
ABSTRACT
The urgency of the problem under study is determined by the high prevalence of arterial hypertension among the indigenous minorities of the North in modern socio-economic conditions. The following article is aimed to evaluate the prevalence of behavioural arterial hypertension risk factors according to the results of single-step epidemiological research of Evenk people in the Republic of Sakha (Yakutia), Russian Federation. The leading approach to the study of this problem was the questioning of the population using the international questionnaire for behavioural risk factors (CYNDI). As a result of research, widespread smoking was found among native population (52.0% of men and 23.7% of women). The frequency of alcohol consumption among the male Evenki is comparable to that in the Yakut population, and among the female, the number is much lower. Evenks including young men belong to the physically inactive population. The frequency of arterial hypertension (AH) cases along with the factors listed above are significantly influenced by: marital status, employment, education, and housing conditions. Article materials may be useful for a differentiated approach in the development of prevention and rehabilitation programs for the indigenous peoples of the North.
Introduction
It is commonly known that there are 3 groups of risk factors for chronic non-communicable diseases – behavioural, biological and social.
The role of behaviour in healthcare is substantial and broad. The importance of behaviour regarding general health, health care and prevention has recently been recognized in the annual report of the National Prevention, Health Promotion and Public Health Council [Citation1]. It was noted that “the most effective approach to solving the main causes of death is to reduce and prevent the main risk factors, including physical activity, poor nutrition, tobacco use and excessive alcohol consumption.”
According to reports by many surgeons, smoking was the main cause of cancer, vascular and pulmonary diseases, and premature death [Citation2]. Life quality of smoking quitters significantly improved in contrast to smokers‘ [Citation3–Citation5]. Lack of physical activity plays a significant role in the aetiology and progression of the disease [Citation6–Citation8]. Randomized trials have shown that physical activity improves the life quality of elder generation [Citation9,Citation10]. Physical activity of 10,000 steps a day for 8 weeks reduced both systolic and diastolic blood pressure [Citation11].
Indigenous Minorities of the North (Indigenous Peoples) nowadays are less likely to adhere to the traditional way of life in the context of modern socio-economic development. Smoking, alcohol consumption, eating disorders lead to an imbalance in the main bodily functions of Indigenous Minorities. Alcohol became a part of the everyday life of Indigenous People relatively recently. The failure of the liver enzyme systems to metabolize exogenous ethanol results in a “quick” alcoholisation of the Northern minority compared to other ethnic groups [Citation12].
Until recent times, diseases such as coronary heart disease and arterial hypertension were rarely observed in the native inhabitants of Yakutia. In modern conditions of socio-economic development, such concepts as alimentary-dependent and alcohol-dependent diseases have appeared. This is indicated by the high rates of morbidity and mortality in the northern regions. At present, there are no data on the health status of the North indigenous population, since according to the Federal State Statistics Service of Yakutia and the Rosstat of the Russian Federation these indicators are published as part of administrative education along with other ethnic groups.
The purpose of this study was to assess the behavioural risk factors for arterial hypertension: smoking, alcohol consumption and physical activity among the indigenous minorities of the North.
Contents and methods
This study was worked on in 2015 in the framework of the “Assessment of the health status and quality of population life in the Oleneksky ulus – the territory of future activities for the rare earth metals (niobium) extraction” research. A study conducted 355 people over the age of 20 in the village of Jilinda, Olenek district of Yakutia, using the international questionnaire for behavioural risk factors (CYNDI) and the questionnaire SF-36. The questionnaire contained following sections: general information (marital status, education), family income, living conditions, employment, type of work, physical activity, questions about smoking status, consumption of alcoholic beverages and quality of life.
The prevalence of smoking was determined by the frequency of positive answers to the question about tobacco smoking and the number of cigarettes smoked per day.
The frequency of alcohol consumption was formed based on the respondents‘ answers to the questions: “how often did you drink beer, wine, fortified wines, hard drinks – once a week, a month, rarely or never.”
Criteria for physical activity (PA) were divided into four categories:
Physically inactive – persons who responded that they mostly sit at work or do not work, while walking less than 30 min a day and do not engage in physical activity at all during their free time;
Those with low levels of PA – those who responded that they mostly sit at work or do not work, while walking from 30 to 60 min a day and do not engage in physical activity during their free time;
Individuals who responded that they mostly walk or lift and carry light loads at work, or walk 60 to 90 min a day, or engage in physical activity during their free time from 1 to 4 days per day were considered to have average PA a week;
Persons who responded that they are engaged in heavy physical work or walk from 90 min a day or more or engage in physical activity during their free time 5 or more days a week were considered to have high levels of PA.
Blood pressure (BP) and heart rate were measured during the study. Blood pressure was measured twice on the right arm in a sitting position after 5 min of rest, the average of 2 measurements was taken into account. The heart rate was recorded on the right hand for 30 s. For AH in accordance with the recommendations of experts WHO/ISAH 1999 was taken the level of the systolic blood pressure (SBP) of 140 mm Hg and more or diastolic blood pressure (DBP) of 90 mm Hg and more.
The software package Statistica 10.0 (analysis of contingency tables; rank correlation analysis) was used as a software for statistical analysis of research materials. The critical level of statistical significance was 0.05.
The study was conducted without violation of ethical standards, with the approval of the local committee on biomedical ethics. Participants gave their written consent after they were informed about the research in verbal and written forms.
Results
Out of the total number of participants (n=355), male accounted for 170 (47.9%), the average age was 39 (30–53) years, female – 185 (52.1%), the average age – 44 (33–56.5) years. Three risk factors for cardiovascular diseases (CVD) were estimated in Evenk population by age and gender: smoking, alcohol consumption and physical activity.
The prevalence of smoking is a factor contributing to a decrease in the health and life quality of the population in the northern region [Citation13]. presents data on the gender and age distribution of “smokers” among the population of Jilinda village.
Table 1. Gender and age distribution of “smokers” among the population of Jilinda village (n=174)
As seen from the table, 121 (71.2%) men and 53 (34.1%) women (p<0.0001) smoke. The vast majority of younger smokers are men – 87.6% and almost half of female population – 48.1% (p<0.0001), middle-aged and elderly men – (54.7% and 47.0%, respectively) numbers are much less for women: 13.9% and 12.1%, respectively (p<0.0001). A similar number of the smoking frequency depending on gender and age were observed among the indigenous population of Gorny, Olekminsky, Tomponsky, Aldansky districts and Yakutsk [Citation13]. Smoking experience over 20 years was observed in 31.2% of the population (42.7% of men and 15.5% of women). The number of heavy smokers among men exceeded those among women more than 3 times (p<0.001).
As can be seen from the , there is a clear dependence of the frequency of smoking with such social factors as marital status, education and employment: single people smoke more often – 54.3%, divorced – 57.1% (p<0.001), with low education – 50.0% (p=0.029) and unemployed – 51.5% (p=0.007).
Table 2. Smoking frequency dependence on social factors
presents the data of the life quality questionnaire SF-36 about the “general health” scale dependence on the intensity of smoking.
Figure 1. General health depending on the number of smoked cigarettes
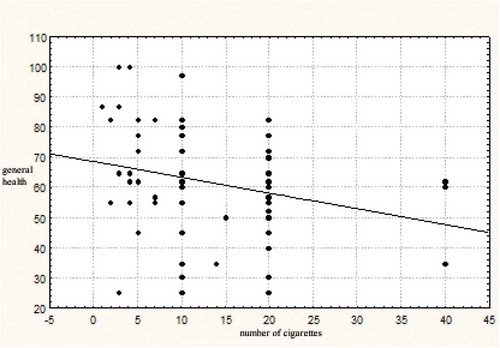
As can be seen from the figure, an inverse correlation was found between the “general health” scale and the intensity of smoking: the general health indicator of smokers decreased with an increase in the number of smoked cigarettes (r=−0.65). For those who smoked 40 cigarettes per day, the value of the “general health” scale did not exceed 64 points, whereas among those who smoked less than 5 cigarettes per day, the “general health” scale reached 100 points. Thus, this example shows that smoking is widespread (1/3 of the population of Jilinda village smoke cigarettes), and it is depended on various social and demographic factors. It is believed that the formation of alcoholism among the indigenous people of the North, occurs 2 or more times faster than among the newcoming population [Citation14]. It depends on the genetic characteristics of the organism, associated with the low ability of liver enzyme systems to utilize exogenous ethanol. Therefore, alcohol abuse exacerbates the physical, psychological, moral and financial degradation of the indigenous people of the North [Citation15]. We have studied alcohol consumption among various social strata of Jilinda village population. It was revealed that 65% of men and 24% of women consume alcohol. However, the frequency of alcohol consumption among the Evenk male in Oleneksky region and among the Yakut men in the Gorny region of the republic was comparable (65% and 74%, respectively), while among female Evenki it was much lower than among female Yakuts – 24% against 81% (p<0.0001). presents the frequency of consumption of alcoholic beverages, depending on gender and age group.
Table 3. The frequency of alcohol consumption depending on gender and age groups (%)
This table shows that the highest frequency of spirits and beer consumption was observed among men under the age of 45 (68%), wine/champagne among women aged 45–64 (55.6%). Statistically significant differences by gender were found in the consumption of beer and spirits in all age groups (p<0.001). It is a well-known fact that the character of alcohol consumption is significantly affected by the socio-economic position of the individual in society ().
Table 4. The frequency of alcohol consumption depending on social status (%)
As can be seen from the table, strong alcohol is mainly consumed by single (61.8%), divorced (60%) and people with secondary and “lower secondary” education (50% and 42.9%), wine and champagne are more often consumed by divorced (71.4%) and persons with higher education (64.7%), and beer by divorced (80%) (p<0.0001). The obtained data is comparable with the results of the alcohol consumption structure analysis in Russia by occupational groups, according to which not only social status but also the level of education is the most important determinant of alcohol consumption, but the gender and age of the respondent appear to be the most important determinant [Citation16,Citation17].
Thus, the frequency of alcohol consumption among the male part of the Evenki is comparable to that in the Yakut population, among the female part the number is much lower, and it is found most often among divorced people. Currently, changes in lifestyle and working conditions have led to a decrease in physical activity (PA) and a decrease in physical exercise. Meanwhile, it is known that low physical activity is a risk factor for the development of cardiovascular and other diseases [Citation18,Citation19]. The risk of CVD for physically inactive people is 2 times higher than for physically active people. When studying the walking time of the Evenki of Jilinda village, it was discovered that men walk an average of 50 min, women – 45 min a day. In accordance with the CYNDI program, such walking duration indicates low physical activity. Young people walk about 50 min during the day, the elderly walk less – about half an hour per day. Depending on the level of physical activity, all the patients were divided into 4 groups: 39.1% of men and 24.7% of women are physically inactive, 7.2% of men and 14.8% of women have low physical activity, average physical activity has – 27.5% of men and 27.2% of women, high physical activity – 23.2% of men and 25.9% of women. In young and middle-aged people, physical activity was higher than in the elderly group. However, it should be noted that more than a third of young people and more than half of middle-aged people were not physically active enough (PA is below average). A more detailed breakdown by age and gender is revealed the following differences:
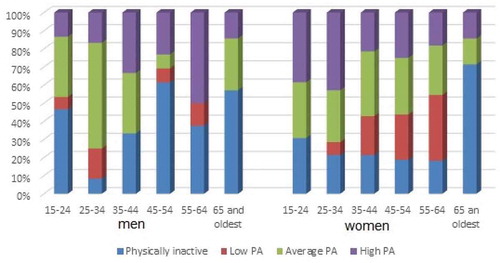
As can be seen from the , more than half of men aged 45–54 years, as well as older persons of both genders, are physically inactive (p<0.001). Nearly half of young men aged 15–24 have low physical activity (46.7%). High physical activity among men is more often observed at the age of 55–64 years (50%) (p<0.001), and among women at the age of 15–34 years (38.5–42.9%) (p=0.01). Women are physically more active than men at age 15–24 and 45–54 (p=0.03 and p=0.0005, respectively). Thus, this population in general is physically inactive, including young men.
Figure 2. The distribution of individuals by physical activity, depending on age and gender
Arterial hypertension (AH) is a substantial but potentially avoidable risk factor that significantly affects cardiovascular morbidity and mortality rates [Citation20,Citation21]. In the studied population, the frequency of AH was 33.1%. In numerous epidemiological studies, it was discovered that the education and social status of the population have an inverse relationship with the level of blood pressure and frequency of AH [Citation17,Citation20,Citation21]. shows the dependence of the AH frequency on various social factors.
Table 5. The dependence of the hypertension frequency on various social factors
As follows from the table, AH was more common among widowers (p<0.001), uneducated people (p<0.001), dissatisfied with living conditions (p<0.001), who used fortified alcoholic drinks (p=0.001), who had not worked for more than 5 years (p<0.001) and physically inactive individuals (p<0.001).
Thus, the frequency of arterial hypertension, in addition to the consumption of strong alcoholic beverages and the nature of physical activity, is influenced by marital status, level of education, employment and housing conditions.
Discussion
The powerful consequences of colonization by outsiders who subsequently dominated societies and alienated natives from their own way of life are common for many indigenous groups. This colonization has adversely affected physical, social, emotional, and mental health and well-being in traditional societies [Citation22]. Over the past 5 centuries, Inuit health has undergone significant changes as a result of the social, cultural, and economic changes brought about by interaction with Europeans. This process accelerated significantly in the second half of the twentieth century. Chronic diseases such as diabetes and cardiovascular diseases are on the rise [Citation23]. This situation appeared due to the rapid social, food, cultural, and environmental changes encountered by Inuit populations, and is characterized by a growing prevalence of behavioural risk factors (smoking, low physical activity and Western diet), obesity, and hypertension [Citation23]. In the population of American Indians and Alaska Natives, cardiovascular diseases and related risk factors are increasingly recognized as growing indicators of global health imbalances [Citation24]. Seventy-nine percent of the native Alaska population had 1 or more of the 6 main risk factors for cardiovascular disease, and 46% had 2 or more [Citation25]. As indicated in recent studies, it is possible that behavioural risk factors mediate the relationship between social conditions and blood pressure [Citation26].
The high incidence of arterial hypertension (AH) defined by us among the Evenks of the Russian Arctic – 33.1%, is comparable to that of Ontario residents (Canada), detected by 3 random telephone surveys of adult men and women (34%) in 2 cities [Citation27]. Among Canadians living in Saskatchewan, the prevalence of AH was lower – 20.3% [Citation28]. Half of our participants were unaware of their hypertension, as well as more than a third of hypertensive population in Canadian provinces [Citation29].
There are socio-economic factors in the structure of most of the studied risks for cardiovascular diseases in the ranked social groups of Greenland Inuits [Citation30]. They also found a reverse U-shaped relationship between the socio-economic conditions of the community and blood pressure with significantly lower SBP and DBP among participants living in remote traditional villages characterized by lower average disposable household income and in rich more urbanized cities [Citation31]. Among indigenous people in Ontario (Canada), rates of cardiovascular disease and the presence of risk factors, including information about hypertension, were higher among people with lower incomes [Citation32]. The negative role of adverse psychosocial factors on control of blood pressure among “white-collar” workers in Quebec (Canada) has also been proved [Citation33]. In our study, hypertension was also much more common among widowers, uneducated, persons unsatisfied with living conditions and long-term unemployed people (p<0.001).
In most parts of the Arctic, the traditional way of life of the indigenous population can no longer be maintained in conditions of rapid natural population growth and commercial exploitation of the circumpolar habitat by multinational corporations of “modern” society [Citation34]. Some indigenous peoples quickly acquire physical, social and mental disorders associated with the abuse of alcohol and other drugs by moving from traditional to transitional and modern lifestyles [Citation22]. Thus, among the Inuit of Greenland, the transition from the traditional to the modern way of life includes the growing prevalence of mental disorders and problems with alcohol [Citation35]. Evenki of Russian Arctic are no exception. We found that the majority of male and a quarter of female population consume alcohol (65% and 24%, respectively). The choice of alcoholic beverage is influenced by both gender and age: young people prefer beer, men prefer vodka/cognac at any age, middle-aged women prefer wine/champagne (p<0.001). However, a statistically significant relationship with hypertension frequency is determined only in relation to fortified wine: those who use it usually suffer from hypertension more often – 50% versus 30.4% (p=0.001). International studies of the health of indigenous and tribal peoples have shown that behaviour and its social structure are largely determined by social factors. In particular, cirrhosis associated with alcoholism is more common in lower socio-economic groups. Countries with tougher alcohol policies tend to have lower levels of alcohol consumption and fewer social problems due to alcohol [Citation36]. Accordingly, we studied the impact of the socio-economic status of the Evenki on alcohol consumption. It was revealed that hard drinks are often consumed by single (p<0.001), divorced (p<0.001), as well as people with secondary education (p=0.01). Besides, divorced people consume beer much more frequently than other categories of the population (p<0.001). Persons with higher education prefer light alcoholic beverages – wines and champagne (p<0.001).
Smoking is one of the most studied risk factors for cardiovascular diseases in ranked social groups of Greenland Inuit people [Citation30]. Inuit has seen an increase in the prevalence of smoking [Citation23]. When interviewing residents of Canadian provinces, smoking and stress or anxiety were mentioned as the main causes of heart disease in the majority of participants [Citation32]. Cardiovascular patients of Toronto also noted smoking as the most frequently identified risk factor for stroke (58.1%) [Citation37]. When studying the spread of smoking among the Evenk, it was revealed that the majority of men (71.2%) and a third of women (34.1%) smoke. The results are slightly lower than those of Inuit Arctic Canada (74%) [Citation38], Greenland (79% and 60%) [Citation35,Citation39], but much higher than those of Saskatchewan Canadians (about a quarter) [Citation28]. The dependence of smoking on socio-economic factors has been researched in a number of works [Citation35,Citation40,Citation41]. Thus, tobacco use and smoking-related diseases are uneven among the different social strata of Alaska Natives [Citation41]. The Inuit of Greenland has a tendency to decrease daily smoking with an increase in social status [Citation35]. Among indigenous people in Ontario (Canada), cardiovascular disease and risk factor occurrence (combined information on hypertension, diabetes, smoking, hyperlipidaemia and obesity) were higher among people with lower incomes [Citation40].
A number of studies have shown that smoking increases hypertension in both Canadians and Oklahoma Indians [Citation28,Citation42,Citation43]. In the Evenk population, we did not find a positive relationship between smoking and hypertension. Apparently, this is due to the fact that the number of smokers among the elderly (over 65 years) were much lower than among the young. However, the intensity of smoking clearly influenced general health: the value of the general health scale decreased with an increase in the number of cigarettes smoked during the day (r=−0.65).
It has been proven that the decrease in physical activity (PA) of Greenland Inuits and Canadians increases cardiovascular risk [Citation29,Citation30]. When interviewing residents of Canadian provinces, lack of exercise amounted to 28% of all heart disease causes [Citation29]. Chance of hypertension caused by obesity in Canadians increases markedly in the absence of PA at baseline [Citation42]. Between 2006 and 2009, in an environment that promotes healthier behaviour regarding PA in 4 different communities in Alberta (Canada), the proportion of people with normal blood pressure increased by 5.9% (p<0.001), while the proportion of people with stage 1 hypertension, decreased by 4.5% (p<0.001) [Citation44]. According to our results, hypertension was detected in more than half of individuals with rare physical exertion, whereas among people with more frequent exertion it was found from 16.7% to 29% (p<0.001). At the same time, there is evidence that the Inuit of Arctic Canada awareness of a chronic disease diagnosis is more associated with knowledge of healthy eating than with the amount of time spent on PA [Citation38]. A study of the total amount of PA and the redistribution of time spent at various objectively measured physical activity intensities in the adult Inuit family in Greenland led to the conclusion that, along with the rapid social, economic and cultural transition, indigenous people in the Arctic expect a more sedentary lifestyle [Citation45]. In the PA study of Canadian males and females aged 35–64, only 39% and 19% of males and females complied with the recommendations of the Canadian Society for Physiology of General Health Exercise PA (150 min per week) [Citation46]. Inuit populations are also characterized by a growing prevalence of low physical activity [Citation23]. Evenki of Jilinda village has the average duration of walking 50 min for men and 45 min for women per day which is insufficient in accordance with the SYNDI program. Even young people walk only about 50 min a day. Strangely enough, there were more physically inactive Evenki men than Evenki women (39.1% versus 24.7%), whereas in Greenland women are less active (30% women versus 14% among men) [Citation39]. It is regrettable that almost half of young men have low physical activity (46.7%). About a quarter of residents had high and medium physical activity, which is comparable with data from Saskatchewan, where 21.3% were highly physically active, and 24.2% were moderately active [Citation28]. In general, the Evenki population is physically inactive, including young men.
Analysis of the relationship between risk factors and control of hypertension among elderly Canadians showed that systolic blood pressure was higher for women than for men [Citation47]. For our Evenki, the frequency of AH did not depend on the gender (p<0.05). A study of the relationship between the frequency of visits to religious services and the prevalence of hypertension in Canada showed that people who attend religious services more than once a week have lower rates of hypertension (OR=0.82) compared to people who have visited religious services less than once per year [Citation28]. Unfortunately, we did not consider such connection, since in Jilinda most of the inhabitants are atheists.
Conclusion
The results of the study showed a high incidence of arterial hypertension and behavioural risk factors for its development (smoking, alcohol consumption, low physical activity) in the Evenk population of the Russian Arctic. It was discovered that the distribution of behavioural risk factors for hypertension depends on the age, gender and social status of each individual.
In order to eliminate modifiable (disposable) risk factors for arterial hypertension in Jilinda village, it is advisable to set up hobby clubs and evenings for single people, improve living conditions of population, limit alcohol consumption, and take measures to increase physical activity and employment of the population. To provide the population with jobs, in particular young men, it is necessary to restore reindeer herding and fishing farms, traditional for the indigenous peoples of the North. Increase of the physical activity, especially among young generation, can be provided by building gyms, volleyball, basketball courts as well as sport clubs in schools. Wide promotion of a healthy lifestyle among students and vulnerable groups of population, individual conversations with each alcohol and cigarette consumer, together with the establishment of Arterial Hypertension School at the hospital will help to raise awareness of the nation.
Public policy has a significant impact on the social determinants of health. In health policy, priority should be given to preventive measures as the most long-term and cost-effective. A lifestyle modification program needs to stimulate physical activity and to limit smoking and alcohol consumption. In the context of socio-economic transformations and environmental pollution caused by active industrial development of the Russian Arctic, it is necessary to monitor hypertension level and risk factors among the indigenous peoples of the North.
The authors are grateful to the head of the Olenek region of Yakutia, A.S. Ivanov, and the deputy of the State Assembly of Yakutia E.Kh. Golomareva for the organizational and financial support of scientific research.
Disclosure statement
No potential conflict of interest was reported by the authors.
Related Research Data
References
- National Prevention, Health Promotion and Public Health Council. 2010 Annual status report of the National Prevention, Health Promotion, and Public Health Council. 2010.
- CDC. The health consequences of smoking: a report of the Surgeon General. Atlanta: USDHHS, CDC, 2004.
- Ostbye T, Taylor DH. The effect of smoking on years of healthy life (YHL) lost among middle-aged and older Americans. Health Serv Res. 2004;39(3):531–9.
- Crothers K, Griffıth TA, McGinnis KA, et al. The impact of cigarette smoking mortality, quality of life, and comorbid illness among HIV-positive veterans. J Gen Intern Med. 2005;20(12):1142–1145.
- Garces YI, Yang P, Parkinson J, et al. The relationship between cigarette smoking and quality of life after lung cancer diagnosis. Chest. 2004;126(6):1733–1741.
- Mokdad AH, Marks JS, Stroup DF, et al. Correction: actual causes of death in the U.S., 2000. JAMA. 2005;293(3):293–294.
- Flegal KM, Williamson DF, Pamuk ER, et al. Estimating deaths attributable to obesity in the U.S. Am J Public Health. 2004;94(9):1486–1489.
- CDC. National Center for Chronic Disease Prevention and Health Promotion. Physical activity and good nutrition: essential elements to prevent chronic diseases and obesity 2003. Nutr Clin Care. 2003;6(3):135–138.
- Drewnowski A, Evans WJ. Nutrition, physical activity, and quality of life in older adults: summary. J Gerontol A Biol Sci Med Sci. 2001;56(SpecNo. 2):89–94.
- Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefıts associated with physical activity. Curr Opin Psychiatry. 2005;18(2):189–193.
- Swartz A, Strath S, Bassett D, et al. Increasing daily walking improves glucose tolerance in overweight women. Prev Med. 2003;37(4):356–362.
- Krivoshapkin VG. Essays on the clinic of internal diseases in the North. Yakutsk: Ministry of Education of Yakutia Press; 2001. ( Russian).
- Baltahinova ME, Klimova TM, Fedorova VI [Smoking and alcohol abuse among the indigenous population of Yakutia]/In the book: all-Russian Conference contradictions of modern cardiology: controversial and unresolved questions. Theses. Ministry of Health and Social Development of the Samara Region; Samara State Medical University; Russian Cardiology Society; Samara Regional Scientific Society of Physicians (section of cardiologists); The Samara Regional Clinical Cardiac Dispensary. Technical organizer “Medforum”. 2012; 216–217. Russian.
- Brittov AN, Eliseeva NA, Deev AD, et al. Socio-psychological factors in establishing the poor health of the population (the results of a population multicenter study). CardioSomatic. 2011;S1:15–16. Russian.
- Fedorova VI, Klimova TM. Habits and style of alcohol consumption among the population of Yakutsk. Electronic scientific and educational bulletin “Health and education in the XXI century”. 2008;10(4):187–188. Russian.
- Ankudinov AB, Lebedev OV. Analysis of the structure of alcohol consumption in Russia by professional groups. Prob Social Hyg Health Hist Med. 2014;1:10–14. Russian.
- Izmozherova NV, Popov AA. Level of education and cardiovascular risk in women in menopause. Cardiovasc Ther Prev. 2009;8(2):5–9. Russian.
- Maksimova TM, Belov VB, Pushkina NP. The prevalence of behavioral risk factors and diseases of the circulatory system. Prob Social Hyg Health Hist Med. 2014;1:3–7. Russian.
- Krivoshapkin VG, Klimova TM. Assessment of the health status of the population of Yakutsk under the CINDI program. Sci Educ. 2006;2:107–111. Russian.
- Shalnova SA, Deev AD, Karpov UA. Arterial hypertension and coronary heart disease in the real practice of a cardiologist. Cardiovasc Ther Prev. 2006;2(5):73–80. Russian.
- Mamedov MN, Deev AD. Assessment of the total risk of developing cardiovascular diseases in adults of working age: lessons of the study crossword. Cardiology. 2008;48(10):28–34. Russian.
- Gracey M, King M. Indigenous health part 1: determinants and disease patterns. Lancet. 2009;374(9683):65–75.
- Bjerregaard P, Young TK, Dewailly E, et al. Indigenous health in the Arctic: an overview of the circumpolar Inuit population. Scand J Public Health. 2004;32(5):390–395.
- Hutchinson RN, Shin S. Systematic review of health disparities for cardiovascular diseases and associated factors among American Indian and Alaska native populations. Plos One. 2014;9(1):e80973.
- Jernigan VBB, Duran B, Ahn D, et al. Changing patterns in health behaviors and risk factors related to cardiovascular disease among American Indians and Alaska Natives. Amer J Public Health. 2010;100(4):677–683.
- Chaix B, Bean K, Leal C, et al. Individual/neighborhood social factors and blood pressure in the RECORD cohort study which risk factors explain the associations? Hypertension. 2010;55(3):769–775.
- Petrella RJ, Speechley M, Kleinstiver PW, et al. Impact of a social marketing media campaign on public awareness of hypertension. Amer J Hypertens. 2005;18(2):270–275.
- Banerjee AT, Boyle MH, Anand SS, et al. The relationship between religious service attendance and coronary heart disease and related risk factors in Saskatchewan, Canada. J Religion Health. 2014;53(1):141–156.
- McCrindle BW, Manlhiot C, Millar K, et al. Population trends toward increasing cardiovascular risk factors in Canadian adolescents. J Pedtatrics. 2010;157(5):837–843.
- Bjerregaard P, Dahl-Petersen IK. How well does social variation mirror secular change in prevalence of cardiovascular risk factors in a country in transition? Amer J Hum Biol. 2011;23(6):774–779.
- Riva M, Larsen CVL, Bjerregaard P. Association between individual-level and community-level socio-economic status and blood pressure among Inuit in Greenland. Intern J Circump Health. 2016;75:32757.
- Kirkland SA, MacLean DR, Langille DB, et al. Knowledge and awareness of risk factors for cardiovascular disease among Canadians 55 to 74 years of age: results from the Canadian Heart Health Surveys, 1986–1992. Can Med Ass J. 1999;161(8):S10–S16.
- Trudel X, Milot A, Gilbert-Ouimet M, et al. Effort-reward imbalance at work and the prevalence of unsuccessfully treated hypertension among white-collar workers. Am J Epidemiol. 2017;186(4):456–462.
- Shephard RJ, Rode A. The health consequences of «modernization»: evidence from circumpolar peoples. Cambridge (UK): Cambridge University Press; 1996.
- Bjerregaard P, Dahl-Petersen IK, Larsen CVL. Measuring social inequality in health amongst indigenous peoples in the Arctic. A comparison of different indicators of social disparity among the Inuit in Greenland. SSM Popul Health. 2018;6:149–157.
- Anderson I, Robson B, Connolly M, et al. Indigenous and tribal peoples‘ health (The Lancet-Lowitja Institute Global Collaboration): a population study. Lancet. 2016;388(10040):131–157.
- Metias MM, Eisenberg N, Clemente MD, et al. Public health campaigns and their effect on stroke knowledge in a high-risk urban population: A five-year study. Vascular. 2017;25(5):497–503.
- Pakseresht M, Mead E, Gittelsohn J, et al. Awareness of chronic disease diagnosis amongst family members is associated with healthy dietary knowledge but not behaviour amongst Inuit in Arctic Canada. J Hum Nutr Diet. 2010;23(1):100–109.
- Bjerregaard P, Mulvad G, Pedersen HS. Cardiovascular risk factors in Inuit of Greenland. Inter J Epidemiol. 1997;26(6):1182–1190.
- Anand SS, Yusuf S, Jacobs R, et al. Risk factors, atherosclerosis, and cardiovascular disease among Aboriginal people in Canada: the Study of Health Assessment and Risk Evaluation in Aboriginal Peoples (SHARE-AP). Lancet. 2001;358(9288):1147–1153.
- Prochaska JJ, Epperson A, Skan J, et al. The healing and empowering Alaskan Lives Toward Healthy-Hearts (HEALTHH) Project: study protocol for a randomized controlled trial of an intervention for tobacco use and other cardiovascular risk behaviors for Alaska Native People. Contemp Clin Trials. 2018;71:40–46.
- Alter DA, Wijeysundera HC, Franklin B, et al. Obesity, lifestyle risk-factors, and health service outcomes among healthy middle-aged adults in Canada. BMC Health Serv Res. 2012;12:238.
- Jernigan VB, Wetherill M, Hearod J, et al. Cardiovascular disease risk factors and health outcomes among American Indians in Oklahoma: the THRIVE Study. J Racial Ethnic Health Disp. 2017;4(6):1061–1068.
- Lytvyak EO, Lee D, Schopflocher DP, et al. Impact of a 3-year multi-centre community-based intervention on risk factors for chronic disease and obesity among free-living adults: the Healthy Alberta Communities study. BMC Public Health. 2016;16:344.
- Dahl-Petersen IK, Jorgensen ME, Bjerregaard P. Physical activity patterns in Greenland: A country in transition. Scand J Public Health. 2011;39(7):678–686.
- Aparicio-Ting FE, Friedenreich C, Kopciuk KA, et al. Intrapersonal and social environment correlates of leisure-time physical activity for cancer prevention: a cross-sectional study among canadian adults. J Phys Activity Health. 2014;11(4):790–800.
- Bushnik T, Hennessy D, McAlister FA, et al. Factors associated with hypertension control among older Canadians. Health Rep. 2018;29(6):3–10.