
ABSTRACT
The second year of the COVID-19 pandemic in the Arctic was dominated by the Delta wave that primarily lasted between July and December 2021 with varied epidemiological outcomes. An analysis of the Arctic’s subnational COVID-19 data revealed a massive increase in cases and deaths across all its jurisdictions but at varying time periods. However, the case fatality ratio (CFR) in most Arctic regions did not rise dramatically and was below national levels (except in Northern Russia). Based on the spatiotemporal patterns of the Delta outbreak, we identified four types of pandemic waves across Arctic regions: Tsunami (Greenland, Iceland, Faroe Islands, Northern Norway, Northern Finland, and Northern Canada), Superstorm (Alaska), Tidal wave (Northern Russia), and Protracted Wave (Northern Sweden). These regionally varied COVID-19 epidemiological dynamics are likely attributable to the inconsistency in implementing public health prevention measures, geographical isolation, and varying vaccination rates. A lesson remote and Indigenous communities can learn from the Arctic is that the three-prong (delay-prepare-respond) approach could be a tool in curtailing the impact of COVID-19 or future pandemics. This article is motivated by previous research that examined the first and second waves of the pandemic in the Arctic. Data are available at https://arctic.uni.edu/arctic-covid-19.
Introduction
The localised outbreak of SARS-CoV-2, popularly known as COVID-19, was first reported in Wuhan, China, and then advanced rapidly as a global pandemic spreading unevenly over time and space [Citation1–5]. Since the beginning of the pandemic, the original COVID-19 virus has mutated into many variants. The first well-known variant, Alpha (B1.1.7) appeared in the U.K. in November 2020, then spread around the world, in part, because it was 30–50% more contagious than the original virus, and by April 2021 had become the dominant variant in the U.S [Citation6]. The Delta variant (officially B.1.617.2) was the most contagious among earlier strains including Alpha [Citation7,Citation8]. Given the high transmissibility due to higher viral load expulsion [Citation9,Citation10], the World Health Organization (WHO) labeled Delta as a variant of concern in May 2021 [Citation11]. The COVID-19 cases due to the Delta surged globally in 2021 to a record high, accounting for 99.8% of total cases reported between October and November [Citation11].
The Delta is not only highly transmissible but also has caused more severe disease compared to other variants in the unvaccinated population. The variant led to an overwhelming increase in hospitalisations and therefore significantly increased people’s risk of death [Citation12–14]. In other words, Delta was optimised for higher infectivity and lethality [just as Yersinia pestis and its pla gene did in the primary wave of the Medieval Black Death; Bossak & Welford, [Citation15] as it outcompeted other COVID-19 variants following its mutation in September or October 2020 [Citation16]. Besides, the Delta’s contagious and severe nature, disparities in the distribution of vaccines, vaccine hesitancy, unequal access to health care, and inconsistency in the implementation of public health and social measure across the globe, including the Arctic, have contributed to the exponential spread of the variant leading to greater loss of life and once again causing social and economy dysfunction [Citation17,Citation18].
Delta was first discovered in India in October 2020 [Citation19] and swept rapidly across the world. Delta was first detected in Russia, the UK, and the US in March 2021 and surfaced in Canada in early April 2021 [Citation20–22]. In Arctic locations like Alaska, Iceland, Greenland, and the Faroe Islands, the first cases of the Delta were reported in the early summer of 2021 [Citation21]. In these Arctic states, Delta arrived because of the loosening of COVID-19 restrictions that allow movement of the labour force, tourists, and other travellers in and out of the region [Citation23,Citation24]. To date, this variant has been identified in 188 countries and is among the most prevalent variants [Citation25].
Smallpox, cholera, the 1918 pandemic influenza, tuberculosis, and the 2009 H1N1 pandemic have all hit the Arctic, particularly remote communities and the Indigenous Peoples [Citation26,Citation27], and had long-term impacts on Arctic communities (Napoleon, 1991). The 1918 pandemic influenza outbreak killed 90% of the total population in Brevig Mission, Alaska, and more than 20% of the total Indigenous population of Labrador Canada [Citation28,Citation29]. Among Alaska’s Indigenous Peoples, the Inupiaq and the Bristol Bay Yupik had the highest mortality around 30% [Citation28,Citation29]. Indigenous populations around the world have experienced COVID-19 mortality at disproportionately higher rates than non-indigenous populations. In Alaska, American Indian and Alaska Native persons are 2.9 times more likely to die of COVID-19 than White persons [Citation30]. Some of the contributing factors that make Arctic populations, including the Indigenous Peoples, vulnerable to COVID-19 include remoteness, underdeveloped health care systems, and infrastructure, a young, but ageing population, political marginalisation, higher prevalence of underlying medical conditions (such as hypertension, diabetes, heart disease, tuberculosis, hepatitis, obesity), poverty, food insecurity, and low living standards characterised by overcrowding, water contamination, and poor sanitation, among others Huot et al. [Citation31,Citation26,Citation32].
The Arctic occupies a special place in COVID-19 research given its remoteness, difficult socioeconomic conditions, population composition, and prevalent health characteristics [Citation26,Citation33]. Pre-existing vulnerabilities combined with the tragic history of pandemic deaths and neglect from respective governments have encouraged the Arctic Indigenous communities to take precautionary measures [Citation34,Citation35]. At the same time, the Arctic benefits from pandemic resilience capacities related to Indigenous knowledge and practices. Many Arctic communities have relied on a unique combination of Indigenous knowledge, leadership, self-determination, and rapid vaccination to curtail the impact of the pandemic [Citation33]. Proactive community leadership anchored in the principles of self-determination and Indigenous knowledge has made some Indigenous communities remarkably resilient to COVID-19 [Citation36].
Previous studies have demonstrated the distinct challenges the Arctic faces in relation to the COVID-19 pandemic and potentially similar public health or infectious disease emergencies. Markova et al. Citation37, Lemieux et al. Citation38, Simonen et al. Citation39, Cook & Johannsdottir [Citation40], Men & Tarasuk Citation41, and Golubeva et al Citation42,all have pointed out that the COVID-19 pandemic has exacerbated the existing socioeconomic vulnerability, food insecurity and health outcomes of the Arctic residents. The pandemic has pushed the people of Sakha (Northeastern Siberia, Russia) into poverty as people have lost their jobs and lacked stable earnings (overdue wage arrears) [Citation37,Citation43]. The pandemic has exacerbated the skilled workforce shortage in Northern Finland, Sweden, and Norway, especially in the five Arctic communities (i.e. Oulu, Rovaniemi, Lulea, Umea, and Tromso) [Citation39,Citation44,Citation45]. Cook & Johannsdottir [Citation40] developed a multiscale framework to assess the impact of COVID-19 on Iceland and Greenland across seven categories [economic, environmental, social-cultural, business, ethical, health, science/education) and found that the pandemic has presented risks in both countries across all categories. Golubeva et al. Citation42,uncovered that self-isolation measures led to deterioration in the mental and physical health of older people as well as of caregivers living in the Russian Arctic.
Within the scientific community, there has also been a focus on the resiliency of Indigenous people that could alleviate the negative impact of a disease outbreak. The Arctic Council Citation46,and Petrov et al. Petrov et al. [Citation33,Citation47] acknowledged the importance of self-sufficiency (e.g. livelihood based on subsistence activities] and Indigenous knowledge in contending with the challenges created by COVID-19. Bogdanov et al [Citation48], Michele et al. [Citation49] and [Citation50] ,emphasised the sovereignty of the Indigenous Peoples, tribes, and local government units as an important tool to fight against the pandemic. Various scholars such as Bogdanova et a. [Citation51], Palomino et al. [Citation52], Petrov et al. Petrov et al. [Citation53], and Retter [Citation54], have also applauded positive measures taken by individuals, (such as online fish skin tanning workshops, organisation of the Arctic Indigenous Artists Virtual Network – AIVAN), and non-governmental organisations (pandemic safety application and game by Inuit Tapiriit Kanatami) to cope with the pandemic.
The above-mentioned literature, by highlighting challenges, assets, and experiences of the Arctic, could serve as powerful tools in decision-making amid the pandemic. Similarly, data on COVID-19 by demographic and socioeconomic characteristics at a granular level are essential for allocating resources and services, and for launching a variety of health campaigns to reach vulnerable populations or populations with the greatest needs. Yet only a few studies have thoroughly examined COVID-19 data at the Arctic’s regional level. Petrov et al [Citation33,Citation55] collected and analysed Arctic regional (subnational) level data at multiple points in time. These analyses, in turn, motivate the present study, which likewise seeks to examine spatiotemporal dynamics of the COVID-19 pandemic from January 2021 to January 2022, particularly with respect to the Delta wave, and to develop a typology of the Arctic regions based on the spatiotemporal patterns of the Delta surge. Further, we extend our analysis to explore the geographies and timing of vaccination that could impact COVID-19 dynamics.
The remainder of this paper is organised as follows. First, we present a data and methods section that describes spatial coverage, data sources, and variables used in our study followed by our findings and then we discuss the typology of the COVID-19 regional dynamics during the Delta wave.
Data and methods
Spatial coverage
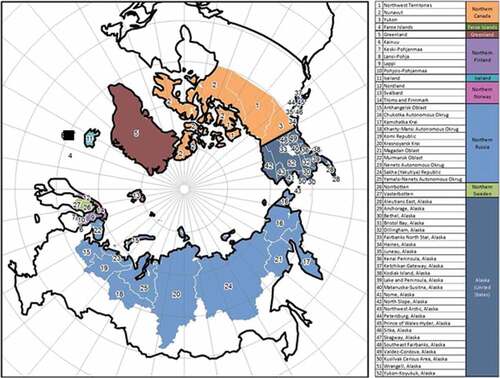
This analysis utilised spatiotemporal data on COVID-19 cases and fatalities collected at the subnational (regional, county) level for 52 regions in eight countries (): Canada, Kingdom of Denmark (Greenland and Faroe Islands), Finland, Iceland, Norway, Sweden, Russia, and the USA. This closely follows the Arctic boundaries established by the Arctic Human Development Report (Einarsson et al. [Citation56] and revised by Jungsberg et al. [Citation57]).
Figure 1. Study area.
Data
We developed and utilised a system that has been automatically collecting daily case and death information from a variety of sources including the Center for Systems Science and Engineering (CSSE) at John Hopkins University for Canada, Greenland, Faroe Islands, Iceland, and the USA (https://coronavirus.jhu.edu/map.html), the Public Health Agency of Sweden (https://www.folkhalsomyndigheten.se/), the National Institute for Health and Welfare of Finland (https://thl.fi), the Government of the Russian Federation (https://стопкоронавирус.рф), and Verdens Gang (Norway) – https://vg.no. The data is extracted at 17:00 GMT each day, stored, and published daily on the Arctic COVID-19 dashboard (https://arctic.uni.edu/arctic-covid-19). The temporal coverage of this database extends from 21 February 2020 (the first documented case in the Arctic) to the present. However, for the purposes of this study, we focused on the COVID-19 dynamics in 2021, in particular Fall 2021, (to capture the Delta “wave” in the Arctic), ending the examined period on 1 January 2022. We used the ArcticVAX tracker (ArcticVAX [Citation58]) to obtain information on vaccination trends for the same period. The definitions of “fully vaccinated” individuals differ by reporting country. However, in most jurisdictions, “fully vaccinated” refers to individuals vaccinated with at least two doses of an mRNA vaccine (e.g. Moderna and Pfizer) or one dose of the Johnson & Johnson vaccine or their equivalents required for full protection [Citation59]. Due to the ineffectiveness of the vaccines against the new strains (e.g. the Delta) of COVID-19 [Citation60], more doses are now required to be considered “fully vaccinated” in many jurisdictions, but these recent recommendations are not reflected in the data used.
Variables and definitions
We analysed key variables used to describe epidemics Dicker et al. [Citation61]. Confirmed cases are individuals detected with SARS-CoV-2 nucleic acid or antigen in their clinical specimen [Citation62] (i.e. symptomatic or asymptomatic persons who tested positive for SARS-COV-2 virus). Daily increase is the number of cases confirmed within 24 hours after the previous reporting. Incidence rate represents a cumulative number of confirmed cases per 100,000 residents in a given period of time. Confirmed deaths are the number of deaths resulting from a clinical illness due to COVID-19 infection [Citation62]. Mortality rate is the number of confirmed deaths attributable to COVID-19 infection per 100,000 residents in a given period of time. Case Fatality Ratio, or CFR, is the total number of deaths divided by the total number of confirmed cases at a given point in time. Given that data are from diverse sources and multiple jurisdictions, the specific definitions used by the reporting agencies may inevitably vary and have to be interpreted with some caution.
Results
In the context of the COVID-19 pandemic, epidemiologists use the term “wave” to define a surge in incidents of the infection followed by a substantial decrease sustaining over a certain period [Citation63]. As per Petrov et al. [Citation33,Citation55], the first case of COVID-19 in the Arctic was reported in February 2020 and spread through its regions in several distinct waves. Although there was some regional variation in the spatiotemporal patterns of the pandemic and numbering of the waves, based on cumulative and daily dynamics of the confirmed cases, the first Arctic-wide wave emerged between May and August of 2020 followed by the second wave starting in mid-September 2020. The second wave peaked in the late fall of 2020 and subsided by the early spring of 2021. Each wave’s period (i.e. start and end), magnitude (i.e. contagious), and intensity (i.e. severity) varied considerably among the Arctic regions [Citation33].
illustrates a cumulative number of confirmed COVID-19 cases in the Arctic from the beginning of the pandemic until 1 January 2022. In 2021 specifically, between January and mid-June, the number of new cases was trending down. However, new cases gradually rose after mid-June, especially in October-December, indicative of the beginning of the third, or “Delta wave”, in the Arctic, i.e. when the Delta variant has been dominant around the globe [Citation11,Citation64]. The rate of increase in new cases was high and relatively constant throughout the second half of 2021.
Figure 2. Cumulative Confirmed COVID-19 Cases in the Arctic (20 February 2020–1 January 2022).
Cumulative COVID-19 cases and deaths per 100,000 for each region of the Arctic, as shown in , signalled that the Delta wave was far more severe than the first and second waves of the pandemic. In fact, this wave signified the full arrival of the COVID-19 pandemic to all Arctic regions and the vast majority of communities. More than 700,000 new cases and over 17,000 new deaths were reported in the Arctic during 2021. These estimates correspond to an increase of 205.8% in cases and 334.8% in deaths compared to the previous year. By 1 January 2022, the Arctic reported 1,066,375 confirmed cases and 22,992 deaths. The majority of these cases and deaths occurred after May 2021.
Figure 3. Cumulative cases per 100,00 (top); Cumulative deaths (bottom) per 100,000.
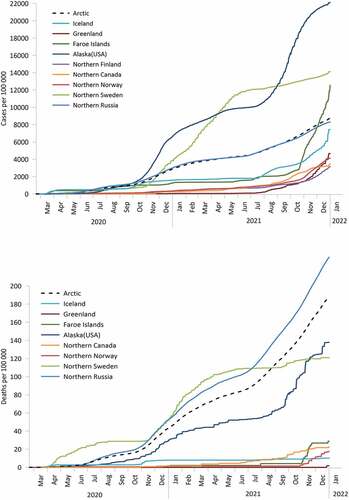
However, the dynamics of the incidence of COVID-19 infection were not uniform across Arctic regions (). Northern Russia, given its large Arctic population, generally defined the overall Arctic trend. After reaching a peak in mid-December 2020 (“second wave” [Citation33]), new COVID-19 cases in Northern Russia decreased in the early months of 2021, but by August, the Delta wave began with a gradual increase in cases and deaths per 100,000. The rate of new confirmed cases continued to rise until the end of the year. In Alaska, after a similar decline in cases early in 2021, confirmed COVID-19 incidents per 100,000 precipitously increased, reaching the highest levels in the Arctic. In fact, they were more than twice as high as the Arctic as a whole. The growth in new cases slowed in December.
Northern Sweden experienced rapid growth in new COVID-19 cases at the beginning of 2021, followed by a decreasing trend in the middle of the year and a slight upward trend at the end of the year 2021. Both cases and deaths per 100,000 in Sweden were exceptionally high during all of 2021, lagging only behind Alaska. At the same time, in the Fall of 2021, Northern Sweden saw a modest increase in new confirmed cases and deaths, seemingly avoiding a distinct Delta wave.
Greenland and Iceland reported very few new COVID-19 cases, just under 2,000 cumulative cases per 100,000, from Jan 2021 till mid-July 2021. Iceland went through a short period of growth and decline in new cases between mid-July and October followed by a rapid increase in the cases from November onward. Meanwhile Greenland, after mid-July, experienced an upward trend in new cases at an exponential rate. The Faroe Islands also saw a dramatic rise in new cases during the Fall of 2021. Even though Greenland and Iceland reported an increase in new cases, these regions had very few deaths, whereas the Faroe Islands observed an increase in the number of deaths in November. After the end of November, the Faroe Islands reported very few new fatalities.
Following a gradual increase beginning in Jan 2021, new monthly cases quickly rose in Northern Norway and Northern Finland from November 2021 to Jan 2022. The number of deaths also started to climb in Northern Norway after November 2021. New cases in Northern Canada gradually declined during the fall of 2021 after a slow steady increase in the beginning and middle of the year. A slight upward trend in new monthly deaths was observed by Northern Canada after mid-summer, with the cumulative number of deaths just under 20 per 100,000.
During the Delta wave, there was a marked decline in the Case Fatality Ratio (CFR), as shown in , in each region (except in Northern Russia) compared to the previous COVID-19 waves. After the summer of 2021, just under one percent of the diagnosed individuals in most Arctic regions died from COVID-19. In contrast, by the end of 2021, Northern Russia’s CFR had exceeded 2%. The Delta variant is highly contagious, as indicated by quickly rising cumulative confirmed cases, but seems less severe in terms of CFR in the Arctic compared to the previous COVID-19 waves, nonetheless. Low CFR can possibly be attributed to mass vaccination campaigns with continued containment measures in the Arctic.
Figure 4. Case-Fatality Ratio (CFR).
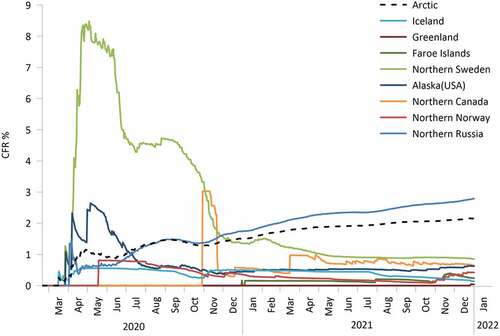
Previous studies indicated that during the earlier COVID-19 waves northern regions were exhibiting lower rates of COVID-19 cases compared to their respective country as a whole [Citation33,Citation55]. In contrast to the first and second waves, after the Delta wave, Arctic regions seemed to experience new confirmed COVID-19 case rates similar to their mainland counterparts. Alaska, Northern Sweden, and Northern Russia had cumulative cases per 100,000 slightly higher, while the Faroe Islands, Northern Finland, and Northern Canada had lower (but the difference diminished compared to the earlier stages) cumulative cases rates than their overall nations. This pattern likely indicates that the northern regions have been “catching up” with the rest of the respective countries as the pandemic arrived in full force in more remote territories. However, the mortality rate and the cumulative CFR for Arctic communities were significantly lower compared to their mainland except for Northern Russia. This is an important discrepancy that may be attributed to vaccination rates and better preparedness of healthcare systems for the third wave later in the pandemic. The notable exception was Russia whereby 1 January 2022, northern regions had reported 231.7 deaths per 100,000, a number far above any other Arctic region and Russia as a whole.
Regional typology of the COVID-19 pandemic dynamics
The notion of “waves” has been often used to provide a useful overarching description for pandemic dynamics [Citation63]. Previous work identified several regional typologies of spatiotemporal trends in the early course of COVID-19 pandemic in the Arctic [Citation33,Citation55]. At that time, four distinct types of dynamics were observed: shockwaves (early onset of the pandemic in the spring of 2020 with a rapid spike in both cases and deaths), protracted waves (protracted “first” and “second” waves with an unsteady, but continued growth in cases and deaths), tsunami wave (low initial COVID-19 presence with a subsequent dramatic peak of cases), tidal waves (a continuously high level of new cases with some fluctuations) and isolated splashes (no early waves, isolated small cases spikes – regional largely unaffected by the pandemic). Some of the early differences in regional patterns are credited to the divergent pandemic prevention policies and vaccine rollouts. For example, Sweden (protracted wave) had taken a herd-immunity approach early in the pandemic by emphasising personal responsibility as opposed to strict isolation measures implemented by its Nordic neighbours Kamerlin & Kasson, [Citation65]020; Yan et al. [Citation66]. Russia (tidal wave) in 2020 focused its efforts on the development of the vaccine rather than prevention measures enforcement (Jones & Roy, [Citation67]).
During the third, Delta wave, regional differences in the temporal dynamics of the COVID-19 pandemic were also evident (). However, the universal pattern was a dramatic increase in both cases and deaths by the end of 2021. If until mid-2021 some Arctic regions, such as Greenland, the Faroe Islands, Northern Canada, Norway, and Finland, nearly avoided COVID-19 outbreaks by applying strict anti-epidemic measures, all of them experienced the rapid arrival of the pandemic later in the year. As was pointed out in the previous studies, the delay of the pandemic onset in some remote jurisdictions could only provide temporary relief, but not stop the eventual start of the pandemic [Citation33]. In the Fall of 2021, a mass growth in cases even in the most isolated regions indicated that the COVID-19 pandemic in the Arctic had advanced to the next, very dangerous stage: limited healthcare infrastructure and resources in northern communities faced formidable challenges on how to provide an adequate response to the spreading disease. At the same time, less substantial growth in fatalities, and relatively low CFR () gave evidence of a less dramatic impact of the pandemic than expected, most likely due to better preparedness and successful vaccination campaigns in early 2021 ().
Figure 5. Daily confirmed COVID-19 cases and deaths (7-day moving average).
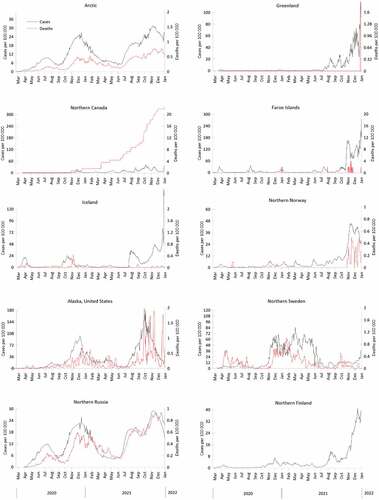
Figure 6. Percent of fully vaccinated individuals in total population.
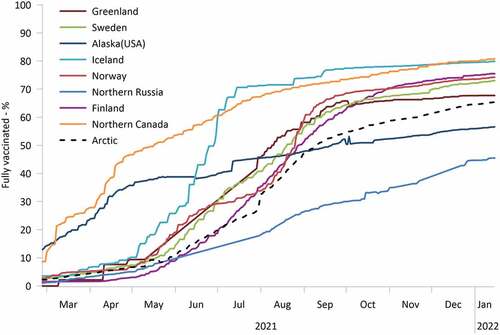
Table 1. COVID-19 Pandemic in the Arctic regions (21 February 2020–1 January 2022).
The “wave” patterns persisted, although they changed their geographies and new types of dynamics emerged, while others disappeared.
Tsunami wave
Many Arctic regions exhibited tsunami-like COVID-19 dynamics with abrupt and dramatic spikes in daily cases (and, in some areas, deaths) that started in late summer or early fall of 2021 and culminated in October-November of 2021 (). This was also reflected in a sharp rise in cumulative cases per 100,000 (). This group includes Greenland, Iceland, the Faroe Islands, Northern Norway, Northern Finland, and Northern Canada. Many of these regions were relatively unaffected by the pandemic before and therefore had to deal with the first major wave of the disease. It is notable, however, that the mortality dynamics did not necessarily follow the cases. We can distinguish between the two types of mortality dynamics: in some regions, the rise in caseloads corresponded with a considerable increase of fatalities in a tsunami-like fashion (e.g. Northern Canada, Northern Norway, and the Faroe Islands), while in others (e.g. Iceland), daily deaths had only isolated splashes following the “tsunami” of cases.
Superstorm
The COVID-19 pandemic in Alaska was generally similar to a tsunami pattern, but the height of the confirmed cases wave separates it from other regions (). The pandemic superstorm commenced in late July – early August 2021 and peaked in September 2021, but new cases remained high until November 2021. By the summer of 2021, Alaska had ended most of its statewide anti-COVID restrictions and mandates (e.g. the State of Alaska COVID-19 Disaster Declaration was discontinued on 30 April 2021) and welcomed tourists. During the Delta wave, Alaska quickly moved to become a hot spot of the pandemic with cases exceeding 22,000 per 100,000 by the end of 2021. Mortality also showed multiple dramatic spikes that followed massive increases in detected cases.
Tidal wave
As in the past, continuously high, albeit fluctuating, daily cases and deaths were observed in Northern Russia. In the summer of 2021, Russia experienced a decline in recorded new cases, but this pattern was reversed in July 2021 to culminate in November 2021 with a pronounced Delta wave. This phase of the pandemic was more severe in the northern regions of Russia compared to the rest of the country (), likely reflecting the low level of preparedness, inconsistent quarantine measures, curtailed healthcare capacities, and limited availability and/or uptake of vaccines in remote areas.
Table 2. Regional Typology of COVID-19 Pandemic Dynamics in the Arctic: 2021 Summary Characteristics.
Protracted wave
Sweden previously experienced protracted waves of the COVID-19 pandemic likely associated with its light-touch approach to the pandemic, resisting lockdowns, underemphasising social distancing and mask-wearing, and believing in building herd immunity. This resulted in a steady growth of cases and deaths and a very high CFR in 2020. When in January 2021 Sweden tightened the rules [Citation68,Citation69], the epidemiological characteristics of Northern Sweden improved () the daily number of cases dropped and the very protracted second wave of the pandemic concluded by July 2021. After implementing these measures and rolling out vaccines, the subsequent Delta wave (Fall of 2021), was very minor compared to the second wave, although it was again protracted spanning between August and December.
Spatiotemporal trends of COVID-19 vaccination in the Arctic
COVID-19 vaccines were first administered in the Arctic in December 2020. Alaskans and Arctic Canadians were among the first individuals across the Arctic and the world to receive doses of COVID-19 vaccines. In January 2021, Alaska led the nation in vaccination rates [Citation70], and by May over 60% of adults (i.e.16 years old and older) living in Aleutians East Borough, Skagway Municipality, Sitka City and Borough, and Yukon-Koyukuk Census Area had received at least one dose (ArcticVAX, 2022). This was a remarkable and unique experience of successful early vaccination rollout administered by the Alaska Native Tribal Health Consortium, an Indigenous-controlled health organisation, in coordination with other agencies and tribes [Citation71]. The campaign was aimed at attaining high vaccination levels in remote predominantly Indigenous communities and was largely successful. A similar early vaccination campaign was organised in northern Canada [Citation72]. Both are clearly illustrated by the vaccination dynamics shown in . However, Alaska vaccination uptake decelerated considerably compared to Northern Canada largely due to vaccine hesitancy in non-Indigenous populations and some Alaska Native groups. Still, Northern Canada and Alaska, arguably some of the most remote parts of the Arctic, led the Arctic regions in terms of vaccination rates until May, when other jurisdictions, most notably the Nordic countries, started to increase their vaccination prevalence. The rates varied depending on vaccination policies, mandates, and availability in each jurisdiction. On the other hand, Russia had reported relatively low vaccination rates, and that rate grew slowly throughout 2021.
Discussion
The term “wave” has been used to describe the various epidemiological phases of COVID-19 variants that have impacted global communities. The results of this analysis indicate that various regions of the Arctic experienced the Delta wave very differently and exhibited four types of COVID-19 spatiotemporal dynamics. Arctic communities, as well as the public health emergencies that affect them, cannot be stereotyped or lumped into one definition. Each Arctic region was impacted by the Delta variant, at different levels of intensity and at various time periods from each other.
This study clearly demonstrated that Arctic regions are diverse, and they vary in how a global pandemic may be experienced. Pre-existing environmental, sociocultural, political, organisational, and geographic conditions can fundamentally impact the timing of when infectious disease outbreaks may occur, the level to which various subpopulations in a region may be affected, and ultimately could help explain the level to which morbidity and mortality rates can be impacted. These differences in experiences can be particularly important to understand as a virus may mutate and pose new threats to communities, even though it is still part of one pandemic.
It is also evident that COVID-19 prevention and mitigation policies played a considerable role in determining the spatiotemporal dynamics of the pandemic. Regions with stronger mandates and policies and with more effective enforcement fared generally better than others. For example, Greenland implemented some of the strictest measures in the Arctic, such as a temporary ban on entering the island, suspension of internal travel, lockdowns, and quarantines in pandemic-affected areas. As a result, it had a very low per capita caseload and mortality. Jurisdictions that were quick to cancel the preventive regulations, such as Alaska, had a very pronounced and steep Delta wave. Another important factor was the rollout and adoption of vaccines, especially successful in Northern Canada, Alaska, and Nordic countries.
Relying on an Indigenous-controlled or focused healthcare system appeared to increase the effectiveness of vaccination campaigns in Indigenous communities [as was shown elsewhere as well: Foxworth et al, Citation73, Haroz et al., Citation74]. Relatively low vaccination rates in Northern Russia along with the low level of preparedness, inconsistent public health prevention measures, curtailed healthcare capacities, and other factors corresponded to high mortality and CFR. Despite a history of coerced medical experimentation and abuse, the Arctic Indigenous communities were among the first to implement mass vaccination as early as December 2020 [Citation71,Citation72]. In Alaska, initial higher vaccination rates can be largely attributed to strong vaccine-distribution networks, tribal cultural values that emphasise protection and honouring of elders, culturally tailored messaging strategies to overcome vaccine hesitancy, and tribal sovereignty that allowed the tribal groups to establish their campaign and priorities [Citation73]. Prioritising vaccination access to certain community members such as elders, knowledge keepers, and health providers, and the door-to-door vaccine outreach to medically fragile community members had boosted the general confidence of Alaskans in the vaccine [Citation73,Citation74].
The aggregate data analysed in this paper does not reveal the differences in COVID-19 impacts on Arctic Indigenous populations compared to non-Indigenous residents. Indigenous populations generally were disproportionately affected by the pandemic around the world [Citation75,Citation76]. A recent retrospective analysis of these discrepancies in Alaska provides additional confirmation of the existing gap: the ratios for case, hospitalisation, and mortality rates for Indigenous Alaskans compared with White persons in 2020 and 2021 were 2.2, 2.7, and 2.9 higher, respectively [Citation30]. The pandemic also disproportionately affected the elderly, a group that has a special role in Indigenous communities [Citation77,Citation78]. These and other inequities are important to examine further at regional and community levels. Another important dimension is the urban-rural divide. More urbanised areas generally had an earlier onset of the pandemic, but during the Delta wave rural, remote areas were more affected (in relative terms) experiencing very high per capita confirmed caseloads.
If early in the pandemic the Arctic benefited from the “blessing of remoteness” (i.e. a delayed start of the pandemic due to being away from large settlements and transportation hubs), in 2021 Arctic regions suffered from the “curse of remoteness” associated with their limited healthcare infrastructure and capacity [Citation33]. However, some communities were able to capitalise on the “blessing” to successfully fight the “curse”. In particular, observations of the Delta wave, alongside previous COVID-19 pandemic dynamics [Citation36,Citation47,Citation55], indicate that Arctic regions, especially remote communities, could have benefited from a three-pronged pandemic response. These three elements include (1) delaying the arrival of the pandemic by using widespread and strict prevention measures, information campaigns, as well as Indigenous knowledge and Indigenous control of their communities; (2) using the time before the arrival of the pandemic to prepare for its eventual onset (e.g. strengthening healthcare system capacities and conducting mass vaccinations on-site), and (3) responding to the pandemic using all available means of the healthcare system, but also engaging Indigenous knowledge and self-determination over healthcare. For example, Indigenous communities in the US High North often benefited greatly from the Alaskan Community Health Aide Program and its strong partnerships with regional hospitals. COVID nursing teams were dispatched to remote villages to conduct testing and vaccinations on-site, with a special focus on providing culturally appropriate care to Elders. Although no single region specifically followed all the steps, Greenland and, possibly, Northern Canada implemented similar approaches in some areas. The Nordic countries also likely benefited from strong, well-organised national health care systems committed to mitigating the spread of the virus.
Examples of policies and actions addressing the epidemic with limited resources that fall within this framework may vary. For instance, with inadequate medical resources and infrastructure, the Delta outbreak in multiple places at the same time in Greenland was predicted to have a catastrophic loss of life. Thus, Greenland focused first on fully vaccinating people in the largest city of Nuuk and towns, assuming an outbreak would be more likely to occur in a town before it spread to a hamlet and whereas vaccination campaigns for hamlets required a large amount of resources, time and effort [Citation23]. In another example, remoteness initially delayed the arrival of COVID-19 in the Baffin (Qikiqtaaluk) region of Nunavut in the Canadian Arctic. Massive awareness campaigns grounded in the local context and drawing upon the knowledge of Indigenous elders and knowledge keepers were launched under the leadership of the Qikiqtani Inuit Association (QIA) [Citation36,Citation79]. The lockdown implemented in Nunavut greatly decreased possible infections in late 2020 and the subsequent vaccination campaign commenced on 6 January 2021, likely prevented thousands of COVID-19 cases [Citation80].
Conclusions
The spatiotemporal dynamics of the COVID-19 pandemic in the Arctic in 2021 were dominated by the Delta wave that generally lasted between July and December 2021 with some variations among Arctic regions. The second year of the pandemic signified a massive increase in cases and deaths among all jurisdictions with COVID-19 finally arriving even in most remote Arctic communities. The onset of the Delta wave corresponded to the steepest growth in confirmed cases and mortality since the beginning of the pandemic in February of 2020. At the same time, the CFR in most Arctic regions did not rise as sharply and was largely below the national level (except for Russia). These dynamics, as well as their regional differences, are likely attributable to changes in the COVID-19 prevention and mitigation measures and varying degrees of vaccination rates. Some Arctic regions led the world in early vaccination efforts (Northern Canada and Alaska), while others lagged (Northern Russia). It also appears that having an Indigenous-controlled healthcare system was a positive factor in the successful vaccine rollout. At the same time, early reopening might have hampered the efforts to curtail the pandemic.
One of the potential lessons from the Arctic is that the three-prong delay-prepare-respond approach may work best in remote and largely Indigenous regions and communities. It entails delaying the onset of the pandemic, preparing and conducting mass vaccinations, and responding by bringing together medical science and Indigenous knowledge within an Indigenous-controlled healthcare system when the pandemic arrives. Indigenous, rural, and remote communities in other parts of the world have much to learn from the Arctic COVID-19 mitigation approach that capitalises on previous pandemic experiences, traditional knowledge, community leadership, self-determination, and public health interventions to deal with the pandemic [Citation47,Citation81]. The Arctic approach not only reduces fatalities but addresses challenges produced by COVID-19 while also offering an important lesson to cope with future pandemics which will likely be inevitable and more aggressive.
COVID-19, including the Delta variant, is only the latest novel virus to create concern for the public health and wellbeing of the world, including that of remote areas like the circumpolar region. The increasingly warming and rapidly changing global High North is no longer isolated, and its human geography is linked to the rest of the world through complex local, regional, national, and international relationships. Novel virus pandemics are expected to increase in frequency and intensity in future years due to climate change, increased globalisation, the need for in-migration of labour, greater human density in urban and littoral areas, and other factors. Public health officials, government leaders, Indigenous organisations, and policymakers must understand that infectious disease prevention and mitigation strategies for global pandemics must include not only transnational cooperation but also take into account local and regional variances in the geography of communities in order to effectively impact outcomes.
Limitations
COVID-19 data in the Arctic is prone to reporting, accuracy, and access issues [see Citation47,Citation55]. This study relied on publicly available datasets that used national/regional definitions and data handling practices. This likely leads to under- or misreporting, inconsistencies and errors. To partially alleviate this, we examined aggregates and longer-term trends rather than individually reported numbers or short-term pandemic events.
Acknowledgments
The authors are grateful to Jonathan Voss for his help with this work. The research is supported by NSF 2034886.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Ciotti M, Ciccozzi M, Terrinoni A, et al. The COVID-19 pandemic. Crit Rev Clin Lab Sci. 2020;57(6):365–15.
- Connolly M, Jacobs B, Notzon FC. COVID-19 among American Indians and Alaska Natives in the USA: an early look. Stat J IAOS. 2021;37(1):25–36.
- Kapitsinis N. The underlying factors of the COVID‐19 spatially uneven spread. Initial evidence from regions in nine EU countries. Reg Sci Policy Pract. 2020;12(6):1027–1045.
- MacIntyre CR. Global spread of COVID-19 and pandemic potential. Global Biosecur. 2020;1(3). DOI:10.31646/gbio.55
- Rose-Redwood R, Kitchin R, Apostolopoulou E, et al. Geographies of the COVID-19 pandemic. Dialogues in Human Geograpghy. 2020;10(2):97–106.
- Paul P, France AM, Aoki Y, et al. Genomic surveillance for SARS-CoV-2 variants circulating in the USA.Morbidity Mortality Weekly Rep. 2021 [December May 2021];70(23):846.
- Li M, Lou F, Fan H. SARS-CoV-2 variants of concern delta: a great challenge to prevention and control of COVID-19. Signal Transduct Target Ther. 2021;6(1):1–3.
- MacDonald NE, Comeau J, Dubé È, et al. Royal society of Canada COVID-19 report: enhancing COVID-19 vaccine acceptance in Canada. Facets. 2021;6(1):1184–1246.
- Mishra S, Mindermann S, Sharma M, et al. Changing composition of SARS-CoV-2 lineages and rise of Delta variant in England. EClinicalMedicine. 2021;39:101064.
- Mosby I, Swidrovich J. Medical experimentation and the roots of COVID-19 vaccine hesitancy among Indigenous peoples in Canada. Cmaj. 2021;193(11):E381–E383.
- World Health Organization. (2021). COVID-19 weekly epidemiological update, 30 November2021. World Health Organization. [cited 2022 April 20]. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19—30-november-2021
- Fisman DN, Tuite AR. Evaluation of the relative virulence of novel SARS-CoV-2 variants: a retrospective cohort study in Ontario, Canada. Canadian Medical Association Journal. 2021;193(42):E1619–E1625.
- Nyberg T, Ferguson NM, Nash SG, et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022;399(10332):1303–1312.
- Twohig KA, Nyberg T, Zaidi A, et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: a cohort study. Lancet Infect Dis. 2022;22(1):35–42.
- Bossak BH, Welford MR. Spatio temporal attributes of pandemic and epidemic diseases. Geogr Compass. 2010;4(8):1084–1096.
- O’Toole Á, Hill V, Pybus OG, et al. Tracking the international spread of SARS-CoV-2 lineages B. 1.1. 7 and B. 1.351/501Y-V2 with grinch. Wellcome open research. 2021. 6.
- Tebor C. (2021. cited July 1). Delta variant causes new lockdowns and coronavirus restrictions across the globe. Los Angels Times. Available from: https://www.latimes.com/world-nation/story/2021-07-01/delta-variant-worldwide-coronavirus-restrictions
- Zhongming Z, Linong L, Xiaona Y, et al. ‘Early stages’ of COVID third wave, amid Delta surge: WHO chief. (2021).
- World Health Organization. (2022). Tracking SARS-CoV-2 variants. [cited 2022 April 20] . Available from: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants
- Centers for Disease Control. (2021). Variants of the Virus. [cited 2022 April 20]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/variants/index.html
- EDC-WHO. (2021). Weekly COVID-19 Surveillance Bulletin. [cited 2022 May 9]. Available from: https://worldhealthorg.shinyapps.io/euro-covid19/
- Kindrachuk J, Shaw S. (2021). COVID-19 Delta variant in Canada: FAQ on origins, hotspots and vaccine protection. The Conversation. [cited 2022 April 20]. Available from: https://theconversation.com/covid-19-delta-variant-in-canada-faq-on-origins-hotspots-and-vaccine-protection-162653
- McGwin K. (2021). Greenland must learn to live with COVID, public health officials say. Arctic Today. [cited 2022 May 2]. Available from: https://www.arctictoday.com/greenland-must-learn-to-live-with-covid-public-health-officials-say/
- Schreiber M. (2021). Iceland fully reopens amid rising vaccinations and demand for tourism. Arctic Today. [cited 2022 May 5] Available from: https://www.arctictoday.com/iceland-fully-reopens-amid-rising-vaccinations-and-demand-for-tourism/
- Centers for Disease Control (CDC). (2022) Global variants report. COVID Data Tracker. [cited 2022 April 24]. https://covid.cdc.gov/covid-data-tracker/#global-variant-report-map
- Arctic Council. (2020). COVID-19 in the Arctic: briefing document for senior Arctic officials. [cited 2022 April 22]. Available from: https://oaarchive.arctic-council.org/handle/11374/2473
- Banning J. Why are Indigenous communities seeing so few cases of COVID-19? Can Med Assoc J. 2020;192(34):E993–4.
- Crosby AW. America’s forgotten pandemic: the influenza of 1918. Cambridge University Press; 2003.
- Mamelund S-E, Sattenspiel L, Dimka J. Influenza-associated mortality during the 1918–1919 influenza pandemic in Alaska and Labrador: a comparison. Social Sci Hist. 2013;37(2):177–229.
- Ward LA, Black KP, Britton CL, et al. COVID-19 cases, hospitalizations, and deaths among American Indian or Alaska Native Persons—Alaska, 2020–2021. Morbidity Mortality Weekly Rep. 2022;71(22):730.
- Huot S, Ho H, Ko A, et al., Identifying barriers to healthcare delivery and access in the Circumpolar North: important insights for health professionals. Int J Circumpolar Health. 2019;78(1):1571385.
- Adams LV, Dorough DS, Adams LV. Accelerating Indigenous health and wellbeing: the lancet commission on Arctic and Northern health. Lancet. 2022;399(10325):613–614.
- Petrov AN, Welford M, Golosov N, et al. The “second wave” of the COVID-19 pandemic in the Arctic: regional and temporal dynamics. Int J Circumpolar Health. 2021a;80(1):1925446.
- Fleury K, Chatwood S. Canadian Northern and Indigenous health policy responses to the first wave of COVID-19. Scand J Public Health. 2022;14034948221092185.
- Hillier SA, Chaccour E, Al-Shammaa H, et al. Canada’s response to COVID-19 for Indigenous peoples: a way forward? Can J Public Health. 2020;111(6):1000–1001.
- Richardson L, Crawford A. COVID-19 and the decolonization of Indigenous public health. Canadian Medical Association Journal. 2020;192(38):E1098–E1100.
- Markova VN, Alekseeva KI, Neustroeva AB, et al. Analysis and forecast of the poverty rate in the Arctic zone of the Republic of Sakha (Yakutia). Stud Russ Econ Dev. 2021;32(4):415–423.
- Lemieux T, Milligan K, Schirle T, et al. Initial impacts of the COVID-19 pandemic on the Canadian labor market. Can Public Policy. 2020;46(S1):S55–S65.
- Simonen J, Moilanen M, Westin L, et al. The Covid-19 pandemic and regional economic resilience in northern Finland, Norway, and Sweden–a pre-study. Oulu: University of Oulu; 2021.
- Cook D, Jóhannsdóttir L. Impacts, systemic risk and national response measures concerning COVID-19—The island case studies of Iceland and Greenland. Sustainability. 2021;13(15):8470.
- Men F, Tarasuk V. Food insecurity amid the COVID-19 pandemic: food charity, government assistance, and employment. Can Public Policy. 2021;47(2):202–230.
- Golubeva E, Emelyanova A, Kharkova O, et al. Caregiving of older persons during the COVID-19 pandemic in the Russian Arctic province: challenges and practice. Int J Environ Res Public Health. 2022;19(5):2775.
- McGwin K. (2021). Four COVID cases in Greenland spur concerns of a Delta-variant outbreak. Arctic Today. [cited 2022 April 23]. Available from: https://www.arctictoday.com/four-covid-cases-in-greenland-spur-concerns-of-a-delta-variant-outbreak/
- Spence N, White JP. Scientific certainty in a time of uncertainty: predicting vulnerability of Canada’s First Nations to pandemic H1N1/09. Int Indig Policy J. 2010;1(1):1.
- State of Alaska, Office of Governor. (cited March 9, 2021). Dunleavy announces COVID-19 vaccine available to all Alaskans-Mike Dunleavy. Available from: https://gov.alaska.gov/newsroom/2021/03/09/dunleavy-announces-covid-19-vaccine-available-to-all-alaskans/
- Arctic Council. (2021). COVID-19: the Arctic Experience. [cited 2022 April 24]. Available from: https://www.arctic-council.org/news/covid-19-the-arctic-experience/
- Petrov AN, Welford M, Golosov N, et al. Lessons on COVID-19 from Indigenous and remote communities of the Arctic. Nat Med. 2021b;27(9):1491–1492.
- Bogdanova E, Andronov S, Asztalos Morell I, et al. Food sovereignty of the Indigenous peoples in the Arctic Zone of Western Siberia: response to COVID-19 pandemic. Int J Environ Res Public Health. 2020;17(20):7570.
- Connolly M, Jacobs B, Notzon FC, COVID-19 among American Indians and Alaska Natives in the United States: an early look. Stat J IAOS. 2021;37(1):25–36.
- Fosse A, Svensson A, Konradsen I, et al. Tension between local, regional and national levels in Norway’s handling of COVID-19. Scand J Public Health. 2022;14034948221075408:1–8.
- Bogdanova E, Filant K, Ivanova M, et al. Strengthening collaboration of the Indigenous peoples in the Russian Arctic: adaptation in the COVID-19 Pandemic Times. Sustainability. 2022;14(6):3225.
- Palomino E, Pardue J. Alutiiq fish skin traditions: connecting communities in the COVID-19 Era. Heritage. 2021;4(4):4249–4263.
- Petrov AN, Hinzman LD, Kullerud L, et al. Building resilient Arctic science amid the COVID-19 pandemic. Nat Commun. 2020b;11(1):1–4.
- Retter GB. Indigenous peoples and COVID-19: challenges to achieving SDGs. Arctic (Inuit Nunaat and Sapmi) regional report. (2020).
- Petrov AN, Welford M, Golosov N, et al. Spatiotemporal dynamics of the COVID-19 pandemic in the Arctic: early data and emerging trends. Int J Circumpolar Health. 2020a;79(1):1835251.
- Einarsson E, Larsen JN, Nilsson A, et al. (2004). Arctic Human Development Report: Stefansson Arctic Institute. Akureyri, Iceland.
- Jungsberg L, Turunen E, Heleniak T, et al. (2019). Atlas of population, society and economy in the Arctic.
- ArcticVAX. (2021). Arctic COVID-19 vaccination. Retrieved April 23,, from https://univnortherniowa.maps.arcgis.com/apps/opsdashboard/index.html#/babca707eeac450c8604afc38230608b
- Forchette L, Sebastian W, Liu T. A comprehensive review of COVID-19 virology, vaccines, variants, and therapeutics. Curr Med Sci. 2021;41(6):1037–1051.
- Zhang M, Liang Y, Yu D, et al. A systematic review of vaccine breakthrough infections by SARS-CoV-2 delta variant. Int J Biol Sci. 2022;18(2):889.
- Dicker RC, Coronado F, Koo D, et al. (2006). Principles of epidemiology in public health practice; an introduction to applied epidemiology and biostatistics.
- ECDC. (2021). Surveillance definitions for COVID-19.European Center for Disease Prevention and Control. [cited 2022 May 9]. Available from: https://www.ecdc.europa.eu/en/covid-19/surveillance/surveillance-definitions
- Zhang SX, Arroyo Marioli F, Gao R, et al. A second wave? What do people mean by COVID waves? – a working definition of epidemic waves. <![cdata[risk Management and Healthcare Policy]]>. 2021;18:3775–3782.
- World Health Organization. (2021) [cited 2021 Jun 29]. COVID-19 Weekly Epidemiological Update, Edition 46, published. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19—29-june-2021
- Kamerlin SC, Kasson PM, Managing coronavirus disease 2019 spread with voluntary public health measures: Sweden as a case study for pandemic control. Clinl Infect Dis. 2020;71(12):3174–3181.
- Yan B, Zhang X, Wu L, et al., Why do countries respond differently to COVID-19? a comparative study of Sweden, China, France, and Japan. The American Review of Public Administration. 2020;50(6–7):762–769.
- Jones I, Roy P, Sputnik V COVID-19 vaccine candidate appears safe and effective. Lancet. 2021;397(10275):642–643.
- Government of Sweden. (2021). About the COVID-19 virus: extensions of national restrictions. Ministry of Health and Social Affairs. [cited 2022 May 11] Available from: https://www.government.se/articles/2021/02/about-the-covid-19-virus-extensions-of-national-restrictions/
- Government of Sweden. (2021). Government plan for phasing out restrictions. Ministry of Health and Social Affairs. [cited 2022 May 15]. https://www.government.se/articles/2021/05/government-plan-for-phasing-out-restrictions/
- Free C (cited 2021, February 4). How is Alaska leading the nation in vaccinating residents? With boats, ferries, planes and snowmobiles. The Washington Post. Available from: https://www.washingtonpost.com/lifestyle/2021/02/04/alaska-vaccine-covid-remote/
- Alaska Department of Health and Social Services (Alaska DHSS). (2021). One-year anniversary of the COVID-19 vaccine: Alaska helped lead the nation in delivering vaccines quickly and equitably. DHSS Insights Blog. [cited 2022 May 15] Available from: https://content.govdelivery.com/accounts/AKDHSS/bulletins/300e04b
- Government of Canada. (2021). Government of Canada COVID-19 update for Indigenous peoples and communities. Indigenous Services Canada. [cited 2022 May 15] https://www.canada.ca/en/indigenous-services-canada/news/2021/01/government-of-canada-covid-19-update-for-indigenous-peoples-and-communities.html
- Foxworth R, Redvers N, Moreno MA, et al. Covid-19 vaccination in American Indians and Alaska Natives—Lessons from effective community responses. N Engl J Med. 2021;385(26):2403–2406.
- Haroz EE, Kemp CG, O’Keefe VM, et al. Nurturing innovation at the roots: the success of COVID-19 vaccination in American Indian and Alaska native communities. Am J Public Health. 2022;112(3):383–387. American Public Health Association.
- Burki T. COVID-19 among American Indians and Alaska natives. Lancet Infect Dis. 2021;21(3):325–326.
- United Nations (UN). (2020). The Impact of COVID-19 on Indigenous peoples. Department of Economic and Social Affairs. Policy Brief 70. [cited 2022 May 11]. Available from: https://www.un.org/development/desa/dpad/wp-content/uploads/sites/45/publication/PB_70.pdf
- Indigenous Russia. (2020). The COVID 19 impact on indigenous peoples of the Russian Arctic, Siberia, and the far East. [cited 2022 May 17]. https://indigenous-russia.com/archives/6552
- Mashford-Pringle A, Skura C, Stutz S, et al. (2021) Indigenous peoples and COVID-19. Public Health Agency of Canada; 2021. [cited 2022 May 7].
- Qikiqtani Inuit Association (QIA). (2021), 2019-2020 Annual report. 2019-2020. [cited 2022 April 25]. https://www.qia.ca/wp-content/uploads/2020/11/qia-annual-report-2019-2020_web.pdf
- Vilches TN, Abdollahi E, Cipriano LE, et al. Impact of non-pharmaceutical interventions and vaccination on COVID-19 outbreaks in Nunavut, Canada: a Canadian Immunization Research Network (CIRN) study. BMC Public Health. 2022;22(1):1–9.
- Chatwood S, Bjerregaard P, Young TK. Global health—A circumpolar perspective. Am J Public Health. 2012;102(7):1246–1249.
