
ABSTRACT
Background: Little is known about how younger schoolchildren in a rural setting experience their sense of coherence (SOC), how they think and reason about health and what they perceive as important to achieve health goals. This study aimed to investigate children’s SOC and their health perceptions.Method: In this mixed-method study 94 children (8-12 years) from three rural schools answered several questionnaires: The Child-SOC (CSOC), Positive Health Scale (PHS) and Cantril’s ladder of life scale. Another 23 children (of 94) participated in four focus group interviews. Thematic analysis was used to identify themes from the interview transcripts.Results: High SOC was reported by 48% of the boys and 22% of the girls. However, no significant gender differences were found. Four themes were generated from the qualitative analysis: Understanding health, Managing health, Doing bodily health and Socialising health. Both younger and older children had a holistic view of health in which health was seen as an individual’s living habits in which social contacts mattered.Conclusion: In a rural context children need to adapt to activities that exist in their immediate environment. Thus, activities during school hours can be an important complement in health promotion.
Growing up in a rural area with long distances between home, school, and classmates creates exceptional living circumstances. A Swedish study found that rural children had paradoxical feelings about their rural setting. Although living in a safe, rural context had a high level of cohesion and trust among children, it also contributed to exclusion, social control, and isolation [Citation1]. Thus, living in a sparsely populated area may limit access to relationships in the neighbourhood and attending a small school limits the number of classmates and access to social capital, but it may also contribute to cohesion moulded through close relationships. Contradictory findings have been reported in several social capital studies on rural living. For instance, while higher levels of networks, civic participation, cohesion and better mental health are often reported [Citation2,Citation3], social capital also has a dark side, namely exclusion or excessive demands on others within the group [Citation4,Citation5]. In summary, social capital is important for the child’s health and sense of coherence (SOC) but is complex as it can both support and aggravate health.
Social capital, understood as the relationships, norms, and trust acquired in meaningful networks, influences children’s health and wellbeing [Citation6,Citation7]. Health is an ambiguous concept with multiple meanings and thus complex and widely debated. Definitions range from those taken from medical models based on the absence of disease and disability to more holistic health models [Citation8–10]. World Health Organization’s (WHO) definition of health, dating back to the 1940s, is “a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity” which represents a holistic approach to health, capturing the subjective dimension of health [Citation11]. Physical health refers to physical capabilities and functional levels; mental health refers to emotional health and wellbeing; and social health refers to how well the person gets along and interacts with other people [Citation12–14]. Despite numerous criticisms of it being utopian and the lack of consensus on the definition of wellbeing, the WHO model is often used in research [Citation8]. Well-being and health as a holistic concept are related to several aspects, e.g. physical activity, living habits, sort of diet and social life. A study by Eriksson, Hochwälder, Carlsund, and Sellström [Citation15] found that higher degrees of social capital in family, school and neighbourhood were all associated with higher levels of wellbeing and lower levels of health complaints. For environmental aspects, neighbourhoods can facilitate or constrain moderate-to-vigorous physical activity and positive outcomes between social capital and physical activity in children [Citation16, Citation17]. Rural-urban differences in children´s level of physical activity have been shown among children in grades 4–6 in that the urban children were the least active overall and children in small cities had the highest activity level [Citation18]. On the other hand, another study concluded that residence has no apparent impact on physical fitness [Citation19]. In a review investigating physical activities and dietary habits in rural and urban children the authors found that rural youth could be more physically active than urban youth but that the diets such as consumption of fruits and vegetable of the rural young may not be optimal [Citation20]. The link between physical exercise and perceived health was confirmed in a study among 12-year-old children showing that physical exercise was most strongly associated with perceived health [Citation21].
Wellbeing and health are often described as related to a person’s sense of coherence (SOC). The concept of SOC is the core element of a salutogenic theory explaining an individual’s capacity to create health [Citation22]. SOC consists of three elements: comprehensibility, manageability and meaningfulness, and reflects the individuals’ coping capacity to deal with everyday life stressors and stay healthy [Citation23]. To explain health and understand how these three elements can be supported both resilient and protective factors need to be considered. Some research suggests that context plays an important role in SOC [Citation24] and that SOC is a vital resource to preserve and promote health [Citation25].
Studies exploring health in a youth context show that young people are prone to distinguish between mental and physical aspects of health and how they are experienced and dealt with [Citation26,Citation27]. Children perceived a healthy diet, exercise/sport, good hygiene, avoiding smoking and substance abuse and taking care of diseases as a healthy lifestyle [Citation28,Citation29]. One study demonstrated that younger children (8–11 years) have a biomedical approach to health and considerable knowledge about health, illness and disease risks. Moreover, they seemed health-conscious and held positive attitudes towards health and health promotion [Citation30]. Health perceptions have been investigated in preschool children as young as 4–5 years old. The overall results show that young children perceive health as a multi-dimensional construct, mostly related to being engaged, performing desirable activities and participating in a supportive everyday context [Citation31]. The children’s descriptions are in line with an action-oriented view of health, as described by Nordenfelt. Citation32,argues for a holistic and action-oriented understanding of health in which a balance exists between what a person wants to do and can do. Children aged 9–11 years were asked about what they consider healthy and unhealthy. The author found that children’s definitions were broad, encompassing illness, good nutrition, environmental health, mental health and cleanliness to name a few [Citation33]. One study showed differences between older (8–11 years) and younger (5–7 years) children in their perceptions of illness and health. The younger children had difficulty with the two concepts of illness and health, whereas the older children had a more multifaceted understanding [Citation34]. In addition, Citation34,showed that illness was largely perceived as a biomedical phenomenon by the children, but health was considered a psychosocial one. Another study examining the understanding of health and illnesses in 5-and 9-year-old children reported that younger children were more likely to focus on being either completely healthy or ill, whereas older children could see nuances in their health [Citation35].
From a health promotion perspective, health initiatives should be implemented with people and not for them. According to the WHO concept Health Promoting Schools (HPS), student participation is central [Citation36,Citation37]. Based on the ambition to increase student involvement, it is paramount to understand the children’s health perceptions. In the Nordic countries the voices of children living in rural areas are seldom heard. Despite a growing body of research on children’s perceptions of health, many questions remain to investigate. Little is known about how younger schoolchildren in a rural setting experience their SOC, how they think and reason about health and what they find important for its achievement. Thus, the study aimed to investigate children’s SOC and their perceptions of health. The following research questions were asked: How do children consider their sense of coherence? How do children describe health and the feeling of being in good health? What factors affect how children manage health?
Methods
Design
The study was part of a project “Health-promoting school” financed and organised by the Swedish National Agency of Education. In the present study children from three health-promoting schools were included and a sequential mixed method design was used [Citation38]. First, age-adapted versions of the SOC questionnaire were collected from younger (8–10 years) and older children (11–15 years), together with the Positive Health Scale (PHS) and Cantril’s ladder of life scale. Second, focus group interviews were conducted with children aged 8–12 years.
Settings and participants
The study was conducted in a rural area in the Northern part of Sweden, where the population density is 1.2 inhabitants per hectare. Tourism industries and small enterprises dominate in terms of business units. The Swedish indigenous people live in this part of the country, i.e. reindeer-herding Sami people. Half of the Sami people speak their native language, and the Sami schoolchildren are taught in Swedish and Sami. Some of the children need to travel by bus between 50 and 70 kilometres in one direction to attend school. In Sweden, elementary school, starting at the age of 6, encompasses 10 years of mandatory schooling.
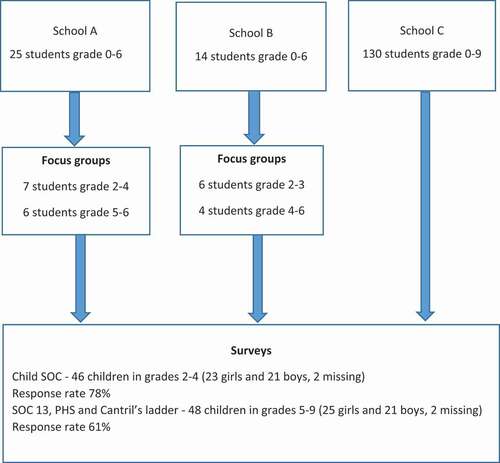
Children from three schools connected to the local project “Health-promoting school” (later referred to as schools A, B, and C) participated in this study. The three schools were recruited through purposive sampling. The total amount of children in the three schools was 170. At these schools, all children in grades 2–6 and their parents were given oral and written information about the study. Children who agreed to participate were also required to obtain informed consent from their parents. In all, 94 children filled in the questionnaires and 23 of these children also took part in focus group discussions.
In total, 94 children participated in the quantitative phase. Forty-six children (23 girls, 21 boys, 2 missing) answered the CSOC and 48 (25 girls and 21 boys, 2 missing) answered the PHS and Cantril’s ladder. Children who did not report their gender were classified as missing and excluded from further analysis. The response rate on the CSOC was 78% in grades 2–4 (8–10 years) and 61% in grades 5–9 (11–15 years). The response analysis showed that only four children in grade 7 and three in grade 8 took part in the survey. This low rate was mostly due to a lack of informed consent from their parents. The data collection procedure is shown in .
Figure 1. Data collection from the three schools
Data collection
Questionnaires
Age-adapted questionnaires on perceptions of health, SOC and the meaning of friends and good health behaviour were collected from 94 children aged 8–15 years (47% boys, 53% girls) from the three schools. Questionnaire items were read out loud by the researcher for the children in their classroom. During this time, the children could ask for clarification of the questions (from 5–8 eight children from each class asked about clarification of the questions). The questions in the Child-SOC needed to be clarified in all classes.
The Child-SOC (CSOC) [Citation39] measures SOC for children from preschool to elementary school and children with learning disabilities. The questionnaire was distributed to 46 children in grades 2–4 (aged 8–10 years). Responses to the CSOC could be given by selecting one of four alternatives from “Never” to “Always”, such as “There is someone who can help me when I need it.“
The SOC-13 [Citation23], measuring SOC (including the dimensions of manageability, comprehensibility and meaningfulness), was distributed to 48 children in grades 5 to 9 [aged 11–15 years). Responses from the SOC-13 could be given by selecting 1 of 7 Likert-type alternatives. As an example, one question was, “Do you feel that you don’t care about what goes on around you?” The seven-point response scale ranged from “Very seldom or never” to “Very often”.
The PHS, validated by [Citation40], measures positive mental and cognitive aspects of health: being alert, happy, relaxed, creative, decisive, finding it easy to concentrate, feeling well, having energy and being social. The questions are worded “In the past 6 months, how often have you … ” and continue with different aspects. The response scale ranges from always to never. The scale ranges from 0 to 36, with a higher score indicative of more positive health.
Cantril’s ladder [Citation41] is a 10-step ladder followed by the text: “Here you see the picture of a ladder. The top of the ladder corresponds to the best life imaginable and the bottom to the worst life you can imagine. If you think about your life in general, where do you think you are right now? Check the box next to the number that best suits you.”
Focus group interviews
To deepen the knowledge of children’s perceptions of health, four focus group interviews were conducted with 23 children of the total sample of 94 children from two (schools A and B) of the three schools who had expressed interest in participating in the interview part of the study. Focus groups can contribute to rich data as discussions in the group are promoted [Citation42]. In this study 23 children (grades 2–6, 8–12 years) participated in the focus group interviews conducted in June 2018. Group 1 consisted of six children in grades 5–6, group 2 six children in grades 2–3, group 3 four children in grades 4–6 and group 4 seven children in grades 2–4. The focus group interviews lasted from 20–30 minutes rendering a total amount of about 2 hours. All interviews were held in a separate classroom. Before the interviews, the children were informed about their right not to answer the questions and withdraw at any time without explanation. They could leave the room if they did not want to participate anymore. Children were asked about their perceptions of health: “What is health?” “What affects health and how you feel? “Is there something you can do by yourself to feel well?” and “How does health relate to how things are going in school?” During the question-answer period, the participating children talked freely with each other and the focus group leader.
Given the difficulty children have in describing such a complex concept as health, a careful and thorough interview was conducted. One author, with extensive experience of interviewing children, conducted all interviews. To obtain a trustworthy description of the children’s responses steps were taken to ensure trustworthiness [Citation43,Citation44]. Confirmation of the results was secured by having all authors engage in the analysis process to negotiate outcome and reflexivity throughout the research process.
Data analysis
Statistical analyses
To assess children’s perceptions of health and their SOC results from three scales were included in the study: CSOC, SOC 13, PHS, and Cantril’s ladder. In the PHS and Cantril’s ladder analyses no age differences were detected, which was likely due to the small sample size.
Cronbach’s alpha was used to evaluate internal reliability. The recommended alpha value is from 0.7 to 0.95 [Citation45]. The analysis led to the following values: CSOC = 0.77, PHS = 0.65, and SOC 13 = 0.26. Because the internal reliability of the SOC 13 was only 0.26, this questionnaire was excluded from further analysis. The Statistical Package for Social Sciences (IBM SPSS Statistics 25) was used to analyse the data.
The Pearson chi-square test was used to assess differences in the CSOC and PHS between boys and girls. Statistical significance was set to p < 0.05. Because of the non-normality of the distribution, the scale was dichotomised by dividing the responses into quartiles, using distribution-based method [Citation46]. That means that the cut off for high positive health was coded 1 and determined to 26+ (scale 0–36) which represent 28,6% (27.3% girls and 30.0% boys) and the lower quartiles (<26) coded 0, indicating low or moderate health. Dichotomising the scale made it easier to analyse potential gender differences and is in line with a cut-off point for positive health [Citation40].
To analyse Cantril’s ladder a binary cut-off of ≥6 was used for high life satisfaction and <6 for low life satisfaction, which is consistent with the Health Behaviour in School-aged Children surveys (HBSC) conducted in more than 40 countries dating back to 2002 [Citation47].
In the analysis all negatively scored items in CSOC were changed to positive scores according to recommendations [Citation48]. The CSOC ranges from 18–72. The scales were dichotomised based on tertiles, which represent 28.08%, based on how the sample was distributed, so-called distribution-based method [Citation46]. The highest tertile indicated high SOC; the cut-off point was ≥51 for CSOC and coded 1. Below 51 was judged as low or moderate SOC and coded 0.
Thematic analysis
The tape-recorded focus group interviews were transcribed verbatim and analysed using thematic analysis [Citation49]. According to Citation49, thematic analysis is a method for identifying, analysing and reporting patterns (themes) within data. A theme captures something important, as a patterned meaning in the data. In the first step the interviews were compiled as one text. All authors applied naïve reading of the text while noting initial ideas. In the next step initial codes were constructed and then collated into different themes. In the last step the themes were reviewed, refined and named. All authors discussed the content of the interviews, participated in the analytical process and contributed to the interpretation of the text. The analysis and interpretation of the results need to be understood in light of the author’s background. None of the authors are from the Sami people. The authors are all middle-aged females and most have a background from middle-sized cities. However, the author responsible for data collection has lived in a rural area with her children for over 20 years and has experience of having her children attending a small school in the countryside. This experience helped her connect with the children in the focus groups.
Ethical considerations
With help from the principal and the teachers at each school, informed consent was sent to and signed by the participating children’s parents. Only children who expressed interest to take part and had a signed informed consent from the parents could participate. All children were informed that participating in the study was voluntary but that they could terminate participation at any time without consequence. The project plan was approved by the Umeå Regional Ethical Review Board (Dnr 2018/190-31).
Results
Reported health
The mean for the PHS (0–36) among the children in grades 5–9 was 21.91, SD 5.056 (girls 21.86, SD 5.759 and boys 21.85, SD 4.428). For the PHS, 27.3% of the girls and 30% of the boys reported high PHS. The chi-square test showed no significant differences between boys and girls. The mean CSOC for children in grades 2–4 was 49.1 for boys and 48.1 for girls. The chi-square test showed no significant gender differences. There were some differences in the CSOC between younger girls and boys (grades 2–4). SOC was high (+51) among 32% of all children. High SOC was reported by 48% of the boys and 22% of the girls. The chi-square test showed no significant differences between boys and girls. Cantril’s ladder (steps 1 to 10) showed a mean of 6.45; high life satisfaction was reported by 73% (n = 48) of the children in grades 5–9. The chi-square test revealed no significant differences between boys and girls.
Children’s perceptions of health
The concept of health and aspects influencing health and wellbeing were further investigated in the interviews. In the analysis four themes were created based on thematic analysis: Understanding health, Managing health, Doing health and Socialising health. The themes are presented below and clarified by the children’s verbatim quotes.
Understanding health
The children explained various aspects of health and how health and wellbeing were perceived. Both younger and older children had a holistic view of health as a concept, with health described as an individual’s living habits and emotions, such as feeling well.
Health was described as holistic.
Yes, health is how well you feel about yourself and how you take care of yourself, and kind of eat good food and move and exercise and a little bit of that, so that you do not eat fast food and stuff like that (group 1).
The children talked mostly about concrete aspects, such as food, eating, sleeping well, and regularly exercising. Both older and younger, but mostly the younger ones, emphasised concrete aspects of an individual’s living habits: “Eating healthy is important for good health”. (group 1) The children also mentioned the connection between health and the body in explaining health, and both the younger and older children stressed the importance of being physically active. Exercising contributed to good health: “Health is when you have [good] condition, your heart beats and you are breathing heavily.” (group 2) Both the younger and older children reported some emotional aspects important to health. They talked about being happy, which was linked to health and the presence of positive emotions was described as important: “Health is to laugh and have fun”. (group 3)
Managing health
The children talked about managing health as the most important determiner of health in daily life. They described the importance of eating healthy and regularly, avoiding fast food and smoking and getting enough sleep. The children explained that the parents were doing what they could to prepare healthy food, but some parents have difficulty doing so because of their long working hours. Late hours and long distances meant that some parents bought home ready to eat food. Getting enough sleep was important to performing and thinking well at school. They were well aware of the relationship between sleeping well and school performance.
The children explained that eating healthy food meant eating homemade food instead of fast food, junk food or semi-manufactured food: “Most of the food you cook at home is healthier.” (group 1). They could point out a good feeling after healthy food: “You feel well in your body when you have been eating healthy food.” (group 3). Milk was preferred over soft drinks: “When you drink soft drinks, you get a sour-feeling stomach but when you drink milk you become happy.” (group 2). They described that families could grow and cultivate some healthy food products at home. In addition to the homemade food, several children said that school food was good: “The best food is at school”. (group 4) They mentioned that it was important not only to eat healthily but also to eat regularly by establishing regular eating habits.
It is also important to eat at the same time, so you adopt a regular eating routine, so one does not eat breakfast at 7 am during weekdays and at noon during the weekend. You also need to eat various kinds of foods, not just to have potatoes on your plate. (group 1)
Several children highlighted how important it was to avoid the dangers of fast food, especially avoiding sugar and sweets. The children gave examples of food that was not considered healthy, such as pizza, potato chips and sweets. As one child explained, “Food you buy in a restaurant and food you don’t cook yourself, food with much fat are not good for your health” (group 1) They had clear views about sugar and sweets: “You get sour in your body when you eat sweets.” (group 2). “Sweets are very addictive.” (group 4). They related the consumption of sugar to illnesses and one child thought that sugar was related to diabetes. Another child said, “Sugar is like cancer – it is really dangerous, but even too much salt is bad.” (group 4) One child described how her father worked far away during the weekdays, and even when he was at home on the weekends, he did not cook any food. Thus, they mostly ate fast food. Another said, “My mother works until 5 o’clock, so she never has time to cook food, so we eat pasta salad 5 days a week. And then maybe we eat something better on Saturdays and Sundays.” (group 1) The children were aware of their parents’ time conflict and talked about the exceptional circumstances the families lived under. One child explained, “The time complicates it and if you have children in kindergarten and at school, and they are very hungry, and then maybe you don’t roll meatballs.” (group 1)
Getting enough sleep was vital in managing health. Children of all age groups talked about sleeping well to cope with school and doing their lessons. Because several children must travel by car to their school, they have to get up incredibly early, which means they must go to bed early. They pointed out that it was the parents who took the responsibility regarding implementing a strict early bedtime. As one child said, “My parents tell me when I need to go to bed.” (group 2) Some children explained that mobile phones kept them awake. Thus, some children left their mobiles outside the bedroom before going to bed. One child described why mobile phones should not be allowed in the bedroom after bedtime. “It is difficult to go to sleep when I have my mobile with me. My brain starts to think and then I cannot sleep, so my mum wants me to leave it downstairs.” (group 1) Several children mentioned the link between sleeping enough and performing at school. Poor sleep resulted in feeling tired at school: “If you are tired when you come to school, you can’t do your school assignments.” (group 1)
Doing bodily health
The children stressed the importance of being physically active during school and leisure time. The children in all age groups were active during school time, emphasising the relationship between exercising/movement during the day and thinking better. The children discussed different activities, the possibility to be active during school time and sport opportunities at school: “We have been talking about having a gym on the schoolyard and we have been talking about why it is good for your health.” (group 4) The children described that if they physically kept active during a school break they acquired new energy and could work better: “If you move a lot during school breaks, you can work better during lessons.” (group 2) Being active led to clearer thinking and not feeling tired during school lessons. If they were looking at their mobiles too much, they became tired.
The children in all age groups were active during leisure time and engaged in several sports depending on the season. Because of the variation in weather and season activities have to be adapted to the weather conditions. During the summer period, they typically cycled, swam, played football and went horseback riding. In the winter they drove a snowmobile, snowracer or went downhill/cross-country skiing. One child drove a dog sled. They trained in handball, floorball and gymnastics indoor. Thus, all participants were engaged in one or more sports. To be physically active was something natural, as one child said: “When you are a child, you move a lot outdoor both during summer and winter, so you do a lot during leisure time.” (group 4) Exercising was experienced as mostly positive, but too much exercise could lead to adverse health consequences, as one girl explained:
If you make these exercise schedules, you should not use apps, … people get eating disorders and want to lose weight and stuff. It’s not good … and then it becomes more exercising than eating. (group 1)
Thus, finding a balance between exercise, food intake and moving for joy was important.
Socialising health – living in a rural context
Health was also experienced through interaction with parents, grandparents, friends and teachers. The quality of relationships, parents’ capacity to enable children’s activities and children solving problems with friends contributed to the overall social health experience.
The importance of parents was described as crucial due to the long travel distances. Thus, parents were vital to ensure that the children could attend various activities. Several children explained that their parents had long working hours and cared for more than one child. Under these circumstances, the children thought that their parents did as well as they could. As one child said, “The parents make children feel good, loved and wanted.” (group 4)
Some children explained that the project inspired their parents. One child described this as, “My mom gets inspired when she sees other people being out and moving. So she said, “come on kids, now we’ll go out.” (group 3) Another child said, “I help my grandma in the strawberry field and that makes me feel good.” (group 3).
The children described the importance of teachers. Teachers who supported the children in being active and showed a health promotive attitude were highly valued. The children explained that the teachers had an impact on their attitudes towards exercising and sports. Teachers influenced the children’s thinking and planned joint school activities in the schoolyard. One child noted, “We have been talking a lot about health at school with our teacher and that we are going to have an outdoor gym.” (group 4). Sometimes the involvement in physical activities started thanks to one active teacher. That we make excursions and move more, it all started when the new teacher came. She was a gymnastics teacher (group 3). The teacher not only talked about health but also explained why it was important to exercise: “We have been talking at school about why it is beneficial for health to exercise.” (group 4).
Connecting with friends in their limited networks was needed to maintain and nurture social contacts given that they were living in a sparsely populated area. The children knew each other at school and they also knew the children’s families, their age, where they lived and so on. The children described the surrounding area as familiar, known and safe. However, having no options to choose new friends, they must come to terms with each other and resolve conflicts. Some children lived far away from each other, which hindered leisure time contact. One child explained that it was 30 km to her best friend. Friends were particularly important: “I think friends are playing quite a big role.” (group 1). Connecting with friends was often a priority: “When I am at home, I chill or mostly play with my friends.” (group 2). The children sometimes entered into conflicts with each other and the importance of resolving possible disputes was highlighted.
If you become unhappy at school, the teacher notices it pretty quickly and then you tell, but if it happens in your leisure time … it will take a while to make it all right again (group 1).
The children emphasised the need to resolve disagreements: “If you become enemies, you will try to sort it out.” (group 1)
Living in a sparsely populated area presented some limitations regarding arranging social contacts and opportunities to practise sports. The environment constituted a unique frame for social contacts. The children described uncertainty about participating in sports or other activities. The leaders of the activities could be older siblings, a parent or a teacher. The children’s opportunities were limited because of life changes, such as when the leader moved to another place, was on parental leave, changed workplace or other reasons. Because of these sudden changes, the children could not continue their favourite sport or other activity. Thus, in addition to being dependent on their parents, they were forced to choose activities that were not always their first choice.
Discussion
This study aimed to investigate the children’s SOC and their perceptions of health, i.e. how children consider their SOC, their description of health, the feeling of being in good health and what factors affect how they manage health.
Gender and age differences in managing health
C-SOC for younger children aged 8–10 years (grades 2–4) showed some gender differences, with 48% of the boys and 22% of the girls reporting high SOC, although these differences were not significant. Although our results are modest and inconclusive, the knowledge of children’s knowledge is important given that SOC seems to be associated with perceived health [Citation21,Citation50,Citation51]. Perceived health is associated with physical activity [Citation21]. Boys tend to self-rate their health higher than girls [Citation52–54]. Moreover, boys are more likely to take part in sports than girls [Citation55–59]. Self-reported higher levels of health and wellbeing among boys may be linked to a fear of concealing health-related problems [Citation60]. These results suggest a gender-sensitive health policy to support holistic health. By influencing children’s attitudes and values, schools play a vital role in addressing the healthy behaviours of children.
Based on the PHS, there were no gender differences in experiencing positive health. About a third of the boys and girls reported high PHS: mean PHS (0–36) among the children in grades 5–9 was 21.91, SD 5.056 (girls 21.86, SD 5.759 and boys 21.85, SD 4.428). Our mean scores are slightly lower than those in a previous study [Citation40]. The analysis of the Cantril’s ladder showed a mean of 6.45. This value is less than the mean of 7.22 in Swedish children aged 11 to 16 years [Citation61]. A previous study [Citation62] found that a lower SOC was consistently related to higher levels of loneliness, lower social status, and lower academic functioning. The present sample consisted of children living in a rural area. Some of these children were from the Sami population, but as ethnicity was not included in the questionnaire, the precise number of Sami children is unknown. Evidence suggests that health-related quality of life is lower among Sami schoolchildren than among Swedish schoolchildren in general [Citation63]. Some age differences were observed from the focus groups, i.e. older children have the ability to see and reflect on the link between living habits and health more clearly than younger children. Mostly, the children talked about food and the difference between junk food and healthy food. Even the younger children knew what food was good for them and what food negatively affected their health. Sugar was particularly described as terrible and dangerous. A similar finding was reported in a study investigating children’s (grades 5–6) perceptions of sugar-sweetened beverages. The study showed that the participants highly aware of the adverse health effects of sweet beverages [Citation64]. However, the children in our study could not resist eating sweets or fast food, despite knowing the impact of such food on their health.
The older children conveyed that they knew their health behaviours. They avoided certain dishes because they considered them unhealthy. They mentioned weight loss apps as dangerous because of the risk of becoming overly obsessed with using these apps, leading to exercising too much and eating too little. They exercised because they know that it is good for them, and sports activities were discussed as acts of enjoyment, especially when the activity was their choice. Some activities ended because of the lack of leaders or teachers taking on parental leave, making the activities person-dependent and temporary. They were well aware of the link between mind and body and that their body was an essential source for good health.
Describing health and the feeling of being in good health
The participants described health as holistic. Their descriptions depicted health as a theoretical concept. Consistent with other findings [Citation30,Citation33], the children could specify aspects that contributed to health. The participants’ main focus was on how to live everyday life. The children emphasised the importance of eating healthy food in general and eating healthy, homemade food in particular. In addition, they underlined the importance of regular physical activity and getting sufficient sleep to be at their best in school.
The children showed awareness that their daily behaviour had a significant effect on their schoolwork and health. The participants were also aware that lack of sleep negatively affects academic performance. Shorter sleep duration affects children’s physical health, cognitive ability and mood [Citation65,Citation66]. Despite their knowledge of the importance of a good night’s sleep, they depended on their parents’ support in controlling bedtime hours and taking care of mobile phones. A meta-analysis investigating children’s sleep confirmed an overall decline of 0.76 min/year in the past century [Citation66]. This study suggests that knowledge is not enough and children’s sleeping habits must be carefully monitored.
Children’s perceptions of health in this study can be related to the original three SOC elements, namely comprehensibility, manageability and meaningfulness [Citation23], as SOC reflects the individual’s capacity to deal with everyday life and perceive life as comprehensible, manageable and meaningful. The children mostly emphasised the manageability of health, but also the comprehensibility of health. Manageability had to do with aspects of doing, feeling and socialising health. In this respect the children claimed to have the necessary resources to deal with different life situations and adapt to varying conditions. Comprehensibility entailed an understanding of the concept of health and what affected health. The older children could also reflect and express awareness and understanding. In their descriptions health was related to both mind and body. The children did not talk about specific aspects that could be directly connected to meaningfulness, except when they mentioned health’s importance. Meaning-making may not be their focus of attention because of the early age of the children and that health was more about doing than about thinking.
Social aspects influencing health
Social contacts were valued as important and influenced children’s health behaviours. Our results indicated that the teachers impacted children’s attitudes towards physical activities, as they provided tangible knowledge of the relationship between health and exercise to inspire the children. One study investigating school climate and perceived health found that school climate was mostly related to health at an individual level, but better heath was reported in classes with helpful teachers [Citation67]. The teachers in this study played a key role in influencing young schoolchildren and are instrumental in how the schoolyard could be improved for outdoor activities. Some children mentioned having learned about health in school.
In addition to the leaders, social support from other sources (e.g. parents and peers) was important in socialising health. In our study, the children were aware of the importance of physical activity but identified barriers to organised activities, such as geographic distance. Safe areas are known to facilitate physical activity among children and youth in rural areas [Citation68,Citation69], children would be given opportunities to socialise health in their close neighbourhood. Having a neighbourhood with safe outdoor and indoor areas would likely facilitate children meeting their peers in person (e.g. in spontaneous play and physical activity regardless of the weather condition (i.e. even under poor weather conditions).
In the children’s daily life parents seemed to play an important role in offering a time frame and suggestions for prioritising and pacing efforts to accomplish various tasks. Children saw their parents as a supporter in bedtime/hours of sleep, food choice and enabler or catalyst for specific physical activities during leisure time. When children in the study talked about their leisure interests, they were often dependent on their parents’ ability to take them to activities that were often several miles away. One study that included 11–14-year-old children found that family structure plays a vital role in how children are physically active. Another study found that children from single-parent families were more sedentary than intact families [Citation70]. In this study the children emphasised that they had to choose local activities because of long travel distances and parents lack of time. They were obliged to be active in seasonal sports and those that were offered. How the children were active was determined not only by their desire but also by the surrounding possibilities. The isolation forced them to live under relatively closed conditions.
A study conducted among rural children showed that the children perceived a lack of social capital due to environmental constraints, even though their wellbeing was enhanced by strong cohesion [Citation1]. Another study found that social capital formed an important basis for primary schoolchildren’s participation in physical activity and that key social influencers shifted from family to peers [Citation71]. Little is known about context in social capital research, especially regarding how context interacts with promoting dynamic health [Citation72Citation73]. The concept of rural life is vague and complex. For instance, Citation1,found that rural children in grade 6 experienced competing feelings about living in a rural area: On the one hand, they felt protected and safe but at the same time they felt isolated and restricted. In keeping with Eriksson our study shows that living in a rural area meant that the children had to rely on their parents to drive them to meet friends and participate in activities. Such a situation can lead to dependence. Still, a rural context was seen as promoting cohesion. The current results show that rural children could have other challenges than the average child in Sweden living in an urban setting that could positively or negatively affect their health.
The children’s strong cohesion in this study was due to their ability to solve conflicts with other children as they have no or few options to choose new friends. The participating children have the resources and strategies to cope with daily life stressors, show understanding of their parents’ circumstances, and adapt their lifestyle to rural circumstances.
Study limitations
One significant limitation concerns the quantitative results of the study. Several questionnaires (CSOC, SOC13, PHS and Cantril’s ladder) were used in different age groups and relatively few children answered the questionnaires. Also, the sample was small, which may have contributed to difficulties in discovering gender differences. Another limitation was the children’s lack of understanding of the questions in the SOC instruments. The CSOC was translated from English to Finnish-Swedish, a similar language as Swedish but with some differences in expressions that may have affected the questions’ understandability. On the other hand, the children could ask for clarification while the interviewer read aloud the questions, which may have contributed to a correct understanding of the questions. Moreover, the children asked questions when they did not understand a question, and the author gave explanations that the other children also heard. Thus, a potential interviewer effect and bias need to be considered. A new validated translation and test-retest are necessary for future use of the CSOC instrument.
The dropout rate was high in the older children (grades 5–9), and was most likely caused by a lack of information from teachers to parents, leading to parents not giving informed consent. However, our data enabled us to use some descriptive statistics in which no significant differences were found. Another limitation entails the transferability of the results. Because the study was conducted in one setting in a rural area in Northern Sweden, this may limit the results’ transferability to other settings.
Conclusions
Children are influenced by the context in which they live. The study shows that schools in rural areas can provide a healthy environment and that teachers with a health-promotive attitude can influence schoolchildren to be more physically active. For the schoolchildren, understanding the importance of and experiencing good health and high SOC are essential prerequisites for optimising school education. In a rural setting children need to adapt to the few regular opportunities for activities in their immediate environment. Accessible outdoor areas and indoor facilities should be addressed when formulating rural child and youth health policies. Finally, activities during school hours can complement leisure time activities in promoting health and wellbeing.
The nine item Positive Health Scale (PHS) together with response scores
Items Response score Always Often Sometimes Rarely Never
In the last 6 months how often have you,
1. Been alert?
2. Been happy, optimistic?
3. Felt calm and relaxed?
4. Been creative?
5. Been decisive?
6. Found it easy to concentrate?
7. Felt well?
8. Had a lot of energy?
9. Been functioning well in contact with other people?
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Eriksson U, Asplund K, Sellström E. Growing up in rural community-children’s experiences of social capital from perspectives of wellbeing. Rural Remote Health. 2010;10(3):1322.
- Kawachi I. Commentary: social capital and health: making the connections one step at a time. Int J Epidemiol. 2006;35(4):989–12.
- Ziersch AM, Baum F, Darmawan IGN, et al. Social capital and health in rural and urban communities in South Australia. Aust N Z J Public Health. 2009;33(1):7–16.
- Portes A. Social capital: its origins and applications in modern sociology. Annu Rev Sociol. 1998;24(1):1–24.
- Villalonga-Olives E, Kawachi I. The dark side of social capital: a systematic review of the negative health effects of social capital. Soc Sci Med. 2017;194:105–127.
- Comer JP. Developing social capital in schools. Society. 2015;52(3):225–231.
- Eriksson M. Social capital and health – implications for health promotion. Glob Health Action. 2011;4(1):5611.
- Larson JS. The conceptualization of health. Med Care Res Rev MCRR. 1999;56(2):123–136. Retrieved from: http://www.ncbi.nlm.nih.gov/pubmed/10373720
- Ott MA, Rosenberger JG, McBride KR, et al. How do adolescents view health? Implications for state health policy. J Adolesc Health. 2011;48(4):398–403.
- White K. An introduction to the sociology of health and illness. Los Angeles: SAGE; 2009.
- WHO. Constitution of the world health organization. Forty-fifth ed, Supplement. [2006October], Geneva. Retrieved from: http://www.who.int/governance/eb/who_constitution_en.pdf
- Nutbeam D. Health promotion glossary. Health Promot Int. 1998;13(4):349–364.
- Russell RD. Social health: an attempt to clarify this dimension of well being. Int J Health Educat. 1973;16(2):74–84. Retrieved from: http://www.scopus.com/inward/record.url?eid=2-s2.0-0015802545&partnerID=40&md5=eaa53b95600c290d48f9a23153b65fb5
- WHO. (2004). Promoting mental health: concepts, emerging evidence, practice: summary report. Retrieved fromWorld Health Organization, 20 Avenue Appia, 1211Geneva 27, Switzerland.
- Eriksson, U., Hochwälder, J., Carlsund, Å., & Sellström, E. (2012). Health outcomes among Swedish children: the role of social capital in the family, school and neighbourhood. Acta Paediatrica, 101(5), 513–517.
- Button B, Trites S, Janssen I. Relations between the school physical environment and school social capital with student physical activity levels. BMC Public Health. 2013;13(1):1191.
- Mitchell CA, Clark AF, Gilliland JA. Built environment 935 influences of children’s physical activity: examining differences by neighbourhood size and sex. Int J Environ Res Public Health. 2016;13(1):130.
- Prins RG, Beenackers MA, Boog MC, et al. Neighbourhood social capital as a moderator between individual cognitions and sports behaviour among Dutch adolescents. Soc Sci Med. 2014;105:9–15.
- Joens-Matre RR, Welk GJ, Calabro MA, et al. Rural–urban differences in physical activity, physical fitness, and overweight prevalence of children. J Rural Health. 2008;24(1):49–54.
- Tsimeas P, Tsiokanos A, Koutedakis Y, et al. Does living in urban or rural settings affect aspects of physical fitness in children? An allometric approach. Br J Sports Med. 2005;39(9):671–674.
- McCormack LA, Meendering J. Diet and physical activity in rural vs urban children and adolescents in the USA: a narrative review. J Acad Nutr Diet. 2016;116(3):467–480.
- Honkinen P-LK, Suominen SB, Välimaa RS, et al. Factors associated with perceived health among 12-year-old school children. Relevance of physical exercise and sense of coherence. Scand J Public Health. 2005;33(1):35–41.
- Braun-Lewensohn O, Idan O, Lindström B, et al. (2016). Salutogenesis: sense of coherence in adolescence. In.
- Antonovsky A. Unraveling the mystery of health: how people manage stress and stay well. San Francisco, Calif.: Jossey-Bass; 1987.
- Olsson M, Hansson K, Lundblad AM, et al. Sense of coherence: definition and explanation. Int J Social Welfare. 2006;15(3):219–229.
- Mittelmark, M. B., Sagy, S., Eriksson, M., Bauer, G. F., Pelikan, J. M., Lindström, B., & Arild Espnes, G. (2017). The handbook of salutogenesis. Springer Nature.
- Landstedt E, Asplund K, Gillander Gådin K. Understanding adolescent mental health: the influence of social processes, doing gender and gendered power relations. Sociol Health Illness. 2009;31(7):962–978.
- MacLean A, Hunt K, Sweeting H. Symptoms of mental health problems: children’s and adolescents’ understandings and implications for gender differences in help seeking. Children Soc. 2013;27(3):161–173.
- Pridmore P, Lansdown R. Exploring children’s perceptions of health: does drawing really break down barriers? Health Educ J. 1997;56(3):219–230.
- Eves, A., Bielby, G., Egan, B., Lumbers, M., Raats, M., & Adams, M. (2006). Food hygiene knowledge and self-reported behaviours of UK school children (4-14 years). British Food Journal, 108(9), 706-720.
- Piko BF, Bak J. Children’s perceptions of health and illness: images and lay concepts in preadolescence. Health Educ Res. 2006;21(5):643–653.
- Almqvist L, Hellnäs P, Stefansson M, et al. ‘I can play!’Young children’s perceptions of health. Pediatric Rehabilitat. 2006;9(3):275–284.
- Nordenfelt L. On the nature of health: an action-theoretic approach. Dordrecht: Kluwer; 1995.
- Reeve S, Bell P. Children’s self‐documentation and understanding of the concepts ‘healthy’and ‘unhealthy’. Int J Sci Educat. 2009;31(14):1953–1974.
- Mouratidi P-S, Bonoti F, Leondari A. Children’s perceptions of illness and health: an analysis of drawings. Health Educ J. 2016;75(4):434–447.
- Bir JE, Podmore VN. Children’s understanding of health and illness. Psychol Health. 1990;4(2):175–185.
- Langford R, Bonell CP, Jones HE, et al. The WHO health promoting school framework for improving the health and well‐being of students and their academic achievement. Cochrane Database Syst Rev. 2014;(4). DOI:https://doi.org/10.1002/14651858.CD008958.pub2.
- World Health Organization. (1986). The Ottawa charter for health promotion: first international conference on health promotion, Ottawa, 1986 Nov 21. Geneva: WHO.
- Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches. Thousand Oaks: SAGE Publications; 2014.
- Margalit M, Efrati M (1995). Sense of coherence, companionship, and loneliness among children with learning disorders. Paper presented at the annual conference of the Society for Research in Child Development, Indianapolis.
- Warne M, Snyder K, Gådin KG. Adaptation and validation of a positive health scale for adolescents. Social Indic Res. 2014;119(2):1079–1093.
- Cantril H (1965). Pattern of human concerns. Rutgers University Press.
- Morgan DL (2002). Focus group interviewing. Handbook of interview research: Context and method, 141–159.
- Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112.
- Lincoln YS, Guba EG. Naturalistic inquiry. Beverly Hills, Calif.: Sage; 1985.
- Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55.
- Streiner DL, Norman GR. Health measurement scales: a practical guide to their development and use. J Epidemiol Community Health. 2008;59:250–251.
- Levin KA, Currie C. Reliability and validity of an adapted version of the cantril ladder for use with adolescent samples. Social Indic Res. 2014;119(2):1047–1063.
- Bengel J, Strittmatter R, Willmann H (1999). What keeps people healthy. The current state of discussion and the relevance of Antonovsky’s salutogenic model of health. Cologne: Federal Centre for Health Education (FCHE).
- Braun V, Clarke V. Using thematic analysis in psychology. Qualitative research in psychology. Qual Res Psychol. 2006;3(2):77–101.
- Apers S, Luyckx K, Rassart J, et al. Sense of coherence is a predictor of perceived health in adolescents with congenital heart disease: a cross-lagged prospective study. Int J Nurs Stud. 2013;50(6):776–785.
- García-Moya I, Rivera F, Moreno C. School context and health in adolescence: the role of sense of coherence. Scand J Psychol. 2013;54(3):243–249.
- Breidablik HJ, Meland E, Lydersen S. Self-rated health in adolescence: a multifactorial composite. Scand J Public Health. 2008;36(1):12–20.
- Jerdén L, Burell G, Stenlund H, et al. Gender differences and predictors of self-rated health development among Swedish adolescents. J Adolescent Health. 2011;48(2):143–150.
- Moksnes UK, Espnes GA. Stress, sense of coherence and subjective health in adolescents aged 13–18 years. Scand J Public Health. 2017;45(4):397–403.
- Button BL, Shah TI, Clark AF, et al. Examining weather-related factors on physical activity levels of children from rural communities. Can J Public Health. 2020;111(1):1–8.
- Evans JR, Wilson R, Coleman C, et al. Physical activity among indigenous Australian children and youth in remote and non-remote areas. Soc Sci Med. 2018;206:93–99.
- Hong J, Choo J, Kim H-J, et al. Gender-specific correlates of sufficient physical activity among vulnerable children. Japan J Nurs Sci. 2020;17(1):e12278.
- Larouche R, Blanchette S, Faulkner G, et al. Correlates of children’s physical activity: a Canadian multisite study. Med Sci Sports Exerc. 2019;51(12):2482–2490.
- Sterdt E, Liersch S, Walter U. Correlates of physical activity of children and adolescents: a systematic review of reviews. Health Educ J. 2014;73(1):72–89.
- Randell E, Jerdén L, Öhman A, et al. Tough, sensitive and sincere: how adolescent boys manage masculinities and emotions. Int J Adolesc Youth. 2015;20:1–13.
- Looze MED, Huijts T, Stevens GWJM, et al. The happiest kids on earth. Gender equality and adolescent life satisfaction in Europe and North America. J Youth Adolesc. 2018;47(5):1073–1085.
- Idan O, Braun-Lewensohn O, Lindstrom B, et al. (2017). Salutogenesis: sense of Coherence in Childhood and in Families. The Handbook of Salutogenesis, 107.
- Omma L, Petersen S (2013). Health-related quality of life in Sami schoolchildren in Sweden.
- Battram DS, Piché L, Beynon C, et al. Sugar-sweetened beverages: children’s perceptions, factors of influence, and suggestions for reducing intake. J Nutr Educ Behav. 2016;48(1):27–34.e21.
- Chaput J-P, Gray CE, Poitras VJ, et al. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41(6):S266–S282.
- Matricciani L, Bin YS, Lallukka T, et al. Past, present, and future: trends in sleep duration and implications for public health. Sleep Health. 2017;3(5):317–323.
- Modin B, Östberg V. School climate and psychosomatic health: a multilevel analysis. Sch Eff Sch Improv. 2009;20(4):433–455.
- Button BLG, Tillmann S, Gilliland J. Exploring children’s perceptions of barriers and facilitators to physical activity in rural Northwestern Ontario, Canada. Rural Remote Health. 2020;20(3):5791.
- Moore JB, Jilcott SB, Shores KA, et al. A qualitative examination of perceived barriers and facilitators of physical activity for urban and rural youth. Health Educ Res. 2010;25(2):355–367.
- Quarmby T, Dagkas S. Children’s engagement in leisure time physical activity: exploring family structure as a determinant. Leisure Stud. 2010;29(1):53–66.
- Everley S, Everley K. Primary school children’s experiences of physical activity: the place of social and cultural capital in participation and implications for schools. Early Child Develop Care. 2019;189(12):2032–2042.
- Shiell A, Hawe P, Kavanagh S. Evidence suggests a need to rethink social capital and social capital interventions. Soc Sci Med. 2020;257:111930.