
ABSTRACT
Southern Westfjords of Iceland is a sparsely populated, remote area with rather high proportion of older residents. This study´s aim was to investigate activities and participation in this population, using a descriptive cross-sectional population-based design. The participants were 129 community-dwelling residents, 65–91 years old. The Late Life Function and Disability Instrument was used to measure participants’ activities and participation. It provides interval scale scores where a higher score means less difficulties in activities, more frequent participation, and fewer participation restrictions. Participants had most difficulties in Advanced Lower Extremity functioning and least in Upper Extremity functioning and scored lower on participation frequency than participation restriction. Overall, men reported fewer difficulties in activities than women and the 65–74 years group fewer difficulties than the 75–91 years group. Frequency of participation was higher for women than men and higher for the younger group than the older one who also experienced their participation to be more limited, but men and women did not differ. The participants described barriers limiting their participation in self-care and social life. The results provide valuable information on activities and participation of older residents living rurally and have practical implications for community services in remote arctic areas.
Background
The life expectancy of Icelanders is high and the proportion of older people in the general population is increasing as in the other Nordic countries [Citation1]. In old age, there is an increased likelihood that people will live with chronic health conditions and dysfunctions affecting their daily activities and social participation [Citation2–4] which can be challenging for older adults, their families and the society [Citation5]. Research results indicate that through appropriate interventions, including an encouraging environment, it is possible to enhance functioning in terms of activities and participation, and thereby improve the lives of older citizens [Citation5]. Therefore, it is important to identify common and potential disabilities among older adults.
Southern Westfjords of Iceland is a sparsely populated, remote and arctic area, where the proportion of older adults has grown steadily in recent years, faster than in the country as a whole [Citation6]. Yet there is a lack of information on these older residents´ health and functioning in daily life. As an example of this ageing among the residents of Southern Westfjords [Citation6]: in 1992, only 9.2% of the residents had reached 65 years of age, the same as for the total Icelandic population; in 2013, the proportion of older residents was 13.6%, which was higher than for the total population (12.9%); and finally in 2019 the proportion of older residents was up to 16.7% while only 14.2% in the total population.
The Icelandic Act on the Affairs of the Elderly clearly states that every older person has the right to live in his/her own home and receive appropriate health and social services [Citation7]. Older people who need help with household chores and/or personal care are entitled to home care services which are provided by the municipalities on the basis of the Municipal Social Services Act[Citation8]. For such services to be appropriate, those who plan and provide them must have accurate information on the functioning, disability, and health of the older population. Therefore, researchers and health and social service providers need to join forces and prepare society for the foreseeable increase in the oldest age group by monitoring and utilising information on the epidemiology of disability among older people, including those who live in sparsely populated and remote areas.
Functioning, disability and health are not easily measured, but these are the core concepts of the International Classification of Functioning, Disability and Health (ICF) [Citation9]. According to the ICF, the functioning and disability of an older adult depends on the interaction between his/her underlying health conditions and contextual factors. Functioning and disabilities are, among other things, manifested in people’s activities and participation, which again have a strong connection to independence and general well-being in old age [Citation10]. In the ICF, activity is defined as an individual’s execution of a task or action and participation as a person’s involvement in life situations [Citation9].
The purpose of this research was to investigate activities and participation among community-dwelling older adults in Southern Westfjords of Iceland both in total and by gender and age-group. More specifically, the aim was to study older adults’ (a) abilities/difficulties in discrete actions or daily activities, (b) frequency of participation in socially defined life tasks, and (c) experienced limitations in the capacity to participate in socially defined life tasks.
Methods
Research area
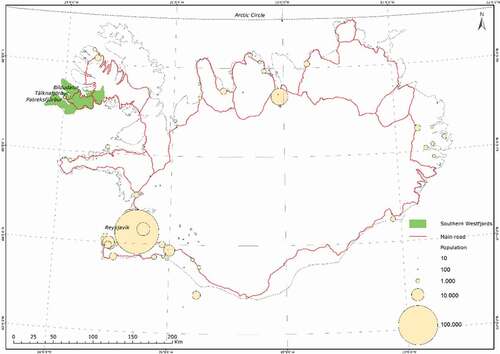
The research was conducted in the Southern Westfjords of Iceland, which includes two municipalities covering over 1500 square kilometres (150000 Hectares) of land. The residents lived either in one of the three villages (Patreksfjordur, Talknafjordur and Bildudalur) or the surrounding rural area ().
Figure 1. A map of the research area, Southern Westfjords (published with permission from the National Land Survey of Iceland)
Participants
The study population included all community-dwelling residents of Southern Westfjords who had reached the age of 65. In 2013, when data was collected, this group represented 161 out of 1240 individuals who at that timed lived in the study area. Statistical power analysis, using G*Power 3.0 showed that a minimum of 128 participants was required to reach a medium effect size (Cohen’s d = 0.5) [Citation11]. The calculations were based on an independent t-test, (1-β = 0.80, α = 0.05) and a two-sided test. Based on a predicted 80% participation rate, we sampled the total study population (161 individuals * 0.8 = 128.8)
Ethics
The research was approved by the Ethics Committee of Akureyri Hospital (No. 1/2013). Names, addresses and social security numbers of the 161 potential participants, were obtained from the National Registry of Iceland. Information letters were sent to these individuals and they were asked to participate in the study. A phone call followed the letters. The researchers were unable to contact seven persons, another seven were away from the research area during the study period, and 15 refused to participate. In total, the actual sample contained 129 older adults out of 161, or 80.1% of the total population sample.
Procedure
One of the researchers (MB) visited all the participants in their homes and collected data via face-to-face interviews and testing. On average, each visit lasted approximately one hour, and the data collection period spanned six months in total (April through June and September through November 2013). At the beginning of the visit, ethical aspects of the study were discussed, and the study procedures were explained in detail before the participant signed an informed consent. Next, the participants gave relevant background information on a selection of contextual factors (e.g. age, gender, education, services received from the community and chronic health conditions). Thereafter, the standardised Late-Life Function and Disability Instrument (LLFDI) was administered following the protocol presented in the LLFDI’s manual () [Citation12–14]. Additionally, those who described their participation as restricted on LLFDI disability component (somewhat, a lot, or completely) were asked to identify/name the perceived barriers. Finally, the participants completed the Mini Mental State Examination (MMSE)[Citation15].
Figure 2. Structure and scales of the Late Life Function and Disability Instrument (LLFDI) and number of items belonging to each scale
Late-life function and disability instrument
The LLFDI was designed to assess two distinct outcomes of function and disability among community-dwelling adults, 60 years of age and older [Citation12–14]. Although the conceptual base of the LLFDI is Nagi’s disablement model [Citation16], the instrument can be used to capture and distinguish the ICF’s activities and participation components [Citation17]. The LLFDI has been used in research on older people in Nordic countries, including Iceland [Citation2,Citation18,Citation19]. It is designed for an interview setting and follows a standard protocol that is described in detail in the manual[Citation14]. The LLFDI produces measures with good psychometric properties in older community-dwelling populations, which supports its use in gerontological research [Citation12–14,Citation19-21]. demonstrates how the LLFDI contains a total of 64 items which are the basis for 10 interval scales, four describing activities and six describing participation.
The LLFDI function component measures activities and includes 32 questions on difficulty in performing discrete actions or activities without help from others [Citation13,Citation14]. Participants are given examples of what may influence difficulty in task performance including: pain, fatigue, fear, weakness, soreness, and health conditions. Participants who use assistive devices for mobility are asked additional questions about their performance with these devices. All questions are phrased “How much difficulty do you have … ? Response options (for each question) are on a 5 to 1 rating scale ranging from no difficulty in performing (“none” = 5) to “cannot do” (1). The answers are summed up and transformed to scaled scores for Activities (total) and three sub-domains: Upper Extremity functioning (activities involving the hands and arms, e.g. “holding a full glass of water in one hand”), Basic Lower Extremity functioning (activities primarily involving standing, stooping, and walking, e.g. “stepping on and off a bus”), and Advanced Lower Extremity functioning (activities involving a high level of physical ability and endurance, e.g. “running 1/2 mile or more”). All four activities scaled (interval) scores can range from zero to 100 where a higher score means better functioning.
The LLFDI disability component measures participation and includes 32 questions on a person’s performance of socially defined life tasks expected of an individual within a typical sociocultural and physical environment” (such as housekeeping or organised social activities) [Citation12,Citation14]. The component includes two separate dimensions, Participation frequency and Participation restrictions, with 16 questions each. The first 16 questions evaluate the individual´s participation frequency or regularity of performing life tasks and the other 16 evaluate limitations (due to contextual factors) in the capability of performing life tasks (participation restriction). Participation frequency questions are all phrased, “How often do you do … ?” with response options ranging from “very often” (5) to “never” (1). An example is “How often do you visit friends or family in their homes?” The answers are summed up and then transformed to scaled scores for Participation frequency (total) and two sub-domains. These are Social role for items reflecting the frequency of performing various social and community tasks, and Personal role for items reflecting the frequency of performing various personal tasks. Participation restriction questions are phrased, “To what extent do you feel limited in … ?” with response options ranging from “not at all” (5) to “completely” (1). An example here is “To what extent do you feel limited in visiting friends or family in their homes?” The answers are summed up and then transformed to scaled scores for Participation restriction (total) and two sub-domains, Instrumental role for items reflecting limitations in activities at home and in the community, and Management role for items reflecting limitations in organisation or management of social tasks. All participation scaled (interval) scores range from zero to 100 where a higher score means better functioning.
Data analysis
The IBM SPSS Statistics for Windows (version 26.0) was used for statistical analysis. Descriptive statistics provided information on all variables´ central tendencies, distribution, frequencies, and proportions for all participants and by groups: men versus women and younger (65–74 years) versus older (75–91 years) age group. To identify significant differences between groups, an independent sample t-test was used on continuous variables that met the criteria for parametric tests, a Chi-square test was used for all dichotomous background variables, and a Mann-Whitney U test was used for the ordinal variable self-rated health. The level of significance was set at p < 0.05, and repeated testing was not corrected for. Finally, the ICF [Citation8] was used as a framework to categorise participants’ barriers into: (a) health conditions or body function, (b) environmental factors, and (c) personal factors.
Results
Participants’ characteristics
Participants (N = 129) were from 65 to 91 years old, 52.7% were women and all spoke Icelandic. presents the background characteristics of the participants in total and analysed by gender and age group. Compared to men, more women lived alone, had family and friends in the neighbourhood, and received informal caregiving, but fewer drove a car. Comparing younger-old (65–74 years) and older-old (75–91 years) participants revealed differences on all background characteristics, except on having children. The younger group scored higher on the MMSE, and additional analysis of MMSE scores for all participants showed that 94 (72.9%) scored 27–30 (out of 30), 29 (22.5%) scored 22–26 and six (4.7%) scored 17–20.
Table 1. Background characteristics (demographics and health) of community-dwelling adults aged 65 to 91 years and older in Southern Westfjords of Iceland, by gender and age group
Activities and participation
presents the results from all ten LLFDI scales in total, by gender and age group. Within the LLFDI activity scales, participants reported having the most difficulties in the Advanced Lower Extremity functioning and the fewest in the Upper Extremity functioning. Within the LLFDI participation scales, participants scored lower on participation frequency than participation restriction.
Table 2. Activities and participation of community-dwelling adults aged 65 to 91 years old in Southern Westfjords of Iceland, by gender and age group
Analysis of the LLFDI results by gender showed that overall, men scored higher than women on the activity scales, except for Basic Lower Extremity functioning where gender difference was not significant. Despite women’s greater difficulty in activities, they scored significantly higher than men on LLFDI participation frequency and did not report more LLFDI participation restrictions than men.
Analysis of the LLFDI results by age showed that overall, the younger age group scored higher than the older one on nine out of ten measures of activity and participation. One LLFDI scale, Personal role, reflected no differences.
Majority of participants (61.2%) indicated at least one item in which participation was somewhat, a lot, or completely restricted due to internal or external barriers. Reporting participation restrictions was significantly (p = 0.012) more prevalent in the older age group than the younger, but the prevalence was the same (p = 0.816) among women and men. Barriers were varied (see ) and reflected participants’ health conditions (e.g. rheumatic diseases), impaired physical function (e.g. lack of balance or self-confidence), social environment (e.g. lack of assistance or encouragement), physical environment (e.g. geographical isolation), and personal factors (e.g. lack of interest or daily routine). A few barriers were labelled as “other/unclassified”, yet linked to the health condition, physical function or mental function.
Figure 3. Most commonly mentioned barriers to participation in the total sample (N = 129). The number of participants stating a given barrier is shown in parentheses
Discussion
This research reveals the overall prevalence of activities, participation frequency and participation restrictions among older community-dwelling adults. The results confirm that with increasing age, older-old community-dwelling adults are more likely than younger-old to report difficulties in a variety of activities in their daily lives. Furthermore, higher age was generally associated with a less frequent participation and more participation restrictions. Overall, participation frequency was low. However, the respondents did not necessarily associate low participation frequency with participation restrictions, as the scores on all the LLFDI participation restriction scales were relatively high. Women described more difficulties in activities than men, but this was not reflected in lower scores in participation frequency or perceived participation restrictions. In addition to these findings, the study highlights the variety of barriers that older adults need to overcome to be independent and able to participate in the community.
The following limitations and strengths should be kept in mind when interpreting/generalising the results of this study. The research area was limited to Southern Westfjords of Iceland; however, the results may be of value for other remote and arctic areas where the culture can be labelled as Western. The sample size was small, which reduced the possibility of further analysis of the data. Therefore, the results are for the total research area, and do not reflect potential differences in age distribution and service options among the small villages and the agricultural farming parts. However, the small sample size and the fact that the study was in a restricted area allowed visits to all participants, including face-to-face interviews and no need to exclude anyone due to hearing or vision impairments or difficulty in writing. This resulted in a participation rate of over 80% which is considered very good. Apart from one standardised test (MMSE), self-assessment questionnaires were used to collect data, which always includes a risk that participants will overestimate or underestimate their capacity and participation. However, questionnaires are a practical way to gather information about daily activities and participation, and the psychometric properties of the LLFDI in comparable populations [Citation19–21], support the validity of the data.
Results from both the activity and participation components of the LLFDI are displayed in scaled scores ranging from zero to 100. There are no truly normative/standard scores or criterion scores available for this Icelandic age group and therefore comparison of these results can only be done between demographic groups in our own study, and with results from other studies using the LLFDI. Our participants described Upper Extremity functioning, Basic Lower Extremity functioning, and Advanced Lower Extremity functioning that were all quite comparable to reports from older adults in a study among urban and rural Icelanders [Citation2]. However, compared to older community-dwelling people in Sweden [Citation19], our participants had higher total scores for activities (64.7 versus 58.0). This may be explained by differences in both demographics and health status as the Swedish group (54 women and 8 men aged 68–88 years) was attending balance training at a hospital, while the Icelandic group was a general older population sample. In our study the highest scores were for Upper Extremity functioning and the lowest for Advanced Lower Extremity functioning, which is consistent with other studies [Citation19,Citation22].
Generally, the results reflect how women experience more limitations in activities than men, both in Upper Extremity and Advanced Lower Extremity functioning. Similar gender differences have been observed in other studies in older Icelanders [Citation2,Citation23], and this difference in the physical capacity of older women and men is known worldwide. Explanations include biological differences, gender-based lifestyles and different gender roles in life [Citation22]. Our results also confirm research revealing that activity limitations increase with age and are most pronounced among people who have reached 75 years [Citation24].
Older residents of the Southern Westfjords had comparable scores on the participation frequency scale as older Icelanders in another study [Citation2], and in both cases the scores were relatively low. But the older adults did not report a matching participation restriction, which may indicate that their low frequency of participation was based on own choice/preferences rather than experienced internal or external barriers. These findings differ from studies that have shown that older people with impaired functioning tend to think that barriers in their environment are the main reason for low participation [Citation25,Citation26]. On other hand it aligns with the socioemotional selectivity theory [Citation27], when older people decide to narrow their goals and life tasks to fit the resources that are available to them. Research has shown such self-regulation strategies to be effective in optimising ageing, especially among people with multiple chronic conditions [Citation28]. The highest score on the LLFDI in our study was 89.6 for the management role and the lowest was 45.5 for the social role. This might indicate that despite geographical isolation, deteriorating health and physical limitations, older adults in Southern Westfjords generally consider themselves to be in control of their lives and that the low frequency of social participation is based on their own choice or limited social activities available. Importantly though, the older age group experienced more participation restrictions and participated less frequently than those who were younger. This may be because a large proportion of the younger age group had not retired, but was still employed and therefore more socially active than those who were older [Citation29]. Participation in the labour market, however, does not explain the more frequent overall participation of women than men, where the women scored higher for both personal role and social role. Interestingly, there was no age group difference in the frequency of personal role (self-care), which might be because this takes place primarily within the home [Citation30], and is essential for people who live independently in the community.
A report on health in the OECD countries, shows that although Iceland is still a relatively “young nation”, Icelanders have a very high life expectancy, both at birth and after 65. Furthermore, healthy life expectancy at the age of 65 in Iceland was the highest of all the European countries in 2013 [Citation31]. The healthy life expectancy of 15 years at the age of 65 supports that when people reach 80 they may expect to experience declining health and functioning, which influences their life roles. In the same OECD report, a projection predicts that by the year 2050, 8% of the Icelandic nation will be 80 years and older. An expanding number of older adults increases the need to study the lives of this population group to find ways to promote health and functioning and organise future welfare services. The aim of such service should be to support longer life with optimal activities and participation. In this context, preventive efforts and health promotion among older people become more important with each year that goes by [Citation31]. Thus, there is a need for increased home services that extend to people in sparsely populated and remote areas, and these services must be based on factual knowledge and research. The current study is one step in this process and its main results have already been introduced to representatives of the Southern Westfjords community.
Geolocation information
The Southern Westfjords of Iceland is a sparsely populated area which includes small fishing villages and rural agricultural area. This area of Iceland is located between 65° and 66° North.
Acknowledgments
The authors wish to thank all participants for contributing their time and effort, and the National Land Survey of Iceland, which prepared to present the research area.
Disclosure statement
The authors report no conflict of interest to declare.
Additional information
Funding
References
- Jorgensen TSH, Fors S, Nilsson CJ, et al. Ageing populations in the Nordic countries: mortality and longevity from 1990 to 2014. Scand J Public Health. 2019;47:611–9.
- Arnadottir SA, Gunnarsdottir ED, Stenlund H, et al. Participation frequency and perceived participation restrictions at older age: applying the international classification of functioning, disability and health (ICF) framework. Disabil Rehabil. 2011;33:2208–2216.
- Goodman RA, Ling SM, Briss PA, et al. Multimorbidity patterns in the USA: implications for research and clinical practice. J Gerontol A Biol Sci Med Sci. 2016;71:215–220.
- Nordic Burden of Disease Collaborators. Life expectancy and disease burden in the Nordic countries: results from the global burden of diseases, injuries, and risk factors study 2017. Lancet Public Health. 2019;4:e658–e69.
- Christensen K, Doblhammer G, Rau R, et al. Ageing populations: the challenges ahead. Lancet. 2009;374:1196–1208.
- Statistics Iceland. Population - Inhabitants. Databases [cited 2020 Nov 11]. Available from: https://www.statice.is/
- Ministry of Welfare Iceland. Act on the Affairs of the Elderly, No. 125/1999.
- Ministry of Welfare Iceland. The municipalities’ social services Act, No. 40/1999.
- World Health Organization [WHO]. International classification of functioning, disability, and health (ICF). Geneva: World Health Organization; 2001.
- Jette AM, Latham NK. Disability research: progress made, opportunities for even greater gains. Phys Ther. 2011;91:1708–1711.
- Faul F, Erdfelder E, Lang AG, et al. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191.
- Jette AM, Haley SM, Coster WJ, et al. Late life function and disability instrument: I. Development and evaluation of the disability component. J Gerontol A Biol Sci Med Sci. 2002;57:M209–16.
- Haley SM, Jette AM, Coster WJ, et al. Late life function and disability instrument: II. Development and evaluation of the function component. J Gerontol A Biol Sci Med Sci. 2002;57:M217–22.
- Jette AM, Haley SM, Kooyoomjian JT. Late life FDI manual. Boston: Boston University; 2002.
- Folstein MF. Folstein SE and McHugh PR. “Mini Mental State”. A practical guide for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–198.
- Verbrugge LM, Jette AM. The disablement process. Soc Sci Med. 1994;38:1–14.
- Jette AM, Haley SM and Kooyoomjian JT. Are the ICF activity and participation dimensions distinct? J Rehabil Med. 2003;35:145–149.
- Arnadottir SA. Physical activity, participation and self-rated health among older community-dwelling Icelanders: a population-based study [PhD thesis]. Umeå University, Sweden; 2010.
- Roaldsen KS, Halvarsson A, Sarlija B, et al. Self-reported function and disability in late life - cross-cultural adaptation and validation of the Swedish version of the Late-Life Function And Disability Instrument. Disabil Rehabil. 2014;36:813–817.
- Beauchamp MK, Schmidt CT, Pedersen MM, et al. Psychometric properties of the Late-Life Function and Disability Instrument: a systematic review. BMC Geriatr. 2014;14:12.
- Beauchamp MK, Jette AM, Ward RE, et al. Predictive validity and responsiveness of patient-reported and performance-based measures of function in the Boston RISE study. J Gerontol A Biol Sci Med Sci. 2015;70:616–622.
- Zunzunegui MV, Alvarado BE, Guerra R, et al. The mobility gap between older men and women: the embodiment of gender. Arch Gerontol Geriatr. 2015;61:140–148.
- Gudmunsdottir H, Bjornsdottir K, Olafsson RF. Likamleg faerni og studningur fra formlegum og oformlegum studningsadilum hja 90 ara og eldri a Íslandi. [Physical functioning among 90+ year-old Icelanders, and support from formal and informal caregivers. Oldrun [Ageing]. 2004;22:10–15.
- Jindai K, Nielson C, Vorderstrasse B, et al. Multimorbidity and functional limitations among adults 65 or older, NHANES 2005-2012. Prev Chronic Dis. 2016;13:E151.
- Keysor JJ, Jette AM, LaValley MP, et al. Community environmental factors are associated with disability in older adults with functional limitations: the MOST study. J Gerontol A Biol Sci Med Sci. 2010;65:393–399.
- White DK, Keysor JJ, Lavalley MP, et al. Clinically important improvement in function is common in people with or at high risk of knee OA: the MOST study. J Rheumatol. 2010;37:1244–1251.
- Carstensen LL, Isaacowitz DM and Charles ST. Taking time seriously. A theory of socioemotional selectivity. Am Psychol. 1999;54:165–181.
- Zhang W, Radhakrishnan K. Evidence on selection, optimization, and compensation strategies to optimize aging with multiple chronic conditions: a literature review. Geriatr Nurs. 2018;39:534–542.
- Hsu HC. Does social participation by the elderly reduce mortality and cognitive impairment? Aging Ment Health. 2007;11:699–707.
- Haak M, Ivanoff SD, Fänge A, et al. Home as the locus and origin for participation: experiences among very old Swedish people. OTJR. 2007;27:95–103.
- Organisation for Economic Co-operation and Development [OECD]. Health at a glance 2015: OECD indicators. Paris: OECD Publishing; 2015.