
ABSTRACT
Background: Colonoscopy is a critical diagnostic and therapeutic procedure that is challenging to access in northern Canada. In part, this is due to frequent cancellations. We sought to understand the trends and reasons for colonoscopy cancellations in the Northwest Territories (NWT).
Methods: A retrospective review of colonoscopy cancellations January, 2018 to May, 2019 was conducted at Stanton Territorial Hospital, NWT. Cancellation details and rationale were captured from the endoscopy cancellation logs. Thematic analysis was used to group cancellation reasons. Descriptive statistics were generated, and trends were analysed using run chart.
Results: Of the scheduled colonoscopies, 368(28%) were cancelled during the 16 month period, and cancellations occurred, on average, 27 days after booking. Cancellation reasons were grouped into 15 themes, encompassing personal, social, geographic and health system factors. The most frequently cited theme was work/other commitments (69 respondents; 24%). Cancellations due to travel and accommodation issues occurred more frequently in the winter.
Conclusion: Over one in four booked colonoscopies were cancelled and the reasons for cancellations were complex. Initiatives focusing on communication and support for patients with personal or occupational obligations could dramatically reduce cancellations. Ongoing collaborative efforts are needed to inform and optimise access to colonoscopy in this region.
Introduction
Populations in the circumpolar north experience multiple health system, sociocultural and geographic barriers to accessing healthcare [Citation1]. This is particularly important when considering access to procedures by specialist such as colonoscopy. Timely colonoscopy is critical to the diagnosis and management of a broad range of digestive diseases [Citation2,Citation3]. This includes colorectal cancer (CRC), as colonoscopy not only confirms diagnosis but also affords an opportunity to remove precancerous adenomas [Citation4,Citation5]. Colonoscopy is typically a 20–40 min procedure, but for northern residents may require 3–4 days away from home to allow for travel, bowel preparation and recovery. Residents of the Northwest Territories (NWT), a northern region of Canada, are nearly twice as likely to die from CRC as other Canadians [Citation6]. These outcomes could be improved with increased access to colorectal cancer screening, including colonoscopy, which has been shown to facilitate earlier diagnosis, and reduce CRC-associated mortality [Citation5,Citation7]. A recent analysis of CRC screening in the NWT, identified that an important factor limiting colonoscopy access is frequency of cancellations [Citation8].
The complex health system, sociocultural and geographic factors that limit access to healthcare for populations in rural and remote regions, may be making residents of the NWT particularly susceptible to cancellation. For instance, locum turnover in remote communities is high and can interrupt continuity of care and communication to patients [Citation8]. Over one third of communities in the NWT have no year-round road access, which complicates safe travel to medical appointments [Citation9]. Additionally, 51% of the population in the NWT self-identify as Indigenous [Citation10]. Studies in other regions, have shown Indigenous individuals to experience disparities in access to colonoscopy when compared to non-Indigenous residents [Citation11,Citation12]. To date, studies have found rural residents experience delays in colonoscopy access in Ontario (Canada) and Western Australia [Citation13,Citation14]. However, no studies have assessed colonoscopy access in northern Canada or specifically the impact of cancellations on access to care. The population of the NWT may be experiencing important limitations to colonoscopy access, manifested as frequent cancellations. Understanding the trends and reasons for these cancellations could help researchers, clinicians and patients to understand and improve healthcare access in other rural and remote regions. To explore this topic further, the aim of this study is to better understand the trends and reasons for colonoscopy cancellation at the largest endoscopy centre in Northwest Territories.
Materials and methods
Setting
The NWT has a population of 44,500 people, distributed across 1.1 million square kilometres of land [Citation10,Citation15]. 47% of the population lives beyond the urban centre of Yellowknife, with 9% living in fly-in communities [Citation9,Citation15]. Many communities with all-season road access, still require flights for routine health services due to the distances and road conditions. Stanton Territorial Health Authority (STHA) is located in Yellowknife and is the largest of two tertiary centres in the territory, and the only one with access to surgical and gastrointestinal specialist services. The endoscopy unit serves approximately 47,960 individuals from 26 communities, including 5 from the neighbouring territory of Nunavut [Citation15,Citation16]. Canada has a publicly-funded healthcare system and the cost of travel, and accommodations to attend medically necessary health services, including colonoscopy, are covered [Citation17]. Flights and accommodations are booked directly by a medical travel agency in the NWT. Patients who are driving to appointments or choose to make their own arrangements will be reimbursed of travel expenses after the fact.
Clerical staff at the endoscopy unit contact the patient by phone at the time of the appointment booking and 2–3 weeks prior to the procedure. All cancellations and associated data, including community of residence, timing of cancellation and reason for cancellation, are recorded by clerical staff in the cancellation log using pre-populated categories and/or free text descriptions.
Data collection
We conducted a retrospective review of all colonoscopy cancellations between January 1 2018 and May 31 2019 at the endoscopy unit of the STHA as identified in the endoscopy cancellation logs. Monthly totals of conducted colonoscopies were obtained from the endoscopy unit records. For cancelled procedures, the timing of cancellation, community of residence and rationale for cancellation were collected. Distances between communities and STHA were calculated using straight line distances from Google Maps. Population estimates in the 2018 NWT and Nunavut 2016 population estimates were obtained from NWT Government Bureau of Statistics [Citation15] and the Government of Nunavut [Citation16] databases.
Data analysis
A thematic analysis of all recorded reasons for cancellation was conducted by NB, HS and AT. Responses were individually assessed and grouped into overarching themes. Themes were further subdivided by who initiated the cancellation, i.e. cancellations initiated by patients versus clinicians/hospital administrator. The themes, subdivisions and their susceptibility to seasonal variation were reviewed by two local patients EL and BB who had an understanding of the patient experience of colonoscopy. Seasonal variation in monthly totals of cancellation were assessed graphically for special cause variation using the run chart analysis [Citation18]. To compare communities, the number of cancellations per 1000 residents were compared. Reported cancellation rates were aggregated by administrative region to obscure patient identifiers (). Time between the cancellation and the scheduled procedure date were compared by the prepopulated categories of “no-show appointments”, “less than 24 hours in advance of scheduled appointment” and “more than 48 hours”. Two sample Student T-test was used for comparing normally distributed continuous variables. A p value of <0.05 was considered to be statistically significant. All descriptive statistics were generated using Microsoft Excel V16.16.13.
Table 1. Administrative regions and associated communities of the NWT with cancellations.
Results
Of the 1335 colonoscopies booked during the 16 month observation period, 372 (28%) were cancelled. 368 were included in our analysis, after excluding 4 due to incomplete data entry. Among the included cancellation events, 90 (25%) were initiated by the clinician or hospital administrator, 198(54%) were cancelled by patients, and the remainder were unknown. Twenty-six (7%) cancellations were identified by clerical staff as being with patients who had had a previous colonoscopy cancellation.
Reason for cancellation
A rationale for cancellation was described in 288 (78%) of cases. The 256 unique responses included personal, social, geographic and health system barriers, which were grouped into 15 themes (). Of those who responded, the most frequently cited thematic reason for cancellation was work/other commitments (identified by 69, 24%) (). Other frequently cited thematic reasons were medical reasons/comorbidities (42, 15%), weather/transportation/hotel issues (31, 11%) and being away from home (31, 11%) ().
Figure 1. Percentage distribution of colonoscopy cancellations, by reason for cancellation. Reasons provided by patients are highlighted in blue, while reasons initiated by providers are highlighted in green.
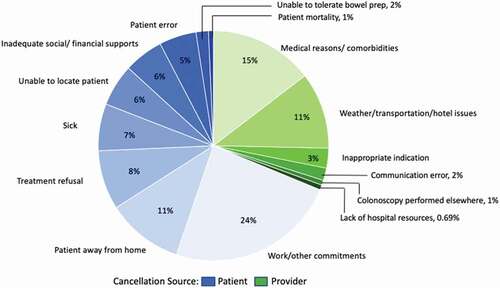
Table 2. Fifteen themes of reasons for colonoscopy cancellation.
Seasonal variation
With assistance from our patient partners, we identified the following thematic reasons for cancellation as ones which were susceptible to seasonal variation: patient was away from home, patient was sick, patient could not be located, patient had work/other commitments, or weather/transportation/hotel issues. Monthly incidence of cancellations for each of these reasons were analysed using probability parameters for non-random variation (supplement Figure 1A-D). For weather/transportation/hotel issues, a shift was present from July 2018 to April 2019, with all values above the median, and an astronomical point identified in September 2018, with 8 (24%) of all 33 weather/transportation/hotel cancellations occurring in a single month (supplement Figure 1E). No other significant shifts, trends, runs or astronomical data points to suggest non-random variation were identified.
Timing of cancellations
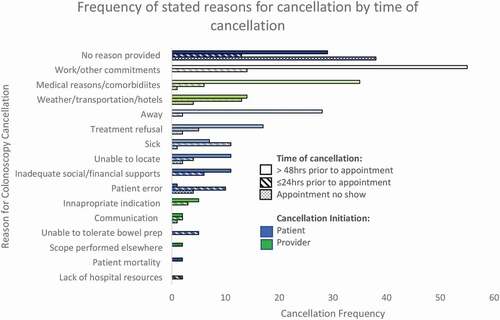
The majority of colonoscopies, 219(60%), were cancelled more than 48 hours in advance of their scheduled procedure date. 96(26%) appointments were cancelled within 24 hours of the scheduled procedure time, and 54 (14%) patients were no-shows. Among cases cancelled more than 48 hours in advance, the most common thematic reasons for cancellation were work/other commitments (55, 25%), and medical reasons/comorbidities (35, 16%) (). Of the cases cancelled within 24 hours, the most common reasons for cancellation were work/other commitments (14,15%) and weather/transportation/hotels (13, 14%) (). Majority of no-show cancellations occurred without any reason provided (38, 70%). In assessing the time elapsed between the booking date and cancellation date, we observed a mean duration of 27 days (standard deviation (SD) 15.7). When comparing this timeframe by reason for cancellation, we observed no difference between patient initiated and provider initiated reasons (mean 27 days and 31 days respectively, (SD 15.2 and 20.9, p = 0.13). On average, cancellations due to communication errors had the longest time from booking date (41 days, SD 7.7) and colonoscopies performed elsewhere had the shortest (10 days, SD 9.0). The shortest time between booking and cancellation was one day, and the longest was 76 days.
Figure 2. Frequency of colonoscopy cancellation reasons categorised by time between cancellation and scheduled appointment.
Cancellations by community
Cancellations occurred among residents from 21 communities across the NWT, and 5 communities in the Kitikmeot region of Nunavut. The community with the highest rate of cancellations was Fort Smith (29 cancellations/1000 people) (). When comparing by region, we observed that the areas with the highest cancellation rate were Fort Smith (29/1000 residents), Tilcho (16/1000 people), Dehcho (14/1000 people), Yellowknife (6/1000 people), Hay River (6/1000 people), the Nunavut communities (3/1000 people), Sahtu (3/1000 people) and Beaufort Delta (2/1000 people).
Figure 3. Cancellations per 1000 residents in administrative regions of NWT and NU serviced by the STHA [Citation38].
![Figure 3. Cancellations per 1000 residents in administrative regions of NWT and NU serviced by the STHA [Citation38].](/cms/asset/d319b642-f685-48c5-92ff-13abd707f04e/zich_a_1816678_f0003_oc.jpg)
Discussion
We observed over one in four colonoscopy appointments booked at STHA were cancelled during the study period. To our knowledge, this is the first study to analyse colonoscopy cancellations in a rural and remote region. Several studies have looked at urban centres and report much lower cancellation rates than we observed [Citation19–Citation21]. For instance, Lee and colleagues report a cancellation rate of only 5.7% at a community hospital in Dublin Ireland. In an academic tertiary care centre in Canada, the no-show rate for colonoscopy was 2.6%. The high rate of cancellations and no-shows we observed raises an important issues in health system access and resource utilisation. The reasons for cancellation we identified align with barriers to healthcare previously identified in for circumpolar north populations: physical geography, communication, sociocultural and systemic factors [Citation1,Citation22]. As such, the reasons and trends of colonoscopy cancellations identified in this study may provide critical insight for providers and policy-makers working to improve access to specialist care in other northern regions.
Cancellations reduce patients’ access to care and waste resources which are already limited in rural and remote settings. This is especially the case for appointments cancelled within 24 hours as they cannot be filled by another patient who has undergone preparation for a colonoscopy. Interestingly, factors identified to be associated with truancy for colonoscopy in another study are rarely an issue at STHA: referral from a specialist, and patients having office-based consults in advance of the procedure [Citation19]. Furthermore, multiple initiatives described in other studies to reduce cancellations have already been implemented at STHA including appointment reminders, pamphlets and over-booking [Citation19,Citation20,Citation23,Citation24,Citation25]. Reducing cancellations appears to be a complex challenge, as demonstrated by the broad scope of reasons for cancellations we observed.
The most frequently cited rationale was work/other commitments. This theme included free text descriptions such as “caring for granddaughter”, “busy at work” and “going to a carnival” which highlights that a broad range of factors may contribute to cancellations in this category. For instance, “caring for granddaughter” may suggest inadequate financial, or social resources to recruit child care support. In 19 of 69 (28% of this category), family commitments were the reason for cancellation. A study outlining the experiences of patients travelling out-of-territory for medical care in the NWT had similar findings, noting that the most frequently cited challenge in accessing care for patients was arranging support for their household while away [Citation26]. Given that half of the population of the NWT is Indigenous, it is also important to consider the role of intergenerational child care for older community members who might also require colonoscopy. In both traditional and contemporary times, grandparents and Elders fulfill important child rearing roles in many First Nations, Metis and Inuit families across Canada and the USA [Citation26–Citation29]. Today, Indigenous children are more likely than non-Indigenous children to live with their grandparents, possibly reflecting these important child care roles that older adults may hold [Citation30]. Initiatives that focus on finding respite for those with family commitments or allow for flexibility in scheduling may therefore enhance appointment attendance. Reasons such as “going to carnival” may suggest a gap in knowledge regarding the value of the procedure, or avoidance by the patient. “Busy at work” was the most frequent reason for cancellation identified in this study and warrants further research to understand and address. It may suggest patients are not given adequate advance notice of the appointment to miss work, or they do not have adequate support from employers to miss work. Missed work can be particularly challenging for individuals working in mines where they are expected to be onsite for several weeks at a time. The issue of work/other commitments is likely compounded by the geographical distance patients have to travel for their colonoscopy appointment. Many patients rely on medical travel to attend a colonoscopy. This typically requires flying to Yellowknife for a minimum 3-day stay in shared accommodations or a hotel to complete the bowel preparation before, and recover after the procedure. Arrangements for medical travel, accommodations and appointments requires complex coordination between health services and related agencies which are vulnerable to miscommunications, and disrupted continuity [Citation8,Citation26]. As such, patients may not receive much advance notice of their appointment, or have control over the details as demonstrated in one cancellation description “medical travel only told patient two days prior”. This creates additional barriers for patients in attempting to adapt their work and family commitments to attend their colonoscopy appointments.
Travel arrangements were also a frequent source of cancellation as demonstrated by weather/transportation/hotel issues being the most frequent reasons for last minute cancellation (<24 hours prior to appointment). This has been identified in other studies looking at rural access to health care [Citation31]. Flights may be cancelled due to inclement weather and driving conditions unfavourable especially with seasonal shutdown of ferries and ice roads. We observed an increase in cancellations between September and April. This may be explained by frequent fog in the autumn months which results flight cancellations to/from Yellowknife [Citation32] as well as the difficult driving conditions in winter. We also observed a peak in September 2018, with seven of eight of these cases cancelled specifically because no hotel room was available. September is peak tourist season in Yellowknife. Strategies to reserve capacity for patient accommodations or adjust scheduling in September may help to optimise endoscopy resources at that time of year.
We also found that a frequent source of cancellation was for medical reasons or comorbidities which included those who required optimisation of their comorbidities prior to colonoscopy, or could not be completed at the endoscopy unit due to their procedural risk. A majority of these were cancelled >48 h in advance (35, 83%). Rural residents have been found to have a greater burden of chronic disease than urban residents [Citation33]. Identifying those who require further investigations before their appointment is especially challenging when only 53% of the population have regular access to a primary care provider [Citation34]. Enhancing systematic triage and referral protocols may help reduce these cancellations. An example of such program is the rapid referral program in the UK which was shown to reduce time to referral and was associated with a reduction in cancer mortality [Citation35].
When looking at cancellations by region, we observed the highest cancellation rates in the Fort Smith region. The reason for this is not clear. The population in this region experienced the same three highest themes for cancellation as the overall population: work/other commitments (17, 23%); weather/transportation/hotel (6, 8%); medical reasons (7, 9%). The lower rates seen in other communities may be due to their proximity to the other endoscopy centre. Endoscopy is available in two other communities in the NWT: Inuvik and Hay River with more complex cases being referred directly to Yellowknife. This likely contributes to the lower cancellation rates seen in Beaufort Delta, Sahtu and Hay River regions where patients may be seen for colonoscopy at these other centres which were not included in this study. The difference in cancellations seen between the regions with endoscopy and those without supports the argument of rurality playing a role in appointment cancellations for procedures [Citation36]. Initiatives targeted at reducing cancellations in the Fort Smith region could reduce this disparity in access.
This study was limited to one tertiary care hospital and to the cancellation rationale transcribed by clerical staff. Thus, it is important to consider underlying reasons for cancellations that might not be easily captured by clerical. For instance, a study of cancellations at a primary care office found that the majority of patients identified emotional barriers, including fear of uncomfortable procedures or negative news, as the underlying reasons for cancellation [Citation37]. Similarly, Yang and colleagues, observed in their systematic review that 16–56% of patients experience significant anxiety regarding their colonoscopy [Citation39]. Patients may not verbalise their concerns to clerical staff, but instead give logistical reasons for their cancellations which are likely contributors but may not be the underlying reason [Citation37]. These limitations are particularly important when analysing barriers encountered by Indigenous patients. Indigenous patients living in the north have been found to encounter discrimination in healthcare institutions related to centuries of colonialism and forced assimilation, limited access to healthcare professionals in remote communities, and differences in culture and language [Citation1,Citation25,Citation40,Citation41]. As such, the findings of this study should be interpreted with the understanding that these complex issues may not readily be expressed by the patient at the time of cancellation. Furthermore, we did not compare anticipated wait time of those cancelled to those completed which may represent another undisclosed reason for cancellation.
Conclusion
The reason that over one in four colonoscopies are cancelled at a remote northern endoscopy unit is complex. We observed work and family commitments, travel complications and medical comorbidities were frequently cited. Reducing cancellations will require collaborative patient-centred initiatives to help overcome the complex social, occupational, cultural, geographic and health system challenges in accessing colonoscopy. Improving communication between providers and enhancing support for patients with conflicting personal obligations may be particularly beneficial. Further analysis of the root causes of the reasons cancellations identified in this study could inform targeted patient-centred interventions. These barriers to accessing healthcare do not appear to be unique to colonoscopy in the NWT, and evaluation of cancellations to other health services and rural and remote regions could help inform and improve access for vulnerable populations in the circumpolar north.
Supplemental Material
Download MS Word (37.9 KB)Acknowledgements
We would like to thank NWT residents Bernice Beaverho and Elaine Look for providing a patient’s perspective to inform the analysis of this work.
Disclosure statement
All authors confirm that they have no competing interests with this study.
Supplementary material
The supplemental data for this article can be accessed here.
Additional information
Funding
References
- Huot S, Ho H, Ko A, et al. Identifying barriers to healthcare delivery and access in the Circumpolar North: important insights for health professionals. Int J Circumpolar Health. 2019 Jan 1;78(1):1571385.
- Paterson WG, Depew WT, Paré P, et al. Canadian consensus on medically acceptable wait times for digestive health care. Can J Gastroenterol. 2006 Jun;20(6):411–8.
- Armstrong D, Barkun AN, Chen Y, et al. Access to specialist gastroenterology care in Canada: the Practice Audit in gastroenterology (PAGE) wait times program. Can J Gastroenterol. 2008 Feb;22(2):155–160.
- Triantafillidis JK, Vagianos C, Malgarinos G. Colonoscopy in colorectal cancer screening: current aspects. Indian J Surg Oncol. 2015 Sep;6(3):237–250.
- Rabeneck L, Paszat LF, Saskin R, et al. Association between colonoscopy rates and colorectal cancer mortality. J Gastroenterol. 2010 Jul;105(7):1627–1632.
- GNWT Health and Social Services. Cancer in the Northwest Territories 2001–2010 [Internet]. Yellowknife: NWT: Government of Northwest Territories; 2014 cited 2020 Apr 11. Available from https://www.hss.gov.nt.ca/sites/hss/files/nwt-cancer-fact-sheets.pdf
- Hewitson P, Glasziou P, Watson E, et al. Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (Hemoccult): an update. Am J Gastroentero. 2008 Jun;103(6):1541–1549.
- Champion C, Alvarez GG, Affleck E, et al. A systems perspective on rural and remote colorectal cancer screening access. J Cancer Policy. 2017 Dec;14:27–32.
- GNWT Careers. Fly in communities [Internet]. Yellowknife, NWT: government of Northwest Territories; [date unknown]. [cited 2020 Mar 14]. Available from: https://www.gov.nt.ca/careers/en/fly-communities
- Statistics Canada. Focus on Geography Series, 2016 Census Catalogue no. 98-404-X2016001 [Internet]. Ottawa, ON: Statistics Canada; 2017 [updated 2019 Apr 10; cited 2020 Mar 14]. Available from: https://www12.statcan.gc.ca/census-recensement/2016/as-sa/fogs-spg/Facts-PR-Eng.cfm?TOPIC=9&LANG=Eng&GK=PR&GC=61
- Towne SD, Smith ML, Ory MG. Geographic variations in access and utilization of cancer screening services: examining disparities among American Indian and Alaska Native Elders. Int J Health Geogr. 2014 Jun;13:18.
- Watanabe-Galloway S, Flom N, Xu L, et al. Cancer-related disparities and opportunities for intervention in Northern Pains American Indian communities. 433021. 2011 May-Jun;126(3):318–329.
- Gillis A, Dixon M, Smith A, et al. A patient-centred approach toward surgical wait times for colon cancer: a population-based analysis. Can J Surg. 2014 Apr;57(2):94–100.
- Emery JD, Walter FM, Gray V, et al. Diagnosing cancer in the bush: A mixed methods study of GP and specialist diagnostic intervals in rural Western Australia. Fam Pract. 2013;30(5):541–550.
- GNWT Bureau of Statistics. Summary of NWT Community Statistics. [Internet]. Yellowknife: NWT: Government of Northwest Territories; 2018 cited 2020 Jan 30. Available from https://www.statsnwt.ca/community-data/
- Nunavut Bureau of Statistics. Population Estimates [Internet]. Iqaluit: NU: Government of Nunavut; 2016 cited 2020 Mar 14. Available from https://www.gov.nu.ca/sites/default/files/population_estimates_report_july_1_2016.pdf
- Services H and S. Medical Travel [Internet]. Yelloknife: NWT: Government of the Northwest Territories. cited 2020 Aug 11. Available from: https://www.hss.gov.nt.ca/en/services/medical-travel
- Perla RJ, Provost LP, Murray SK. The run chart: a simple analytical tool for learning from variation in healthcare processes. BMJ Qual Safe. 2011 Jan 1;20(1):46–51.
- Wong VK, Zhang H-B ER. Factors associated with patient absenteeism for scheduled endoscopy. World J Gastroenterol. 2009 Jun 21;15(23):2882–2886.
- Lee CS, McCormick PA. Telephone reminders to reduce ron-attendance rate for endoscopy. J R Soc Med. 2003 Nov 1;96(11):547–548.
- Badurdeen DS, Umar NA, Begum R, et al. Timing of procedure and compliance to out-patient endoscopy among an underserved population in an inner city tertiary institution. Ann Epidemiol. 2012 Jul;22(7):531–535.
- Chan J, Friborg J, Chernov M, et al. Access to radiotherapy among circumpolar Inuit populations. Lancet Oncol. 2019 Oct 1;20(10):e590–600.
- Hasvold PE, Wootton R. Use of telephone and SMS reminders to improve attendance at hospital appointments: a systematic review. J Telemed Telecare. 2011 Oct;17(7):358–364.
- Denberg TD, Coombes JM, Byers TE, et al. Effect of a mailed brochure on appointment-keeping for screening colonoscopy: a randomized trial. Ann Intern Med. 2006 Dec 19;145(12):895–900.
- Reid MW, May FP, Martinez B, et al. Preventing endoscopy clinic no-shows: prospective validation of a predictive overbooking model: am. J Gastro. 2016 Sep;111(9):1267–1273.
- Kerber K, Kolahdooz F, Otway M, et al. Opportunities for improving patient experiences among medical travellers from Canada’s far north: a mixed-methods study. BMJ Open. 2019 Dec;9(12):e030885.
- Eni R, Harvey CD, Phillips-Beck W. In consideration of the needs of caregivers: grandparenting experiences in Manitoba First Nation communities. First Peoples Child & Fam Rev. 2009;4(2):85–98.
- Tam BY, Findlay LC, Kohen DE. Indigenous families: who do you call family? J. Fam Stud. 2017;23(3):243–259.
- Canadian First F-TE. Nations grandparents raising grandchildren: A portrait in resilience. Int J Aging Hum Dev. 2005 Jun;60(4):331–342.
- Turner A. Living arrangements of Aboriginal children aged 14 and under, Catologue no. Catalogue no. 75-006-X[Internet]. Ottawa ON: Statistics Canada; April 2016 [cited 2020 Jun 12]. Available from: https://www150.statcan.gc.ca/n1/en/pub/75-006-x/2016001/article/14547-eng.pdf?st=veD19vB2
- Howard AF, Smillie K, Turnbull K, et al. Access to medical and supportive care for rural and remote cancer survivors in northern British Columbia. J Rural Health. 2014 Jun 1;30(3):311–321.
- Klock R, Hudson E, Aihoshi D, et al. The Weather of the Northwest Territories and Western Nunavut. Graphic Area Forecast 35 [Internet]. Ottawa, ON:NavCanada. 2001. cited 2020 Mar 24. Available from: https://www.navcanada.ca/EN/media/Publications/Local%20Area%20Weather%20Manuals/LAWM-Yukon-NWT-EN.pdf
- Kulig JC, Williams AM, editors. Health in rural Canada. Vancouver: UBC Press; 2013c. p. 570.
- Lewis JP, Boyd K, Allen J, et al. “We raise our grandchildren as our own:” Alaska Native grandparents raising grandchildren in Southwest Alaska. J Cross Cult Gerontol. 2018 Sep;33(3):265–286.
- Møller H, Gildea C, Meechan D, et al. Use of the English urgent referral pathway for suspected cancer and mortality in patients with cancer: cohort study. BMJ. 2015 Oct 14:351. cited 2020 Aug 10. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4604216/
- Seidel JE, Beck CA, Pocobelli G, et al. Location of residence associated with the likelihood of patient visit to the preoperative assessment clinic. BMC Health Serv Res. 2006 Feb 22;6(1):13.
- Lacy NL, Paulman A, Reuter MD, et al. Why we don’t come: patient perceptions on no-shows. Ann Fam Med. 2004 Nov;2(6):541–545.
- ConceptDraw. GeoMap Canada vector stencils library [Internet]. San Jose, CA: ConceptDraw; [date unknown]. cited 2020 May 20. Available from: https://www.conceptdraw.com/examples/northwest-territories
- Yang C, Sriranjan V, Abou-Setta AM, et al. Anxiety associated with colonoscopy and flexible sigmoidoscopy: A systematic review. Am J Gastro. 2018 Dec;113(12):1810–1818.
- Gracey M, King M. Indigenous health part 1: determinants and disease patterns. Lancet. 2009;374(9683):65–75.
- Wilk P, Maltby A, Cooke M. Residential schools and the effects on Indigenous health and well-being in Canada—a scoping review. Public Health Rev. 2017 Mar 2;38(1):8.