbance (). Participants also commented on changes in how they felt about themselves, feeling emotional or sad, experiencing negative thoughts (quote 4.2.3.1, ), and having a limited capacity to worry about the person with ALS. Four spouses did not report any change in terms of frank depression, though most reported mild changes.
Burden. Only three participants reported increased feelings of burden (see for examples). One participant who expressed an increase in burden described it as resulting from a lack of professional support during the pandemic (quote 4.3.1.2, ). Others felt that the pandemic had not caused them to experience more burden or reported that they were not yet a caregiver and so felt no associated burden.
ALS behavioral or cognitive change
According to the spouse participants, none of the pwALS had received a clinical diagnosis of behavioral impairment, cognitive impairment, or ALS-FTD.
Behavioral change noticed by spouses. Three participants (P1, P4, P9; ) noticed behavioral change in the person with ALS that had occurred since the beginning of the pandemic. The most common change was apathy; emotional lability and becoming more detail oriented, denial or lack of insight were also reported. Apathy was perhaps noticed by spouses during the pandemic because usual activities for the person with ALS were disrupted and they had no interest in finding something else to do with their time, particularly the activities suggested by the spouse (quote 5.1.2.1, ).
Behavioral change that directly affects the spouse. Two spouses reported behavioral change in pwALS that impacted their interactions with them (P1, P9; ). One participant reported an increase in abrupt communication, although they questioned whether this was related to dysarthria rather than reflecting behavioral change. The other reported an increase in egocentric behavior which included ignoring the spouse to the extent that they felt “invisible”, and they described this behavior as “bizarre” (quote 5.2.2.1, ). If participants had noticed changes in the behavior of the person with ALS since the beginning of the pandemic, they did not believe that the pandemic had influenced these changes. None of these participants reported that behavioral changes in the person with ALS made dealing with the lockdown more difficult. None of the spouses reported any cognitive changes in the person with ALS.
Discussion
We identified four superordinate themes from the accounts given by spouses of pwALS: (i) pandemic behaviors; (ii) changes to daily life caused by the coronavirus pandemic and progression of ALS; (iii) spouse distress; (iv) ALS behavioral change. These superordinate themes are consistent with themes identified from surveys of pwALS concerning the pandemic (Citation4). Aspects of their reactions may resemble those seen in the general population or other vulnerable groups (Supplementary Information 4).
What is particularly noteworthy is how the restrictions in place to prevent the spread of COVID-19 were reported to have interacted with disease progression over the pandemic period to result in a sense of lost time; pandemic restrictions prevented life-enriching activities and mobility declined at such a rate that when pandemic restrictions were lifted, it would have been impossible for pwALS to physically participate in those life-enriching activities. ALS participants in another qualitative study (Citation1) hinted at this when they reported not being able to visit and socialize with loved ones during the pandemic, feeling that they had limited time to do this before deterioration prevented them from so doing.
The other particularly important finding is that some spouses felt their lives had not changed at all, even in full lockdown conditions, because their lives were already so restricted by the disease. Previous qualitative studies have similarly reported that isolation due to the pandemic was not problematic because pwALS and their caregivers were already isolated due to ALS symptoms (Citation1, Citation18).
Views about digital medical appointments were mostly positive, with comments focusing on the reduction in costs, stress and time associated with traveling to appointments, supporting other findings (Citation1, Citation2, Citation11, Citation19). Concerns were primarily over the ability of clinicians to make accurate remote assessments of physical symptoms.
Anxiety was frequently reported by spouses in this study, as found elsewhere in caregivers of pwALS (Citation6). Feelings of anxiety reported by the current spouses were often connected to the thought of the person with ALS contracting COVID-19, consistent with other studies (Citation18, Citation20).
Increased apathy in pwALS was the most frequently reported type of behavioral change over the pandemic period; the pandemic disrupted routine activity and pwALS demonstrating apathy appeared uninterested in finding something new to do. This finding is unsurprising given that apathy is the most common behavioral change in pwALS (Citation21). In addition to apathy and reduced interest in activities, loss of insight and egocentric behavior in pwALS were reported here, as elsewhere (Citation22). The three participants who reported behavioral change in the person with ALS did not believe that the pandemic had affected behavioral deterioration despite noticing the behavioral change during the pandemic. This may be because lockdown restrictions and shielding behaviors changed their lifestyles, such as interrupting regular hobbies and increasing time at home with their spouse. Therefore, spouses may have had more opportunities to notice behavioral symptoms during the pandemic, although they may have also noticed these had the pandemic not occurred. Given that during this period, access to clinical support was restricted as appointments were canceled and digital alternatives to face-to-face clinical assessments fell short for some participants, describing them as rushed and doubting the ability of clinicians to make thorough assessments, it will be important for clinicians to ask about cognitive and behavioral change in pwALS during future remote as well as face-to-face appointments and offer appropriate support.
Other key findings included increases in caregiver duties, increases in burden, loss of support, and a reduction in opportunities to take a break from the caregiver role (for those who reported having caregiving duties; ) during the pandemic, as also found reported elsewhere (Citation1, Citation11, Citation18–20, Citation23).
Strengths and limitations
This is one of the first qualitative interview studies of the effects of the coronavirus pandemic on spouses of pwALS in the United Kingdom and is the first to enquire about cognitive and behavioral change in pwALS within the context of spouse experience during the pandemic.
This study has some limitations. The generalizability of findings is limited for a few reasons. Firstly, the final sample of nine participants is not large but is consistent with appropriate sample sizes for thematic analysis (Citation24) and saturation of themes was reached. In addition, ALS may have been less severe in the patients whose spouses were included since the relevant pwALS had participated in another study by these authors, having to be able to communicate clearly orally or to write/type clearly. Consequently, this sample of spouses may have experienced different care duties to those of less independent pwALS with advanced mobility and communication difficulties, which appears to be the case given that 6/9 spouses provided caregiving for less than one hour per week. It would have been informative to have been able to describe the pwALS in terms of disease stage (Citation25) and explore how this might have impacted responses to the pandemic and lockdowns, but this information was not available. However, disease duration of the pwALS varied () and caring duties were more likely to be reported by the spouses where disease duration was longer.
While none of the pwALS related to this study had received a clinical diagnosis of cognitive or behavioral impairment or ALS-FTD, some participants were nonetheless spouses of pwALS who met cutoff scores for impairment on at least one of three cognitive screening tools (3/9 participants; ) or at least one of five behavioral screening tools (5/9 participants; ).
All participants had experienced the first lockdown in England and had experienced restrictions being lifted. However, three experienced additional lockdowns prior to being interviewed, two of whom were interviewed during a lockdown (P7, P8, ). Therefore, subsequent experiences and effects of delayed recall may have influenced their accounts.
Our study has identified specific behavioral changes in pwALS, such as increased apathy, reduced interest in activities, loss of insight, and egocentric behavior, for which caregivers may require support. Clinicians should acknowledge spouses’ concerns about remote consultations in adapting to the changing healthcare delivery landscape, actively enquire about cognitive and behavioral changes, and ensure that caregivers are aware of available support services, particularly in terms of respite care to alleviate feelings of burden. In conclusion, our findings suggest areas for improvement in service delivery in times of future national health crises and aspects of carers’ experiences that should deserve attention and support.
Authors’ contributions
Conceptualization: Lyndsay Didcote and Laura H Goldstein; methodology: Lyndsay Didcote and Laura H Goldstein; formal analysis and investigation: Lyndsay Didcote; writing – original draft preparation: Lyndsay Didcote; writing – review and editing: Lyndsay Didcote, Ammar Al-Chalabi and Laura H Goldstein; funding acquisition: Laura H Goldstein and Ammar Al-Chalabi; supervision: Ammar Al-Chalabi and Laura H Goldstein.
Ethical approval
This study received ethical approval from the London-Dulwich Research Ethics Committee 18/LO/1257. All participants gave written informed consent to participate.
Supplemental Material
Download Zip (116.9 KB)Acknowledgements
The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. For the purposes of open access, the authors have applied a Creative Commons Attribution (CC BY) licence to any Accepted Author Manuscript version arising from this submission.
Data availability statement
Qualitative interview data cannot be made publicly available due to the possible risk of compromising participants’ confidentiality.
Disclosure statement
AAC reports consultancies or advisory boards for Amylyx, Apellis, Biogen, Brainstorm, Cytokinetics, GenieUs, GSK, Lilly, Mitsubishi Tanabe Pharma, Novartis, OrionPharma, Quralis, Sano, Sanofi, and Wave Pharmaceuticals. AAC reports the following patent: Use of CSF-Neurofilament determinations and CSF-Neurofilament thresholds of prognostic and stratification value with regards to response to therapy in neuromuscular and neurodegenerative diseases. The other authors have no conflicts of interest to declare.
Additional information
Funding
References
- Genuis SK, Luth W, Bubela T, Johnston WS. Covid-19 threat and coping: application of protection motivation theory to the pandemic experiences of people affected by amyotrophic lateral sclerosis. BMC Neurol. 2022;22:140.
- Chan-Nguyen S, Karacam M, Ritsma B, Appireddy R. Patient perceptions on the virtual amyotrophic lateral sclerosis clinic during COVID-19. Can J Neurol Sci. 2022;49:618–22.
- Gonçalves F, Magalhães B. Effects of prolonged interruption of rehabilitation routines in amyotrophic lateral sclerosis patients. Palliat Support Care. 2021;4:1–6.
- Musson LS, Collins A, Opie-Martin S, Bredin A, Hobson EV, Barkhouse E, et al. Impact of the covid-19 pandemic on amyotrophic lateral sclerosis care in the UK. Amyotroph Lateral Scler Frontotemporal Degener. 2023;24:91–9.
- Gentili D, Deiana G, Chessa V, Calabretta A, Marras E, Solinas C, et al. Quality of life in amyotrophic lateral sclerosis patients and care burden of caregivers in sardinia during COVID-19 pandemic. Healthcare 2023;11:1641.
- Consonni M, Telesca A, Dalla Bella E, Bersano E, Lauria G. Amyotrophic lateral sclerosis patients’ and caregivers’ distress and loneliness during COVID-19 lockdown. J Neurol. 2021;268:420–3.
- Glasmacher SA, Larraz J, Mehta AR, Kearns PKA, Wong M, Newton J, Wong M, et al. The immediate impact of the COVID-19 pandemic on motor neuron disease services and mortality in Scotland. J Neurol. 2021;268:2038–40.
- De Marchi F, Cantello R, Ambrosini S, Mazzini L, Sarnelli MF, De Marchi I, et al. Telemedicine and technological devices for amyotrophic lateral sclerosis in the era of COVID-19. Neurol Sci. 2020;41:1365–7.
- De Marchi F, Gallo C, Sarnelli MF, De Marchi I, Saraceno M, Cantello R, et al. Accelerated early progression of amyotrophic lateral sclerosis over the COVID-19 pandemic. Brain Sci 2021;11:1291.
- De Marchi F, Sarnelli MF, Serioli M, De Marchi I, Zani E, Bottone N, et al. Telehealth approach for amyotrophic lateral sclerosis patients: the experience during COVID-19 pandemic. Acta Neurol Scand. 2021;143:489–96.
- Smaling HJA, Tilburgs B, Achterberg WP, Visser M. The impact of social distancing due to the COVID-19 pandemic on people with dementia, family carers and healthcare professionals: a qualitative study. Int J Environ Res Public Health. 2022;19.519. doi: 10.3390/ijerph19010519.
- Testoni I, Palazzo L, Pompele S, Vincenzo CD, Perardi M, Ronconi L. Coping and managing ALS disease in the family during COVID-19: caregivers’ perspective. OBM Neurobiol. 2023;07:1–26.
- Brown J, Kirk-Wade E. Coronavirus: a history of lockdown laws in England. House of Commons Library. 2021. https://researchbriefings.files.parliament.uk/documents/CBP-9068/CBP-9068.pdf
- Boddy CR. Sample size for qualitative research. QMR. 2016;19:426–32.
- Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18:59–82.
- Mason M. Sample size and saturation in PhD studies using qualitative interviews. Forum Qual Soc Res. 2010;11. doi: 10.17169/FQS-11.3.1428.
- Evaer Technologies E. AnyCap screen recorder software. New York: Evaer Technologies, 2020.
- UK Cabinet Office. COVID-19 response – Spring 2021 (Summary). 2021. Available at: https://www.gov.uk/government/publications/covid-19-response-spring-2021/covid-19-response-spring-2021-summary
- Bombaci A, Giusiano S, Peotta L, Iazzolino B, Mastro E, Arcari M, et al. Amyotrophic lateral sclerosis patients’ quality of life and their caregiver burden during COVID-19 pandemic. J Neurol Sci. 2021;429:117701.
- Lorenz-Dant K, Comas-Herrera A. The impacts of COVID-19 on unpaid carers of adults with long-term care needs and measures to address these impacts: a rapid review of evidence up to November 2020. J Long Term Care. 2021;124–53. doi: 10.31389/jltc.76.
- Witgert M, Salamone AR, Strutt AM, Jawaid A, Massman PJ, Bradshaw M, et al. Frontal-lobe mediated behavioral dysfunction in amyotrophic lateral sclerosis. Eur J Neurol. 2010;17:103–10.
- Gibbons ZC, Richardson A, Neary D, Snowden JS. Behaviour in amyotrophic lateral sclerosis. Amyotroph Lateral Scler. 2008;9:67–74.
- Budnick A, Hering C, Eggert S, Teubner C, Suhr R, Kuhlmey A, et al. Informal caregivers during the COVID-19 pandemic perceive additional burden: findings from an ad-hoc survey in Germany. BMC Health Serv Res. 2021;21.353. doi: 10.1186/s12913-021-06359-7.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101.
- Roche JC, Rojas-Garcia R, Scott KM, Scotton W, Ellis CE, Burman R, et al. A proposed staging system for amyotrophic lateral sclerosis. Brain. 2012;135:847–52.
- Abrahams S, Newton J, Niven E, Foley J, Bak TH. Screening for cognition and behaviour changes in ALS. Amyotroph Lateral Scler Frontotemporal Degener. 2014;15:9–14.
- Woolley SC, York MK, Moore DH, Strutt AM, Murphy J, Schulz PE, et al. Detecting frontotemporal dysfunction in ALS: utility of the ALS cognitive behavioral screen (ALS-CBSTM). Amyotroph Lateral Scler. 2010;11:303–11.
- Hsieh S, Mcgrory S, Leslie F, Dawson K, Ahmed S, Butler CR, et al. The mini-Addenbrooke’s cognitive examination: a new assessment tool for dementia. Dement Geriatr Cogn Disord. 2015;39:1–11.
- Elamin M, Pinto-Grau M, Burke T, Bede P, Rooney J, O’sullivan M, et al. Identifying behavioural changes in ALS: validation of the Beaumont behavioural inventory (BBI). Amyotroph Lateral Scler Frontotemporal Degener. 2017;18:68–73.
- Raaphorst J, Beeldman E, Schmand B, Berkhout J, Linssen WHJP, Van Den Berg LH, et al. The ALS-FTD-Q: a new screening tool for behavioral disturbances in ALS. Neurology 2012;79:1377–83.
- Mioshi E, Hsieh S, Caga J, Ramsey E, Chen K, Lillo P, et al. A novel tool to detect behavioural symptoms in ALS. Amyotroph Lateral Scler Frontotemporal Degener. 2014;15:298–304.