
ABSTRACT
Type 2 diabetes is a complex chronic disease rapidly increasing among young people and disproportionately impacting Indigenous youth. Treatment programs are often inadequate for this population as they lack cultural relevance. A scoping review was conducted to explore traditional Indigenous approaches for diabetes prevention and management, to inform a program aimed at supporting Indigenous youth and families with type 2 diabetes. We seek to answer the following question: “Which traditional medicines and practices have been incorporated into intervention or prevention strategies for Indigenous people living with diabetes?” Search was done June 2021 using Ovid Medline, ESBCO and ProQuest databases. Terms included wellbeing, intervention, diabetes, and traditional approaches. Of the 2138 titles screened, 34 met inclusion criteria. Three studies integrated traditional Indigenous approaches into Western-based intervention programming. Content included traditional food and nutrition programs, gardening programs, Elder knowledge sharing, story telling, talking circles, feasting, prayer, traditional dancing, hunting, and school-based wellness curricula. Many were wholistic, co-created with community, Indigenous-led and held in accessible community spaces. The heterogeneity in approaches reflects the diversity of Indigenous nations and communities. This review identifies important elements to include in culturally relevant programs to address diabetes-related wellness.
Background
According to Elder Belinda Vandenbroeck, carrier of her Ininew language and Ways of Being and Thinking, from, traditional diets of Indigenous Peoples pre-contact were high in protein and low in carbohydrates. She emphasises the importance of implementing a culturally relevant wellness program for Indigenous people, to offer traditional perspectives on diet, exercise and living well. Elder Vandenbroeck believes that it is critical that Indigenous people reconnect with their spirit and those who serve as spirit guides, to make decisions about their life from such relationships related to thought process, survival, and sustenance. Existing mainstream methods in nutrition education (such as National Food Guides) do not always offer culturally specific options for Indigenous people. However, the most recent iteration of Canada’s Food Guide provides considerations for Indigenous Peoples that were created in consultation with Indigenous healthcare professionals and national Indigenous-led organisations [Citation1]. Organizations that have embedded Indigenous healing practices in treatment strategies have observed increased uptake and improvement in wellness indicators [Citation2–6] Centre for Addiction and Mental Health, n.d.]. A gap exists around reducing inequities in type 2 diabetes rates among Indigenous youth and Indigenous communities in North America [Citation7]. Through this scoping review we [Citation8–13] sought to gather information through existing literature to inform the co-development of a culturally specific program with Indigenous communities, to support the prevention or management of type 2 diabetes among First Nations youth and their caregivers in Manitoba.
Wellbeing as understood by many Indigenous peoples is a wholistic concept that is in a continual state of development. In many cases, wellness involves finding balance between the spiritual, mental, emotional and physical aspects of a person’s health. Within each of these aspects is the inclusion of family wellness, community wellness, the wellbeing of the land, and feeling a sense of belonging within one’s environment Health and wellbeing among Indigenous people are intimately linked to their traditional lands, languages and cultural practices, and colonisation has been associated with disrupted wellness for Indigenous Peoples and disparities in several chronic diseases, including type 2 diabetes [Citation14,Citation15]. Prior to colonisation, diabetes was seldom observed among Indigenous people [Citation16]. The effects of forced cultural assimilation and colonialism on the increased prevalence of diabetes among Indigenous peoples have been documented for multiple decades
Type 2 diabetes is a rapidly increasing chronic disease among young people in Canada, documented to impact marginalised or non-white demographics facing systemic oppression disproportionately [Citation17]. Both physical and mental wellbeing is significantly impacted in youth with type 2 diabetes [17, 18, 47, Schwimmer, 2003]. Nearly 20% of patients with type 2 diabetes also experience depression, schizophrenia, bipolar disorder, autism, intellectual disabilities, attention-deficit hyperactivity disorder and/or obsessive-compulsive disorders [Citation18]. From a public health perspective, the development of diabetes at a young age hinders the longitudinal productivity of this demographic due to years lost from complications of the disease [Citation19].
Study rationale
In our community of Manitoba, Canada, there is a high prevalence of type 2 diabetes among First Nations children, especially those who live in northern rural communities [Citation20]. There are similar concerns across Canada and for other Indigenous communities around the world [Citation21,Citation22]. Between 2015/2016 and 2016/2017, there were 108,942 Manitobans ages seven and older with type 2 diabetes. Sixteen percent of these individuals were First Nations, whereas only 10% of the Manitoba population in that age range were First Nations [Citation23]. A scoping review was chosen to allow for an overview of extant literature on the topic of traditional cultural practices and Indigenous framework approaches used in diabetes care programs or intervention strategies among Indigenous people. The evidence found can be used to inform the development of culturally aligned programming.
Research question
The scoping review was guided by the research question, “Which traditional medicines and practices have been incorporated into intervention or prevention strategies for Indigenous people living with diabetes?” Studies from Canada, the USA, Australia, and New Zealand were qualified for this investigation. These four countries were chosen because their Indigenous populations share similar ways of being and knowing [Citation24]. While we acknowledge that all Indigenous nations have distinct laws and systems (including those within Canada), we also recognise commonalities across Indigenous cultures with regard to sacred and spiritual understandings of wellbeing. The scoping review was selected in place of a systematic review with meta-analysis as the variability in outcome measures and the quasi-experimental nature of most study designs in this area precluded a meta-analysis of outcomes. We also felt that a narrative review could result in biased, less comprehensive description of the interventions studied to date.
Objectives
This scoping review will provide insight into the variety of interventions and preventative measures used with Indigenous peoples with diabetes. The initial search strategy included only articles pertaining to type 2 diabetes among youth. However, search criteria were eventually expanded to include all age groups to be more inclusive, and in response to limited literature found on exclusively paediatric populations. Our objectives are to:
Identify components of existing diabetes management and prevention programs that are related to traditional medicines and healing practices,
Identify gaps in current literature related to traditional approaches in diabetes care, and
To inform the development of a culturally relevant diabetes management program for First Nations youth and caregivers in Manitoba.
Methods
Guiding approach
In alignment with scoping review best practices [Citation25], the review was carried out in five key phases: (1) establishing a research question and objectives, (2) developing inclusion criteria, (3) identifying appropriate studies (4) extracting data, and (5) synthesising results. We also added to the fifth phase by synthesising and interpreting the results with Indigenous Knowledge Keepers to determine the cultural aspects of each intervention, in addition to the interpretations from the internal research team.
Indigenous advisory elements
There is an expanding agreement that research pertaining to Indigenous populations should be conducted or co-directed by Indigenous persons (First Nations Information Governance Centre, 2020). Thus, the present research was both led by Indigenous students (MGu; LB; SLP) and guided by Indigenous Knowledge Keepers (an Indigenous community member possessing extensive knowledge of traditional ways of being, knowing, and doing) (BV; SC). Such guidance from the Knowledge Keepers was invaluable to the research process as they carry traditional knowledge and wisdom regarding the appropriateness of our project. The Knowledge Keepers were consulted during the first three phases of the screening process: (1) establishing a research question and objectives, (2) developing inclusion criteria, (3) consulting of the identification of appropriate studies and providing feedback on manuscript development.
Conceptual Framework
Our conceptual framework was largely characterised by TRC call to Action #18 that disparities in diabetes rates are the direct result of colonisation and settler systems [Citation26] and call to action #22 to recognise the value of Indigenous healing practices [Citation27]. Our work addressing these TRC calls to action are consistent with theory of decolonisation with emphasis on cultural, psychological and economic freedom and self-determination as a means to reducing the health disparity specifically noted in youth onset type 2 diabetes. Within the Integrated Life Course and Social Determinants Model of Aboriginal Health (ILCSDAH) framework by Reading and Wien, our work focused on the role of cultural continuity as an intermediate determinant of health and self-determination as a distal determinant of health (2009). This is reflected in both the process used to conduct this review, specifically with our consistent Indigenous advisors, as well as in our objective of understanding practices using traditional Indigenous approaches in diabetes care [Citation28].
Selection of Sources
During the first stage of screening, researchers evaluated article content based on reading the titles, keywords, and abstracts (MGu; LB; LM; MD). All articles were screened using their title and abstracts by any two of the reviewers who had the option to select “yes”, “no” or “maybe”, depending on if they believed the article fit within the inclusion criteria. Any arising conflicts were resolved at a weekly meeting, which included all reviewers and a third party for advisory (SLP).
This procedure was continued until all the articles, titles, and abstracts were screened. Articles considered admissible were noted for further screening at a more thorough level. Once the initial screening was complete, articles requiring a full-text review were pulled from their respective databases and each article was examined for eligibility. All reviewers were again involved in this full-text screening process, with two screening each article. Conflicts were resolved at a weekly meeting. Based on the eligibility criteria, articles were deemed as either suitable or unsuitable for inclusion in the data charting process.
Protocol
The PRISMA-ScR [extension for Scoping Reviews, 61] was selected as the protocol designated for the present study. This model is grounded in the original PRISMA framework, which has been used for meta-analysis and systemic reviews. The PRISMA-ScR was constructed to incorporate higher levels of suitable information and methodology within the scoping review process.
Eligibility criteria
Eligible studies met the following criteria: (1) Published in 1980 or later, (2) written in English, (3) involving Indigenous populations from Canada, The USA, Australia or New Zealand, and (4) involving traditional medicine or cultural practices and Indigenous framework approaches in the prevention and/or management of diabetes. Traditional medicine and cultural practices were defined as plant medicines, ceremony, and other approaches grounded in ancestral knowledge, and confirmed by the Knowledge Keepers on the team. Studies focused on gestational diabetes however were excluded as they would not be as immediately applicable to the development of our own programming with youth and caregivers.
Information sources
The search was conducted in June 2021. The databases Ovid Medline, ESBCO and ProQuest were searched for documents that could be relevant to the study and were published between 1980 and June 2021. The search strategy was reviewed by team members and Indigenous Knowledge Keepers who helped revise the search strategy. The results from each database were uploaded into a systematic review management software, CovidenceTM.
Search strategy
The search strategy consisted of the following keywords: “diabetes” and “traditional” or “cultural wellness” or “teaching(s)” or “knowledge keeper(s)” or “alternative medicine” or “elder(s)” or “mental health” or “medicine man/men” or “medicine woman/women” or “holistic” or “wholistic”, and “Indigenous” or “native(s)” or Indian” or “aboriginal(s)” or “First Nation(s)”.
Limitations applied to the search were any articles published in a language other than English, articles published before 1980 (prior to 1980 studies did not routinely include Indigenous scholarly input), population not from North America, Australia, or New Zealand, no mention/section on traditional medicine incorporation, community wellness, or prevention of chronic disease (diabetes). No dissertations were included. There were no limits on the type of research, both qualitative and quantitative studies were included.
Data charting process
A data extraction sheet was created to provide a template for the reviewers when pulling key findings from the articles. This sheet underwent multiple revisions and input from the Knowledge Keepers. Each article was assigned to two reviewers who filled out the data extraction sheet separately (LB and MDV). Conflicts were resolved at a weekly meeting.
Data collection
Variables extracted from articles included reference information such as authors, year of publication, and location of the study. The program title and modality were also collected. Since cultures across Indigenous communities differ from one another, the community’s name and location were important. How the traditional content was accessed (i.e. the level and type of community engagement) type of cultural content, and who delivered the content was further extracted from the articles. Additional information extracted included study design, the main study results, and any informative comments from participants.
Critical appraisal of individual sources of evidence
Indigenous input was examined for each source of evidence according to our guiding framework of self-determination. It was considered present if an author of the paper disclosed Indigenous identity or if authors noted that community members were involved in the design or implementation of the study.
Synthesis of results
The results below were summarised from the extracted data of the full-text review. During the extracting process, notes were taken regarding the relationship of each article to the research questions and objectives, i.e. traditional content used, type of program, approach, and development process, etc. These details were charted in an Excel file, which was later cleaned and reported herein (). We used this table to categorise program/approach type in the results section.
Table 1. Evidence Sources.
Results
Selection of sources of evidence
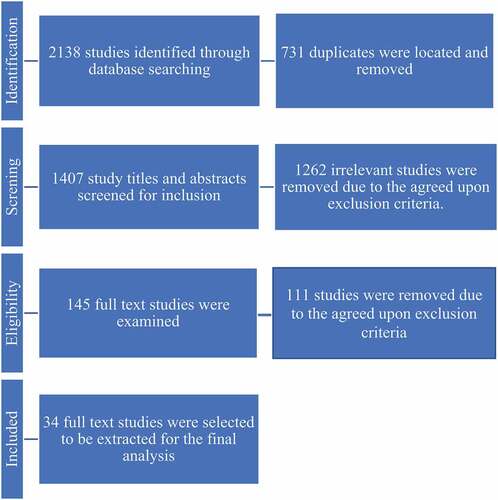
After entering our search criteria into systematic review management software CovidenceTM, 2138 studies were imported for screening potentially relevant citations. A total of 731 duplicates were located and removed before the reviewers screened the remaining 1407 study titles and abstracts. After screening the study titles and abstracts, 1262 irrelevant studies were removed due to the agreed upon exclusion criteria. The final remaining 145 full-text studies were examined, and 34 full-text studies were selected to be extracted for the final analysis. All included articles were published between 1998 and 2021 (
Table 2. Review articles.
The entire process of article screening from the initial recognition stage to the final inclusion stage is presented in (PRISMA flowchart of study selection process).
Figure 1. Electronic database searches – COVIDENCE.
Results have been categorised by program type, including community gardening, school-based curriculum, sharing circles and focus groups, and community-based approaches. No negative effects were observed from traditional approaches used in the identified evidence sources found (
Table 3. Traditional content summary.
Characteristics of sources of evidence
Fourteen studies found were from Canada, 17 from the USA, one from Australia, one study involved all four countries (Canada, The USA, Australia, and New Zealand), and another involved Canada, the USA, and New Zealand. These involved Alaska Native, Anishinaabe, Australian Aboriginal, Blackfoot, Ininew, Haida Gwaii, Māori, Haudenosaunee, Native American Indian, Navajo, and Anishininew Nations. Importantly, the heterogeneity in approaches found reflects the diversity of Indigenous nations and communities. Variations in components of programming must be understood as a demonstration of the values held by each community, representing histories and relationships with each other and the land in a given area.
Community gardening programs
Four of the admitted articles were group gardening programs that emphasised the importance of community collaboration [5, 9; 38, 59]. Many Indigenous communities face health challenges that are related to food insecurity due to historical and on-going impacts of colonisation, such as high rates of diabetes [Citation29]. In addressing limited access to nutritional foods [59], worked alongside community members in constructing hoop houses for vegetable gardens in Wapekeka First Nation, North-Western Ontario. In addition to growing vegetables, participants also felt a deeper connection to the land, traditional food practices, and each other. In a similar study, community gardening participants reported lower rates of depression, higher quality of life, good glucose management, and a greater willingness to consume vegetables when compared to the control group [Citation30].
School-based curriculum
A number of school-based diabetes prevention articles were examined, which centred on intervention programs with child and youth populations [Citation31–35]. Many of these studies were community centred and based on a partnership between community researchers and academic researchers [Citation32,Citation34]. One such intervention program is known as the “Kahnawake Schools Diabetes Prevention Project” (KSDPP) [Citation32–34]. Schools also implemented a year-long curriculum that covered healthy eating, physical activity, storytelling, science and tradition, and the risks of diabetes [Citation31,Citation35]. One community incorporated Haudenosaunee food cooking workshops for students [Citation33]. These workshops were deemed culturally acceptable and focused on traditional food, medicines, and spirituality.
Collecting information through focus groups and sharing circles
A common method across our search was using focus groups to qualitatively collect data from participants [Berry et al., 10, 11, 30, 42, 45, 52, 55, 60, 65]. Many of these researchers decided to facilitate the focus groups as talking circles or sharing circles. This choice was made so that the process would be more inviting and culturally appropriate.
Diabetes prevention and management within the community
Out of 34 articles, 27 of the studies were interested in diabetes prevention or management in the context of community (i.e. with programs delivered by community members, created in collaboration with community members, and/or held in community spaces) [1, 2; 5, 6, Broome & 8, 10, 9, 11, 13, 21, 22, 28, 30, 31, 36, 38, 59, 57, 41, 42, 49, 53, 55, Smith-52, 59; 65]. Sixteen of the sources identified were focused on adults, five were paediatric (focusing on children and youth), three included both a paediatric and adult population, and others did not specific an age category. It is important to note the adaptability of diabetes prevention and management programs between communities. In one study, across 11 cooperative American Indian and Alaska Native communities, each diabetes prevention or management program was uniquely tailored from one another in some way [Citation36].
Non-Intervention
Some studies within the selected literature were not intervention-based. The researchers chose to include one systematic review article because it pertained directly to the research question of how both traditional and contemporary medicine are used by Indigenous populations with type 2 diabetes [Citation37]. Findings concluded that Indigenous Peoples sought out traditional healing methods outside of healthcare systems when mainstream approaches were not inclusive of wholistic and culturally relevant methods of care. Key implications of this work included calls for public health providers to offer traditional healing methods to Indigenous patients alongside mainstream treatment approaches. Other reviews were included similarly due to relevant content related to community involvement in diabetes-specific health promotion projects as well as the importance of cultural traditions in healing programs [8,28,38,61; Stewart].
Two anthropological observation studies were also admitted as these articles focussed on the historical progression of type 2 diabetes among American Indian and Alaska Native communities [Citation38,Citation39]. Results highlight a need for systematic change, such as access to clean water, wholistic intervention, and treatment options that incorporate traditional food, activities, and teachings.
Results of individual sources of evidence
Of the 34 selected articles, three studies were diabetes programs that were closely related to our research question regarding traditional practices being incorporated into Western medicine for Indigenous persons with type 2 diabetes.
Rosas et al. [52] developed an enhanced diabetes prevention program that also included a psychosocial support component for self-declared obese participants with type 2 diabetes. Participants [n = 102] were randomised to either the enhanced diabetes prevention program with mental health supports, or the standard diabetes prevention program without mental health supports. Researchers collected Quality of Life measurements as well as body mass index. Although quantitative results were not included in this article, the paper discusses future data collection and the results of talking circles from individuals who participated in the program. Qualitative interviews with participants revealed that community members were enthusiastic to be learning about diabetes management and health advancement. Other identified program components were wholistic views of a person’s well-being and how local knowledge about diabetes is mediated through lived experiences.
Dart et al. [11] designed a two-year full circle diabetes management program in collaboration with the diabetes community council. The first year of the program was designed to include monthly group meals that distributed diabetes management content and group exercise classes, which took place four times a week. The second year of the program replaced the monthly group dinners with a five-week workshop that involved peer-teacher training. The traditional elements that were incorporated included time for prayers and blessings, talking circles, a wholistic health approach, and the involvement of Elders. Data were collected through surveys which gauged participant satisfaction with community activities, talking circles, nutritional teachings, group exercise classes, and traditional ceremonies and prayers. Out of the 249 urban male and female participants [ages: <40, 40–59, >60], two-thirds expressed having learned valuable knowledge for improved management of type 2 diabetes. Of all the surveyed activities, the most popular among participants were the group diabetes breakfasts, which also served to deliver nutritional content.
Brain et al. [30] carried out the Haida Gwaii diabetes project in two phases beginning with chart reviews and obtaining the Haida Gwaii community’s support. Permissions were sought prior to programming. The feedback from the focus groups was then used to plan out diabetes-related activities with community members. The second phase of the project involved the implementation and observation of prepared activities as well as hosting exit clinics. These activities included a 10-day traditional diet trial, a 40-day traditional herbal medicines trial, and the Getting Stronger exercise program. The Getting Stronger exercise program and traditional medicine and diet trials were well attended (7 community members attended the traditional medicine program regularly and an average of four people attended per class across 153 classes of the Getting Stronger program over a 13-month period). Researchers found a significant decrease in total cholesterol as well as an increase in high-density lipoprotein. Surveys of participants revealed that they were excited about the traditional diet, it was challenging for participants to obtain traditional foods and eat differently from others in their households due to inconveniences associated with finding and eating foods not offered in local stores, and the overall lack of availability of such foods in communities. Participants also reported that their favourite learning formats for diabetes education were the focus groups, video presentations, and lectures.
Discussion
This review sought to systematically compile published studies that describe traditional medicine, cultural practices and Indigenous framework approaches that have been incorporated into intervention or prevention strategies for Indigenous people living with, or at risk for diabetes. Results revealed processes through which diabetes prevention and intervention programs were developed and implemented, with limited details on specific traditional medicines and practices used within the programs. The types of programs presented here, however, include important cultural practices that could be replicated in future studies intervention studies. Program types include nutrition courses that are being implemented in schools, exercise programs that are being provided in communities, and mental health supports that are being offered as additional resources [2,22,41,49,52,53]. Traditional methods used in development and implementation processes include the incorporation of wholistic values related to spiritual, emotional, mental and physical wellbeing. Community gardening programs were also used, generating both a connection to land and each other, as well as an opportunity for access to traditional foods and plant medicines [Citation29,Citation30,Citation40,Citation41]. Other programs involve Elder counselling, prayer, sharing circles, and storytelling, fostering a sense of community surrounding diabetes-related wholistic health and wellbeing dialogues [2,5,6,11,40,60]. These sources exemplify the benefits of traditional approaches seen across mental and physical health dimensions. According to Article 24 of the United Nations Declaration on the Rights of Indigenous Peoples, Indigenous peoples have the right to maintain the use of traditional medicines and health practices [Citation42]. Further, the Truth and Reconciliation Commission of Canada outline in Call to Action 18 that health issues among Indigenous people are direct results of colonisation and cultural genocide. Equally in Call to Action 21 that traditional healing and cultural practices are an ideal path to reducing inequities [Citation15].
Other important components of program development included community consultation, Elder advisory roles, Indigenous methodological consideration, and community delivery to ensure autonomous control and self-determination in wellness care for other community members [Citation7,Citation29,Citation33–35,Citation40,Citation43–54]. Other programs were hosted in accessible, safe, and culturally meaningful buildings, or during ceremony [Citation35,Citation43,Citation49]. It becomes clear that a wholistic understanding of wellness must be translated into a dynamic and multi-component cultural program to best serve the diverse needs of Indigenous people at risk of or living with diabetes.
These findings align with recommendations from Elder Vandenbroeck regarding the value of returning to the sanctity in traditional ways of understanding 40. This is valuable when seeking to address and prevent adversity experienced by Indigenous youth living with type 2 diabetes, through culturally relevant diet and exercise programs, and a connection to spirituality. Taken together, there are several examples of Indigenous-led programs consisting of various traditional approaches to diabetes-related wellness based on values specific to respective Indigenous nations, with particular emphasis on wholistic health, community development, and Elder consultation. Aligned with this review’s conceptual foundation in self-determination, the results largely reflect a theme of Indigenous sovereignty through the recurring values of community programming developed and implemented by and for Indigenous community.
Limitations of this study include its lack of grey literature examination, potentially failing to capture existing programs and approaches that are not reported in academic journals or programs delivered in Indigenous communities grounded in Indigenous teachings/philosophies that were not identified within our search strategy [Citation55–58].
Next Steps
Moving forward, results can inform clinicians and community leaders to support Indigenous people managing type 2 diabetes. For our research group, these results will inform a pilot study to improve wellness in First Nations youth with type 2 diabetes. In partnership with an Indigenous advisory circle, we plan to implement cultural elements into a skills-based Dialectical Behavioural Therapy program to improve quality of life, and ultimately chronic disease management among this demographic of youth [Citation59,Citation60].
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Health Canada Office of Nutrition Policy and Promotion. (2019). The New Food Guide. Retrieved 2022 Jul 18, from https://www.canada.ca/content/dam/hc-sc/documents/services/canada-food-guide/resources/stakeholder-toolkit/canada-food-guide-presentation-eng.pdf
- Anishinawbe Health Toronto. (2022). Services. Retrieved 2022 Jul 27, from https://aht.ca/our-services/
- Centre for Addiction and Mental Health. (nd.). Building your medicine bundle: understanding your mental health journey. [Tip sheet]. [cited 2021 Jun 28]. https://indspire.ca/wp-content/uploads/2021/02/Indspire_CAMH_TipSheet-1.pdf
- Dart AB, Wicklow BA, Sellers EA, et al. The improving renal complications in adolescents with type 2 diabetes through the research (ICARE) Cohort Study: rationale and Protocol. Can J Diabetes. 2014;38(5):349–14.
- Daudt HML, Van Mossel C, Scott SJ. Enhancing the scoping study methodology: a large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med Res Methodol. 2013;13(1):1–9.
- Type 2 diabetes First Nations Information Governance Center. (2020). OCAP®. Retrieved 2020 Jul 21, from https://fnigc.ca/ocap
- Conti KM. Diabetes prevention in Indian country: developing nutrition models to tell the story of food-system change. J Transcult Nurs. 2006;17(3):234–245.
- Berry D, Samos M, Storti S, et al., Listening to concerns about Type 2 diabetes in an Native American community. J Cult Div. 2009. 16(2)
- Coser A, Sittner KJ, Walls ML, et al. Caregiving stress among American Indians with type 2 diabetes: the importance of awareness of connectedness and family support. J Fam Nurs. 2018;24(4):621–639.
- Dart AB, Wicklow B, Blydt-Hansen TD, et al. A Holistic Approach to Risk for Early Kidney Injury in Indigenous Youth With Type 2 Diabetes: a Proof of Concept Paper From the iCARE Cohort. Can J Kidney Health Dis. 2019;6:2054358119838836.
- Dart A, Martens P, Rigatto C, et al. Earlier onset of complications in youth with type 2 diabetes. Diabetes Care. 2014;37(2):436–443.
- Edwards KA, Pryor S, Jacobsen S, et al. Calorie use and obesity among diabetic and non-diabetic Mvskoke Indians. J Cult Div. 2000;7(2):36.
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473.
- King M, Smith A, Gracey M. Indigenous health part 2: the underlying causes of the health gap. Lancet. 2009;374(9683):76–85.
- Truth and Reconciliation Commission of Canada. (2015) Truth and Reconciliation Commission of Canada Calls to Action. [cited 2021 Jun 30]. Retrieved from http://www.trc.ca
- West KM. Diabetes in American Indians and other native populations of the New World. Diabetes. 1974;23(10):841–855.
- Jensen ET, Dabelea D. Type 2 diabetes in youth: new lessons from the SEARCH study. Curr Diab Rep. 2018;18(6):1–7.
- Levitt Katz LE, Swami S, Abraham M, et al. Neuropsychiatric disorders at the presentation of type 2 diabetes mellitus in children. Pediatr Diabetes . 2003;6(2):84–89.
- Dean H, Moffatt ME. Prevalence of diabetes mellitus among Indian children in Manitoba. Arct Med Res. 1988;47(1):532–534.
- Sellers EA, Wicklow BA, Dean HJ. Clinical and demographic characteristics of type 2 diabetes in youth at diagnosis in Manitoba and Northwestern Ontario (2006–2011). Can J Diabetes. 2012;36(3):114–118.
- Crowshoe L, Dannenbaum D, Green M, et al. Type 2 diabetes and Indigenous peoples. Can J Diabetes. 2018;42:S296–S306.
- Naqshbandi M, Harris SB, Esler JG, et al. Global complication rates of type 2 diabetes in Indigenous peoples: a comprehensive review. Diabetes Res Clin Pract. 2008;82(1):1–17.
- Ruth C, Sellers E, Chartrand C, et al. Type 2 Diabetes in Manitoba. Winnipeg: MB. Manitoba Centre for Health Policy; 2020.
- Boot GR, Lowell A. Acknowledging and promoting indigenous knowledges, paradigms, and practices within health literacy-related policy and practice documents across Australia, Canada, and New Zealand. Int Indig Policy J. 2019;10(3).
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Social Research Methodology: Theory and Practice. 2005;8(1):19–32.
- Smylie J, Harris R, Paine SJ, et al. Beyond shame, sorrow, and apologies—action to address indigenous health inequities. bmj. 2022;8: 378.
- Richardson L, Boozary A. Truth and reconciliation in Canada’s health system. Elsevir Ltd. United States of America: Lancet (London, England); 2021.
- Reading CL, Wien F (2009). Health inequalities and the social determinants of Aboriginal peoples’ health.
- Thompson HA, Mason CW, Robidoux MA. Hoop house gardening in the Wapekeka first nation as an extension of land-based food practices. Arctic. 2018;71(4):407–421.
- Brown B, Dybdal L, Noonan C, et al. Group gardening in a native American community: a collaborative approach. Health Promot Pract. 2020;21(4):611–623.
- Aho L, Ackerman J, Bointy S, et al. Health is life in balance: students and communities explore healthy lifestyles in a culturally based curriculum. Pimatisiwin. 2011;8(3):151.
- Delormier T, Cargo M, Kirby R, et al., Activity implementation as a reflection of living in balance: the Kahnawake schools diabetes prevention project. J Aboriginal & Indigenous Com. 2003. 1(1)
- Murdoch-Flowers J, Tremblay MC, Hovey R, et al. Understanding how Indigenous culturally-based interventions can improve participants’ health in Canada. Health Promot Int. 2019;34(1):154–165.
- Potvin L, Cargo M, McComber AM, et al. Implementing participatory intervention and research in communities: lessons from the Kahnawake schools diabetes prevention project in Canada. Soc sci med. 1982;56(6):1295–1305.
- Rosecrans AM, Gittelsohn J, Ho LS, et al. Process evaluation of a multi-institutional community-based program for diabetes prevention among First Nations. Health Educ Res. 2007;23(2):272–286.
- Satterfield D. Health promotion and diabetes prevention in American Indian and Alaska Native communities—Traditional foods project, 2008–2014. MMWR supplements. 2016: 65
- Gall A, Butler TL, Lawler S, et al. Traditional, complementary and integrative medicine use among Indigenous peoples with diabetes in Australia, Canada, New Zealand and the USA. Aust N Z J Public Health. 2021;1–8. DOI:10.1111/1753-6405.13120
- Olson B. applying medical anthropology: developing diabetes education and prevention programs in American Indian cultures. Am Indian Culture Res J. 1999;23(3):185–203.
- Smith-Morris. Community Participation in Tribal Diabetes Programs. Am Indian Culture Res J. 2006;30(2):85–110.
- Armstrong DL. A Community Diabetes Education and Gardening Project to Improve Diabetes Care in a Northwest American Indian Tribe. Diabetes Educ. 2000;26(1):113–120.
- Lombard KA, Forster-Cox S, Smeal D, et al. Diabetes on the Navajo nation: what role can gardening and agriculture extension play to reduce it? Rural Remote Health. 2006;6(4):1–16.
- United Nations. (2007). United Nations Declaration on the Rights of Indigenous Peoples. [cited 2021 Jun 28]. Retrieved from https://www.un.org/development/desa/indigenouspeoples/declaration-on-the-rights-of-indigenous-peoples.html
- Abbott PA, Davison JE, Moore LF, et al. Effective Nutrition Education for Aboriginal Australians: lessons from a Diabetes Cooking Course. J Nutr Educ Behav. 2012;44(1):55–59.
- Brown BD, Harris KJ, Harris JL, et al. Translating the Diabetes Prevention Program for Northern Plains Indian Youth Through Community-Based Participatory Research Methods. Diabetes Educ. 2010;36(6):924–935.
- Castro S, O’Toole M, Brownson C, et al. A diabetes self-management program designed for urban American Indians. Prev Chronic Dis. 2009;6(4):A131–A131.
- Heffernan C, Herbert C, Grams GD, et al. The Haida Gwaii Diabetes Project: planned response activity outcomes. Health Soc Care Community. 1999;7(6):379–386.
- Hindelang M, Traditional ecological knowledge of the Lake Superior region explorations to engage students in culture scientific inquiry, and wellness activities. J Aboriginal & Indigenous Community Health. 2006. 4(2)
- McKennitt DW, Evaluation: professional relations in Aboriginal diabetes education program at the Aboriginal diabetes wellness program. Pimatisiwin: A Journal of Aboriginal & Indigenous Community Health. 2006. 4(1)
- Murphy E, McAuley KA, Bell D, et al. A new approach to design and implement a lifestyle intervention programme to prevent type 2 diabetes in New Zealand Maori. Asia Pac J Clin Nutr. 2003;12(4):419–422.
- Oster RT, Grier A, Lightning R, et al. Cultural continuity, traditional Indigenous language, and diabetes in Alberta First Nations: a mixed methods study. Int J Equity Health. 2014;13(1):92–99.
- Pilon RS, Benoit M, Maar M, et al. Decolonizing Diabetes. Int J Indigenous Health. 2019;14(2):252–275.
- Rosas LG, Vasquez JJ, Naderi R, et al. Development and evaluation of an enhanced diabetes prevention program with psychosocial support for urban American Indians and Alaska natives: a randomized controlled trial. Contemp Clin Trials. 2016;50:28–36.
- Tremblay MC, Bradette‐Laplante M, Witteman HO, et al. Providing culturally safe care to Indigenous people living with diabetes: identifying barriers and enablers from different perspectives. Health Expectations: International Journal of Public Participation in Health Care and Health Policy. 2021;24(2):296–306.
- Wakani L, Bernier I, Macdonald ME, et al. Diabetes Bingo! Using participatory research to tackle diabetes with the Algonquin of Barriere Lake. 2014.
- Eskicioglu P, Halas J, Sénéchal M, et al. Peer mentoring for type 2 diabetes prevention in first nations children. Pediatrics. 2014;133(6):e1624–e1631.
- Kakekagumick KE, Naqshbandi Hayward M, Harris SB, et al. Sandy lake health and diabetes project: a community-based intervention targeting type 2 diabetes and its risk factors in a first nations community. Front Endocrinol (Lausanne). 2013;4:170.
- Lopresti S, Willows ND, Storey KE, et al., IYMP National Team. Indigenous Youth Mentorship Program: essential characteristics of a Canadian multi-site community-university partnership with Indigenous communities. Health Promot Int. 2022;37(1):daab039.
- Narayan KM, Hoskin M, Kozak D, et al. Randomized clinical trial of lifestyle interventions in Pima Indians: a pilot study. Diabet Med. 1998;15(1):66–72.
- Dimeff L, Linehan MM. Dialectical behavior therapy in a nutshell. The California Psychologist. 2001;34(3):10–13.
- Vandenbroeck B, Cree Nation O. Lives in Headingley, Manitoba. Oral teaching. Personal communication.
- Broome. Native Americans: traditional healing. Urol Nurs. 2007;27(2):161–173.
- DeBruyn L, Fullerton L, Satterfield D, et al. Integrating Culture and History to Promote Health and Help Prevent Type 2 Diabetes in American Indian/Alaska Native Communities: traditional Foods Have Become a Way to Talk About Health. Prev Chronic Dis. 2020;17:12.
- Harris SB. What works? Success stories in Type 2 diabetes mellitus. Diabetic Med. 1998;15(S4 4):S20–S23.
- Jennings D, Johnson-Jennings M, Little M. Utilizing webs to share ancestral and intergenerational teachings: the process of co-building an online digital repository in partnership with Indigenous communities. Genealogy. 2020;4(3):70.
- Kirby AM, Lévesque L, Wabano V, A qualitative investigation of physical activity challenges and opportunities in a northern-rural, aboriginal community: voices from withiN. Pimatisiwin: A Journal of Aboriginal & Indigenous Community Health. 2007. 5(1)
- Patten SB, Beck CA, Kassam A, et al. Long-term medical conditions and major depression: strength of association for specific conditions in the general population. Can J Psychiatry. 2005;50(4):195–202.
