
Abstract
“Compulsive Shopping” is characterized by poorly controlled preoccupations/urges/behaviors focused on shopping and spending, causing significant distress/impairment. This study looked at what roles executive and related memory problems might exist in compulsive shopping. 205 adults completed on-line questionnaires measuring compulsive shopping, mood, as well as working memory and inhibition components of executive function. The Bergen Shopping Addiction Scale was used to assign participants to either a High Compulsive Shopping (HCS) group or Low Compulsive Shopping (LCS) group. Working memory (WM) and inhibition control (IC) were measured as two components of executive function (EF) using the Adult Executive Functioning Inventory (ADEXI), the Dysexecutive Questionnaire Revised (DEX-R) measured general EF. The Hospital Anxiety and Depression Scale measured anxiety and depression. MANCOVA and mediation analyses were carried out controlling for age, gender, anxiety, depression. The HCS group scored significantly higher on all three EF measures, indicating greater executive difficulties. Subsequent mediation analyses with the ADEXI-IC as the mediator removed the significance of the relationship between Group and both the DEX-R and ADEXI-WM outcome variables. Thus, observed Group difference in DEX-R and ADEXI-WM could be fully accounted for by group differences in inhibitory control. The results highlight the role inhibitory control plays in compulsive shopping.
Introduction
Shopping for, and buying, non-essential items are something that almost everyone finds pleasurable to some degree. However, when shopping becomes a kind of “compulsion” or “addiction” it can become problematic and can lead to significant issues in many spheres of life, including personal, occupational, and financial domains. Compulsive Buying or Shopping is characterized by excessive or poorly controlled preoccupations, urges, and/or behaviors focused on shopping and spending, which can cause psychological distress and lead to a reduced quality of life (Black, Citation2007, Citation2010; Dell’Osso et al., Citation2008; Koran et al., Citation2006). Maraz et al. (Citation2016) in their meta-analytic review reported that individuals with “Compulsive Buying Disorder” (CBD) experienced elevated occurrences of debt, legal and financial problems, criminal-legal problems and guilt. They also noted that individuals with CBD were more likely to have recreational drug issues. In this review Maraz et al., Citation2016 noted an incidence rate of approximately 5% in the general population, but with excessive heterogeneity, associated with factors such as age and gender. Some research noted that around 80% of individuals with CBD were women (Christenson et al., Citation1994; McElroy et al., Citation1994), others reported higher values, and suggested that this does represent a genuine sex difference in behavior, rather than a sampling bias (e.g. Dittmar, Citation2004). The onset of compulsive buying appeared to be around the late teens or early twenties, presumably when individuals gained some financial independence (Christenson et al., Citation1994; Schlosser et al., Citation1994).
The main characteristics of CBD include a preoccupation with looking and shopping for items that one covets, but do not necessarily need, having difficulty in resisting the urge to purchase such items, as well as the financial, social and personal consequences that can follow (Black, Citation2007; Christenson et al., Citation1994; Tyagi & Shyam, Citation2019). Individuals with CBD typically report strong feelings of depression, anxiety, boredom, and self-criticism, all of which are reduced by a subsequent spending spree, which brings about temporary relief and even euphoria (Bani-Rshaid & Alghraibeh, Citation2017; Gallagher et al., Citation2017; Miltenberger et al., Citation2003). McElroy et al. (Citation1994) provided an operational definition of CBD, noting that it displays both cognitive and behavioral components: (i) a preoccupation with buying or shopping and impulsive urges to shop; (ii) marked distress relating to the impulses and their negative social and financial consequences, (iii) lack of restriction of the shopping behaviors during periods of hypomania or mania.
There is evidence that CBD runs in families, and is also linked with mood disorders, anxiety problems and substance misuse. For example, in their report of CBD cases McElroy et al. (Citation1994) noted that 17/18 had one or more first degree relatives suffer from depression, eleven had relatives suffering from drug or alcohol problems and three had relatives with anxiety disorders. Other studies have reported strong associations between CBD and Axis I disorders, including mood disorders (e.g. Black et al., Citation1997; McElroy et al., Citation1994; Unsalver et al., Citation2018); substance use disorders (e.g. Black et al., Citation1998 Brook et al., Citation2015); eating disorders (e.g. Harnish et al., Citation2019; McElroy et al., Citation1994) and impulse control disorders (e.g. Christenson et al., Citation1994; Jung, Citation2017). It has also been associated with Axis II disorders with obsessive-compulsive disorder being the most commonly linked (e.g. Schlosser et al., Citation1994). Although CBD is not classed as a formal psychiatric disorder and does not appear in the DSM-5, it is often likened to a “behavioural addiction” because of the compulsive and obsessive nature of the behavior (Hollander & Allen, Citation2006) and its relationship with generic impulse control disorders (Jung, Citation2017; Muller et al., Citation2009).
One aspect of CBD not yet full articulated in the research is the association with executive dysfunction, despite the suggestions above of a core challenge to impulse control. Executive dysfunction relates to challenges in high level cognitive control, emotional regulation and behavioral impulsivity (or disinhibition, Robbins & Clark, Citation2015), and is associated with impaired pre-frontal networks (Simblett et al., Citation2017). The relationship of impulse control and addictive behaviors has been made explicit in the Interaction of Person-Affect-Cognition-Execution (I-PACE) model (Brand et al., Citation2019). The emphasis in this account has been upon the characterization of the neuropsychological features present across a range of addictive behaviors, including CBD. The authors identified executive function challenges as a vulnerability factor for addiction, rather than a consequence of the addiction. A common element of many compulsive and addictive behaviors is that the individual is faced with a contrasting combination of pleasurable outcomes, the participation in the activity itself, versus negative outcomes, which in the context of compulsive buying may be debt, legal problems, guilt etc. Thus, the individual places themselves in a context of decision making under risk conditions (Schiebener & Brand, Citation2015). In order to objectively assess the benefits and potential disadvantages a range of cognitive and emotional processes are recruited into the decision processing; prior outcomes and emotional reactions, and executive resources which can retrieve this information and inform decision making in working memory ( see Figure 2, Schiebener & Brand, Citation2015). A further key process in the decision process is inhibitory control. In the I-PACE account (Brand et al., Citation2019) inhibitory control was seen as an essential component in both the early (vulnerability) and later stages of the addiction process. Robbins and Clark (Citation2015) differentiated between various aspects of inhibitory or impulsive behaviors: impulsive action as is seen in the Go-No Go RT paradigm; impulsive choice, e.g., as in the temporal discounting delayed gratification paradigm. Robbins and Clark also distinguished between inhibitory responses required before or after response initiation, a waiting/stopping dichotomy. They argued that impaired “stopping” behavior could lead to continued repetition of behavior despite the possibility of negative consequences.
Research by Yan et al. (Citation2021) looked at a number of inhibitory processes in young adults with high levels of compulsive internet gaming or substance dependency. The study found a common pattern of inhibitory impairment in these two groups with respect to Delayed Discounting, Go-No Go and Stroop task performances. This finding supported the generic impulse control prediction of the I-PACE model (Brand et al., Citation2019). This notion of a general inhibitory deficit was explored in a CBD context by Lindheimer et al. (Citation2020) who employed a generic inhibitory motor task, the Stroop, with a sample of participants varying in compulsive buying characteristics. These authors found that variation in compulsive buying characteristics significantly accounted for 5% of unique variance in Stroop performance.
Rationale and hypotheses
The Brand et al. (Citation2019) model, like many other accounts of addictive behavior, placed an emphasis upon the role of dopaminergic reward systems in the behavior. A key component of this are the neurons in the mesolimbocortical dopamine system which originate in the midbrain region, in particular the ventral tegmental area. From here the pathway projects to the striatum, the ventral striatum of which consists of the nucleus accumbens and the olfactory tubercle. Nucleus accumbens activation has been strongly implicated in the reward-related cue response process in addictive behaviors in general and compulsive buying in particular (Trotzke et al., Citation2021; Wegmann et al., Citation2018). The ventral tegmental projection also targets the cerebral cortex, where dopamine density is relatively strong in the pre-frontal cortex (PFC), as well as in the hippocampal region (D’Esposito & Postle, Citation2015). The PFC projection is associated with working memory function, but interestingly, D’Esposito and Postle considered working memory performance in terms of both PFC and striatum activity. For the purposes of the present paper, the key element of these observations is that dopaminergic processes are important for effective functioning in both emotional and cognitive regulation and that dopamine dysregulation is likely to be associated with challenges to emotional regulation processes associated with addictive behaviors, and to cognitive control process.
The present study aimed to extend the findings of the Lindheimer et al. (Citation2020) research by looking at the relationship between compulsive shopping and self-reported executive functioning. Measures such as the Dysexecutive Questionnaire Revised (DEX-R, Simblett et al., Citation2017) and the Adult Executive Functioning Inventory (ADEXI: Holst & Thorell, Citation2018) are viewed as more ecological measures of executive efficacy in daily life contexts (Thorell & Nyberg, Citation2008; Toplak et al., Citation2013). Contexts where cognitive and emotional factors could contribute to the decision making underlying the behaviors. Consequently, the use of the DEX-R and the ADEXI can be considered to extend and complement the use of lab-based task procedures. In addition, the ADEXI measures distinguishes between an executive working memory component (ADEXI-WM) and an executive inhibitory control process (ADEXI-IC).
Excessive purchasing requires decision making in a risky context, with pleasure in the activity may come the perils of debt, guilt and other negative consequences. Schiebener and Brand (Citation2015) place a combination of cognitive and emotional processes at the heart of these decision-making processes; executive processes are critically involved in the retrieval and organization of prior experiences and the development of judgment strategies within working memory. Inhibitory processes will impact upon the outcome of these judgment formulations, dependent upon the pleasure/risk deliberation. Given the suggestion in this research that executive, working memory and inhibition processes are critical in the decision-making process, it was predicted that performance in the three executive measures, DEX-R, ADEXI-WM and ADEXI-IC would be relatively impaired, in the group of participants with high Compulsive Shopping behaviors. In addition, given the central importance of inhibition in executive functioning (Miyake & Friedman, Citation2012) and the importance of inhibitory control in the I-PACE model (Brand et al., Citation2019) it was further predicted that the ADEXI-IC measure could act as a significant mediator of the Compulsive Shopping—DEX-R relationship and the Compulsive Shopping—ADEXI-WM relationship. In all of these analyses, age gender, depression and anxiety measures were employed as covariates.
Methods
Design
Since the primary aim of the study was to determine the relationship between compulsive shopping and executive function, a quantitative between-groups design was adopted. Age, gender, and HADS (depression and anxiety) scores were employed as control variables. Outcome variables were the ADEXI-Working Memory, ADEXI-Inhibitory Control, and the DEX-R measure. Scores on the Bergen Shopping Addiction Scale (Andreassen et al., Citation2015) were used to create a dichotomous variable of “High Compulsive Shopping” (HCS) and “Low Compulsive Shopping” (LCS) groups based on the participant scores on the scale. The Adult Executive Functioning Inventory (Holst & Thorell, Citation2018) measured working memory and inhibition, and the Dysexecutive Questionnaire Revised Adult Executive Functioning Inventory (Simblett et al., Citation2017) measured global executive function. Demographic data was comprised of age and gender of participant. Finally, the Hospital Anxiety and Depression Scale (Snaith & Zigmund, Citation1994) provided a measure of both anxiety and depression symptomatology.
Participants
Participants for the study were unpaid volunteers and were recruited via emails and advertising on social media sites, such as Facebook and Twitter. The inclusion criteria for the sample was that the participant must be 18-years or over. They were also advised not to participate if they suffered from some condition which might cause them difficulty or distress when completing the tasks, such as a neurological or psychiatric condition. The study was conducted online using Qualtrics software and 225 participants were recruited, from which 20 failed to complete the survey and were therefore omitted from the data base. For the 205 participants who completed the survey, their overall mean age (SD) was 26.3 (8.9) years, and with age ranging from 18 to 48 years. Forty-two participants were allocated to the HCS group (39 females) with a mean (SD) of 25.4 (8.73) years, 163 participants were in the LCS group (135 females) with a mean (SD) age of 26.5 (8.96). Analysis indicated a non-significant difference in the mean ages of the two groups, F (1, 204) = 0.56, p > .05. 39. Chi Square analyses indicated a non-significant difference in the relative frequency of women and men across the two groups, Χ2 = 2.59, df = 1, p > .05.
Materials
Compulsive Shopping was measured using the Bergen Shopping Addiction Scale (Andreassen et al., Citation2015) which consists of 28 statements and asked the participant to rate how strongly each statement relates to their thoughts and behavior over the previous 12 months (Andreassen et al., Citation2015). The 5-point response options were completely disagree (0), disagree (1), neither disagree nor agree (2), agree (3), and completely agree (4), with the higher score indicating a greater level of “compulsive shopping”. Groups of four items are targeted toward each of seven addiction criteria (salience, mood modification, conflict, tolerance, withdrawal, relapse, and problems). To create a dichotomous variable of a High Compulsive Shopping (HCS) group and a Low Compulsive Shopping (LCS) group, the participant had to score at least 3 or 4 on the scale on at least 4 of the seven addiction criteria, therefore a high score on over 50% of the addiction criteria, before they were assigned to the HCS group. Anyone rating below this was assigned to the LCS group. This procedure is recommended by the authors of the BSAS and is consistent with calculations for other measures of addiction (see Andreassen et al., Citation2015, p. 9).
Working memory and cognitive inhibition were measured using the Adult Executive Functioning Inventory (Holst & Thorell, Citation2018). This is a 14‐item self-report scale that measures both working memory and inhibition in adulthood and uses a 5-point Likert scoring scale ranging from 1 (definitely not true) to 5 (definitely true). Examples of questions include: “I have difficulties with tasks or activities that involve several steps.” (working memory) and “I have a tendency to do things without first thinking about what could happen.” (cognitive inhibition). A higher score indicates poorer executive working memory and executive inhibitory control.
The Dysexecutive Questionnaire Revised (Simblett et al., Citation2017) was used as a generic measure of executive functioning. The DEX-R is a 37-item self-report questionnaire constructed to assess a wide range of common processes that make up executive function and is a valid and reliable measure of global executive function (Simblett et al., Citation2017). Scoring is based on a 5-point rating scale from 0 (never) to 4 (very often) and examples of the questions include: “I have trouble making decisions.” and “I find it difficult to do or concentrate on two things at once.” A total score is calculated a higher score indicates more executive function problems experienced by the person.
Finally, mood (anxiety and depressed mood) was measured using the Hospital Anxiety and Depression Scale (Snaith & Zigmund, Citation1994). This is a 14-item, self-report scale employing a four-choice response format. Seven items relate to generalized anxiety symptoms (e.g., “I feel tense or ‘wound up’”) and 7 relate to depressive symptomatology (e.g., “I have lost interest in my appearance”). The focus is on the last few days. Two separate scores are obtained, one for anxiety and one for depression, with the higher scores on each scale indicate more severe characteristics.
Procedure
Following institutional ethical approval, participants were directed to the online survey tool Qualtrics where they received information about the study. After providing informed consent they were asked to provide basic demographic data (age and sex) and were then asked to complete the measures in their own time. Each participant completed the BSAS first, followed by the ADEXI, DEX-R and finally the HADS. Each participant was asked to provide a unique code so that their data could be withdrawn later is they so wished. On completion all participants were fully debriefed and confidential helplines were provided for those who felt they needed them.
Data treatment
The data was analyzed using SPSS 26. Descriptive statistics were initially carried out to identify Group (Non-Compulsive Shopping, Compulsive Shopping) mean and standard deviation scores in the three executive measures; the Dysexecutive Questionnaire Revised (DEX-R), the Adult Executive Functioning Inventory—Working memory component (ADEXI-WM), and the Adult Executive Functioning Inventory—Inhibitory Control component (ADEXI-IC). Means and standard deviations were also calculated for the covariates of age, anxiety, and depression. Three one-way ANOVAS looked at the difference between the groups in terms of age, anxiety, and depression scores. The subsequent MANCOVA looked at the differences between the groups, in terms of the three executive measures, controlling for age, gender, anxiety and depression. Mediation analyses were then carried out, with Group as the main predictor, DEX-R and ADEXI-WM as the outcome variables, with ADEXI-IC as the mediator variable and with age, gender, anxiety, and depression as the covariates. Inhibitory control was chosen as the mediator variable given the key role it plays in the early and later stages of addiction formation and the role it plays in compulsive buying disorder—that is the inability to stop shopping compulsively despite its negative consequences. It is conventional to consider discriminant functional analyses after MANOVA, however, it was felt that the standardized canonical coefficients or effect sizes whilst showing the relative importance of the inhibitory control measure for the group difference does not, in our opinion, fully highlight, the importance of inhibition for each of the DEX-R and ADEXI-WM relationships with group membership in the way that separate mediation analyses would. In the mediation figure and reported statistics, all of the reported beta values were standardized.
Data analyses
The descriptive statistics comparing both groups on age, anxiety, and depression, are included in . The Group descriptive statistics indicated that with all three of the executive measures, the Compulsive Shopping group had higher mean values, indicating greater executive challenges (see ).
Table 1. Group differences as a function of age, anxiety, depression and three executive measures; the Dysexecutive Questionnaire Revised (DEX-R), the Adult Executive Functioning Inventory—Working memory component (ADEXI-WM), and the Adult Executive Functioning Inventory—Inhibitory Control component (ADEXI-IC).
None of the three co-variates were associated with the Group factor; Group-Age, rpb = −.054, p = .442; Group-HADS Anxiety, rpb = .106, p = .131; Group-HADS Depression, rpb = .125, p = .073. Three one-way ANOVAS, with Bonferroni correction set at p = .017, revealed no significant between group differences for age (F (1, 203) = 0.59, p = .442), anxiety (F (1, 203) = 2.29, p = .131), or depression (F (1, 203) = 3.24, p = .073). The pattern of data in the descriptive statistics for the executive measures was further investigated with a MANCOVA and revealed a statistically significant difference in overall executive function score between the groups. Using Wilk’s lambda, the MANCOVA revealed a significant effect associated with Group, λ = 0.85, F (3,197) = 11.38, p < .001, partial η2 = .148. The subsequent ANOVA analyses, with Bonferroni correction set at p = .017, showed a significant Group effect with DEX-R, F (1,199) = 10.49, p < .001, partial η2 = .050; ADEXI-WM, F (1,199) = 4.22, p = .041, partial η2 = .021; and ADEXI-IC, F (1,199) = 33.92, p < .001, partial η2 = .146.
For the DEX-R, gender did not significantly contribute to the model F (1, 199) = 0.09, p = .763, partial η2 = .000. Age did contribute significantly to the model F (1, 199) = 21.93, p <.001, partial η2 = .100, as did anxiety F (1, 199) = 3.92, p = .049, partial η2 = .019 and depression F (1, 199) = 107.54, p <.001, partial η2 = .351. For the ADEXI-WM, gender did not significantly contribute to the model F (1, 199) = 0.11, p = .742, partial η2 = .001, nor did age F (1, 199) = 1.72, p = .191, partial η2 = .009 or anxiety F (1, 199) = 1.26, p =.263, partial η2 = .006. Depression did significantly contribute to the model F (1, 199) = 10.28, p = .002, partial η2 = .049. For the ADEXI-IC, gender did not significantly contribute to the model F (1, 199) = 0.28, p = .595, partial η2 = .001/Age did contribute significantly to the model, F (1, 199) = 13.64, p < .001, partial η2 = .064. Anxiety was not significant, F (1, 199) = 1.26, p =.263, partial η2 = .006. Depression did significantly contribute to the model F (1, 199) = 8.62, p < .001, partial η2 = .042.
With all three of the executive measures, significantly higher scores, higher executive challenges, were observed in the Compulsive Shopping group compared to the Non-Compulsive Shopping group. The final mediation analyses can be seen in . Initial analyses revealed significant associations between the Group and the two outcome variables; Group-DEX-R, rpb = .252, p < .001; Group- ADEXI-WM, rpb = .184, p = .008.
Figure 1. The contribution of ADEXI-Inhibitory Control as a mediator of the Group—DEX-R and the Group—ADEXI-Working Memory relationships. Note. The indirect effect, b, is standardized.
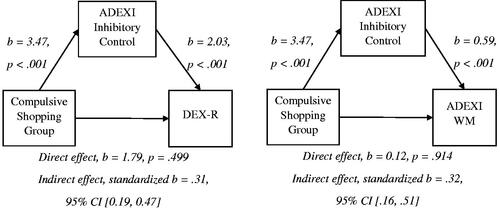
shows the standardized effects associated with ADEXI-IC mediation on the Group—DEX-R, and Group—ADEXI-WM relationships. All of the reported beta values are standardized. In the Group—DEX-R analysis, the mediation effect of ADEXI-IC was highly significant, the direct effect Group—DEX-R was not significant. The standardized coefficients for covariates Gender, Age, Anxiety and Depression were −.027, −.153, .136, and .495 respectively. In the Group—ADEXI-WM analysis, the mediation effect of ADEXI-IC was highly significant, the direct effect Group—DEX-R was not significant. The standardized coefficients for covariates Gender, Age, Anxiety and Depression were .010, −.006, .111, and .166 respectively.
Discussion
Compulsive behaviors reflect impaired decision making in contexts where in addition to the benefits which may be gained from the activity itself there is the risk of negative consequences, compulsive shopping is one such behavior. Excessive purchasing requires decision making in such a risky context, there may pleasure in the action of purchasing new commodities, but this brings the risk of many negative consequences. The Brand et al. (Citation2019) and Schiebener and Brand (Citation2015) theoretical deconstruction of the decision-making processes in addictive behavior contexts highlights a crucial role for executive function, in the retrieval and organization of information from long term memory, the integration of this cognitive and emotional information takes place in working memory and inhibitory processes contribute to the decision-behavior phase of the process. Consequently, this study aimed to investigate executive functioning, generic, working memory and inhibitory with measures designed to reflect not only cognitive but emotional processes in ecological contexts, the DEX-R and the ADEXI measures.
The present study provides evidence that compulsive shopping is indeed characterized by an impairment in self-reported executive function; with all three executive measures, DEX-R, ADEXI-WM and ADEXI-IC, showing significant deficits in the High Compulsive Shopping group when compared with the Low Compulsive Shopping group. In the subsequent mediation analyses with the ADEXI-Inhibitory Control measure as the mediator, the findings suggested that a key element of the generic and working memory executive impairments is inhibitory control. This is consistent with a view that prefrontal processes act to maintain relevant goals, targets and planned activities in working memory whilst inhibiting inappropriate and impulsive influences from subcortical processes (Miyake & Friedman, Citation2012; Munakata et al., Citation2011) and is consistent with recent research on the relationship between inhibitory control and working memory (see Mashburn et al., Citation2020). Thus, when inhibitory control is impaired, (ultimately) inappropriate affective and cognitive responses to the environmental triggers which typically elicit shopping motivation will now drive the decision-behavior process (Brand et al., Citation2019).
The Brand et al. (Citation2019), Schiebener and Brand (Citation2015) and Miyake and Friedman (Citation2012) accounts of inhibitory control are not specific to a context of compulsive shopping. The Brand et al., model is an attempt to interpret and articulate the I-PACE model within a range of addictive behaviors, e.g., gambling, gaming, compulsive sexual behaviors etc. Hoarding could be viewed as the compulsive collection of items which the individual does not discard leading to a cluttered and at times hazardous living space (Heffernan et al., Citation2021). Heffernan et al. investigated the executive functioning of a sample of the general population who varied in their hoarding characteristics. The group with the highest hoarding tendencies showed impaired executive function on the DEX-R, and the ADEXI-Inhibitory Control measures, a pattern similar to the current High Compulsive Shopping group in the present study. An unreported mediation analysis in the Heffernan et al study with ADEXI-IC and hoarding group as the predictor variable and DEX-R revealed that there was a significant indirect contribution of the ADEXI-IC variable. Thus, inhibition as measured by the ADEXI-IC is important in both a compulsive shopping and a hoarding context. However, it should be noted that the compulsive shopping and hoarding individuals did differ in two respects. Working memory as measured by the ADEXI-WM was impaired in the compulsive shopping group in the present study but not in the excessive hoarding group. Secondly, whilst the ADEXI-IC mediation was significant in both shopping and hoarding contexts, its impact was greater in the current shopping context. The ADEXI-IC accounted for all of the compulsive shopping group differences in DEX-R and ADEXI-WM (see above) but did not in the hoarding group DEX-R difference. Therefore, there are indeed commonalities between the two compulsive behavior contexts, but also differences.
The use of the self-report executive measures can be seen as an advantage as it highlights an understanding of executive function within a more naturalistic and ecological context recruiting cognitive and emotional processes in the decision making underlying the behaviors (Toplak et al., Citation2013). However, the ADEXI measure does not allow a nuanced consideration of discrete inhibitory processes to executive behavior. The paper by Robbins and Clark (Citation2015) identified several forms of inhibition, e.g., the inhibition of impulsive behaviors as measured in the Go-No Go paradigm, and the requirement of inhibition of inhibitory responses after a response has been initiated, a stopping process. The ADEXI-IC items appear to be predominantly assessing inhibition in the context of impulse control, e.g., “I have a tendency to do things without first thinking about what could happen,” “I sometimes have difficulty refraining from smiling or laughing in situations where it is inappropriate,” and only one item appearing to reflect a failure in stopping “I sometimes have difficulty stopping an activity that I like.” Though given that the ADEXI-IC measure did reveal compulsive shopping group differences in the present study it suggests that these two inhibitory processes/contexts are not entirely independent.
Future research should examine a range of inhibitory processes, both task-based and self-report in individuals with compulsive shopping behavior to articulate in more detail the inhibitory process profile in this group. For example, laboratory measures of inhibitory control include the Spatial Stroop task and the Stop Signal task. The spatial Stroop task is a procedure where both relevant and irrelevant information is presented within the same stimulus. For example, where a participant is required to attend to the direction of an arrow (left/right) whilst ignoring its position (presented in the left field of vision, or right). The person is instructed to name the direction of the arrow, whilst ignoring its position. Those with good inhibitory control produce faster, more accurate responses. The Stop signal task is one in which the participant is asked to carry out a particular procedure as quickly as possible to a predetermined stimulus (e.g., a green light), the go trial, but to stop their response when a subsequently presented stop signal is displayed (e.g., a red light). Speed and accuracy on the go trials are measured and provide an indication of the effectiveness of your inhibitory control. Such measure have been used in previous research to compare performance across both self-reports and objective measures of inhibitory control (Enticott et al., Citation2006). A further limitation of the present study is its failure to measure “cognitive flexibility”—a core dimension of EF which allows one to switch effectively between tasks, future research should explore this in addition to WM and IC.
Although data on age and sex was gathered, the study did not record other key socio-demographic data such as race, economic status, geographical location or mental health status. It is possible that these factors can influence compulsive shopping (see e.g., Mueller et al., Citation2010), therefore future research should include key socio-demographic information to provide a fuller picture of how such factors impact upon compulsive shopping behavior and/or executive ability.
Finally, the fact that the participants were recruited through online advertising and word-of-mouth and therefore may not be as representative as those who had been recruited via community samples, for example, those who have been diagnosed with Compulsive Shopping Disorder, therefore future work may wish to include a clinical group. It would also be insightful to compare examine executive functions in online shopping “addicts” as well as compulsive shoppers, to compare whether there are executive deficits that are common to both types of behavioral conditions, including what role inhibitory control plays in both these conditions.
Conclusions
The findings from the current study suggest that compulsive shopping is characterized by impairment in self-reported executive function; with the High Compulsive Shopping group showing significant impairments in all three executive measures, the DEX-R, ADEXI-WM and ADEXI-IC, when compared with the Low Compulsive Shopping control group. A subsequent mediation analyses with the ADEXI-Inhibitory Control measure as the mediator, suggested inhibitory control was a key element of the generic and working memory executive impairments found in Compulsive Shopping. This may explain why compulsive shoppers continue with their dysfunctional shopping behavior despite its negative consequences (legal and financial problems, distress) due to their inability to cognitively regulate their emotional response to shopping/buying and control their urges to purchase unnecessary items. These findings provide further insight into the cognitive underpinnings of compulsive buying/shopping and could have implications for interventions in this area.
Our focus in this current paper is on the association of variability in shopping compulsion and in executive cognitive control. Whilst this has implications for treatment and intervention, we would refer readers to studies such as Hui et al. (Citation2021), del Campo et al. (Citation2013) where intervention and treatment of dopaminergic dysregulation has been explicitly considered and emphasized.
Ethical approval
Approval for this study was granted by the ethics committee at Northumbria University, UK. Informed consent was obtained from all participants.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
References
- Andreassen, C. S., Griffiths, M. D., Pallesen, S., Bilder, R. M., Torsheim, T., & Aboujaoude, E. (2015). The Bergen Shopping Addiction Scale: Reliability and validity of a brief screening test. Frontiers in Psychology, 6, 1374.
- Bani-Rshaid, A. M., & Alghraibeh, A. M. (2017). Relationship between compulsive buying and depressive symptoms among males and females. Journal of Obsessive-Compulsive and Related Disorders, 14, 47–50. https://doi.org/10.1016/j.jocrd.2017.05.004
- Black, D. W. (2007). Compulsive buying disorder: A review of the evidence. CNS Spectrums, 12(2), 124–132.
- Black, D. W. (2010). Compulsive buying disorders. In E. Aboujaoude & L. Koran (Eds.), Textbook of impulse control disorders (pp. 5–22). Cambridge University Press.
- Black, D. W., Monahan, P., & Gabel, J. (1997). Fluvoxamine in the treatment of compulsive buying. The Journal of Clinical Psychiatry, 58(4), 159–163. https://doi.org/10.4088/jcp.v58n0404
- Black, D. W., Repertinger, S., Gaffney, G. R., & Gabel, J. (1998). Family history and psychiatric comorbidity in persons with compulsive buying: preliminary findings. The American Journal of Psychiatry, 155(7), 960–963. https://doi.org/10.1176/ajp.155.7.960
- Brand, M., Wegmann, E., Stark, R., Müller, A., Wölfling, K., Robbins, T. W., & Potenza, M. N. (2019). The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: Update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neuroscience and Biobehavioral Reviews, 104, 1–10. https://doi.org/10.1016/j.neubiorev.2019.06.032
- Brook, J. S., Zhang, C., Brook, D. W., & Leukefeld, C. G. (2015). Compulsive buying: Earlier illicit drug use, impulse buying, depression, and adult ADHD symptoms. Psychiatry Research, 228(3), 312–317.
- Christenson, G. A., Faber, R. J., de Zwaan, M., Raymond, N. C., Specker, S. M., Ekern, M. D., Mackenzie, T. B., Crosby, R. D., Crow, S. J., & Eckert, E. D. (1994). Compulsive buying: descriptive characteristics and psychiatric comorbidity. The Journal of Clinical Psychiatry, 55(1), 5–11.
- Dell’Osso, B., Allen, A., Altamura, A. C., Buoli, M., & Hollander, E. (2008). Impulsive-compulsive buying disorder: Clinical overview. Australian & New Zealand Journal of Psychiatry, 42(4), 259–266. https://doi.org/10.1080/00048670701881561
- D’Esposito, M., & Postle, B. R. (2015). The cognitive neuroscience of working memory. Annual Review of Psychology, 66, 115–142.
- del Campo, N., Fryer, T. D., Hong, Y. T., Smith, R., Brichard, L., Acosta-Cabronero, J., Chamberlain, S. R., Tait, R., Izquierdo, D., Regenthal, R., Dowson, J., Suckling, J., Baron, J.-C., Aigbirhio, F. I., Robbins, T. W., Sahakian, B. J., & Müller, U. (2013). A positron emission tomography study of nigro-striatal dopaminergic mechanisms underlying attention: Implications for ADHD and its treatment. Brain : A Journal of Neurology, 136(Pt 11), 3252–3270.
- Dittmar, H. (2004). Understanding and diagnosing compulsive buying. In R. Coombs (Ed.), Addictive disorders: A practical handbook (pp 411–450). Wiley.
- Enticott, P. G., Ogloff, J. R., & Bradshaw, J. L. (2006). Associations between laboratory measures of executive inhibitory control and self-reported impulsivity. Personality and Individual Differences, 41(2), 285–294. https://doi.org/10.1016/j.paid.2006.01.011
- Gallagher, C. E., Watt, M. C., Weaver, A. D., & Murphy, K. A. (2017). “I fear, therefore, I shop!” exploring anxiety sensitivity in relation to compulsive buying. Personality and Individual Differences, 104, 37–42. https://doi.org/10.1016/j.paid.2016.07.023
- Harnish, R. J., Gump, J. T., Bridges, K. R., Slack, F. J., & Rottschaefer, K. M. (2019). Compulsive buying: The impact of attitudes toward body image, eating disorders, and physical appearance investment. Psychological Reports, 122(5), 1632–1650.
- Hui, Q., Yao, C., & You, X. (2021). The mechanism of executive dysfunction in depressive symptoms: the role of emotion regulation strategies. Current Psychology. https://doi.org/10.1007/s12144-021-01528-7
- Heffernan, T., Hamilton, C., & Neave, N. (2021). Self-reported memory and executive function in adult non-clinical hoarders. Applied Neuropsychology: Adult. https://doi.org/10.1080/23279095.2021.1917578
- Hollander, E., & Allen, A. (2006). Is compulsive buying a real disorder, and is it really compulsive? The American Journal of Psychiatry, 163(10), 1670–1672. https://doi.org/10.1176/ajp.2006.163.10.1670
- Holst, Y., & Thorell, L. B. (2018). Adult executive functioning inventory (ADEXI): Validity, reliability, and relations to ADHD. International Journal of Methods in Psychiatric Research, 27(1), e1567. https://doi.org/10.1002/mpr.1567
- Jung, J. (2017). Impact of motives on impulsivity and compulsivity in compulsive buying behavior. Social Behavior and Personality: An International Journal, 45(5), 705–718. https://doi.org/10.2224/sbp.5885
- Koran, L. M., Faber, R. J., Aboujaoude, E., Large, M. D., & Serpe, R. T. (2006). Estimated prevalence of compulsive buying in the United States. American Journal of Psychiatry, 163(10), 1806–1812. https://doi.org/10.1176/ajp.2006.163.10.1806
- Lindheimer, N., Nicolai, J., & Moshagen, M. (2020). General rather than specific: Cognitive deficits in suppressing task irrelevant stimuli are associated with buying-shopping disorder. Plos One, 15(8), e0237093. https://doi.org/10.1371/journal.pone.0237093
- Maraz, A., Griffiths, M. D., & Demetrovics, Z. (2016). The prevalence of compulsive buying: A meta‐analysis. Addiction (Abingdon, England), 111(3), 408–419. https://doi.org/10.1111/add.13223
- Mashburn, C. A., Tsukahara, J. S., & Engle, R. W. (2020). Individual differences in attention control. In R. H. Logie, V. Camos, & N. Cowan (Eds.), Working memory: The state of the science. Oxford University Press.
- McElroy, S., Keck, P. E., Jr., Pope, H. G., Jr., Smith, J. M. R., & Strakowski, S. M. (1994). Compulsive buying: A report of 20 cases. The Journal of Clinical Psychiatry, 55(6), 242–248.
- Miltenberger, R. G., Redlin, J., Crosby, R., Stickney, M., Mitchell, J., Wonderlich, S., Faber, R., & Smyth, J. (2003). Direct and retrospective assessment of factors contributing to compulsive buying. Journal of Behavior Therapy and Experimental Psychiatry, 34(1), 1–9. https://doi.org/10.1016/S0005-7916(03)00002-8
- Miyake, A., & Friedman, N. P. (2012). The nature and organization of individual differences in executive functions: Four general conclusions. Current Directions in Psychological Science, 21(1), 8–14.
- Mueller, A., Mühlhans, B., Silbermann, A., Müller, U., Mertens, C., Horbach, T., Mitchell, J. E., & de Zwaan, M. (2009). Compulsive buying and psychiatric comorbidity. Psychotherapie, Psychosomatik, medizinische Psychologie, 59(8), 291–299.
- Mueller, A., Mitchell, J. E., Crosby, R. D., Gefeller, O., Faber, R. J., Martin, A., Bleich, S., Glaesmer, H., Exner, C., & de Zwaan, M. (2010). Estimated prevalence of compulsive buying in Germany and its association with sociodemographic characteristics and depressive symptoms. Psychiatry Research, 180(2–3), 137–142.
- Munakata, Y., Herd, S. A., Chatham, C. H., Depue, B. E., Banich, M. T., & O’Reilly, R. C. (2011). A unified framework for inhibitory control. Trends in Cognitive Sciences, 15(10), 453–459.
- Robbins, T. W., & Clark, L. (2015). Behavioral addictions. Current Opinion in Neurobiology, 30, 66–72.
- Schiebener, J., & Brand, M. (2015). Decision making under objective risk conditions–a review of cognitive and emotional correlates, strategies, feedback processing, and external influences. Neuropsychology Review, 25(2), 171–198.
- Schlosser, S., Black, D. W., Repertinger, S., & Freet, B. A. (1994). Compulsive buying: Demography, phenomenology, and comorbidity in 46 subjects. General Hospital Psychiatry, 6, 205–212.
- Simblett, S. K., Ring, H., & Bateman, A. (2017). The Dysexecutive Questionnaire Revised (DEX-R): An extended measure of everyday dysexecutive problems after acquired brain injury. Neuropsychological Rehabilitation, 27(8), 1124–1141.
- Snaith, R. P., & Zigmund, A. S. (1994). The hospital anxiety and depression scale. NFER-Nelson Publishing Company Ltd.
- Thorell, L. B., & Nyberg, L. (2008). The Childhood Executive Functioning Inventory (CHEXI): A new rating instrument for parents and teachers. Developmental Neuropsychology, 33(4), 536–552.
- Toplak, M. E., West, R. F., & Stanovich, K. E. (2013). Practitioner review: Do performance‐based measures and ratings of executive function assess the same construct? Journal of Child Psychology and Psychiatry, and Allied Disciplines, 54(2), 131–143.
- Trotzke, P., Starcke, K., Pedersen, A., & Brand, M. (2021). Dorsal and ventral striatum activity in individuals with buying‐shopping disorder during cue‐exposure: A functional magnetic resonance imaging study. Addiction Biology, 26(6), e13073. https://doi.org/10.1111/adb.13073
- Tyagi, P., & Shyam, R. (2019). Shopaholism from a psychological perspective. International Journal of Social Sciences Review, 7, 1379–1381.
- Unsalver, B. O., Koc, S., & Evrensel, A. (2018). A study of compulsive buying disorder comorbidity in psychiatric outpatients attending a foundation university outpatient clinic. Medicine, 7(4), 861–866.
- Wegmann, E., Müller, S. M., Ostendorf, S., & Brand, M. (2018). Highlighting Internet-communication disorder as further Internet-use disorder when considering neuroimaging studies. Current Behavioral Neuroscience Reports, 5(4), 295–301. https://doi.org/10.1007/s40473-018-0164-7
- Yan, W. S., Chen, R. T., Liu, M. M., & Zheng, D. H. (2021). Monetary reward discounting, inhibitory control, and trait impulsivity in young adults with internet gaming disorder and nicotine dependence. Frontiers in Psychiatry, 12, 28. https://doi.org/10.3389/fpsyt.2021.628933