
Abstract
Study Design: Experimental, randomised crossover study.
Objectives: To investigate if three different interventions that provided plantar proprioceptive input were able to make acute improvements to the one-legged standing balance.
Background: Improved balance reduces the risk of falling. Therefore, it would be interesting if it were possible to improve balance with a simple intervention.
Methods: Eighteen healthy able-bodied subjects (4 males) were included in the study. Self-massage, Kinesio® tape and a custom-made insole were tested in a crossover design. The order of the interventions was randomised for each participant. The participants were asked to keep the balance on an instrumented wobbleboard. Differences between the three interventions was tested with an ANOVA with Tukey-corrected post-hoc tests.
Results: The custom-made insoles improved the standing balance by nine percent compared to baseline. This difference was statically significant (p < .05). The balance was not significantly better with the insole compared to self-massage or Kinesio® tape.
Conclusion: We found that an individually moulded insole improved one legged standing balance. Neither Kinesio® tape or self-massage with a massage ball on the plantar sole proved to improve balance.
Introduction
Balance is an important bodily attribute, because it is an imperative part of the human mobility.
A impaired balance leads to increased risk of falling [Citation1,Citation2]. Furthermore, when the standing balance in an individual is challenged, it can lead to reduced quality of life [Citation3]. In contrast, an improved balance can enhance sports performance and reduce lower limb injury frequency [Citation4]. Therefore, it would be interesting if it were possible to improve balance instantly with a simple intervention. It is well known that strength training and cardio-respiratory training in combination with functional training can improve cognitive and functional function in adults aged 65 + [Citation5], but as an addition to this progression in physical ability, a simple intervention with a positive effect would be very beneficial.
According to Shumway-Cook & Woollacott, the proprioception plays an important role in motor control [Citation6] and therefore, an increased proprioceptive input could have beneficial effects on balance tasks. The CNS can use ankle proprioceptive input to generate and modulate muscle activity in the region in order to maintain balance and stability in motor tasks [Citation7–9]. In 2006, Perry [Citation10] reported that the plantar-surface sensation is important for balance control because of the ability to sense changes in centre of pressure. Therefore, an increased awareness of the area could potentially lead to an improvement in the ability to sense the location of the centre of pressure.
Previously, Steinberg et al. [Citation11,Citation12] used textured insoles that stimulated the foot sole to improve ankle proprioception and postural balance in ballet dancers. They found that the ankle proprioception improved, whereas the postural balance only improved in the male dancers. Therefore, the mechanical stimulation with an insole on the foot sole can be expected to improve ankle proprioception and maybe balance [Citation13], but it is unknown if other interventions can produce a similar effect.
The purpose of the study was to investigate if three different interventions that provided plantar proprioceptive input were able to make acute improvements to one-legged standing balance on a wobble board. Our hypothesis was that one or more of the interventions would acutely improve the balance.
Methods
Subjects
Eighteen healthy able-bodied subjects (4 males) were included in the study. The participants had a mean age of 27.6 years (21–48 years) and were recruited from an educational facility in the Capital Region, Denmark and among family and friends of the authors. All participants gave their informed written consent prior to inclusion in the study. The participants were treated according to the Helsinki declaration and they were free to withdraw their consent at any time. Furthermore, we monitored the results over the course of the study and were particularly aware about negative adverse effects. The participants reported no adverse effects and no participants withdrew from the study. This study was conducted as a project with the University College Capital, School of Physiotherapy, Denmark and according to Danish legislation projects of this kind are not subject to ethical assessment as long as they are not invasive or investigating participant sensitive information.
Interventions
As a means of stimulating the proprioception on the sole of the foot, three different interventions were applied: A massage ball (), an individually fitted insole, and Kinesio® tape was used. For the massage ball-intervention, participants were asked to sit on a chair with one foot on the ball (shoes and socks off), and told to roll the ball around so that all of the foot was stimulated. This process was supervised by one of the test leaders and corrected if unsatisfactory. The stimulation of the foot sole continued for five minutes.
Figure 1. The massage ball.

The second intervention was a set of insoles of the brand SuperSole (Clinical Innovation, Hedehusene, Denmark). Prior to the moulding of the insole, the participant was asked to stand on a set of cushions. With the participant standing weight bearing on the cushions, the heated insoles were moulded by hand to fit the foot of each participant (). During the testing, the insoles of the participants’ shoes were exchanged with the individually moulded insole.
Figure 2. The insole moulding process.

Kinesio® tape has previously been found to increase the proprioception around the ankle [Citation14]. Therefore, this taping intervention was also included in the present study. For the Kinesio® tape-intervention, participants were asked to stand with one knee on a chair. Two Kinesio® tape strips were used for each application, one fan-cut and one I-strip (both 22,5 × 5 cm). The base of the fan-cut was placed without stretch on the plantar aspect of the heel. The fans were applied with moderate to maximal stretch on the sole of the foot. The first fan was placed in the direction of the first toe and the fourth fan was placed in the direction of the fifth toe. The remaining two fans were placed 1/3 from the first and fourth fan respectively. The base of the I-strip was placed without stretch on the lateral edge of the foot approximately five cm proximally from the metatarsophalangeal-joint of the fifth toe (). Moderate to maximal stretch was applied to the tape as it was placed with direction towards the medial malleolus.
Figure 3. The Kinesio® tape application.

All participants were tested with all three interventions. We randomised the order of the interventions for each participant. Combining the three interventions gave us six different orders of interventions to randomise. This was done by rolling a dice prior to the arrival of each participant. The eyes on the dice represented the combination that the participant was to follow. Whenever an order of interventions had been used three times, it was closed and not used again.
Balance testing
To evaluate the balance of the participants, we used an instrumented balance board (MiniBoard, Sensamove, Groessen, The Netherlands). The balance board appears to be a conventional wobble board (). However, the instrumentation makes it interactive and allows the user to follow the centre of pressure on a screen as a red dot.
Figure 4. The experimental setup.
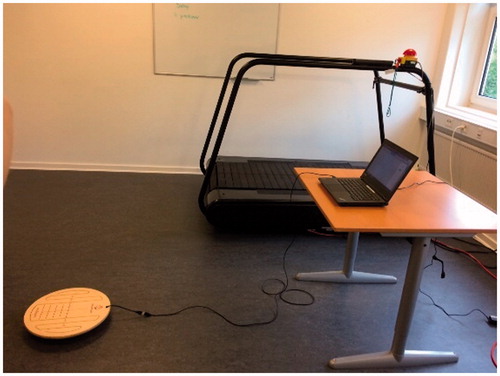
During the tests the participants could follow their movements on the wobble board via the red dot on the screen. For the tests a target area was displayed on the screen, and participants were asked to keep the dot within the target circle (). The participants performed the tests standing on the wobble board on one leg with their own shoe on and hands across the chest. During the testing of the insole intervention the removable sole was taken out of the shoe and replaced with the custom-made insole. Each participant was allowed three practice trials on one leg, during which they were asked to select their subsequent test leg. After the practice sessions, participants had to complete four balance test on the wobble board. Each of the four tests was performed with the target circle in a different position on the screen (45°, 135°, 225° and 315°). Participants completed three trials on every target circle position with a duration of 20 seconds each for all three interventions. A trial was discarded if the balance was lost, the subject touched anything with the hands or touched the ground with the other foot. In order to reduce any potential carry-over-effect between the interventions, the participants were asked to take a five-minute break between the trial bouts. The outcome of the trials was the percentage of the time that the dot was within the target circle. The overall average percentage including all positions for each target circle position was used for comparison between interventions. Also, analyses of inversion and eversion directions were performed. Differences between right and left leg trial were accounted for by reversing the placement of the target circle. Hence, the mirrored anatomy between right and left leg did not interfere with the results.
Figure 5. The participants were asked to keep the dot within the target circle.

A one-way ANOVA was applied to test for statistically significant differences. A number of Tukey-Kramer corrected post hoc test were then performed to determine which groups were significantly different. Level of significance was set at p ≤ .05.
Results
Selected demographic and bodily values are noted in .
Table 1. Demographic data for the participants.
The ANOVA rejected the nil-hypothesis at p ≤ .05, therefore the post hoc t-tests were performed. Overall percentage scores are noted in . The insole intervention was significantly better than the baseline measurement (p = .03). There were no significant differences between any of the remaining interventions.
Table 2. Overall percentage scores of time spend within target circle.
The results divided on inversion and eversion are noted in . The insole intervention was significantly better in the inversion direction than baseline and there was a near-significant effect of the massage ball in the inversion direction compared to baseline (p = .06). There were no other differences between interventions and baseline in inversion or eversion directions, nor did we find any differences between the interventions.
Table 3. Average percentage scores divided on inversion and eversion of the ankle.
Discussion
In the present study, we investigated three different interventions with a theoretical potential for improving standing balance. We confirmed our hypothesis and found that an individually fitted insole significantly improved standing balance measured on an instrumented wobble board. Kinesio® tape and stimulation with a massage ball did not improve balance significantly compared with the baseline. There was no significant difference between the interventions. However, the three interventions differed in the way they stimulated the proprioception. The massage ball provided stimulation while it was in contact with the sole of the foot. The contact between foot and ball ceased prior to the balance tests. Therefore, this intervention was based on the notion that some of the proprioceptive effect would last throughout the tests even though the stimulation had stopped. There was no indication in the data that the effect wore off over the course of testing. The Kinesio® tape was glued to the sole of the foot, allowing the tape to work throughout the tests. Therefore, the assumed proprioceptive stimuli from the tape was present during the testing. However, the Kinesio® tape is very elastic and is not designed to provide much mechanical stability or support. Therefore, the only effect was the assumed proprioceptive stimulus. The insoles was the only intervention with a potential mechanical support. The massage ball did not provide any mechanical support during the tests, and the level of mechanical support in the Kinesio® tape is thought to be insignificant. However, the insoles did support the medial longitudinal arch somewhat. The fact that there was support to control the inversion direction during tests, could be an explanation for the significant difference between the insole and the baseline measurements. Another explanation could be that the insole was in contact with a larger area on the sole of the foot than the Kinesio® tape and therefore allowed more proprioceptive input. We constructed the massage ball intervention to stimulate the whole foot sole and this intervention had a near-significant effect compared to baseline in the inversion direction (p = 0.06). Therefore, the authors lean towards the latter explanation of the effect of the insoles. The stimulation on the entire foot sole seemed to have potential for improving standing balance. This subject should be investigated further in future studies.
The effect of proprioceptive interventions on the foot to improve the standing balance has not been the subject of much research previously. However, the findings in the current study does concur with what has been found earlier. Steinberg et al. [Citation11,Citation12] found that a textured insole improved the ankle proprioception but only improved postural balance in males. Fayson et al. [Citation15] found that a lateral ankle sprain Kinesio® tape increased the ankle stiffness but did not increase the dynamic balance. However, this was done on the ankle and not the foot itself. In a population of elderly adults, Vaillant et al. [Citation16] found that manual massage and joint mobilisation improved performance in Timed Up and Go and One Legged Balance statistically and clinically significant compared to a control group that received a placebo intervention. The authors argumented that the increased somatosensory information could explain the effect they found. In the present study, the underlying argument was that the increased stimulation of the plantar sole could potentially increase balance performance. We have shown that the individually moulded insoles did improve standing balance, but none of the other interventions did. However, this does not mean that the effect was a consequence of the increased proprioceptive input. The mechanism may also be of a mechanical nature. Based on the data from the present study we cannot conclude anything in that regard.
There are some limitation to the study. In the randomisation process, the baseline measurement was not included. This could potentially induce a learning bias towards all interventions seeming better than the baseline measurements. Based on the data from the present study this could have added to the effects. Furthermore, the participants only received three practice trials. This may not have been enough to make them feel comfortable with the setup. This could therefore also have contributed to the effect via a learning bias.
In addition, this study was performed on healthy young adults with no recent history of balance issues. Therefore, the results can not be transferred directly to patients with balance impairments, but future research should investigate the effects of the present interventions on balance impaired adults.
Conclusion
We found that an individually moulded insole improved the one legged standing balance. Neither Kinesio® tape or self-massage with a massage ball on the plantar sole proved to improve balance.
Disclosure statement
Henrik Koblauch has previously been employed with Clinical Innovation (2007–2008), which is the Danish distributor of SuperSole.
References
- Fabre JM, Ellis R, Kosma M, et al. Falls risk factors and a compendium of falls risk screening instruments. J Geriatr Phys Ther. 2010;33:184–197.
- Maki BE, Holliday PJ, Topper AK. A prospective study of postural balance and risk of falling in an ambulatory and independent elderly population. J Gerontol. 1994;49:M72–M84.
- Haider S, Luger E, Kapan A, et al. Associations between daily physical activity, handgrip strength, muscle mass, physical performance and quality of life in prefrail and frail community-dwelling older adults. Qual Life Res. 2016;25:3129–3138.
- Han J, Anson J, Waddington G, et al. The Role of Ankle Proprioception for Balance Control in relation to Sports Performance and Injury. Biomed Res Int. 2015;2015:842804. doi:10.1155/2015/842804.
- Bouaziz W, Lang PO, Schmitt E, et al. Health benefits of multicomponent training programmes in seniors: a systematic review. Int J Clin Pract. 2016;70:520–536.
- Shumway-Cook A, Woollacott MH. Motor control: theory and practical applications. 2. ed. Philadelphia: Lippincott Williams & Wilkins; 2001.
- Fitzpatrick R, McCloskey DI. Proprioceptive, visual and vestibular thresholds for the perception of sway during standing in humans. J Physiol. 1994;478: 173–186.
- Colledge NR, Cantley P, Peaston I, et al. Ageing and balance: the measurement of spontaneous sway by posturography. Gerontology 1994;40:273–278.
- Goble DJ, Coxon JP, Van IA, et al. Brain activity during ankle proprioceptive stimulation predicts balance performance in young and older adults. J Neurosci. 2011;31:16344–16352.
- Perry SD. Evaluation of age-related plantar-surface insensitivity and onset age of advanced insensitivity in older adults using vibratory and touch sensation tests. Neurosci Lett. 2006;392:62–67.
- Steinberg N, Waddington G, Adams R, et al. The effect of textured ballet shoe insoles on ankle proprioception in dancers. Phys Ther Sport. 2016;17:38–44.
- Steinberg N, Waddington G, Adams R, et al. Use of a Textured Insole to Improve the Association Between Postural Balance and Ankle Discrimination in Young Male and Female Dancers. Med Probl Perform Art. 2015;30:217–223.
- Hijmans JM, Geertzen JH, Dijkstra PU, et al. A systematic review of the effects of shoes and other ankle or foot appliances on balance in older people and people with peripheral nervous system disorders. Gait Posture. 2007;25:316–323. doi:10.1016/j.gaitpost.2006.03.010.
- Murray H, Husk L. Effect of KinesioTM taping on proprioception in the ankle. J Orthop Sports Phys Ther. 2001;31:A1–44.
- Fayson SD, Needle AR, Kaminski TW. The effects of ankle Kinesio taping on ankle stiffness and dynamic balance. Res Sports Med. 2013;21:204–216.
- Vaillant J, Rouland A, Martigne P, et al. Massage and mobilization of the feet and ankles in elderly adults: effect on clinical balance performance. Man Ther. 2009;14:661–664.