
ABSTRACT
Following the current outbreak, the mpox virus (formerly: monkeypox virus) is a highly threatening pathogen with public health significance, although mpox is still considered a neglected disease. Previously confined mainly to Africa, the virus spread globally in 2022. However, knowledge about mpox is limited, causing a distorted perception of the disease. Therefore, this study aimed to collect all information on scientific mpox publishing and to analyse them according to their chronological, geographical, and epidemiological patterns. It was not until the global outbreak that the relatively small number of publications was replaced by the immense increase in annual publication numbers. The most important player is the USA with a central role in international networking. They collaborated mainly with the Democratic Republic of Congo, a primary endemic country where the first viral clades were determined. Nigeria and other African countries were also represented, although mainly in the form of co-authorships. The fact that few of the first authors are from low- or middle-economic countries demonstrates the need to promote equitable networking at the global level and their support for surveillance and targeted immunization programmes.
GRAPHICAL ABSTRACT

Introduction
As an emerging zoonotic disease, mpox is characterized as a neglected disease despite the epizootic nature and the risk of transmission also from human to human with a broad spectrum of mammal infections [Citation1]. The mpox virus is regarded as a highly threatening pathogen with public health significance [Citation2]. The frequency and geographical distribution have steadily risen in the last years [Citation1] culminating in the escalating outbreak in 2022. After the eradication of smallpox (SPX), it is considered the most important infection of the orthopoxvirus genus in humans [Citation2]. mpox virus, first isolated in 1958 from cynomolgus macaques, causes infections with clinical presentations similar to those of SPX [Citation3,Citation4]. The features of the pathology described to date may change due to the changing spectrum. So far, fever, severe headache, fatigue, myalgia and severe lymphadenopathy are the most common symptoms in the invasion phase [Citation1,Citation4,Citation5]. Encephalitis, pneumonitis, keratitis, and secondary bacterial infections were reported as possible complication [Citation5]. The natural host is still unknown [Citation2]. Therefore, a diagnosis based on clinical manifestations alone is not enough. Real-time PCR (polymerase chain reaction) is necessary for differentiation [Citation6].
Human cases were not reported until the 1972 [Citation7] but could be misdiagnosed earlier as other rash diseases [Citation1]. Rodents are the primary animal reservoir, despite the earlier mpox designation as monkeypox, which may have contributed to the emergence of the disease in humans [Citation8]. Also, for reasons of racism and stigma associated with the term monkeypox, the World Health Organization (WHO) in 2022 recommended instead the term mpox [Citation9].
Mpox is endemic in West and Central Africa (Clade I) / Congo Basin (Clade II) [Citation10], where virus clades with differential epidemiology and clinical manifestations were differentiated [Citation11]. Most mpox outbreaks originated in West Africa, where less severe forms of the disease occur (CFR = case fatality rate <1%) [Citation2]. The clades of the Congo Basin show the highest virulence (CFR up to 11%) [Citation2,Citation12]. Initially, secondary spread outside Africa was limited, as the endemic form is generally self-limiting [Citation5]. An alarming resurgence of mpox was indicated in 2022, confirmed by WHO reports in Africa and in non-endemic countries worldwide. The first case of this global outbreak was detected in a traveller from Nigeria in the UK on 6th May 2022 [Citation13]. In June 2022, 3413 cases were confirmed in 50 countries/territories were confirmed, 2933 cases (86%) reported in European countries. One death was reported in Nigeria [Citation14]. End of July 2022, the General Director of the WHO declared mpox as a “public health emergency of international concern (PHEIC)” [Citation15]. Analyses stated that the mpox virus is central to the outbreak and correlated with persons that were arriving from the Canary Islands [Citation10]. A total of more than 68,000 cases in 108 countries were confirmed in October 2022 [Citation16]. This outbreak might be influenced by the cessation of smallpox vaccination brought a decline in immunity in the population [Citation17]. Other explanations for increasing incidence are the more often exposure to animal reservoir species [Citation18] and the increased human-to-human transmission rate [Citation12]. Global interconnectedness, climate change, migration, and flight, also as a result of civil wars, deforestation and agriculture, also played a role [Citation19]. Advances in diagnoses also led to increased registration [Citation20].
Although the use of the SPX vaccine proved to be 85% effective in mpox, the vaccine itself may pose a health risk because it is a live vaccine administered through the skin [Citation21]. Recent studies of modified strategies have shown that these risks can be reduced by pre-exposure vaccination of high-risk patients [Citation22] or by the use of a new generation of smallpox vaccine such as the modified vaccinia Ankara (MVA) vaccine, an attenuated, non-replicating live vaccine [Citation23]. Immunity to mpox virus was achieved by SPX vaccination [Citation24] because the genetic characteristics were nearly identical [Citation25]. During the current outbreak the viruses were proved to carry distinct genetic variations for which the effect of vaccination still has to be evaluated but first results show that antibodies elicited by SPX vaccines can neutralize Clade II infection [Citation26].
Until now, knowledge of emergence, epidemiology, and ecology is missing. Hence, many aspects need to be clarified. Despite the long time since the discovery of the mpox virus, there are no standard guidelines for clinical management or approved treatment for mpox [Citation27].
Clinicians must also be aware of prevention, prophylaxis, and basic infection control [Citation28].
Knowledge on transmission is limited [Citation29]. Prior to the current outbreak, outbreaks were infrequently reported and poorly managed, leading to a distorted perception of the importance of the disease [Citation2]. Therefore, establishing cross-regional surveillance programmes and conducting targeted interdisciplinary studies is extremely necessary. A comprehensive understanding of past research activities, their incentives and barriers is essential for developing and implementing future studies to promote appropriate prevention and response measures. Because resource allocation depends on scientific evidence of gaps and needs, including at the regional level, this study contributes by identifying global “white spots” with unknown epidemiologic characteristics but a high estimated disease burden. The present study was conducted to assist the scientific community and all stakeholders with information on the global research patterns of mpox from chronological and geographic aspects.
Methods
Methodological platform and search strategy
The data source for this analysis is Clarivate's Web of Science (WoS) Core Collection, a comprehensive multidisciplinary high-demand online scientific database. It serves as default source for all studies embedded in the New Quality and Quantity Indices in Science (NewQIS) methodological platform [Citation30]. The NewQIS method has been applied in the past in a large number of bibliometric studies on various biomedical topics. To collect the meta-data of publications related to mpox research, the search terms were “monkey pox” OR “monkeypox”. They were used in the title, abstract, and keywords as included in the TOPIC search tool of WoS. Data retrieval was performed on 10/05/2022. Socioeconomic and epidemiological assessment data were collected in November and December 2022.
Data processing and analyses
Subsequently, the metadata were recorded in an MS Access database and sorted according to the analysis parameters. Data of the authors’ names and affiliations as well as the denomination of research areas had to be manually standardized or corrected. Country entries were cross-checked and updated with a contemporary list of countries or regional territories.
Subsequently, the articles’ metadata could be assessed by chronological and global geographical patterns: annual publication and citation numbers, publication numbers and citation rate of countries, most-cited publications, most frequently assigned research areas and their evolution over time, and keywords used. International collaborative partnerships and the proportion of first and single authorship by country were identified. National socioeconomic and epidemiological metrics were included for a more in-depth analysis of country participation in mpox research. For this purpose, the population size and gross domestic product (GDP) were used based on data from the UNESCO Institute of Statistics (UIS) [Citation31]. For countries for which UIS data were not available, World Bank data were used [Citation32]. The total number of confirmed new cases reported through November 2022 was used for an epidemiologic assessment of the countries’ research efforts on mpox [Citation16].
Visualization techniques
Density-equalizing map projections (DEMP) were performed to visualize the results of some country analyses. These cartograms are based on an algorithm developed by Gastner and Newman that follows the physical principle of osmotic pressure equalization [Citation33]. They distort the size of the countries depending on the analysed parameter. The countries with high values are enlarged and the countries with small values are reduced in size. This technique leads to the creation of a distorted map whose information is easy to capture. The VOSviewer was used to perform the cluster analysis of the keywords and visualize the results. The colour-coded nodes of the identified clusters are connected with lines symbolizing the level of co-occurrences [Citation34].
Limitation and strengths
First, the quality of all bibliometric analyses depends on the quality of the data source used. The WoS is one of the most important online databases that lists only journals that are equipped by an impact factor and rigorous peer review procedures. This results in a reduction in entries provided, but an increase in research standards and reliability. The English-bias of WoS is well-known and often discussed [Citation30]. Second, the best developed search term cannot guarantee inclusion of all publications. The approach must be weighted by increasing the size of the database and minimizing the inclusion of false entries. The newly defined term “mpox” was not included because it had not yet been introduced at the time of the analysis. Third, the interpretation of citation counts is subject to various limitations based on spurious or self-citations, limiting their validity as a measure of a publication's quality. The collection of socioeconomic or epidemiological data is not possible for all countries because the case numbers reported by each country are unreliable or unavailable.
Results
Based on the search term used, 1537 publications (n) on mpox were identified.
Chronological patterns
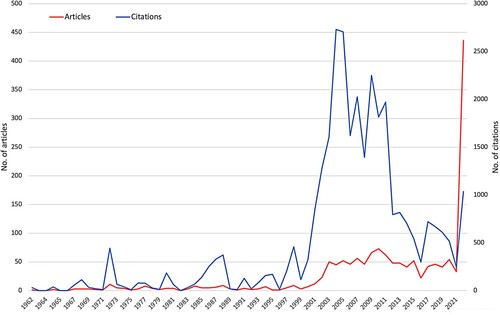
By October 2022, n = 436 publications (28.37%) were published. The first publication on mpox that was listed in WoS in 1962. In 2003, the first considerable increase in mpox publications can be seen that remained on a similar level until 2022 between 20 and 70 annual publications. With 2731 and 2705 citations, the publications of 2004 and 2005, respectively, received the most citations (c) until now. Further annual citation maxima can be seen: In 1972, the first peak (c = 444), followed by some smaller ones, in 2009 (c = 2250) and – again a smaller one – in 2017 (c = 720). By the time of the analysis, c = 1037 has already been reached in 2022 ().
Figure 1. Annual publication and citation numbers until 10/05/2022.
Geographical patterns
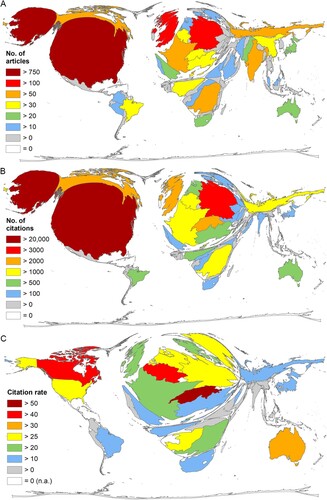
Of the total database, n = 1399 (91.02%) could be assigned to a country of origin and thus included in the analysis of publishing countries. The most frequently publishing country on mpox was the USA (n = 781), followed at a great distance by Germany (n = 119), and the United Kingdom (UK, n = 109). Unusually compared to other scientific topics [Citation30], the Democratic Republic of Congo (DRC, n = 79) ranked 4th, followed by Russia (n = 64). The second most frequently publishing African country was Nigeria (ranked 9th, n = 50) ((A)). The distribution of citations more or less follows that of publication numbers (USA: c = 20,896; Germany: c = 3165, Switzerland: c = 2741) ((B)). In terms of citation rate, Switzerland ranked first (cr = 54.82), followed by Canada (cr = 41.52), and Belgium (cr = 41.23) ((C)).
Figure 2. Publication output of countries. (A) Number of publications. (B) Number of citations. (C) Citation rate (threshold = 10 publications on mpox).
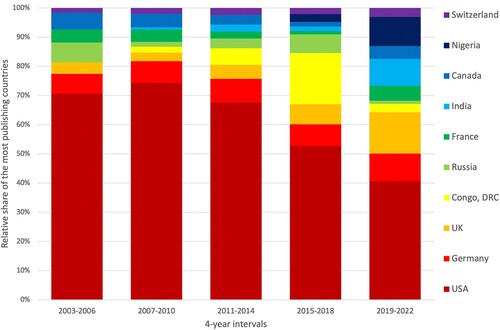
Considering the development of countries’ performances on mpox research over time, we see that the relative share of US mpox articles among the ten countries with the most publications decreased from 70.62% to 40.63%. In contrast, the relative share of the UK, India, and Nigeria increased over time (). China, ranked 15th regarding the total number of publications, climbed to 9th when considering only the last evaluation interval from 2019 to 2022.
Figure 3. Development of the relative share of the most publishing countries of mpox research in 4-year intervals from 2003 until 2022.
Socio-economic patterns
The evaluation of the calculation of the socio-economic ratios RPOP (number of articles on mpox / population size in 10 mill) and RGDP (number of articles on mpox / GDP in 10 bn US-$) resulted in the following rankings of the first five countries:
RPOP: Switzerland (RPOP = 57.37), Belgium (RPOP = 33.53), Congo (RPOP = 30.05) (Supp. (A)).
RGDP: CAR (RGDP = 43.71), DRC (RGDP = 14.64), Congo (RGDP = 13.57) (Supp. (B)).
The socio-economic ranking of countries with at least 10 articles on mpox (threshold) is shown in .
Table 1. Socio-economic ratios of countries with at least 10 articles on mpox, RGDP = Number of articles / Gross Domestic Product in 10 billion US-$, RPOP = Number of articles / Population in million inhabitants (sorted by RGDP).
Epidemiological patterns
Globally, 81,351 new mpox cases were confirmed through November 2022 (date of data collection) [Citation16]. A total of 58 deaths were confirmed worldwide, with the most occurring in the USA (14 deaths) and in Brazil (13 deaths). Seven people died in Nigeria, and four each in Ghana and Mexico.
The calculation of the quotients Cases / Articles (C/A) and Articles / Cases (A/C) resulted in the following rankings of the five leading countries:
Cases / Articles: Mexico (C/A = 548.67), Brazil (C/A = 312.44), Spain (C/A = 264.57) ((A)). This ranking highlights countries with high caseloads associated with a relatively low article performance.
Articles / Cases: Russia (A/C = 32), Egypt (A/C = 17), Iran (A/C = 15) ((B)). This ranking highlights countries with low caseloads associated with a relatively high article performance.
Figure 4. Number of registered cases of mpox [Citation45]. (A) Ratio of the number of mpox cases registered until November 2022 and the number of articles on mpox per country. (B) Ratio of the number of articles on mpox and the cases registered until November 2022. (C) Residual of linear regression between number of articles on mpox and new cases of mpox per country.
![Figure 4. Number of registered cases of mpox [Citation45]. (A) Ratio of the number of mpox cases registered until November 2022 and the number of articles on mpox per country. (B) Ratio of the number of articles on mpox and the cases registered until November 2022. (C) Residual of linear regression between number of articles on mpox and new cases of mpox per country.](/cms/asset/6e7bed53-5582-4b16-98bb-60578c72b650/temi_a_2210696_f0004_oc.jpg)
The linear regression between the number of articles and the number of cases registered by November 2022 for countries with at least one confirmed case and one article on mpox was significant (r2 = 0.82). The correlation between both parameters was also significant (Spearman, p = 0.0003).
The residuals of the linear regression are shown in (C). A distinction can be made between countries that produced comparatively more (negative values) or fewer articles (positive values) in relation to cases.
The number of international collaborations increased at the same rate as the annual number of articles over time. A total of n = 399 articles were registered that were authored by at least two countries. In 2022 (up to the retrieval date), 141 international collaborations have already been published. The most frequently collaborating partner countries and the share of collaborations in their total number of articles are listed in .
Table 2. Most productive bilateral collaborations on mpox (number of collaboration articles ≥ 10) and the percentage of collaborations in the number of articles on mpox of each country, DRC = Democratic Republic Congo.
The most productive partnership in mpox research was between the USA and the DRC. The USA wrote 30.86% of its articles in collaboration with another country, while the DRC wrote 92.40% of its articles in collaboration with another country. With the exception of Nigeria, the percentage of collaborations in low- or middle-income countries (LMIC) was generally much higher than in high-income countries (HIC) (). Russia produced only 15.62% of its articles (n = 64) together with another country (n = 10) ().
Figure 5. International collaborations (display threshold ≥ 3 collaboration articles). Numbers in brackets (articles on mpox / collaboration articles), DRC = Democratic Republic Congo.
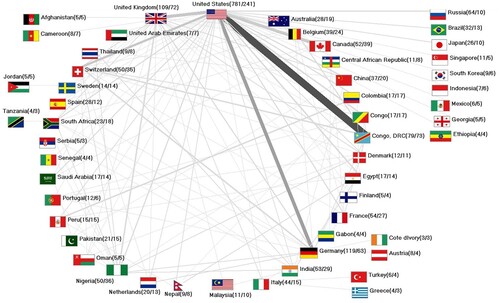
The percentage of first or single authorships among the countries also differs, mainly depending on their economic status. Developing countries, for example, occupy first or single authorship positions less frequently (). Only Nigeria has a higher share here as well, while Switzerland and Canada, as HICs, achieve a comparatively low share of first authorships.
Table 3. Number and percentage of first-authorships (FA) and single-authorships (SA) of most collaborating countries (sorted by number of FA), CAR = Central African Republic, DRC = Democratic Republic Congo.
Publishing institutions
Most institutions that published on mpox were from the USA: the Center for Disease Control & Prevention (CDC: n = 232), the National Institutes of Health (NIH: n = 100), and the US Army (n = 95). These were followed by the National Institute for Biomedical Research in the DRC (n = 41). All institutions with at least 20 articles on mpox are listed in the Supplement Table 1.
Looking at collaborations at the institutional level more closely, some US national collaborations and USA/DRC partnerships stood out. Here, the WHO emerged as an additional link between CDC and the DRC Ministry of Health (Supp. ).
Discussion
Mpox research and funding have been comparably low, consistent with its status as a neglected disease [Citation5]. The main results of this study show that this is reflected in the low number of articles until the current global outbreak in 2022 when the annual number of publications increased approximately tenfold. The USA occupies a central position in international cooperation, which has mainly taken place with the DRC. In addition to European countries, Nigeria and Russia ranked high. Authors from low-or middle-economy countries were mainly co-authors.
Discussion of chronological patterns
Our results show that after the initial very low annual publication numbers, there was a slight increase in 1972, accompanied by a significant increase in citation numbers. This was due to the first human infection in 1970, when a child was infected in the DRC.
The relationship between the timing of the emergence of mpox cases in non-Africa and the increase in publication numbers is demonstrable. The results of this study show a publication peak in 2003 attributable to the mpox outbreak in the USA. The interest in mpox research during this period was also reflected in the sharp increase in the numbers of citations in the following years. The decline in citation numbers after 2011, due in part to short citation durations in later years, was briefly interrupted in 2017/2018 when another mpox outbreak occurred in the UK, indicating increasing scientific interest. Exceptions, forced by small annual peaks in the number of citations, were recorded in 1980, 1988, and 1998. After the eradication of SPX in 1980, mpox virus was described as the major orthopoxvirus in 1987 [Citation35,Citation36]. These events contributed to the respective citation peaks of those years. The peak in 1998 indicates the re-emergence of mpox in African countries where large outbreaks occurred in 1996 and 1997. The results of a study from this period showed that most secondary infections were due to human-to-human transmission [Citation37]. Given these contexts, it becomes clear that human epidemiology and outbreaks, particularly outside Africa, stimulated scientific interest in mpox events, albeit on a time-limited scale. A comparable publication phenomenon can be observed, for example, in the development of coronavirus research, which was only briefly spurred by earlier outbreaks and led to an explosion of research activity in the wake of the global COVID-19 pandemic [Citation38].
Geographical patterns
What is not unusual or unique for mpox research is the fact that the USA as well as Germany and the UK are top ranked in mpox research. The Swiss publication performance on mpox, which resulted in a top ranking in terms of citation rate and the demographic ratio, was dominated by the influence of research with WHO participation. More striking is the high ranking of Russia. After the eradication of SPX in 1980, the agent of variola virus was held captive in a Russian (VECTOR: State Research Center of Virology and Biotechnology) and a US laboratory [Citation39], which explains Russia's comparatively high and constant involvement in mpox research. China’s relatively low rank in mpox publications is also striking. China is only gradually increasing its mpox research activities compared to other research areas where it has often already overtaken the USA in publication rankings [Citation40].
The relationship between incidence and publication effort was evident not only in the trend of publication numbers, but also in the geographic context, as the parameters were significantly correlated at the country level. This fact comparatively sets back countries with a high number of current mpox cases, such as Mexico and Brazil, but underscores the particular importance of some African countries. In particular, the DRC and Nigeria, where mpox is endemic, achieve high publication numbers on mpox [Citation30]. In other scientific fields, there is rarely a high level of participation from developing countries. Only in research into diseases that are either limited to Africa or have an extremely high incidence there is a high level of participation by African countries evident. In the case of Ebola, e.g. Gabon was among the ten countries that published the most [Citation41].
Some LMICs are also at the top of the ranking in terms of the ratios of publication numbers to the economic power of the publishing countries (RGDP). The fact that mpox is endemic in Nigeria and the DRC [Citation29,Citation42] necessitates international collaboration with these countries to obtain a valid set of data for scientific analyses. In addition, the USA, through the CDC, provides technical and financial support to African institutions working on mpox. For example, the Nigerian Field Epidemiology and Laboratory Training Program (NFELTP), hosted by the Nigerian Center for Disease Control (NCDC) and the Federal Ministry of Health, is supported by the US CDC [Citation43]. After almost 40 years of no reported cases in Nigeria, mpox reappeared there in 2017, raising concerns of a new spread [Citation44], which has indeed now reached many parts of the world. Accordingly, the present results show that the Nigerian contribution to mpox research became visible during this period and subsequently increased. It is primarily coordinated by the NCDC. In contrast, the national mpox programme of the DRC, which has a long history in mpox epidemiology and research, is less well-funded and also heavily dependent on foreign donors.
The current mpox outbreak is driving research activities around the world and international scientific collaboration is increasing. The results of the network analysis show that the proportion of articles written in collaboration is significantly higher in countries with lower economic power. This is particularly true in Congo, the DRC, Peru, Colombia, and Egypt, where more than 80% of articles were written in international collaboration. In contrast, the average collaboration rate is about 25% [Citation40]. In scientific publications, the order in which authors are listed usually determines their role and function. First authors usually have a leading role and are the principal investigators. It has been demonstrated that in LMICs the share of single and first authorships is lower compared to countries with high economic power. The majority of first authorships and the generally high position of HICs in the global research landscape increase their influence on research strategies.
The results of this study thus show that LMICs, which are among the most affected countries in the world, need to be more involved in scientific planning and decision-making in the future. A network of equals is needed that benefits all partners and creates a win-win situation in the transfer of human, technical, and financial resources.
Conclusions
The results of this study show the global pattern of mpox research from 1962 to October 2022. This also reflects the recent outbreak expanding the affected African regions to many parts of the world. Initially, however, interest in the research was sparked by the emergence of mpox cases outside of African endemic areas. High-income countries were prompted to seek collaborative partners from highly affected African countries. Here, the USA played a key role, especially in collaboration with the Democratic Republic of Congo. Nevertheless, the participation of low- and middle-income countries, which is certainly higher here compared to other research topics, is mainly characterized by co-authorships. This underscores the leadership, responsibility, and direction giving that rests primarily with high-income countries. Therefore, the objective should be to achieve a greater balance in the planning and focus of research projects. The focus should not only be on epidemiological needs, but should also be broadened to include regional, historical, ethnic, and cultural characteristics of all participating countries, so that a win-win situation can be created for both better-resourced regions and regions with fewer available resource. This could be achieved by establishing long-term multinational collaborations, scientific exchange at the level of personnel and equipment, and funding targeted projects, to name just a few measures. Nevertheless, explicit solutions need to be concretized through dedicated scientific approaches.
Geological information
This study includes the global data of all countries that have published on mpox up to the time of the evaluation.
Supplemental Material
Download MS Word (2.1 MB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data underlying this article will be shared with the corresponding author upon reasonable request, provided the recipient has a Web of Science license.
References
- Parker S, Nuara A, Buller RML, et al. Human monkeypox: an emerging zoonotic disease. Future Microbiol. 2007 Feb;2(1):17–34.
- Sklenovska N, Van Ranst M. Emergence of monkeypox as the most important orthopoxvirus infection in humans. Front Public Health. 2018 Sep 4;6:241.
- Hatmal MM, Al-Hatamleh MAI, Olaimat AN, et al. Comprehensive literature review of monkeypox. Emerg Microbes Infec. 2022 Dec 31;11(1):2600–2631.
- WHO. World Health Organization, monkeypox, key facts; 2022 [cited 2023 Jan]. Available from: https://www.who.int/news-room/fact-sheets/detail/monkeypox
- Thornhill JP, Barkati S, Walmsley S, et al. Monkeypox virus infection in humans across 16 countries – April–June 2022. Lancet Neurol. 2022 Oct;21(10):872–872.
- Li Y, Zhao H, Wilkins K, et al. Real-time PCR assays for the specific detection of monkeypox virus West African and Congo Basin strain DNA. J Virol Methods. 2010 Oct;169(1):223–227.
- Ladnyj ID, Ziegler P, Kima E. A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo. Bull World Health Organ. 1972;46(5):593–597.
- Reynolds MG, Carroll DS, Karem KL. Factors affecting the likelihood of monkeypox's emergence and spread in the post-smallpox era. Curr Opin Virol. 2012 Jun;2(3):335–343.
- WHO. World Health Organization, WHO recommends new name for monkeypox disease; 2022 [cited 2023 Jan]. Available from: https://www.who.int/news/item/28-11-2022-who-recommends-new-name-for-monkeypox-disease
- Alcoba-Florez J, Muñoz-Barrera A, Ciuffreda L, et al. A draft of the first genome sequence of monkeypox virus associated with the multi-country outbreak in May 2022 from the Canary Islands, Spain; 2022 [cited 2022 Nov]. Available from: https://virological.org/t/a-draft-of-the-first-genome-sequence-of-monkeypox-virus-associated-with-the-multi-country-outbreak-in-may-2022-from-the-canary-islands-spain/864
- Likos AM, Sammons SA, Olson VA, et al. A tale of two clades: monkeypox viruses. J Gen Virol. 2005 Oct;86:2661–2672.
- Chen NH, Li GY, Liszewski MK, et al. Virulence differences between monkeypox virus isolates from West Africa and the Congo basin. Virology. 2005 Sep 15;340(1):46–63.
- GOV.UK. Monkepox cases confirmed in England – latest updates; 2022 [cited 2022 Oct]. Available from: https://www.gov.uk/government/news/monkeypox-cases-confirmed-in-england-latest-updates
- PAHO. Pan American Health Organization / World Health Organization, Epidemiological Update Monkeypox in non-endemic countries – 13 June 2022; 2022 [cited 2022 Nov]. Available from: https://www.paho.org/en/documents/epidemiological-update-monkeypox-non-endemic-countries-13-june-2022
- WHO. WHO Director General declares the ongoing monkeypox outbreak a Public Health Emergency of International Concern; 2022 [cited 2022 Oct]. Available from: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern
- Our_World_in_Data. Monkeypox data explorer; 2022 [cited 2022 Oct]. Available from: https://ourworldindata.org/explorers/monkeypox?tab=table&time=2022-05-24..latest&facet=none&Metric=Confirmed+cases&Frequency=Cumulative&Relative+to+population=false&country=~OWID_WRL
- Simpson K, Heymann D, Brown CS, et al. Human monkeypox – after 40 years, an unintended consequence of smallpox eradication. Vaccine. 2020 Jul 14;38(33):5077–5081.
- Rimoin AW, Mulembakani PM, Johnston SC, et al. Major increase in human monkeypox incidence 30 years after smallpox vaccination campaigns cease in the Democratic Republic of Congo. Proc Natl Acad Sci USA. 2010 Sep 14;107(37):16262–16267.
- Tehranchinia Z, Robati RM, Moravvej H, et al. Monkeypox disease with a focus on the 2022 outbreak; a narrative review. Arch Acad Emerg Med. 2023;11(1):e19.
- Li D, Wilkins K, McCollum AM, et al. Evaluation of the GeneXpert for human monkeypox diagnosis. Am J Trop Med Hyg. 2017;96(2):405–410.
- Hooper JW, Thompson E, Wilhelmsen C, et al. Smallpox DNA vaccine protects nonhuman primates against lethal monkeypox. J Virol. 2004 May;78(9):4433–4443.
- Merad Y, Gaymard A, Cotte L, et al. Outcomes of post-exposure vaccination by modified vaccinia Ankara to prevent mpox (formerly monkeypox): a retrospective observational study in Lyon, France, June to August 2022. Eurosurveillance. 2022 Dec 15;27(50):23–29.
- Kennedy JS, Greenberg RN. IMVAMUNE®: modified vaccinia Ankara strain as an attenuated smallpox vaccine. Expert Rev Vaccines. 2009 Jan;8(1):13–24.
- Zaeck LM, Lamers MM, Verstrepen BE, et al. Low levels of monkeypox virus-neutralizing antibodies after MVA-BN vaccination in healthy individuals. Nat Med. 2022 Oct 18;29:270–278.
- Shchelkunov SN, Totmenin AV, Babkin IV, et al. Human monkeypox and smallpox viruses: genomic comparison. FEBS Lett. 2001 Nov 30;509(1):66–70.
- Criscuolo E, Giuliani B, Ferrarese R, et al. Smallpox vaccination-elicited antibodies cross-neutralize 2022-monkeypox virus Clade II. J Med Virol. 2023 Mar 8;95(3):e28643.
- Petersen E, Kantele A, Koopmans M, et al. Human monkeypox epidemiologic and clinical characteristics, diagnosis, and prevention. Infect Dis Clin N Am. 2019 Dec;33(4):1027–10–+.
- Bryer J, Freeman EE, Rosenbach M. Monkeypox emerges on a global scale: a historical review and dermatologic primer. J Am Acad Dermatol. 2022 Nov;87(5):1069–1074.
- Brown K, Leggat PA. Human monkeypox: current state of knowledge and implications for the future. Trop Med Infect Dis. 2016 Dec 20;1(1):8.
- Groneberg DA, Klingelhofer D, Bruggmann D, et al. New quality and quantity indices in science (NewQIS): results of the first decade-project progress review. Scientometrics. 2019;121(1):451–478.
- UIS.Stat. Data 2017; 2022 [cited 2019 Nov]. Available from: http://data.uis.unesco.org/Index.aspx
- World_Bank. Population, total; 2021 [cited 2022 Dec]. Available from: https://data.worldbank.org/indicator/SP.POP.TOTL
- Gastner MT, Newman MEJ. Diffusion-based method for producing density-equalizing maps. Proc Natl Acad Sci USA. 2004 May 18;101(20):7499–7504.
- van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010 Aug;84(2):523–538.
- Hutson CL, Nakazawa YJ, Self J, et al. Laboratory investigations of African pouched rats (Cricetomys gambianus) as a potential reservoir host species for monkeypox virus. Plos Neglect Trop D. 2015 Oct;9(10):e0004013.
- McCollum AM, Damon IK. Human monkeypox. Clin Infect Dis. 2014 Jan 15;58(2):260–267.
- Heymann DL, Szczeniowski M, Esteves K. Re-emergence of monkeypox in Africa: a review of the past six years. Br Med Bull. 1998;54(3):693–702.
- Klingelhofer D, Braun M, Bruggmann D, et al. Coronavirus: an insight into global research until outbreak of COVID-19 and its implications for the future. J Glob Health. 2020 Dec;10(2):020508.
- Mucker EM, Hartmann C, Hering D, et al. Validation of a pan-orthopox real-time PCR assay for the detection and quantification of viral genomes from nonhuman primate blood. Virol J. 2017 Nov 3;14:210.
- NSF. National Science Foundation: publication output: U.S. trends and international comparisons. Executive summary; 2022 [cited 2023 Jan]. Available from: https://ncses.nsf.gov/pubs/nsb20214
- Quarcoo D, Bruggmann D, Klingelhofer D, et al. Ebola and its global research architecture-need for an improvement. Plos Neglect Trop D. 2015 Sep;9(9):e0004083.
- WHO. Monkeypox – United Kingdom of Great Britain and Northern Ireland; 2022 [cited 2022 Oct] Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON381
- TEPHINET. Nigeria field epidemiology and laboratory training; 2022 [cited 2022 Oct]. Available from: https://www.tephinet.org/training-programs/nigeria-field-epidemiology-and-laboratory-training-program
- Alakunle E, Moens U, Nchinda G, et al. Monkeypox virus in Nigeria: infection biology, epidemiology, and evolution. Viruses-Basel. 2020 Nov;12(11):1257.
- WHO. World Health Organization, multi-country monkeypox outbreak: situation update; 2022 [cited 2022 Nov]. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396