
ABSTRACT
High quality ultrasound is required for evaluating carpal tunnel dynamics. The purpose of this study was to subjectively assess ultrasound video quality of the carpal tunnel with two commonly used coupling media (coupling gel, 7 mm standoff pad) in two wrist positions (0° neutral, 30° flexion) over the entire time course of a pinch grip. Seventeen participants completed a pinch grip while their carpal tunnel was scanned with ultrasound. The ultrasound videos were graded by two independent reviewers using 10-point scales encompassing median nerve detail, resolution, and total video quality. Intra- and inter-rater reliability were highest for median nerve detail (ICCs>.85). Ultrasound videos in the 0° neutral wrist condition resulted in significantly greater ratings of nerve detail compared to those in 30° wrist flexion. Future studies may benefit from a more customised approach to standoff pad thickness during dedicated analysis of the median nerve in a neutral wrist position.
Introduction
Ultrasound is used in the clinical diagnosis of carpal tunnel syndrome as well as the biomechanical analysis of carpal tunnel structures. Clinically, median nerve (MN) cross-sectional area obtained from B-mode ultrasound, nerve stiffness via shear wave elastography, and blood flow within the wrist from Doppler ultrasound have been investigated for their diagnostic potential (Lin et al. Citation2019, Citation2022). Biomechanical analyses also involve B-mode or compound mode imaging of the MN before and after a finger movement or a gripping task to quantify deformation, including changes in nerve width, height, circularity, and cross-sectional area (van Doesburg et al. Citation2012; Tat et al. Citation2013; Loh et al. Citation2016; Cowley et al. Citation2017; Turcotte and Kociolek Citation2021). For example, Turcotte and Kociolek (Citation2021) found that MN cross-sectional area and circularity changed following a forceful and repetitive tripod grip. Biomechanical analyses enable researchers to elucidate the complex mechanisms causing compression of the MN (Tat et al. Citation2013; Cowley et al. Citation2017; Turcotte and Kociolek Citation2021). However, to develop a greater understanding of both the healthy and pathological carpal tunnel, continued research is needed to investigate carpal tunnel dynamics throughout the entire time course of finger movements and gripping tasks.
The utility of measuring MN deformation depends on ultrasound image quality throughout the task to ensure accurate and reliable outcomes. For example, to derive nerve cross-sectional area and circularity, b-mode or compound mode images are typically imported into an image processing software that enables manual tracing of the nerve’s borders (Loh et al. Citation2016; Cowley et al. Citation2017). As such, image perception, including the ability to differentiate the borders of adjacent carpal tunnel structures, plays an important role in accurate and reliable measurements (Fowler et al. Citation2015). However, ultrasound analysis of the carpal tunnel throughout a gripping task poses several unique challenges that may affect image quality. The uneven contours of the wrist as well as the palmar-dorsal displacement of the finger flexor tendons during a dynamic assessment make it difficult to maintain coupling between the transducer and the wrist. Palmar-dorsal displacement of the tendons and nerve within the carpal tunnel may further result in these structures moving away from the focal zone, impacting resolution. Variation in participant carpal tunnel anatomy may also create differences in image quality (Crass et al. Citation1987; Nam et al. Citation2021). Ultrasound image artefacts such as anisotropy and section-thickness artefact may result from these scanning challenges and degrade image quality (Baad et al., Citation2017; Wu et al., Citation2020), ultimately reducing the accuracy of any biomechanical measurements.
While recent advances in artificial intelligence show very promising applications for the automatic assessment of MN morphology (Wu et al. Citation2021; Di Cosmo et al. Citation2022), many biomechanical assessments of the carpal tunnel through ultrasound are still performed manually (Cowley et al. Citation2017; Loh et al. Citation2019; Moon et al. Citation2020). Accordingly, subjective assessment of image quality is important to characterise authentic human perception. Image quality obtained between different ultrasound machines or coupling media is often assessed subjectively by reviewers through the use of a grading scale (Aziz et al. Citation2018; Yambot et al. Citation2018; Mount et al. Citation2021). A grading scheme encompassing structure detail, image resolution, and total image quality has been used extensively (Aziz et al. Citation2018; Binkowski et al. Citation2014, Blaivas et al. Citation2002; Riguzzi et al. Citation2017; Shapiro et al. Citation1998).
The purpose of this study was to subjectively assess ultrasound image quality over the entire time course of an active pinch gripping task; images were obtained using two media regularly used to maximise acoustic coupling (gel and standoff pad) and in two common wrist positions (0° neutral and 30° flexion) used in carpal tunnel analyses (Wilson et al. Citation2017; Ehmke et al. Citation2021; Turcotte and Kociolek Citation2021). We hypothesised that image quality would be greater in 0° neutral compared to 30° flexion of the wrist. We also hypothesised that a standoff pad would improve image quality, particularly in 30° wrist flexion.
Materials and methods
Participants
Seventeen healthy participants provided written informed consent prior to completing this study, which was approved by the Nipissing University Research Ethics Board (File # 102857). The exclusion criteria included comorbidities to carpal tunnel syndrome and any injury or pathology that may affect carpal tunnel mechanics (Racine et al. Citation2023; Turcotte and Kociolek Citation2021).
Experimental setup
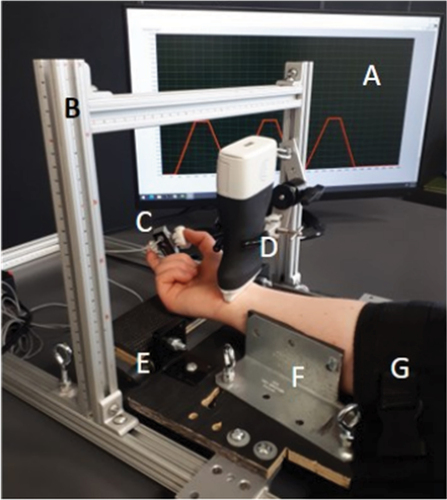
Participants were seated at a table with their dominant upper arm in approximately 0° of abduction, elbow flexed to 120°, and forearm fully supinated and supported within the testing apparatus (). A custom probe holder supported the linear array ultrasound transducer (L15, Clarius Mobile Health, Vancouver, BC) on the participant’s wrist in line with the distal wrist crease (Filius et al. Citation2015). Commercial coupling gel (Aquasonic, Parker Laboratories, Fairfield, NJ) and a standoff pad (Aquaflex, Parker Laboratories, Fairfield, NJ) cut to a depth of 7 mm (Loh et al. Citation2016) were applied to each participant’s wrist during ultrasound scans. The participant interacted with a grip dynamometer (MLP-75, Transducer Techniques, Temecula, CA) with a grip span of 4.5 cm and a sample rate of 1000 Hz to perform maximal voluntary exertions (MVE) as well as various pinch grip trials with the index finger and thumb in opposition. A computer monitor provided force feedback (LabVIEW 14.0, National Instruments Corp, Austin, TX).
Figure 1. Custom built testing apparatus supporting the right arm of a participant during a two-finger pulp pinch grip. Set-up includes (A) monitor displaying force profiles, (B) 80/20 aluminium extrusion and linear motion components, (C) dynamometer, (D) probe holder, (E) hinge allowing for wrist flexion, (F) metal brackets supporting forearm, (G) Velcro strap holding forearm in supination.
Experimental protocol
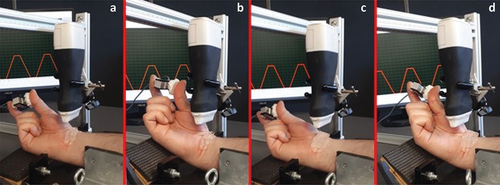
Each participant performed three pinch MVE trials (Racine et al. Citation2023; Turcotte and Kociolek Citation2021). Next, a template consisting of three trapezoidal shaped force profiles was constructed in LabVIEW to reach 40% of the participant’s MVE (Racine et al. Citation2023). Each subsequent trial involved pinch gripping three times while tracing the trapezoidal force template shown on a monitor. The force template consisted of a 2.5 s ramp up to 40% MVE, 1.5 s plateau at 40% MVE, 2.5 s ramp down to 0% MVE, and a 1.5 s pause between each of the three force profiles. In total, participants completed four pinch trials corresponding to the following conditions: 0° wrist flexion with coupling gel, 0° wrist flexion with standoff pad, 30° wrist flexion with coupling gel, and 30° wrist flexion with standoff pad ().
Figure 2. Four experimental conditions: (a) 0° wrist flexion with coupling gel, (b) 30° wrist flexion with coupling gel, (c) 0° wrist flexion with standoff pad, and (d) 30° wrist flexion with standoff pad.
Data collection
The ultrasound system scanned at 24 frames per second in compound mode with an acquisition frequency of 14 MHz. Ultrasound depth was adjusted based on the medium used and the participant’s individual carpal tunnel anatomy so that the focal point was in line with the MN. Gain was optimised for the first image capture of each participant and left in place for subsequent captures (Mount et al. Citation2021). A static image of the carpal tunnel was captured at the beginning of each condition. Subsequently, a 30-second Cine-loop of the transverse carpal tunnel was captured over the entire time course of the pinching task in each of the four experimental conditions. In total, four static images and four 30-second videos were captured for each participant. All ultrasound images and videos were collected by the lead author (D.B) for scanning consistency. The ultrasound collection was overseen by the corresponding author (A.M.K), who has 10 years of experience in carpal tunnel ultrasound collection.
Data analysis
Static ultrasound images were imported into ImageJ (v1.53k, National Institutes of Health, Bethesda, MD) and the MN was traced using the polygon tool by following its hyperechoic border (Racine et al. Citation2023; Turcotte and Kociolek Citation2021). The distance from the nerve’s centroid to the: (a) skin, (b) transducer head, and (c) focal point, were all measured. Next, the 30-second videos were de-identified to remove any evidence of the coupling media (Mount et al. Citation2021). Twelve videos from three participants were selected from the larger data collection for a training protocol. The remaining 56 videos from 14 participants were used to determine image quality in this study, which were presented in pairs (side-by-side) on the same screen to facilitate grading (Supplemental 1). Two independent biomechanists with graduate level experience in ultrasound-based carpal tunnel research served as reviewers of ultrasound video quality. Both reviewers were blind to the research with no knowledge of the study. Video quality grading was facilitated by three, 10-point scales encompassing MN detail, resolution, and total video quality in Supplemental 2 (Shapiro et al. Citation1998; Blaivas et al. Citation2004; Aziz et al. Citation2018).
Both reviewers underwent an identical training protocol to become familiarised with the scales and spectrum of video quality, in which the reviewers graded randomised videos using the three scales, with grading performed twice on separate days. Following the training sessions, the reviewers graded the remaining 56 videos to determine scores of video quality. The videos were presented in three separate clusters with breaks between each cluster. The presentation order of the three clusters as well as the video order within each cluster were randomised for each reviewer (Hemmsen et al. Citation2010). Both reviewers viewed and graded the ultrasound videos using the same 23.8” monitor (P2419H, Dell, Round Rock, TX).
Statistical analysis
Intra-rater reliability was assessed with intra-class correlations (ICCs) and 95% confidence intervals for the two training sessions based on a single-measures, absolute-agreement, 2-way mixed-effects model. Similarly, inter-rater reliability was determined from ICC estimates and 95% confidence intervals for both the training and the formal grading sessions based on a single-measures, consistency, 2-way random-effects model (Koo and Li Citation2016). Repeated-measures ANOVAs (α = 0.05) were conducted for each image quality parameter (MN detail, resolution, and total quality) as well as each depth measurement (skin to nerve, transducer to nerve, and focal point to nerve) to determine the effects of coupling media and wrist position. Bonferroni-corrected pairwise comparisons determined the location of significant main effects or interactions. All analyses were performed using SPSS (v28, IBM, Armonk, NY).
Results
Intra- and inter-rater reliability
ICCs and 95% confidence intervals for intra- and inter-rater reliability are presented in , which ranged from good to excellent for the scale of MN detail. ICCs for resolution and total video quality ranged from poor to excellent.
Table 1. Intraclass correlation coefficients (ICCs) and 95% confidence intervals for intra- and inter-rater reliability.
Ratings of video quality
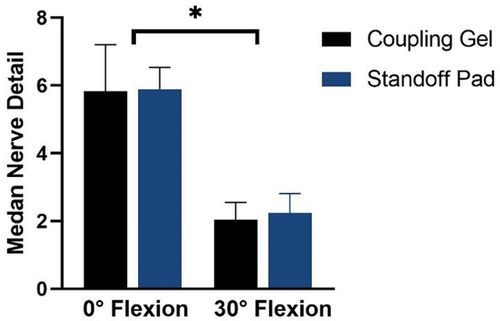
The 0° neutral wrist position resulted in significantly greater MN detail than 30° wrist flexion (F1,13 = 35.87, p=<0.001, ES = 0.73). Media had no effect on nerve detail ().
Figure 3. Mean (±95% CI) of median nerve detail (no units) obtained by scanning through coupling gel and a standoff pad in 0° neutral and 30° flexion wrist positions.
Depth measurements
There was a significant main effect of media on distance between the transducer head and MN (F1,16 = 319.99, p=<0.001, ES = 0.95), demonstrating that despite any pressure applied to the standoff pad by the ultrasound and subsequent compression, the standoff pad maintained a greater scanning depth. However, there was no significant difference in the distance between the MN and focal zone between the two media.
Discussion
Image quality plays a key role in accurately measuring carpal tunnel dynamics. In this study, carpal tunnel video quality throughout a dynamic pinch grip task was subjectively assessed by two blinded, independent reviewers. Intra- and inter-rater reliability were both good to excellent for MN detail (Koo and Li Citation2016); however, more work is needed on the measures of resolution and total video quality, which ranged from poor to excellent. To the best of our knowledge, this is the first study to assess the reliability of this commonly used grading scheme. In accordance with the hypothesis, the 0° neutral wrist position generated significantly greater MN detail compared to 30° wrist flexion. Unfortunately, the 30° wrist flexion condition resulted in lower quality images due to the exaggerated curvature of the palmar wrist tendons, leading to difficulties maintaining transducer contact with the wrist. These results suggest that researchers should focus carpal tunnel analyses on the nerve in a neutral wrist position when participants or patients are asked to perform a finger movement or grip task to assess carpal tunnel dynamics.
Despite the purpose of the standoff pad to bring the MN more in-line with the focal point (Crass et al. Citation1987; Biller and Myer Citation1988; Moudgil et al. Citation2021), the 7 mm standoff pad failed to accomplish this. A one-size-fits-all approach negated this attribute of the standoff pad, suggesting that a more customised approach to standoff pad thickness is required to appropriately position an individual’s target structure within the focal point. In addition, future research may benefit from continued exploration of artificial intelligence to assess ultrasound image quality and for the calculation of ultrasound based biomechanical measurements of MN deformation and displacement.
Supplemental Material
Download MS Power Point (12 MB)Supplemental Material
Download MS Word (13.1 KB)Acknowledgements
The authors would like to acknowledge Amanda Farias Zuniga, PhD and Gabrielle Racine, MSc for their roles as reviewers of video quality in this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author, A.M.K., upon reasonable request.
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/21681163.2024.2312171
Additional information
Funding
Notes on contributors
Denise Balogh
Denise Balogh is a PhD student in the Canadian Centre for Rural and Agricultural Health within the Department of Medicine at the University of Saskatchewan. Her research interests include occupational ergonomics with a focus on the wrist and shoulder.
Michelle Campbell
Michelle Campbell is a MSc student in the Sensory-Movement Behaviour Laboratory within the School of Physical and Health Education at Nipissing University. Her research interests include sensory-motor behaviour of fine motor control skills, especially in relation to gripping.
Aaron M. Kociolek
Aaron M. Kociolek is an Associate Professor in Biomechanics and Ergonomics within the School of Physical and Health Education at Nipissing University. He received his PhD in Occupational Biomechanics from McMaster University in 2015. He has conducted both laboratory- and field-based research with an interest in elucidating injury mechanisms and preventing work-related musculoskeletal disorders of the distal upper limb. His current research uses kinesiological modalities, including ultrasound, motion capture, and electromyography to study neuromusculoskeletal interactions underlying mechanics and control of the wrist and hand.
References
- Aziz A, Dar P, Solorzano C, Muller MM, Salmon C, Salmon M, Benfield N. 2018. Cassava flour slurry as a low-cost alternative to commercially available gel for obstetrical ultrasound: a blinded non-inferiority trial comparison of image quality. BJOG-Int J Obstet Gy. 125(9):1179–5. doi: 10.1111/1471-0528.15123.
- Baad M, Lu ZF, Reiser I, Paushter D. 2017. Clinical significance of US artifacts. Radiogr. 37(5):1408–1423. doi: 10.1148/rg.2017160175.
- Biller DS, Myer W. 1988. Ultrasound scanning of superficial structures using an ultrasound standoff pad. Vet Radiol Ultrasound. 29(3):138–142. doi: 10.1111/j.1740-8261.1988.tb01764.x.
- Binkowski A, Riguzzi C, Price D, Fahimi J. 2014. Evaluation of a cornstarch-based ultrasound gel alternative for low-resource settings. J Emerg Med. 47(1):E5–E9. doi: 10.1016/j.jemermed.2013.08.073.
- Blaivas M, Brannam L, Theodoro D. 2004. Ultrasound image quality comparison between an inexpensive handheld emergency department (ED) ultrasound machine and a large mobile ed ultrasound system. Acad Emerg Med. 11(7):778–781. doi: 10.1197/j.aem.2003.12.030.
- Blaivas M, DeBehnke D, Sierzenski PR, Phelan MB. 2002. Tissue harmonic imaging improves organ visualization in trauma ultrasound when compared with standard ultrasound mode. Acad Emergency Med. 9(1):48–53. doi: 10.1111/j.1553-2712.2002.tb01166.x.
- Cowley JC, Leonardis J, Lipps DB, Gates DH. 2017. The influence of wrist posture, grip type, and grip force on median nerve shape and cross‐sectional area. Clin Anat. 30(4):470–478. doi: 10.1002/ca.22871.
- Crass JR, Pozniak MA, Baumann JL, Feinberg SB. 1987. A device to aid in ultrasound imaging. J Clin Ultrasound. 15(3):211–217. doi: 10.1002/jcu.1870150313.
- Di Cosmo M, Fiorentino M, Villani F, Frontoni E, Smerilli G, Filippucci E, Moccia S. 2022. A deep learning approach to median nerve evaluation in ultrasound images of carpal tunnel inlet. Med Biol Eng Comput. 60(11):3255–3264. doi: 10.1007/s11517-022-02662-5.
- Ehmke S, Farias Zuniga A, Keir PJ. 2021. Effect of force, posture, and repetitive wrist motion on intraneural blood flow in the median nerve. J Ultrasound Med. 40(5):939–950. doi: 10.1002/jum.15467.
- Filius A, Scheltens M, Bosch HG, van Doorn PA, Stam HJ, Hovius SER, Amadio PC, Selles RW. 2015. Multidimensional ultrasound imaging of the wrist: changes of shape and displacement of the median nerve and tendons in carpal tunnel syndrome. J Orthop Res. 33(9):1332–1340. doi: 10.1002/jor.22909.
- Fowler RJ, Hirsh D, Kruse K. 2015. The reliability of ultrasound measurements of the median nerve at the carpal tunnel inlet. J Hand Surg Am. 40(10):1992–1995. doi: 10.1016/j.jhsa.2015.07.010.
- Hemmsen MC, Petersen MM, Nikolov SI, Nielsen MB, Jensen JA 2010. Ultrasound image quality assessment: a framework for evaluation of clinical image quality. In: Proceedings of SPIE Med Imag; Mar 2010; San Diego (CA). p. 76290.
- Koo TK, Li MY. 2016. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 15(2):155–163. doi: 10.1016/j.jcm.2016.02.012.
- Lin T, Chang K, Wu W, Özçakar L. 2022. Ultrasonography for the diagnosis of carpal tunnel syndrome: An umbrella review. J Neurol. 269(9):4663–4675. doi: 10.1007/s00415-022-11201-z.
- Lin C, Chen I, Chang K, Wu W, Özçakar L. 2019. Utility of ultrasound elastography in evaluation of carpal tunnel syndrome: a systematic review and meta-analysis. Ultrasound Med Biol. 45(11):2855–2865. doi: 10.1016/j.ultrasmedbio.2019.07.409.
- Loh PY, Nakashima H, Muraki S. 2016. Effects of grip force on median nerve deformation at different wrist angles. PeerJ. 4(e2510):e2510. doi: 10.7717/peerj.2510.
- Loh P, Yeoh W, Muraki S. 2019. An overview of hand postures and aging on morphological changes of the median nerve. J Physiol Anthropol. 38(1):9. doi: 10.1186/s40101-019-0201-6.
- Moon H, Lee B, Park D. 2020. Change to movement and morphology of the median nerve resulting from steroid injection in patients with mild carpal tunnel syndrome. Sci Rep. 10(1):15607. doi: 10.1038/s41598-020-72757-2.
- Moudgil S, Singh L, Raina S. 2021. A substitute of ultrasound acoustic stand-off pad made from locally available material: an innovation to survive in resource limited conditions. Fortune J. 5(1):61–67. doi: 10.26502/acbr.50170150.
- Mount C, Taylor D, Skinner C, Grogan S. 2021. Intravenous fluid bag as a substitute for gel standoff pad in musculoskeletal point-of-care ultrasound. Mil Med. 188(5–6):e949–e952. usab422. doi:10.1093/milmed/usab422.
- Nam K, Peterson SM, Wessner CE, Machado P, Forsberg F. 2021. Diagnosis of carpal tunnel syndrome using shear wave elastography and high-frequency ultrasound imaging. Acad Radiol. 28(9):e278–e287. doi: 10.1016/j.acra.2020.08.011.
- Racine G, Holmes MWR, Kociolek AM. 2023. Time‐varying changes in median nerve deformation and position in response to quantified pinch and grip forces. J Orthop Res. 2023:1–9. doi: 10.1002/jor.25737.
- Riguzzi C, Binkowski A, Butterfield M, Sani F, Teismann N, Fahimi J. 2017. A randomised experiment comparing low-cost ultrasound gel alternative with commercial gel. Emerg Med J. 34(4):227–230. doi: 10.1136/emermed-2016-206169.
- Shapiro RS, Wagreich J, Parsons RB, Stancato-Pasik A, Yeh HC, Lao R. 1998. Tissue harmonic imaging sonography: evaluation of image quality compared with conventional sonography. Am J Roentgenol. 171(5):1203–1206. doi: 10.2214/ajr.171.5.9798848.
- Tat J, Kociolek AM, Keir PJ. 2013. Repetitive differential finger motion increases shear strain between the flexor tendon and subsynovial connective tissue. J Orthop Res. 31(10):1533–1539. doi: 10.1002/jor.22391.
- Turcotte KE, Kociolek AM. 2021. Median nerve travel and deformation in the transverse carpal tunnel increases with chuck grip force and deviated wrist position. PeerJ. 9:e11038–e11038. doi: 10.7717/peerj.11038.
- van Doesburg MHM, Henderson J, Yoshii Y, van der Molen ABM, Cha SS, An KN, Amadio PC. 2012. Median nerve deformation in differential finger motions: ultrasonographic comparison of carpal tunnel syndrome patients and healthy controls. J Orthop Res. 30(4):643–6486. doi: 10.1002/jor.21562.
- Wilson KE, Tat J, Keir PJ. 2017. Effects of wrist posture and fingertip force on median nerve blood flow velocity. Biomed Res Int. 2017:7156489. doi: 10.1155/2017/7156489.
- Wu W, Chang K, Hsu Y, Hsu P, Ricci V, Özçakar L. 2020. Artifacts in musculoskeletal ultrasonography: from physics to clinics. Diagn. 10(9):645. doi: 10.3390/diagnostics10090645.
- Wu C, Syu W, Lin M, Yeh C, Boudier-Reveret M, Hsiao M, Kuo P. 2021. Automated segmentation of median nerve in dynamic sonography using deep learning: evaluation of Model performance. Diagnostics. 11(10):1893. doi: 10.3390/diagnostics11101893.
- Yambot K, Dilay R, Mauhay J, Mendoza M, Caparas A, Dumaoal O. 2018. Comparison of KY-jelly and ultrasound transmission gel as coupling medium for ultrasound imaging. Asia P J Health Sci. 1:27–34.