
Abstract
PTSD symptomatology is known to be associated with executive dysfunction. Inhibitory control is a core component of executive functioning, and inhibitory skills are essential both for adequate functioning in everyday life and important in situations following trauma. The aim of the present study was to examine the relationship between trauma exposure, inhibitory control and PTSD symptomatology in adolescent survivors of the terror attack at Utøya, Norway on the 22nd of July, 2011. In this cross-sectional case-control study, 20 trauma exposed adolescents and 20 healthy controls matched in age and gender were compared on a neuropsychological test of cognitive inhibition (Color-Word Interference Test) and a self-report measure of inhibition ability (BRIEF-A). Our analyses revealed that the trauma exposed group differed significantly on the self-reported measure of inhibitory control compared to the control group, but there were no differences between groups on the objective measures of cognitive inhibition. Follow-up analyses with subgroups in the trauma exposed group based on PTSD symptomatology (PTSD + and PTSD-) and the control group revealed that the PTSD- group showed significantly better results than both the PTSD + and the control group on the measures of inhibitory control. Moreover, the follow-up analyses showed that the PTSD + group showed significantly poorer results from the other two groups on the measures of inhibitory control and self-reported inhibition. We conclude that impaired inhibitory control, measured both objectively and by self-reported questionnaire, is related to PTSD symptomatology. Findings suggest that inhibitory dysfunctions may be a vulnerability factor for the development of PTSD symptomatology in trauma exposed adolescents, and thus it seems that the ability to exhibit inhibitory control could be a possible resilience factor to prevent the development of PTSD symptoms.
On July 22nd, 2011, two major terror attacks were executed in Norway by the same person. A bomb explosion in the government district in central Oslo that killed eight people and severely injured nine, was followed by a brutal massacre at Utøya Island, killing 69 innocent people in total, 66 were physically injured. These terror attacks represent the worst violent acts committed in Norway during peacetime. The terror attacks in Norway on this day left an entire nation in fear and grief. In addition to those killed or physically injured, many were affected as they fled for life, witnessed the killings, lost their friends, were family members, volunteers, or rescue workers. At the time of the attack, the Norwegian Labor Party’s youth organization hosted their annual summer camp at Utøya. Five hundred-and-sixty-four people were on the island when the perpetrator arrived, most of them politically active adolescents and youth (Dyb et al., Citation2014). The perpetrator moved around the island while shooting and killing everyone in sight, until the police arrested him roughly 90 minutes later. Most survivors were exposed to major psychological traumas through either direct shooting, witnessing the death of others, or through other traumatic experiences and there are reasons to believe that they still are affected by this tragedy (Glad et al., Citation2017)
Traumatic events and trauma symptomology
Over the lifetime, 70% of people are exposed to a traumatic experience (Iyadurai et al., Citation2019), such as accidents, terror, climate catastrophes, sexual violation or other situations that threaten one’s own life or that of others (Costanzi et al., Citation2021). Such emotionally negative events wield the power to pay frequent and unwanted revisits to the experiencer’s awareness (Herz et al., Citation2020). These intrusive memories i.e., involuntary, reiterating thoughts, are defined as a core symptom of post-traumatic stress disorder (PTSD) (American Psychiatric Association, Citation2013). American Psychiatric Association (Citation2013) other common symptoms are a generally lowered mood, deficient memory and concentration, lower sleep quality and self-destructive behavior (American Psychiatric Association, Citation2013).
However, not everyone who experiences a traumatic event will suffer from long-term post-traumatic stress symptoms (PTSS) or develop PTSD. Although most trauma survivors will suffer from intrusions, these tend to decline over the course of the first few months (Dougall et al., Citation1999; Ehlers, Citation2010). The high diversity in responses to trauma implies great individual differences in how people deal with dreadful memories in the aftermath of the traumatic event. Recent research considers inhibitory control as a main factor involved in the development of PTSD symptomology due to its importance in suppressing unwanted thoughts (Costanzi et al., Citation2021).
Inhibitory control
Inhibitory control is one of the core human executive functions (EFs) which further include planning, working memory, behavioral inhibition, cognitive flexibility, and problem solving (Li et al., Citation2019; Nyvold et al., Citation2022). Common examples of employing inhibitory control are stopping automatic or unwanted thoughts and actions as well as blocking out distracting information in line with internal goals (Kelder et al., Citation2018). Inhibitory control is therefore considered to constitute an important factor in protecting mental health by suppressing distressing thoughts or memories which may otherwise reach conscious awareness (Anderson & Levy, Citation2009; Gagnepain et al., Citation2014; Mary et al., Citation2020).
Inhibitory control is commonly subdivided into its functional concepts of response (or motor) control and cognitive inhibition (Nigg, Citation2017). While the latter one is usually referred to one’s ability of exerting control over thoughts and emotions as well as deliberate direct attention, response control is mostly used in the context of stopping the execution of an automatic motor response or behavior. This division contributes to the specific conceptualization of experimentally task related (e.g., Think/No Think vs Stop Signal task) or real-life situational requirements (e.g. stopping the reflex to catch a falling knife vs suppressing the hurtful memory of a prior argument). However, recent research has suggested the domain-general nature of inhibitory control (Apšvalka et al., Citation2022; Depue et al., Citation2016). These lines of research show not only that both response and cognitive inhibition are highly correlated in behavioral performance but also share same areas in the prefrontal cortex exhibiting domain general neural activity accounting for both response and thought inhibition (Apšvalka et al., Citation2022).
Yet, it still is up for future research to discover if this suggested domain-general nature holds especially for groups of patients suffering symptoms defined by specific inhibitory control deficits as for example evident in PTSD patients experiencing intrusions (i.e., control over thoughts).
Assessment of inhibitory control
Inhibitory control can be assessed with different neuropsychological test batteries and instruments. Among the most extensively applied paradigms is the so-called Stroop task (Nyvold et al., Citation2022; Stroop, Citation1935). The Stroop task follows a simple logic of causing cognitive interference by presenting colored words while the semantics of the word partly do not match its color (e.g., “red” written in blue). Since the participant is asked to state as fast as possible the word’s actual color, the automatic response of reading out the word must be inhibited. Thus, it is referred to as the “Stroop effect”, which occurs when the current processing of a target stimulus feature (i.e., the word’s colouring) interferes with the simultaneous processing of another attribute of the stimulus (i.e., the word’s meaning).
A more subjective approach to assess inhibitory control capacity is to ask for an individual’s self-perceived skills to for instance inhibit, resist, or not act on an impulse. Former research has not found correlations between subjective and objective measurements (Ott et al., Citation2016; Schmid & Hammar, Citation2021; Svendsen et al., Citation2012), which was suggested to be an issue of ecological validity. Laboratory tasks to assess inhibitory control might thus not always reflect the individually experienced deficiencies which become immanent in daily life (Toplak et al., Citation2013).
PTSD and inhibitory control
The association between impaired inhibitory control and PTSD has been shown both in the behavioral (e.g., motor control tasks) and cognitive domain (Rooij & Jovanovic, Citation2019). Commonly, trauma survivors try to employ a variety of avoidance strategies to prevent trauma related thoughts from reaching awareness when confronted with a potential retrieval cue triggering mnemonic reexperience (Catarino et al., Citation2015). Inhibitory control has therefore been suggested a critical component of PTSD development since the suppression of intrusions seems to largely depend on the successful recruitment of inhibitory control resources (Costanzi et al., Citation2021; Hulbert & Anderson, Citation2018). Two recent meta-analyses reported medium large overall effect sizes of impairments in trauma exposed children and adolescents compared to healthy controls for executive functions in general and inhibitory control in particular (Kelder et al., Citation2018; Nyvold et al., Citation2022). It is noteworthy that Nyvold and colleagues’ meta-analysis states that trauma-exposed children without trauma-related symptoms exhibited significantly better executive functions compared to the trauma-exposed group with PTSD. This finding implies that differences in executive functioning could constitute a susceptibility factor underlying the development of PTSD. However, it is important to note that in children and adolescents the brain areas mainly underlying inhibitory control capacities (i.e., the prefrontal cortex) are not yet fully matured (Ordaz et al., Citation2013). Studies investigating trauma-related symptoms and inhibitory control in specifically younger samples may thus be limited in their generalizability.
Inhibitory control and memory suppression
Inhibitory control might determine how successfully an individual suppresses unwanted thoughts (Anderson & Green, Citation2001). Difficulties in suppressing unwanted memories tested with a retrieval inhibition task and self-reported thought control have been previously associated with PTSD (Catarino et al., Citation2015; Küpper et al., Citation2014).
Stopping an unwanted memory from unfolding when triggered by an external cue is defined as retrieval suppression and leads to suppression induced forgetting which describes the lowered accessibility of a frequently successfully suppressed memory (Anderson & Hanslmayr, Citation2014). The capacity of retrieval suppression and subsequent adaptive forgetting processes have been widely connected to inhibitory control (Catarino et al., Citation2015; Gagnepain et al., Citation2014; Küpper et al., Citation2014). Findings also indicate a strong correlation between suppression induced forgetting and an individual’s self-perceived thought control ability (Küpper et al., Citation2014). Therefore, adaptive forgetting could be one underlying mechanism explaining the suggested relationship of inhibitory control and PTSD symptomology.
Nevertheless, not all studies managed to find an association between PTSD and inhibitory control. As Melinder et al. (Citation2015) report, a decreased ability to shift between tasks and avoidance symptoms in PTSD patients were correlated, but no association with inhibitory control was found. However, the authors further state that the test battery employed would solely account for behavioral but not the cognitive part of inhibitory control (Melinder et al., Citation2015), which could explain the lack of correlation. Accordingly, the employment of both the Stroop task and the self-rating (BRIEF) in the current study may be more suited to measure general inhibitory control and its potential sub-domains.
In summary, a large body of literature reports a link between impaired inhibitory control and PTSD symptoms, while trauma exposure without the development of trauma related symptoms seems not to be associated with inhibitory control deficits. One core question in trauma research is why some individuals seem to cope better with traumatic events while others are haunted by intrusions, developing debilitating symptoms. Could inhibitory control contribute to an individual’s lowered susceptibility to develop trauma related symptoms?
Inhibitory control as a resilience factor?
The prepotent link between inhibitory control and PTSD raises the possibility that inhibitory control constitutes a protective factor for mental health of trauma survivors (i.e., after trauma exposure) as well as a possible predisposing resilience factor preventing the development of none or less trauma related symptoms in the aftermath of a traumatic event (Bryant, Citation2019; Mary et al., Citation2020). In line with this, Mary’s and colleagues’ study (2020) showed that trauma exposed, symptom-free individuals exhibited successful inhibition of intrusive thoughts compared to trauma survivors diagnosed with PTSD. Further, the strong correlation found between self-reported thought control ability and suppression induced forgetting (Küpper et al., Citation2014) indicates that the ability to control unwanted thoughts is beneficial to forgetting undesired memories in the long-term. This may imply that inhibitory control directly impacts the ability to eliminate disturbing memories. Contemporary neuroscience models suggest adaptive forgetting to be an active cognitive modulation which helps to shape one’s individual memory landscape (Anderson & Huddleston, Citation2011). In line with this notion, studies report that healthy controls with better engagement (e.g., inhibitory control) of their memory control system experience fewer intrusions after having been exposed to emotionally negative film scenes (Streb et al., Citation2016). Accordingly, adaptive forgetting follows the suppression of undesired thoughts which seems to largely depend on an individual’s inhibitory control. Successfully exerting inhibitory control over intrusive memories could therefore be a resilience factor for managing core symptoms of PTSD.
Avoidance strategies
Theories of PTSD usually consider memory avoidance via thought suppression to promote the persistence of intrusions and is therefore considered unfavorable for patients suffering from PTSD (Bishop et al., Citation2018; Ehlers & Clark, Citation2000; Magee et al., Citation2012). However, if suppression via inhibitory control is successfully employed, this avoidance strategy may indeed contribute to better mental health through diminished intrusions (Anderson & Green, Citation2001; Benoit & Anderson, Citation2012; Gagnepain et al., Citation2014). Counteracting the core symptom of experiencing intrusions, inhibitory control would thus function as a protective factor of successful symptom management.
As suggested by Catarino et al. (Citation2015) it seems important to furthermore differentiate between forms of psychological avoidance, i.e., suppressing the memory or suppressing possible reminders. While the latter likely restricts the individual freedom in daily life and deprives one of the possibilities to effectively remodulate the trauma memory, successful inhibition via retrieval suppression has shown positive outcomes on adaptive forgetting (Anderson & Levy, Citation2009; Lin et al., Citation2021) and mental health in trauma survivors (Nørby, Citation2018).
A predisposing resilience factor?
These formerly mentioned findings indicate that individual inhibitory control render some individuals more and others less susceptible to suffer from PTSD symptoms in the aftermath of a traumatic event. Research on healthy individuals points toward inhibitory control as a preexisting resilience factor. Those with higher inhibitory control seem to experience less intrusions after a trauma analogue induction (Benoit & Anderson, Citation2012; Gagnepain et al., Citation2014).
Hulbert and Anderson (Citation2018) suggest however that a better inhibitory control capacity could also be an acquired skill following trauma. This claim is based on two studies with healthy college students, dividing the sample into groups of high or low/no traumatic life experiences. Evidently, the group having experienced more prior traumatic events showed better overall inhibitory control and specifically memory suppression capacity than the matched controls with less or no trauma experience (Hulbert & Anderson, Citation2018). These findings indicate trainability of memory inhibition which could have remarkable implications for clinical applications. It does nevertheless not exclude that strong preexisting inhibitory control could still render individuals less susceptible to develop PTSD.
Inhibitory control as a risk factor?
On the opposite, poor inhibitory control leading to failed suppression attempts of unwanted memories and less adaptive forgetting processes appears to have detrimental effects on individuals’ mental well-being (Gagnepain et al., Citation2014; Legrand et al., Citation2020). In line with this notion individuals who exhibit deficient inhibitory control in a retrieval suppression task are more prone to suffer from persisting PTSD symptoms compared to those who recover following trauma (Catarino et al., Citation2015). The study of Streb et al. (Citation2016) found that people with lower retrieval suppression ability also reported higher distress for intrusive memories in the aftermath of watching a trauma-analogue movie, suggesitng they lacked the inhibitory control to suppress intrusive memories in the first place.
Together, these findings indicate that while stronger inhibitory control could function as a resilience factor, deficient inhibition is likely a risk factor for developing trauma-related symptoms. Since weaker inhibition would lead more likely to the persistence of intrusions, less successful memory suppression would as well result in lowered adaptive forgetting processes (Hulbert & Anderson, Citation2018; Mary et al., Citation2020). Since mental images or other sensory triggers of the trauma memory are reactively revisited without succeeding to push them away, failing inhibitory control attempts could actively undermine trauma survivors’ mental health.
The main aim of the present study
The current study aims to contribute to the ongoing discussion of whether inhibitory control constitutes a possible risk and/or resilience factor for the development of trauma related symptoms and PTSD within the context of real-life trauma exposure.
Research questions
If inhibitory control is a resilience factor, we expect to find higher subjective and objective scores in individuals who had been exposed to the Utøya attack, without developing PTSD symptoms, compared to both adolescents who developed PTSD symptoms as well as to healthy controls. The control group is considered to reflect the matching population which would therefore offer a “baseline” for inhibitory control scores while including most likely both individuals with norm deviant high and low scores, averaging out the extremes. Therefore, the “resilient” trauma survivors without PTSD symptomatology would be expected to exhibit increased inhibitory control compared to baseline. We hypothesize that if inhibitory control is a resilience factor, this capacity will be measured higher for trauma-exposed individuals without symptoms (PTSD-) compared to both baseline (control group) and trauma-exposed individuals with symptoms (PTSD+).
Further, following previous literature which is suggesting deficient inhibitory control to be a risk factor for the development of PTSD, we hypothesize that individuals that developed symptoms (PTSD+) would show lower inhibitory control compared to both control group and symptom free trauma survivors (PTSD-).
In order to assess inhibitory control, we chose to apply both an objective measure based on the Stroop paradigm and a subjective measure based on a self-reported questionnaire.
Methods
Participants
The sample consisted of 20 survivors of the Utøya terror attack and 20 control participants. Participants in the two groups were matched by age, gender, and level of education. There was a total of 14 males and 26 females in the sample. They were between the ages of 17–24, with a total mean age of 19.98 (SD = 1.51; Males: M = 20, SD = 1.88; Females: M = 19.96, SD = 1.31). All participants were either employed or in education.
The trauma exposed group
Written invitations were sent out to 45 Utøya survivors between the ages of 16–25 in two Norwegian counties (Hordaland and Rogaland). The ethical approval was valid for these two counties only. Invitations were sent through the Resource center for Violence, Traumatic Stress and Suicide prevention region West (RVTS West) and contained information about the study and the tests. Participants who were interested answered by returning a signed consent form. Participants were excluded if they had a history of endocrinological, psychiatric or neurologic illness prior to the Utøya attack, previous experience of head trauma leading to unconsciousness longer than 10 minutes, substance abuse, or current pregnancy. Travel expenses related to participation were covered and all subjects received an honorarium of 500 NOK.
After receiving an invitation, 29 of the 45 survivors handed in the consent form, resulting in a response rate of 64%. In addition to the 29 potential participants, two Utøya survivors learned about the study through the media and contacted the research team directly with requests to participate. Phone interviews of the 31 potential participants were carried out to ensure that the inclusion criteria were met (Utøya survivors of both genders, aged between 16–25).
The interviews led to exclusion of four survivors who were difficult to contact, or who did not meet the age inclusion criteria, whereas seven individuals did not turn up to the neuropsychological testing (seven males and four females). None of the remaining participants withdrew during testing.
The control group
The control sample was an age-, gender- and education-matched group consisting of politically active youths from other political youth organizations. Several approaches were used to recruit control subjects successively as participants from the trauma exposed group were included. Control participants were meticulously paired on an individual basis with the Utøya sample, first ensuring congruence in terms of age and gender, followed by aligning their educational attainment levels. Leaders of political youth organizations in Hordaland County were contacted for permission to visit the political party meetings and hand out invitations to participate in the study. After recruiting some participants, they took initiative of collecting contact information from other interested youths. In addition, adolescents known to be politically active were contacted directly and invited to participate. Prior to participation, all interested subjects were given information handouts describing the main purpose of the study along with consent forms for participation. Inclusion criteria were being aged between 16–25 years, being a member of a political party, and not involved in the Utøya massacre themselves or acquainted with any of the victims or survivors. Exclusion criteria were none psychiatric illness or diagnose, endocrine or neurological illness or substance dependence as determined by a short interview.
In addition to the exclusion criteria mentioned above, control subjects with ongoing or previous history of psychiatric illness (assessed through Mini International Neuropsychiatric Interview [MINI]; Sheehan et al., Citation2010) were screened out as this would affect the results. Fifty-one control subjects were recruited, whereof eight were immediately excluded based on their age. During the testing, further twenty-three participants were excluded from the data, due to psychiatric symptoms reported in the neuropsychiatric interview, ongoing substance abuse, or different inconveniences such as technical failure in a computer program.
Procedures
The data for this study was collected between 21 and 33 months after the terror attack. The participants in the trauma exposed group were a part of an extensive research project on long-term outcomes of the Norwegian terror attack. All the participants in the control group were included within the ∼ same time frame as the trauma exposed group. The investigation comprehends in this order of an fMRI scan (one hour duration) with a diurnal saliva cortisol sampling (pre-post test); a neuropsychiatric interview, placement of an actigraphy wearable, and neuropsychological tests. The current study concerns a subset of the neuropsychological assessments.
Diagnostic evaluation and procedure
Mini international neuropsychiatric interview (MINI)
Qualified health professionals administered the Norwegian version of MINI (MINI, 6.0.0;Sheehan et al., Citation2010) to all participants. MINI is a structured interview that detects psychiatric diagnoses according to diagnostic manuals (ICD-10 and DSM-IV). It is known to be applicable, with good results on measures of validity and reliability (Sheehan et al., Citation1998). MINI explores both ongoing and previous disorder based on criterion symptoms, as it differentiates between current symptoms and symptoms from an earlier time. When questions are answered confirmatory, follow-up questions determine the presence of sufficient symptoms to fulfill diagnostic criteria. The 27 MINI diagnoses assessed in the present study were clustered into six categories: eating disorder, abuse/addiction, mania, depression, anxiety, and suicidality. In addition, occurrence of clinical and subclinical posttraumatic stress disorder was examined to detect those who confirmed symptoms of PTSD but who did not fulfill the whole diagnostic criteria (post-traumatic stress symptoms, PTSS).
Subgroups in the exposed trauma group
The trauma exposed group was subdivided based on presence (+) or absence (-) of posttraumatic stress symptoms (PTSD+/-). The PTSD + group (n = 13) included participants who qualified for a PTSD diagnosis (n = 6) or reported a subclinical level of PTSD symptoms according to MINI, while the PTSD- group (n = 7) comprised those without reported symptoms.
Following Mary and colleagues’ procedure who did relatable research on survivors of the Paris terror attack in 2015 (Mary et al., Citation2020), we grouped trauma-exposed individuals with subthreshold PTSD (PTSS), (n = 7) and fully diagnosed PTSD (n = 6) into the PTSD + group. Subthreshold PTSD was defined by the occurrence of subclinical posttraumatic stress symptoms (Korte et al., Citation2016; Mishra et al., Citation2010) while not fulfilling the full diagnostic criteria for PTSD. If participants answered the MINI item H6 with “No” but three or more times “Yes” on H4 and H5, several subthreshold symptoms of PTSD were indicated to be present without fulfilling the diagnosis of full PTSD, i.e., subclinical level of PTSD. If participants answered H3 with “No” they were categorized into the PTSD- group, indicating no sub-clinically relevant symptoms.
The manifestation of PTSD symptomology even in its subclinical form has shown to be correlated with critical impairments in individuals’ daily psychological and social functioning (Zlotnick et al., Citation2002). Thus, subclinical PTSD is likely to bear important clinical implications (Mota et al., Citation2016), specifically considering the experience of intrusions (Pietrzak et al., Citation2012).
Neuropsychological assessment
The participants underwent a comprehensive neuropsychological assessment. The test battery included measures of IQ and other standardized and experimental tests and administrated by a trained test technician. In addition, self-report tests were employed. All testing was performed during regular working hours, administered in the same sequence to all participants, and took approximately four hours to complete. All applied assessments were employed in Norwegian language. The present study includes the objective and subjective tests measuring inhibitory control (see ).
Figure 1. PTSD + labels the subgroup of trauma-exposed individuals who developed post-traumatic stress symptoms in the aftermath of the Utøya terror attack. PTSD- labels the subgroup of trauma-exposed individuals who did not developed post-traumatic stress symptom. The idea for the figure’s design is partly inspired by Mary et al. (Citation2020).
Wechsler abbreviated scale of intelligence (WASI)
WASI is a short test that estimates verbal IQ, performance IQ and full scale IQ (Ryan et al., Citation2003). The WASI, Norwegian version (copyright Pearson assessment, 2007) generates a general intellectual function based on two subtests of verbal abilities and two subtests of performance. It is known to have sufficient internal consistency and test-retest reliability for the three IQs (Axelrod, Citation2002; Siqveland et al., Citation2014).
Measurements of inhibition and EF
Two measurements of inhibition were carried out: One objective measure as a standardized test from the Delis-Kaplan Executive Function System (D-KEFS; Delis et al., Citation2001) administered by a trained technician, and one subjective measure, the self-reported form The Behavior Rating Inventory of Executive Function–Adult version (BRIEF-A).
D-KEFS color-word interference test (CWIT)
D-KEFS CWIT is based on the Stroop (Citation1935) procedure. The test consists of four conditions: color naming (C), word reading (W), inhibition (CW), and inhibition/switching (IS), the Inhibition (CW) and Inhibition/switching (IS) measuring inhibitory control and inhibitory control/mental flexibility (Delis et al., Citation2001). Response time and number of errors and corrected errors were recorded for each condition. In order to control for the effect of processing speed on the inhibition and inhibition/switching conditions, interference scores were calculated, to subtract the response time in the C and W conditions from the response time on the CW and IS conditions as potential performance on these variables could distort the interpretation of results on the CW and IS conditions (for instance IS_score/CW_score = (C + W)/2))–CW/IS). This calculation derived two contrast scores; Interference CW and Interference IS, which are used in the main analyses. Norwegian translation was used (Harcourt Assessment, Citation2005).
BRIEF-a
The BRIEF-A is a standardized measure that assess perception of behavioral and emotional manifestations of executive dysfunction in everyday life for adults aged 18 to 90 years, which consists of a self-reported rating form. Although one participant in the control group was 17 years and 10 months at inclusion, the participant was assessed with BRIEF-A and included in the analysis. It is based on the original BRIEF and contains 75 items reflecting behaviors to be rated as often a problem (score 3), sometimes a problem (score 2), or never a problem (score 1) in everyday life during the last months in nine clinical scales and three validity scales. Higher scores reflect greater self-reported impairment in EF (Gioia et al., Citation2000). Norwegian version was administered (Nicholas & Solbakk, Citation2006). Only results from the inhibition subscale (BRIEF inhibition) will be used in the analyses.
Statistical analyses
All statistical analyses were conducted using the IBM SPSS, version 28. Statistical significance was defined as p < .05 for all results. All data are expressed as mean ± standard deviation (SD).
Preliminary analyses
The trauma exposed group and the control group were matched on the variables gender, age, and education. Independent t-tests were subsequently conducted to ensure that the matching on age and education level had been successful in eliminating differences between the groups. To further assure that the groups were sufficiently similar before conducting analyses, we compared the trauma exposed group and the control group on WASI total intelligence quotient (IQ). The same analysis was applied to inspect demographic variables and IQ in the two subgroups (PTSD + and PTSD-) of the trauma exposed participants.
Main analyses
Preliminary assumption testing for MANOVA was conducted by assessing for univariate and multivariate outliers, linearity, homogeneity of variance, covariance matrices, and multicollinearity. No serious violations were noted when testing the preliminary assumptions to execute univariate and multivariate analysis of variance.
MANOVA
One-way between groups MANOVAs were performed to investigate inhibitory control between the control group (baseline) and the trauma exposed group. The two groups were used as levels of the independent variable “group”, and the results on the tests CWIT and BRIEF inhibition were used as dependent variables. For the CWIT, an interference score for inhibition (CW) and inhibition/switching (IS), for each participant was calculated by subtracting the score in the color naming and word reading conditions from the score in the inhibition and the inhibition/switching conditions: Inhibition (CW-((C + W)/2), Inhibition/switching (IS-((C + W)/2).
The follow-up MANOVAs with post-hoc testing, using LSD significance difference were applied to investigate the original trauma exposed group divided into different subgroups based on PTSD symptom criteria and the control group (PTSD+, PTSD-) and control group (CG)), and with regard to PTSD symptomatology we divided the PTSD + group into subclinical PTSD (PTSS) and clinical PTSD (PTSD). Group was used as the independent variable, and the response on Interference CW and Interference IS and the BRIEF inhibition as the dependent variables.
Correlation analysis
Since the raw data scores were normally distributed, a Pearson correlation was carried out on the interference variables CW and IS of the CWIT, and the BRIEF inhibition in order to investigate the linear relationship between objective and subjective inhibition scores.
Logistic regression analysis
Direct logistic regression was performed to assess the impact of inhibition and inhibition-switching performance on the probability to distinguish between trauma exposed adolescents who had PTSD symptoms (PTSD+) from those without symptoms (PTSD-).
Results
Descriptive analyses
Results of the t-tests revealed that there were no significant differences between the trauma exposed group and the control group (see ) or the subgroups in the exposed group based on PTSD status (see ) on the variables age, and WASI IQ. The PTSD- group had significantly higher years of education compared to the PTSD + with approximately one year in mean difference.
Table 1. Means and Standard deviations on the variables age, years of education and WASI IQ for the trauma exposed group and the control group.
Table 2. Means and Standard deviations on the variables age, years of education and WASI IQ in the two trauma exposed groups (PTSD + and PTSD-).
Main analyses
A one-way between groups MANOVA was carried out, using group membership (i.e., trauma exposed, control) as the independent variable and interference score of inhibition (Interference CW), interference score of inhibition-switching (Interference IS) and BRIEF inhibition as dependent variables. There was a statistically significant difference between the groups on the dependent variables, F (3,36) = 2.510; Wilks’ Lambda = .74; partial eta squared = .173. When the results for the dependent variables were considered separately, there was a significant difference on the BRIEF inhibition. An investigation of the mean scores indicated that the trauma exposed group reported greater difficulties with inhibition than the control group (see ).
Table 3. Means and Standard deviations of CWIT conditions Interference score of CW and is, BRIEF inhibition, when using the trauma exposed group and control group (CG).
Correlation analyses showed that there was a strong positive correlation between performance on the Interference CW and Interference IS condition (r = .416, N = 40, p = .008). There were no significant correlations between BRIEF-A self-reported inhibition and performance on the Interference CW condition (r = −.043, N = 40, p = .791) or the Interference IS condition (r = .051, N = 40, p = .757).
Follow-up MANOVA with groups determined by PTSD status and control group
A MANOVA using PTSD status as the independent variable, interference score of inhibition (CW), interference score of inhibition-switching (IS) and BRIEF inhibition as dependent variables was carried out. There was a statistically significant difference main effect on the dependent variables, F (6 70) = 5.68; Wilks’ Lambda <.001; partial eta squared = .328. When the results for the dependent variables were considered separately, there was a significant difference between groups on the interference score of inhibition (CW), interference score of inhibition-switching (IS), and BRIEF inhibition. A multivariate analysis of variance with post hoc comparisons (LSD) was conducted to explore the differences in objective and subjective inhibition measures, between the PTSD+, PTSD- and the control group. Post hoc analysis showed that the PTSD- performed significantly better compared to the other groups on the measures of interference score of inhibition (CW). Further, the post hoc showed that the PTSD + group performed significantly poorer compared to the other two groups on the measures of the interference score of inhibition-switching (IS) and BRIEF inhibition self-report (see for results on MANOVA using groups determined by PTSD status and for CW and IS results). A multivariate analysis of variance with post hoc comparisons (LSD) was conducted to explore the differences in objective and subjective inhibition measures, between the participants with subclinical symptoms (PTSS) and clinical symptoms of PTSD in the PTSD + group and the PTSD- group. The analysis revealed no significant differences between the PTSS group and the PTSD group on any of the inhibition outcome measures. On BRIEF-A self-reported inhibition and on the Interference IS condition only the PTSD group was significantly different from the PTSD- group. On the Interference CW condition, the PTSD- group was significantly different from the two other groups (see ).
Figure 2. The Figure shows inhibitory control for the survivors, divided into two groups based on PTSD status, and the control group. The PTSD- group performed significantly better compared to the other groups on the measures of interference score of inhibition (CW), and the PTSD + group performed significantly poorer compared to the other two groups on the measures of the interference score of inhibition-switching (is). * The result is significant at the 0.05 level.
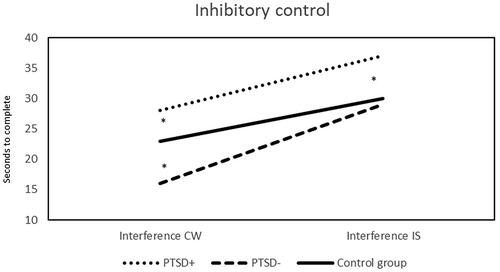
Table 4. Follow-up MANOVA with groups determined by PTSD status and control group.
Table 5. Multivariate analysis of variance with post hoc comparisons for the survivors, divided into three groups based on PTSD status.
Predicting PTSD symptomatology
The direct logistic regression model contained two independent variables (interference score of inhibition (CW), interference score of inhibition-switching (IS). The full model containing all predicters was statistically significant x2 (2, N = 20) = 9.03, p < .011, indicating that the model was able to distinguish between the exposed adolescents reporting PTSD and those who did not develop symptoms. The model, explained between 36.3% (Cox and Snell R square) and 50% (Negelkerke R Square) of the variance of PTSD symptom status, and correctly classified 85% of the cases. As shown in , only one of the independent variables made a unique statically significant contribution to the model (inhibition performance), recording an odds ratio of 1.17. This indicates that trauma exposed adolescents who need longer time to perform the inhibition test were twice as more likely to report PTSD symptoms, thus the model indicates a reasonable prediction estimate of group affiliation based on inhibitory control performance.
Table 6. Logistics regression predicting likelihood of classifying PTSD + or PTSD-.
Discussion
This study aimed to investigate the relationship between trauma exposure, inhibitory control, and the development of PTSD in survivors of the Utøya terror attack in 2011. Inhibitory control was measured both subjectively with a self-rating questionnaire and objectively with a Stroop task requiring cognitive interference handling as well as task switching ability.
Of the same population of trauma-survivors, not all individuals developed PTSD. Thirteen out of twenty trauma exposed individuals who participated in our study developed full or subclinical PTSD which is in line with previous studies showing that 60–62% of the terror attack survivors at Utøya (Bugge et al., Citation2015) were diagnosed with partial or full PTSD.
The trauma-exposed participants expressed lower perceived inhibitory control compared to the matched control group on the subjective measure, but there was no difference between the groups on the objective measures. However, we found significantly higher inhibitory control within the trauma-exposed subgroup who did not suffer from post-traumatic stress symptoms (PTSD-) compared to both the control group and the trauma-exposed group with PTSD (PTSD+). Opposite, the PTSD + group showed diminished inhibitory control capacity compared to both the control and the PTSD- group. The same pattern was evident for self-reported inhibition, showing that the PTSD + group reports significant more inhibition symptoms compared to the two other groups. Thus, our hypotheses were supported with major indications pointing toward inhibitory control as both a possible resilience and risk factor for the development of trauma related symptoms in the aftermath of a real-life trauma. Furthermore, inhibitory control score was shown to be a highly accurate predictor of determining subgroup belongingness.
By following Mary and colleagues’ procedure of grouping survivors into trauma-exposed individuals with subthreshold PTSD (PTSS) and fully diagnosed PTSD into one PTSD + group, we might have missed important clinical differences regarding symptom load. Thus, we conducted a follow up analysis comparing the two clinical groups, despite low power and high variance. Interestingly, the two clinical symptom groups did not differ on any outcome measures, however one might expect in larger samples that there is an interaction between symptom load and cognitive inhibitory control.
These findings are in line with previous research stating a systematic relationship between trauma symptomology and inhibitory control (Nyvold et al., Citation2022; Rooij & Jovanovic, Citation2019). However, further prospective study designs with larger N including different populations are needed to analyze the potentially predisposing and causal influence which inhibitory control may exert on PTSD. Therefore, experimental, and longitudinal designs with full control over baseline inhibitory control (pre-traumatic experience) and their possible development are necessary to conduct.
Inhibitory control as a resilience factor?
As hypothesized, trauma survivors with no PTSD symptoms displayed higher objectively measured inhibitory control compared to both the control and the PTSD + group. It is noteworthy that we found that the control group expressed significantly worse inhibitory control compared to the PTSD- group. Thus, it is conceivable that trauma exposure “separated” individuals with high and low inhibitory control into a more (PTSD-) and less resilient (PTSD+) group. The present results suggest inhibitory control as a resilience factor possibly protecting from the development of PTSD. It is assumable that our control group consists of individuals exhibiting a natural variability of inhibitory control.
We can however only speculate if the PTSD- group benefited from initially high inhibitory control thus protecting them from developing PTSD symptoms, or if their inhibitory control was increased after and maybe even along the trauma exposure. Both suggestions are hitherto derived from prior research (Hulbert & Anderson, Citation2018; Samuelson et al., Citation2020).
Apart from not being able to assess individuals’ pre-trauma inhibitory control we did not consider for instance social support from participants’ networks or their inter-individually differing experience of the actual traumatic event. In addition, the PTSD- group had significantly more years of education, albeit only one year. These factors could–among others –possibly have mediating or moderating effects on individuals’ inhibitory control and thus influenced symptom pressure.
Inhibitory control as a risk factor?
Not surprisingly, our findings show that the PTSD + group exhibited diminished inhibitory control which is in line with a large body of literature reporting a general deficit of inhibitory control in PTSD populations (Costanzi et al., Citation2021; DeGutis et al., Citation2015; Vasterling et al., Citation1998). Since the PTSD + group displays significantly lower inhibitory control compared to the PTSD- group and the control group, we conclude that the deviation from average is reasonable.
On the one hand, we suggest that inhibition control deficit might have led to higher susceptibility of developing PTSD symptoms after the terror attack. Though the association between lowered inhibitory control and PTSD would imply that diminished inhibition capacity could be a possible risk factor, longitudinal studies with controlled trauma-mirroring manipulations would be necessary for confirmation. On the other hand, inhibitory control deficit could also be the consequence of trauma symptomology. Studies have pointed out that maladapted avoidance strategies applied to suppress unpleasant trauma reminders may have a detrimental effect on mental health through strengthening intrusive memories and thus worsening the symptomology overall (Mitchell et al., Citation2007; Wegner, Citation1994). Unsuccessful memory suppression attempts might therefore exacerbate PTSD symptoms, potentially mediated by a lack of inhibitory control capacity (Gagnepain et al., Citation2014; Küpper et al., Citation2014; Nørby, Citation2018).
Subjective and objective inhibitory control
Interestingly, we found an apparent discrepancy between subjective and objective scores for inhibitory control indicating that the total group of trauma survivors rated themselves lower than the controls on self-perceived inhibitory control while there was no such difference for the objective measures. However, when inspecting the mean post-hoc scores, it is evident that the PTSD + group reports increased subjective challenges in everyday life while the PTSD- group showed the same perceived inhibitory control capacity as the controls. Thus, PTSD + perceived themselves to have worse inhibitory control than both other groups (PTSD- and control group). That led to a meaningful difference between trauma exposed and control group on the subjective rating of inhibitory control. For the objective measures however, the PTSD- group showed an average on the inhibitory control score that equalized the scores in both the control and PTSD + group resulting in no noticeable differences between controls and trauma survivors. Therefore, what at the first glance seemed like a discrepancy between objective and subjective results is explained when considering the subgroup scores in more detail.
Avoidance strategies
Since memory suppression has been shown to be highly intertwined with inhibitory control (Anderson & Levy, Citation2009; Catarino et al., Citation2015), we assume that participants displaying higher inhibitory control also apply more successful avoidance strategies. These would hinder unwanted thoughts to fully intrude awareness and in turn leading to a lowered long-term accessibility of trauma related memories. A diminished inhibitory control could potentially have the opposite effect, paradoxically strengthening the unwanted memories by focusing cognitive resources through inefficient suppression attempts and preventing the occurrence of otherwise favorable adaptive forgetting processes (Anderson & Hanslmayr, Citation2014; Hulbert et al., Citation2016).
Thus, repeated vivid retrieval of the emotionally strong trauma memory becomes even more accessible, intruding more frequently an individual’s mind and promoting eventually lasting PTSD symptoms. However, to test these hypotheses future research should assess trauma survivors’ most frequently applied avoidance strategies in relation to individual symptom pressure.
Clinical implications
Our results imply a meaningful relationship between inhibitory control capacity and trauma related symptom development which is in accordance with previous research (Mary et al., Citation2020; Samuelson et al., Citation2020). Noteworthy, similar relationships have been observed for depressed patients (Schmid & Hammar, Citation2021), and therefore a variety of patients suffering mental disorders might benefit from strengthening their inhibitory control (Bradley et al., Citation2005; Loerinc et al., Citation2015; Anderson & Levy, Citation2009; Bryant et al., Citation2021; Reuveni et al., Citation2022).
Considering the possibly gap between the demands of classical inhibitory control tasks and real-life situations these methods should be designed with highest possible ecological validity. For PTSD patients that could mean to develop strategies how to successfully inhibit intrusive thoughts or deliberately lower the emotional intensity of associated memories when confronted with a possible trauma reminder in daily life.
Our results further indicate that individuals with lower inhibitory control might be more susceptible for developing PTSD. This is relevant in terms of risk group assessment and possibly individualized and intensified follow-up measures for trauma survivors who show heightened susceptibility. Targeted and novel interventions are much needed in the field to increase treatment perspectives for PTSD patients (Iyadurai et al., Citation2019). Already existing treatment methods working to improve patients’ cognitive functioning as for instance cognitive remediation (Kim et al., Citation2018) should specifically consider the importance of inhibitory control capacity and be adapted for the needs of an individual’s symptomology.
On a further note, this study separated participants into apparent categories (PTSD+, PTSD-) to facilitate the reporting of results. Instead of separating the groups by taking the strict definition of not/fully diagnosed PTSD, we included subthreshold PTSD symptomology, recognizing the possibly high burden by any trauma related symptom manifestation for the individual. We suggest, it might be most appropriate in clinical research and practice to adopt a dimensional perspective on PTSD, taking individual manifestations into account, even besides the mere (non-)occurrence of core symptoms.
Strengths and limitations
Although larger sample sizes would have increased statistical power in the subgroup analyses, the present sample represents a uniquely homogenous group exposed to a severe life-threatening trauma experience in young age. Despite the low sample size did prevent us to conduct robust analyses between individuals with fully diagnosed and subclinical PTSD, a comparison which–given a higher power–would have been potentially informative. However, analysis revealed no differences between clinical and subclinical participants in the PTSD + group on the outcome measures.
There are several considerations to be aware of in the recruitment process and during testing. To minimize the risk that the control group would differ substantially from the quite homogenous trauma exposed group, we carefully selected and matched individuals in age, gender and on various factors like their social and political interests, however the inclusion and matching of more specific data, such as ethnicity, race and sexual orientation might have strengthened generalizability even more. Additionally, we might consider a self-selection effect as it is expected that individuals who suffer from the most severe symptoms would probably have refrained from participating in the current study. However, one might expect that these individuals are also most likely displaying lower inhibitory control capacity. This is why we would assume the found effect of diminished inhibitory control in the PTSD + group to even be higher in the whole population of Utøya trauma-survivors.
The terror attack on Utøya was directed toward a summer camp mainly attended by adolescents. Naturally the results obtained in this sample can hardly be generalized to other populations. without considering the developmental trajectory of the prefrontal cortex. Since executive functions such as inhibitory control are tightly connected to the maturation of the frontal lobes (Ordaz et al., Citation2013) the baseline inhibitory control capacities observed in our sample might underestimate those of the general (adult) population.
Our prediction model categorizing individuals into the respective subgroups (PTSD +/-) based on their inhibition scores performed highly accurate. It is desirable, that for future clinical applications trauma research engage actively into developing good predictor models which involve a variety of possibly relevant and interacting factors to gain more insight into resilience and risk factors of PTSD development.
Considering inhibitory control, we applied both subjective and objective measures, aiming for a holistic and differentiated assessment. We employed a version of the well validated and frequently used Stroop task (Kelder et al., Citation2018; Stroop, Citation1935), which is a common neuropsychological measurement for inhibitory control. However, the addition of a task evaluating an individual’s memory suppression capacity would have probably given further insight into the specifically relevant ability to manage intrusive thoughts (Catarino et al., Citation2015; Küpper et al., Citation2014).
Finally, it is imperative to underscore that inhibitory control, while recognized as a significant component contributing to the comprehension of the intricate trajectory of trauma-related symptomology, represents merely one facet within this broader framework. Other critical elements, including personality traits, emotional response styles, and external resources such as social support, warrant careful consideration. These variables, despite their relevance, were not encompassed within the scope of the present study.
Conclusions
The results of our study indicate that inhibitory control measured both objectively and subjectively is associated with trauma related symptom development. Our findings indicate that diminished inhibitory control could render trauma exposed individuals more susceptible to develop symptoms. Another possibility is that symptom development leads to lower inhibitory control. On the other hand, higher inhibitory control capacity seems to serve as a possible resilience factor to not develop symptoms in the aftermath of trauma exposure. Despite the small sample size, this study potentially offers a significant contribution to psychological trauma research and can set a basis for future research in the area of social and emotional clinical neuropsychology. These results bear important clinical implications for considering inhibitory control in both risk group assessment and for the development of interventions for patients with a trauma history. Future endeavors should consider experimentally controlled and longitudinal study designs, aiming to shed light into the possibly causal role of an individual’s inhibitory control capacity as a risk and/or resilience factor in PTSD development.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- American Psychiatric Association, DSM-5 Task Force. (2013). Diagnostic and statistical manual of mental disorders: DSM-5™ (5th ed.). American Psychiatric Publishing, Inc. https://doi.org/10.1176/appi.books.9780890425596
- Anderson, M. C., & Green, C. (2001). Suppressing unwanted memories by executive control. Nature, 410(6826), 366–369. https://doi.org/10.1038/35066572
- Anderson, M. C., & Hanslmayr, S. (2014). Neural mechanisms of motivated forgetting. Trends in Cognitive Sciences, 18(6), 279–292. https://doi.org/10.1016/j.tics.2014.03.002
- Anderson, M. C., & Huddleston, E. (2011). True and false recovered memories. Nebraska Symposium on Motivation, 76, 53–120. https://doi.org/10.1007/978-1-4614-1195-6_3
- Anderson, M. C., & Levy, B. J. (2009). Suppressing unwanted memories. Current Directions in Psychological Science, 18(4), 189–194. https://doi.org/10.1111/j.1467-8721.2009.01634.x
- Apšvalka, D., Ferreira, C. S., Schmitz, T. W., Rowe, J. B., & Anderson, M. C. (2022). Dynamic targeting enables domain-general inhibitory control over action and thought by the prefrontal cortex. Nature Communications, 13(1), 274. https://doi.org/10.1038/s41467-021-27926-w
- Axelrod, B. N. (2002). Validity of the wechsler abbreviated scale of intelligence and other very short forms of estimating intellectual functioning. Assessment, 9(1), 17–23. https://doi.org/10.1177/1073191102009001003
- Benoit, R. G., & Anderson, M. C. (2012). Opposing mechanisms support the voluntary forgetting of unwanted memories. Neuron, 76(2), 450–460. https://doi.org/10.1016/j.neuron.2012.07.025
- Bishop, L. S., Ameral, V. E., & Reed, K. M. P. (2018). The impact of experiential avoidance and event centrality in trauma-related rumination and posttraumatic stress. Behavior Modification, 42(6), 815–837. https://doi.org/10.1177/0145445517747287
- Bradley, R., Greene, J., Russ, E., Dutra, L. & Westen, D. (2005). A Multidimensional Meta-Analysis of Psychotherapy for PTSD. American Journal of Psychiatry, 162(2), 214–227. https://doi.org/10.1176/appi.ajp.162.2.214
- Bryant, R. A. (2019). Post‐traumatic stress disorder: a state‐of‐the‐art review of evidence and challenges. World Psychiatry, 18(3), 259–269. https://doi.org/10.1002/wps.20656
- Bryant, R. A., Williamson, T., Erlinger, M., Felmingham, K. L., Malhi, G., Hinton, M., Williams, L. & Korgaonkar, M. S. (2021). Neural activity during response inhibition associated with improvement of dysphoric symptoms of PTSD after trauma-focused psychotherapy—an EEG-fMRI study. Translational Psychiatry, 11(1), 218.https://doi.org/10.1038/s41398-021-01340-8
- Bugge, I., Dyb, G., Stensland, S. Ø., Ekeberg, Ø., Wentzel-Larsen, T., & Diseth, T. H. (2015). Physical injury and posttraumatic stress reactions. A study of the survivors of the 2011 shooting massacre on Utøya Island, Norway. Journal of Psychosomatic Research, 79(5), 384–390. https://doi.org/10.1016/j.jpsychores.2015.09.005
- Catarino, A., Küpper, C. S., Werner-Seidler, A., Dalgleish, T., & Anderson, M. C. (2015). Failing to forget: Inhibitory-control deficits compromise memory suppression in posttraumatic stress disorder. Psychological Science, 26(5), 604–616. https://doi.org/10.1177/0956797615569889
- Costanzi, M., Cianfanelli, B., Santirocchi, A., Lasaponara, S., Spataro, P., Rossi-Arnaud, C., & Cestari, V. (2021). Forgetting unwanted memories: Active forgetting and implications for the development of psychological disorders. Journal of Personalized Medicine, 11(4), 241. https://doi.org/10.3390/jpm11040241
- DeGutis, J., Esterman, M., McCulloch, B., Rosenblatt, A., Milberg, W., & McGlinchey, R. (2015). Posttraumatic psychological symptoms are associated with reduced inhibitory control, not general executive dysfunction. Journal of the International Neuropsychological Society, 21(5), 342–352. https://doi.org/10.1017/s1355617715000235
- Delis, D. C., Kaplan, E., & Kramer, J. H. (2001). Delis-Kaplan Executive Function System (D–KEFS) [Database record]. APA PsycTests. https://doi.org/10.1037/t15082-000
- Depue, B. E., Orr, J. M., Smolker, H. R., Naaz, F., & Banich, M. T. (2016). The organization of right prefrontal networks reveals common mechanisms of inhibitory regulation across cognitive, emotional, and motor processes. Cerebral Cortex (New York, N.Y.: 1991), 26(4), 1634–1646. https://doi.org/10.1093/cercor/bhu324
- Dougall, A. L., Craig, K. J., & Baum, A. (1999). Assessment of characteristics of intrusive thoughts and their impact on distress among victims of traumatic events. Psychosomatic Medicine, 61(1), 38–48. https://doi.org/10.1097/00006842-199901000-00008
- Dyb, G., Jensen, T., Glad, K. A., Nygaard, E., & Thoresen, S. (2014). Early outreach to survivors of the shootings in Norway on the 22nd of July 2011. European Journal of Psychotraumatology, 5(1), 23523. https://doi.org/10.3402/ejpt.v5.23523
- Ehlers, A. (2010). Understanding and treating unwanted trauma memories in posttraumatic stress disorder. Zeitschrift Fur Psychologie, 218(2), 141–145. https://doi.org/10.1027/0044-3409/a000021
- Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4), 319–345. https://doi.org/10.1016/s0005-7967(99)00123-0
- Gagnepain, P., Henson, R. N., & Anderson, M. C. (2014). Suppressing unwanted memories reduces their unconscious influence via targeted cortical inhibition. Proceedings of the National Academy of Sciences of the United States of America, 111(13), E1310–9. https://doi.org/10.1073/pnas.1311468111
- Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2000). Behavior rating inventory of executive function. Child Neuropsychology, 6(3), 235–238. https://doi.org/10.1076/chin.6.3.235.3152
- Glad, K. A., Hafstad, G. S., Jensen, T. K., & Dyb, G. (2017). A longitudinal study of psychological distress and exposure to trauma reminders after terrorism. Psychological Trauma, 9(Suppl 1), 145–152. https://doi.org/10.1037/tra0000224
- Harcourt Assessment. (2005). Harcourt Assessment, Inc., U.S.A Norsk Copyright. Psykologförlaget AB.
- Herz, N., Bar-Haim, Y., Holmes, E. A., & Censor, N. (2020). Intrusive memories: A mechanistic signature for emotional memory persistence. Behaviour Research and Therapy, 135, 103752. https://doi.org/10.1016/j.brat.2020.103752
- Hulbert, J. C., & Anderson, M. C. (2018). What doesn’t kill you makes you stronger: Psychological trauma and its relationship to enhanced memory control. Journal of Experimental Psychology General, 147(12), 1931–1949. https://doi.org/10.1037/xge0000461
- Hulbert, J. C., Henson, R. N., & Anderson, M. C. (2016). Inducing amnesia through systemic suppression. Nature Communications, 7(1), 11003. https://doi.org/10.1038/ncomms11003
- Iyadurai, L., Visser, R. M., Lau-Zhu, A., Porcheret, K., Horsch, A., Holmes, E. A., & James, E. L. (2019). Intrusive memories of trauma: A target for research bridging cognitive science and its clinical application. Clinical Psychology Review, 69, 67–82. https://doi.org/10.1016/j.cpr.2018.08.005
- Kelder, R. O. d., Akker, A. L. V. d., Geurts, H. M., Lindauer, R. J. L., & Overbeek, G. (2018). Executive functions in trauma-exposed youth: a meta-analysis. European Journal of Psychotraumatology, 9(1), 1450595. https://doi.org/10.1080/20008198.2018.1450595
- Kim, E. J., Bahk, Y.-C., Oh, H., Lee, W.-H., Lee, J.-S., & Choi, K.-H. (2018). Current status of cognitive remediation for psychiatric disorders: A review. Frontiers in Psychiatry, 9, 461. https://doi.org/10.3389/fpsyt.2018.00461
- Korte, K. J., Allan, N. P., Gros, D. F., & Acierno, R. (2016). Differential treatment response trajectories in individuals with subclinical and clinical PTSD. Journal of Anxiety Disorders, 38, 95–101. https://doi.org/10.1016/j.janxdis.2016.01.006
- Küpper, C. S., Benoit, R. G., Dalgleish, T., & Anderson, M. C. (2014). Direct suppression as a mechanism for controlling unpleasant memories in daily life. Journal of Experimental Psychology. General, 143(4), 1443–1449. https://doi.org/10.1037/a0036518
- Legrand, N., Etard, O., Vandevelde, A., Pierre, M., Viader, F., Clochon, P., Doidy, F., Peschanski, D., Eustache, F. & Gagnepain, P. (2020). Long-term modulation of cardiac activity induced by inhibitory control over emotional memories. Scientific Reports, 10(1), 15008. https://doi.org/10.1038/s41598-020-71858-2
- Li, G., Wang, L., Cao, C., Fang, R., Cao, X., Chen, C., Elhai, J. D., & Hall, B. J. (2019). Posttraumatic stress disorder and executive dysfunction among children and adolescents: A latent profile analysis. International Journal of Clinical and Health Psychology : IJCHP, 19(3), 228–236. https://doi.org/10.1016/j.ijchp.2019.07.001
- Lin, X., Chen, D., Yao, Z., Anderson, M. C., & Hu, X. (2021). Observing the suppression of individual aversive memories from conscious awareness. BioRxiv, 2021.10.17.464746. https://doi.org/10.1101/2021.10.17.464746
- Loerinc, A. G., Meuret, A. E., Twohig, M. P., Rosenfield, D., Bluett, E. J. & Craske, M. G. (2015). Response rates for CBT for anxiety disorders: Need for standardized criteria. Clinical Psychology Review, 42, 72–82. https://doi.org/10.1016/j.cpr.2015.08.004
- Magee, J. C., Harden, K. P., & Teachman, B. A. (2012). Psychopathology and thought suppression: a quantitative review. Clinical Psychology Review, 32(3), 189–201. https://doi.org/10.1016/j.cpr.2012.01.001
- Mary, A., Dayan, J., Leone, G., Postel, C., Fraisse, F., Malle, C., Vallée, T., Klein-Peschanski, C., Viader, F., Sayette, V. d l., Peschanski, D., Eustache, F., & Gagnepain, P. (2020). Resilience after trauma: The role of memory suppression. Science (New York, N.Y.), 367(6479), eaay8477. https://doi.org/10.1126/science.aay8477
- Melinder, A., Augusti, E.-M., Matre, M., & Endestad, T. (2015). Associations between executive functions and long-term stress reactions after extreme trauma: a two-year follow-up of the utøya survivors. Psychological Trauma : theory, Research, Practice and Policy, 7(6), 583–590. https://doi.org/10.1037/tra0000048
- Mishra, S., Goebert, D., Char, E., Dukes, P., & Ahmed, I. (2010). Trauma exposure and symptoms of post-traumatic stress disorder in emergency medical services personnel in Hawaii. Emergency Medicine Journal, 27(9), 708–711. https://doi.org/10.1136/emj.2009.080622
- Mitchell, J. P., Heatherton, T. F., Kelley, W. M., Wyland, C. L., Wegner, D. M., & Macrae, C. N. (2007). Separating sustained from transient aspects of cognitive control during thought suppression. Psychological Science, 18(4), 292–297. https://doi.org/10.1111/j.1467-9280.2007.01891.x
- Mota, N. P., Tsai, J., Sareen, J., Marx, B. P., Wisco, B. E., Harpaz-Rotem, I., Southwick, S. M., Krystal, J. H., & Pietrzak, R. H. (2016). High burden of subthreshold DSM-5 post-traumatic stress disorder in U.S. military veterans. World Psychiatry, 15(2), 185–186. https://doi.org/10.1002/wps.20313
- Nicholas, J., & Solbakk, A. K. (2006). BRIEF-P norwegian manual supplement. Psychological Assessment Resources.
- Nigg, J. T. (2017). Annual Research Review: On the relations among self‐regulation, self‐control, executive functioning, effortful control, cognitive control, impulsivity, risk‐taking, and inhibition for developmental psychopathology. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 58(4), 361–383. https://doi.org/10.1111/jcpp.12675
- Nørby, S. (2018). Forgetting and emotion regulation in mental health, anxiety and depression. Memory (Hove, England), 26(3), 342–363. https://doi.org/10.1080/09658211.2017.1346130
- Nyvold, O., Nygaard, E., Augusti, E.-M., & Tamnes, C. K. (2022). Unity or diversity of executive functioning in children and adolescents with post-traumatic stress symptoms? A systematic review and meta-analysis. Child Neuropsychology, 28(3), 374–393. https://doi.org/10.1080/09297049.2021.1979950
- Ordaz, S. J., Foran, W., Velanova, K., & Luna, B. (2013). Longitudinal Growth Curves of Brain Function Underlying Inhibitory Control through Adolescence. The Journal of Neuroscience, 33(46), 18109–18124. https://doi.org/10.1523/jneurosci.1741-13.2013
- Ott, C. V., Bjertrup, A. J., Jensen, J. H., Ullum, H., Sjælland, R., Purdon, S. E., Vieta, E., Kessing, L. V., & Miskowiak, K. W. (2016). Screening for cognitive dysfunction in unipolar depression: Validation and evaluation of objective and subjective tools. Journal of Affective Disorders, 190, 607–615. https://doi.org/10.1016/j.jad.2015.10.059
- Pietrzak, R. H., Schechter, C. B., Bromet, E. J., Katz, C. L., Reissman, D. B., Ozbay, F., Sharma, V., Crane, M., Harrison, D., Herbert, R., Levin, S. M., Luft, B. J., Moline, J. M., Stellman, J. M., Udasin, I. G., Landrigan, P. J., & Southwick, S. M. (2012). The burden of full and subsyndromal posttraumatic stress disorder among police involved in the World Trade Center rescue and recovery effort. Journal of Psychiatric Research, 46(7), 835–842. https://doi.org/10.1016/j.jpsychires.2012.03.011
- Reuveni, I., Herz, N., Peri, T., Schreiber, S., Harpaz, Y., Geisser, R., Bonne, O. & Goldstein, A. (2022). Neural oscillations while remembering traumatic memories in post-traumatic stress disorder. Clinical Neurophysiology. https://doi.org/10.1016/j.clinph.2022.04.002
- Rooij, S. J. H. v., & Jovanovic, T. (2019). Impaired inhibition as an intermediate phenotype for PTSD risk and treatment response. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 89, 435–445. https://doi.org/10.1016/j.pnpbp.2018.10.014
- Ryan, J. J., Carruthers, C. A., Miller, L. J., Souheaver, G. T., Gontkovsky, S. T., & Zehr, M. D. (2003). Exploratory factor analysis of the wechsler abbreviated scale of intelligence (WASI) in adult standardization and clinical samples. Applied Neuropsychology, 10(4), 252–256. https://doi.org/10.1207/s15324826an1004_8
- Samuelson, K. W., Newman, J., Amara, D. A., Qian, M., Li, M., Schultebraucks, K., Purchia, E., Genfi, A., Laska, E., Siegel, C., Hammamieh, R., Gautam, A., Jett, M., & Marmar, C. R. (2020). Predeployment neurocognitive functioning predicts postdeployment posttraumatic stress in Army personnel. Neuropsychology, 34(3), 276–287. https://doi.org/10.1037/neu0000603
- Schmid, M., & Hammar, Å. (2021). First-episode patients report cognitive difficulties in executive functioning 1 year after initial episode of major depressive disorder. Frontiers in Psychiatry, 12, 667238. https://doi.org/10.3389/fpsyt.2021.667238
- Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., Hergueta, T., Baker, R., & Dunbar, G. C. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. The Journal of Clinical Psychiatry, 59(Suppl 20), 22–33.
- Sheehan, D. V., Sheehan, K. H., Shytle, R. D., Janavs, J., Bannon, Y., Rogers, J. E., Milo, K. M., Stock, S. L., & Wilkinson, B. (2010). Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). The Journal of Clinical Psychiatry, 71(3), 313–326. https://doi.org/10.4088/jcp.09m05305whi
- Siqveland, J., Dalsbø, T. K., Harboe, I., & Leiknes, K. A. (2014). Måleegenskaper ved den norske versjonen av wechsler abbreviated scale of intelligence (WASI). In Rapport fra Kunnskapssenteret nr 20-2014. Research overview (pp. 1890–1298). Available at www.fhi.no/en
- Streb, M., Mecklinger, A., Anderson, M. C., Lass-Hennemann, J., & Michael, T. (2016). Memory control ability modulates intrusive memories after analogue trauma. Journal of Affective Disorders, 192, 134–142. https://doi.org/10.1016/j.jad.2015.12.032
- Stroop, J. R. (1935). Studies of interference in serial verbal reactions. Journal of Experimental Psychology, 18(6), 643–662. https://doi.org/10.1037/h0054651
- Svendsen, A. M., Kessing, L. V., Munkholm, K., Vinberg, M., & Miskowiak, K. W. (2012). Is there an association between subjective and objective measures of cognitive function in patients with affective disorders? Nordic Journal of Psychiatry, 66(4), 248–253. https://doi.org/10.3109/08039488.2011.626870
- Toplak, M. E., West, R. F., & Stanovich, K. E. (2013). Practitioner review: Do performance‐based measures and ratings of executive function assess the same construct? Journal of Child Psychology and Psychiatry, and Allied Disciplines, 54(2), 131–143. https://doi.org/10.1111/jcpp.12001
- Vasterling, J. J., Brailey, K., Constans, J. I., & Sutker, P. B. (1998). Attention and memory dysfunction in posttraumatic stress disorder. Neuropsychology, 12(1), 125–133. https://doi.org/10.1037/0894-4105.12.1.125
- Wegner, D. M. (1994). Ironic processes of mental control. Psychological Review, 101(1), 34–52. https://doi.org/10.1037/0033-295X.101.1.34
- Zlotnick, C., Franklin, C. L., & Zimmerman, M. (2002). Does “subthreshold” posttraumatic stress disorder have any clinical relevance? Comprehensive Psychiatry, 43(6), 413–419. https://doi.org/10.1053/comp.2002.35900