
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Public financial management (PFM) theory suggests that improvements in the allocation, execution, and monitoring of public funds can result in improved sectoral outcomes, including in health. However, the existing literature on the relationship between PFM quality and health outcomes provides limited empirical documentation and insufficient explanation of the mechanics of that relationship. This paper contributes to the literature by estimating the correlation between PFM quality and health outcomes from a sample of sub-Saharan African countries over the period 2005–2018, using a pooled ordinary least squares (OLS) estimator. The analysis uses Public Expenditure and Financial Accountability (PEFA) scores as proxies for PFM quality. The findings indicate that countries with high-quality PFM tended to have the lowest maternal, under-five and noncommunicable diseases (NCDs) mortality. Among the standard PFM dimensions, the one associated with the higher correlation with maternal and under-five mortality was “predictability and control in budget execution.” Better PFM quality was significantly associated with a drop in maternal and under-five mortality in countries which allocated a higher proportion of their budget to the health sector. In countries allocating a lower proportion of their budget to health, the correlations between PFM quality and the three mortality indicators were not significant. The negative correlations between PFM quality and maternal and under-five mortality were significant only in countries with more effective governance. These findings support an emphasis on strengthening PFM as a means of improving health service provision and health outcomes.
Introduction
Does PFM Impact Health Outcomes?
There is an emerging consensus in the theoretical literature and among practitioners that the quality of a country’s public financial management (PFM) system plays a role in determining health service provision and thus in affecting health outcomes.Citation1–3 The theory holds that the quality of budget formulation, budget execution, and budget oversight impacts the quality and coverage of, and access to, a country’s health services.Citation4–8 The literature’s assumptions about how the principal PFM phases can affect health service provision and thus health outcomes, are as follows.
Budget Formulation
During budget formulation, policy makers determine where and how financial resources will be spent in the health sector. As these decisions have implications for downstream expenditure, including health services purchasing, they influence health outputs.Citation5,Citation6,Citation9 The alignment of the budget with sector priorities, and flexibility in budget structure, are key enablers for health spending that is effective and responsive to needs.Citation10
Budget Execution
The rules and processes for budget execution can either support or hinder service providers’ ability to deliver health services and to respond to emerging needs.Citation5,Citation11 The following measures can enable budget execution to better respond to service providers’ needs: (i) the budget is planned and structured in line with service-delivery needs; (ii) budget execution rules are sensitive to service providers’ needs; (iii) the budget is disbursed in full and in a timely manner, and is managed flexibly by service providers.
Budget Oversight
Budget oversight, consisting of financial reporting mechanisms and audits, provides information on expenditure. The way the budget is monitored and reported affects health service provision, e.g., through excessive administrative burdens for medical staff.Citation5,Citation12 In addition, timely and accurate information on expenditure and performance can help to enhance the next round of budget preparation and thus strengthen health service delivery and outcomes.
Empirical Testing of the Hypothesized Relationship Between PFM and Health Outcomes
Existing studies have explored and tested the relationship between PFM quality and health service delivery and/or health outcomes.Citation3–5,Citation13 Piatti and Schneider analyzed the relationship between PFM and health service delivery in Tanzania and Zambia.Citation5 The study highlighted several PFM-related bottlenecks that impact health service delivery including the lack of budgetary flexibility to provide additional resources, the misalignment between budgeting and planning, the fragmentation of funding sources, the rigidity in internal controls, and the accumulation of arrears resulting from insufficient budget allocation provision. Welham et al. used 78 observations to assess the statistical relationship between PFM, approximated by Public Expenditure and Financial Accountability (PEFA) average scores and health outcomes in low- and middle-income countries (LMICs).Citation3 They found that PFM quality was negatively correlated with infant and child mortality and positively correlated with life expectancy at birth. The authors acknowledge that their data and methodology allowed the estimation of correlation but not of causation, and suggest interpreting the results with caution. Piatti-Fünfkirchen and Smets analyzed 215 observations and PEFA scores from a sample of LMICs, finding that better PFM quality resulted in a decrease in child and maternal mortality, with a stronger effect in countries where health services were publicly financed.Citation4 Fritz et al found no relationship between PFM quality and health or education outcomes, although the limitations of available indicators may explain the absence of a relationship.Citation13
Framework and Objectives of This Paper
The relationship between PFM quality and health outcomes is likely to be significant in countries where public funding plays a major role in financing health services.Citation4,Citation9
Our analytical framework builds on existing studies of the statistical relationship between PFM quality and health outcomes, as summarized above, adding a health financing dimension to better examine whether and how financing affects the links between PFM and health.
As illustrated below (), the three common stages in the budget cycle (budget formulation, budget execution, and budget monitoring) have an impact on the three health-financing functions (how financing is raised and pooled in health, and how health services are purchased).Citation14
Figure 1. Analytical framework: linking PFM, health financing and health outcomes.
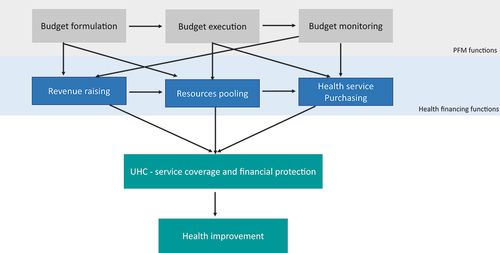
Budget formulation (or how the budget is developed, formed, and formulated) is likely to impact revenue-raising and pooling for health, by determining the required amount and the organization of compulsory, pre-paid health funding.
Budget execution and monitoring rules, which govern how public funding is spent, controlled, and accounted for, affect how health service providers receive funding and the extent to which they have flexibility in using and managing those funds.
The three PFM functions play a critical role in strengthening health financing, which is recognized to support progress toward the UHC goals and ultimately toward improved health outcomes.Citation15–19
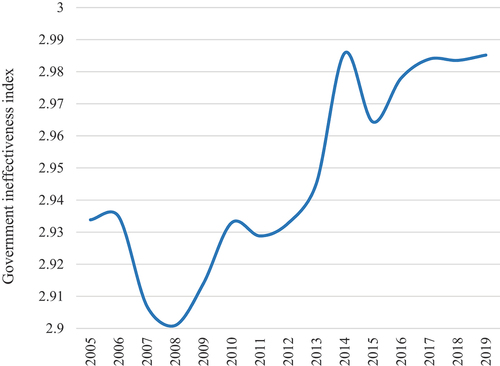
This paper aims to contribute to the literature by empirically assessing the statistical relationship between PFM quality and health outcomes, with a focus on LMICs in sub-Saharan Africa (SSA), which tend to have poorer outcomes in both PFM and health than in many other regions. The intent is to add to the existing literature, by building a case for accelerating investments in PFM systems. First, in addition to estimating the PFM relationship with maternal and child mortality as previous literature has assessed,Citation3,Citation4 this paper also focuses on the NCDs mortality rate. The latter is important, as SSA countries tend to experience a double burden from the gradual emergence of NCDs and the persistence of communicable diseases. Second, to complement the evidence provided by Welham et al and Piatti-Fünfkirchen and Smets,Citation3,Citation4 this paper assesses the extent to which budget prioritization for health, and institutional quality, play a role in the relationship between PFM quality and health outcomes. This question is critical as the average share of health in SSA countries’ budgets decreased between 2005 and 2019 from 7.3% to 6.6% (), with governance also worsening over the same period ().
Figure 2. Trend in budget prioritization for health.
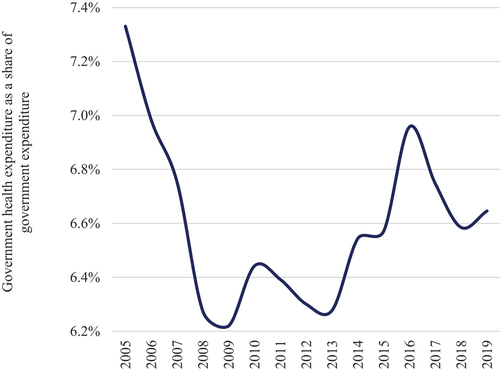
Figure 3. Trend in a key proxy for institutional quality.
Methods
This study estimates the statistical relationship between PFM quality and health outcomes, using data from 42 SSA countries spanning the period 2005 to 2018 (Appendix 1).Footnote1 The countries and time period were sampled according to the availability of Public Expenditure and Financial Accountability (PEFA) scores, an assessment framework that is widely used to assess the strengths and weaknesses of PFM.Citation20,Citation21 These scores are qualitative ratings that provide a snapshot of PFM performance at a specific point in time, using a methodology that can be replicated in subsequent assessments.
As our study’s panel data were strongly unbalanced, we follow the same methodological approach as Welham et al.Citation3 This consisted of using pooled ordinary least squares (OLS) as an estimator, covering between 29 and 94 observations to estimate the correlation between PFM quality and health indicators, controlled for a key variable. In the econometric model, the variables are expressed in logarithmic terms to estimate the elasticity of health outcomes against PFM and other determinants. The descriptive statistics and data sources are reported in Appendix 2. The econometric model is specified as follows:
Where:
: Health outcomes in the country «i»;
: PFM quality in the country «i»;
: the control variable;
: the idiosyncratic disturbance; and
; and
: the parameters to be estimated.
Dependent Variables
Three indicators are used: the maternal mortality ratio per 100,000 live births; the under-five mortality rate per 1,000 live births; and the NCDs mortality rate per 1,000 inhabitants.
Variables of Interest
PEFA ratings, on an alphabetical scale ranging from “A” to “D,” are used as a proxy for quality of PFM. Two assessment frameworks of PEFA ratings were developed in 2011 and 2016 by the PEFA Secretariat, the latter including more indicators than the former but having been the least used for country PFM assessment. The paper uses the 2011 assessment framework, since it provides more results available than the second.Citation20 Following the 2011 approach, PFM includes indicators grouped into the following seven standard dimensions:
Credibility of the budget: the extent to which the budget is realistic and is implemented as intended;
Comprehensiveness and transparency: the extent to which the budget and oversight of fiscal risk are comprehensive, and fiscal and budget information are accessible to the public;
Policy-based budgeting: the extent to which the budget is prepared with due regard to government policy;
Predictability and control in budget execution: the extent to which the budget is implemented in an orderly and predictable manner, and there are arrangements for control and stewardship in the use of public funds;
Accounting, recording, and reporting: the extent to which adequate records and information are produced, maintained, and disseminated for decision-making, control, and management purposes;
External scrutiny and audit: the extent to which arrangements for the scrutiny of public finances and follow-up by the government are operational;
Donor practices: The extent to which direct budget support is predictable, financial information is provided by donors for budgeting and reporting on project and program aid and external funding are managed in line with national procedures and rules.
We converted the PEFA alphabetical ratings into numerical values, as was done in previous studies, and following the PEFA Secretariat’s guidance for research.Citation22,Citation23 To focus our analysis on the government’s own capacity to better manage the public purse, the overall PEFA average score was calculated without including the “donor practices” dimension.
Control Variable
GDP per capita, regarded as a key determinant of health, is included in the model to control for all dimensions related to macroeconomic and socioeconomic conditions. As many drivers influence a country’s welfare, GDP per capita serves as a general control.Citation4
Other Variables
This study also assesses the differential correlation between PFM quality and health outcomes, based on a) “budget prioritization for health,” and b) public sector institutional quality.
Piatti-Fünfkirchen and Smets used public health spending as a share of GDP as a proxy for budget prioritization for health,Citation4 which instead provides an approximation of the weight of public spending for health in a country’s economy. To provide a more accurate proxy of budget prioritization for health, the paper uses the share of the health allocation within the overall budget.
The government effectiveness index (−2.5 [low] to 2.5 [high]) is used as a proxy for institutional quality. It captures perceptions of the quality of public services and the degree to which those services are independent from political pressures, the quality of policy formulation and implementation, and the credibility of the government’s commitment to such public policies. To transform the index into logarithmic form, this index was reversed using the formula: , where
and
represent the proxy indicator for institutional quality and its reverse, respectively. This reversed index was then used as a proxy for government ineffectiveness, assessing the extent to which a government with worsened credibility (in terms of follow-through on commitments) provides poor-quality public services and implements inadequate policies.
In the estimation of differential correlations between PFM quality and health outcomes, the health budget share and the government ineffectiveness index are not directly included in the model because of a potential multicollinearity bias resulting from their high negative correlation with PEFA scores and GDP per capita, respectively (Appendix 3). Instead, we first divided the sample into two subsamples based on the median value of health budget share and government ineffectiveness index. Then, in each subsample, we used the same model specified above to estimate the relation between PFM and mortality indicators.
Results
Descriptive Analysis
PEFA Score and Health Outcomes Distribution
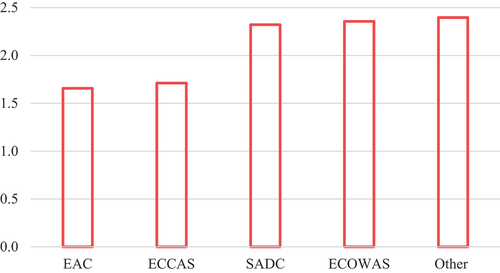
Comparing the overall PEFA score by sub-Saharan African subregion, the Economic Community of West African States (ECOWAS) scored the highest for PFM quality, followed by the Southern African Development Community (SADC), the Economic Community of Central African States (ECCAS), and the East African Community (EAC) ().
Figure 4. PEFA score distribution per sub-Saharan African subregion.
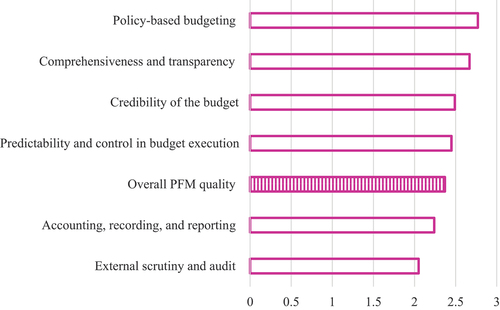
Among the individual PFM dimensions, scores were highest on average for “policy-based budgeting” and “comprehensiveness and transparency,” and lowest for “external scrutiny and audit” ().
Figure 5. PEFA score distribution per PFM dimension.
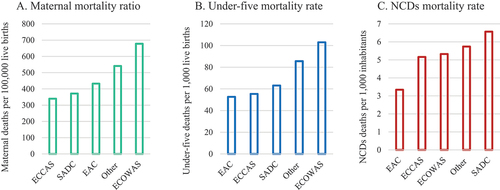
ECOWAS had the highest maternal and under-five mortality while ECCAS and EAC recorded the lowest maternal and under-five mortality, respectively. The NCDs mortality rate was highest in SADC and lowest in EAC ().
Figure 6. Key health outcomes distribution per sub-Saharan African subregion.
Statistical Relation Between PEFA and Health Outcomes
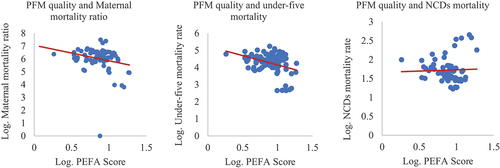
The analysis reveals a negative correlation between individual countries’ overall PEFA score, and maternal and under-five mortality respectively, with significant correlation coefficients estimated at 22.9% and 31.7%, respectively (). The correlation between the overall PEFA score and NCDs mortality rate is calculated at 3.6% but is not significant.
Figure 7. Scatterplots between overall PFM quality and health outcomes.
Econometric Analysis
Testing for the Statistical Relationship Between PFM Quality and Health Outcomes
The study’s results suggest that countries with higher PFM quality have the lowest maternal and under-five mortality and NCDs mortality rate. The overall PEFA score is associated with significant and negative coefficients (). A robustness check, consisting of additional controls, confirms the negative correlations between PFM quality and maternal and under-five mortality and the NCDs mortality rate (Appendix 4).
Table 1. Findings from the estimation of statistical relationship between PFM quality and health outcomes.
The assessment of the specific associations between PFM dimensions and health outcomes found that most of the PFM dimensions are negatively and significantly correlated to under-five mortality, except for “external scrutiny and audit.”
The dimensions which are negatively and significantly correlated to maternal mortality are: “comprehensiveness and transparency,” “predictability and control in budget execution,” and “donor practices.” The dimensions which are negatively and significantly correlated to NCDs mortality rate are: “accounting, recording and reporting” and “external scrutiny and audit.” Among the dimensions, “predictability and control in budget execution” is most significantly and negatively correlated to under-five and maternal mortality. reports the key findings from these estimations while the other key statistics resulting from these regressions are provided in Appendix 5.
Table 2. Findings from the estimation of statistical relationship between PFM dimensions and health outcomes.
Testing for the Statistical Relationship Between PFM Quality and Health Outcomes, Depending on Budget Prioritization for Health
The study found a significant and negative correlation between the overall PEFA score and maternal, under-five and NCDs mortality, only in countries which allocated a higher proportion of their budget to health ().
Table 3. Findings from the estimation of statistical relationship between PFM quality and health outcomes, depending on budget prioritization for health.
Testing for the Statistical Association Between PFM Quality and Health Outcomes Depending on Government Ineffectiveness
The findings suggest that the overall PEFA score is significantly and negatively correlated to maternal and under-five mortality in countries with the most effective governance while the correlation is not significant in countries with the most ineffective governance. The negative correlation between the overall PEFA score and the NCDs mortality rate is only significant in countries where governance is the most ineffective. This result is not conclusive and should be treated with caution ().
Table 4. Findings from the estimation of statistical relationship between PFM quality and health outcomes, depending on governance ineffectiveness.
Discussion
This study analyzed the statistical relationship between PFM quality and a set of health outcomes. We used PEFA scores as a proxy for PFM quality, with a focus on three indicators of health outcomes: maternal and under-five mortality and NCDs mortality rates. The study drew on 42 SSA countries covering the period 2005 to 2018, with 29 to 94 observations. Using pooled OLS estimations, we found that countries with high-quality PFM had the lowest maternal, under-five and NCDs mortality rates. Specifically, higher-quality PFM, combined with high-level political commitment backed by budget allocations, could contribute to more favorable health outcomes. This finding is important for policy makers, not least because it could justify the lengthy and complex reforms needed to improve the quality of PFM. Similarly, this finding confirms the importance of active involvement by other health stakeholders in supporting the strengthening of PFM in the region.Citation24
This study’s analysis by PFM dimension provides a helpful focus for policy makers. Of the seven PFM dimensions tested, “predictability and control in budget execution” had the greatest correlation with maternal and under-five mortality. In a region where health budget execution tends to be low generally—studies have reported execution levels of 60–80%—this analysis shows the importance of improving levels, effectiveness, and regularity of budget implementation as a direct contributor to better health outcomes.Citation11,Citation24 Governments should prioritize actions to understand the causes of, and identify solutions to, chronic under-execution of health budgets, as this could have a significant effect on health outcomes.
This study also showed that the negative correlations between PFM quality and maternal, under-five, and NCDs mortality were significant in countries which allocated a higher proportion of their budgets to health; this was not the case in countries where health budget prioritization was lower. This finding suggests that improvements in PFM quality need to be complemented by adequate budget allocations if they are to result in significant health benefits. This point has particular salience given that many sub-Saharan African LMICs have deprioritized health in their budgets since 2008.Citation12,Citation25,Citation26
Finally, the negative correlation between PFM quality and maternal and under-five mortality was only significant in countries with higher governance effectiveness. This finding aligns with existing literature on the favorable effects of improved governance on sectoral outcomes, while adding the observation that poor institutional quality reduces that effect.Citation27–30 To maximize PFM’s utility in achieving more favorable health outcomes, there is clear value in studying PFM and political economy factors jointly, particularly in environments facing challenges with governance.
Limitations
This study has several limitations.
First, we did not include time effects in the econometric model because not all the sampled countries had annual PEFA scores for every year of the study period. The PEFA Secretariat commonly varies the years in which it conducts annual assessments of countries’ PFM quality. Pooled OLS can be used to estimate correlations but not causal effects. Better availability of multi-year data for each country would make it possible to include time effects and estimate a causal PFM effect on health outcomes.
Second, PEFA scores covered all public sectors, without specific scoring for health-based PFM quality. It would have been more relevant to test for the effect of health-specific PFM quality on health outcomes, had those data been available. In addition, PEFA indicators assess the forms of PFM systems and process and do not necessarily account for their functional quality. They measure “how PFM looks” rather than “how PFM actually functions.” As a result, PEFA scores do not capture all aspects of PFM.Citation3
Third, calculating the overall PEFA score based on a mean may give rise to biases resulting from two potential causes: first, it assumes an equal weighting for the different PFM processes. As specified by Welham et al, this would not reflect the actual weight of each PFM dimension in the provision of health care services.Citation3 Second, an average hides PFM variations within a country, for example between rural and urban areas. Yet it is precisely these variations that must be analyzed to provide a more rigorous estimate of the effects of PFM on health outcomes.
Fourth, the paper does not identify the channels through (or levers by) which PFM quality can affect health outcomes. Analysis of these channels could provide insight into possible practical approaches, and should be the subject of a separate study.
Conclusion
The study confirms a clear relationship between PFM quality and health outcomes. The evidence suggests that countries with high-quality PFM had the lowest maternal, under-five mortality and NCDs mortality rates. Together, these findings support an emphasis on strengthening PFM as a means of improving health outcomes. Better quality PFM—as manifested through credible, multi-year, and flexible budget formulation, simple, timely, and empowering budget execution, and budget monitoring which is output-oriented, transparent, and digital—may result in more predictable and transparent health financing and a more strategic allocation and efficient use of resources. This would allow governments to provide higher quality and more accessible health care services, increased use of which would improve the health of patients.
The negative correlations with mortality were stronger when budgets included higher allocations for health and when health budgets were implemented fully and in a timely fashion. Governance seems to be complementary to PFM quality. Better governance was associated with a higher negative correlation between PFM quality and the mortality indicators.
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
Notes
[1] The sample encompasses 6 EAC, 11 SADC, 12 ECOWAS and 7 ECCAS member-countries as well as 3 countries associated with two different regional-integration zones (Burundi, Rwanda, and Tanzania) and 3 others that do not belong to any regional-integration zone (Ethiopia, Mauritania, and Sudan).
[2] Annual completion rate refers to the percentage of years in which data was provided.
References
- World Health Organization, Organization for Economic Co-operation and Development & International Bank for Reconstruction and Development. Delivering quality health services: a global imperative for universal health coverage. Geneva (Switzerland): World Health Organization; 2018 [accessed 2023 Jan 19]. https://apps.who.int/iris/handle/10665/272465.
- Goryakin Y, Revill P, Mirelman A, Sweeney R, Ochalek J, Suhrcke M. Public financial management and health service delivery: a literature review. London (UK): Overseas Development Institute; 2017 [accessed 2023 Jan 18]. https://cdn.odi.org/media/documents/11463.pdf.
- Welham B, Hart T, Mustapha S, Hadley S. Public financial management and health service delivery: necessary, but not sufficient? report. London (UK): Overseas Development Institute; 2017 [accessed 2023 Dec 3]. https://cdn.odi.org/media/documents/Public_financial_management_and_health_service_delivery_necessary_but_not_sufficient.pdf.
- Piatti-Fünfkirchen M, Smets L. Public financial management, health financing, and under-five mortality: a comparative empirical analysis. Washington (DC): Inter-American Development Bank; 2019. IDB Working Paper Series No: IDB-WP-976. [accessed 2023 Jan 19]. doi:10.18235/0001561.
- Piatti-Fünfkirchen M, Schneider P. From stumbling block to enabler: the role of public financial management in health service delivery in Tanzania and Zambia. Health Syst Reform. 2018;4(4):336–13. [accessed 2023 Jan 19]. doi:10.1080/23288604.2018.1513266.
- Cashin C, Bloom D, Sparkes S, Barroy H, Kutzin J, O’Dougherty S. Aligning public financial management and health financing: sustaining progress toward universal health coverage. Geneva: World Health Organization; 2017. Health Financing Working Paper No: 4. [accessed 2023 Jan 18]. https://apps.who.int/iris/handle/10665/254680.
- Hadley S, Hart T, Welham B. Review of public financial management diagnostics for the health sector. London (UK): Overseas Development Institute; 2020. Working Paper, No: 574. [accessed 2023 Jan 18]. https://cdn.odi.org/media/documents/200217_pfm_health_paper_final_web.pdf.
- UHC2030. Public financial management for universal health coverage: why and how it matters. Policy Note. 2020 [accessed 2023 Jan 19]. https://www.uhc2030.org/fileadmin/uploads/uhc2030/Documents/About_UHC2030/UHC2030_Working_Groups/2017_Financial_Management_Working_Group/UHC_PFM_policy_note_02XII20_online.pdf.
- Barroy H, Dale E, Sparkes S, Kutzin J. Budget matters for health: key formulation and classification issues. Geneva (Switzerland): World Health Organization; 2018 Health financing policy brief no: 4. [accessed 2023 Jan 18]. https://apps.who.int/iris/handle/10665/273000.
- Barroy H, Blecher M, Lakin J. How to make budgets work for health? A practical guide to designing, managing and monitoring programme budgets in the health sector. Geneva (Switzerland): World Health Organization; 2022 [accessed 2023 Dec 3]. https://apps.who.int/iris/handle/10665/356893.
- Piatti-Fünfkirchen M, Barroy H, Pivodic F, Margini F. Budget execution in health: concepts, trends and policy issues. Washington (DC): The World Bank; 2021 [accessed 2023 Jan 19]. http://hdl.handle.net/10986/36583.
- Barroy H, Vaughan K, Tapsoba Y, Dale E, Van de Maele N. Towards universal health coverage: thinking public: overview of trends in public expenditure on health (2000–2014). Geneva (Switzerland): World Health Organization; 2017. Health Financing Working Paper No: 7. [accessed 2023 Jan 18]. https://apps.who.int/iris/handle/10665/255782.
- Fritz V, Sweet S, Verhoeven M. Strengthening public financial management: exploring drivers and effects. Washington (DC): World Bank; 2014. Policy Research Working Paper No: 7084. [accessed 2023 Dec 3]. doi: 10.1596/1813-9450-7084.
- Kutzin J. A descriptive framework for country-level analysis of health care financing arrangements. Health Policy (New York). 2001;56(3):171–204. [accessed 2023 Dec 3]. doi:10.1016/s0168-8510(00)00149-4.
- Rutherford ME, Mulholland K, Hill PC. How access to health care relates to under-five mortality in sub-saharan Africa: systematic review. Trop Med Int Health. 2010;15(5):508–519. [accessed 2023 Dec 3]. doi:10.1111/j.1365-3156.2010.02497.x.
- Teleayo A. Assessing the impact of universal healthcare coverage on maternal and child health outcomes in Nigeria. J Community Health Provision. 2023;3(1):1–7. doi:10.55885/jchp.v3i1.219.
- Moreno-Serra R, Smith PC. Does progress towards universal health coverage improve population health? Lancet. 2012;380(9845):917–923. doi:10.1016/S0140-6736(12)61039-3.
- Bokhari FAS, Gai Y, Gottret P. Government health expenditures and health outcomes. Health Econ. 2007;16(3):257–273. doi:10.1002/hec.1157.
- Tapsoba PY Sustainable health financing for progress towards universal health coverage in low-and middle-income countries [ doctoral dissertation]. Université Clermont-Auvergne; 2017. HAL ID: tel-02121742. [accessed 2023 July 30]. https://theses.hal.science/tel-02121742/.
- Secretariat PEFA. PEFA 2016: guidance on tracking PFM performance for successive assessment. https://www.pefa.org/global-report-2020/en/report/methodology/.
- PEFA Secretariat. Public expenditure and financial accountability database [online database]. Washington, DC: PEFA Secretariat; 2018 [accessed 31 Oct 2019]. https://pefa.org/assessments.
- De Renzio P. Taking stock: what do PEFA assessments tell us about PFM systems across countries? London (UK): Overseas Development Institute; 2009. Working Paper, No: 302.
- Hashim A, Piatti M. A diagnostic framework to assess the capacity of a government’s financial management information system as a budget management tool. Washington (DC): The World Bank; 2016. doi:10.1596/25267.
- Barroy H, Kabaniha G, Boudreaux C, Cammack T, Bain N. Leveraging public financial management for better health in Africa: key bottlenecks and opportunities for reform. Geneva (Switzerland): World Health Organization; 2019. Health Financing Working Paper No: 14. [accessed 2023 Jan 18]. https://apps.who.int/iris/handle/10665/339297.
- Tandon T, Fleisher L, Li R, Yap W. Reprioritizing government spending on health: pushing an elephant up the stairs? WHO South-East Asia J Public Health. 2014;3(3–4):206–12. World Health Organization. Regional Office for South-East Asia. https://apps.who.int/iris/handle/10665/329750.
- World Health Organization. Global expenditure on health: public spending on the rise? Geneva (Switzerland): World Health Organization; 2021 [accessed 2023 Jan 19]. https://apps.who.int/iris/handle/10665/350560.
- Rajkumar AS, Swaroop V. Public spending and outcomes: does governance matter? J Dev Econ. 2008;86(1):96–111. [accessed 2023 Jan 19]. doi:10.1016/j.jdeveco.2007.08.003.
- Lewis M. Governance and corruption in public health care systems. Washington (DC): Center for Global Development; 2006. Working Paper No: 78. [accessed 2023 Jan 19]. https://www.cgdev.org/sites/default/files/5967_file_WP_78.pdf.
- Gupta S, Verhoeven M. The efficiency of government expenditures: experiences from Africa. J Policy Model. 2001;23(4):43367. [accessed 2023 Jan 18]. doi:10.1016/S0161-8938(00)00036-3.
- Hu B, Mendoza RU. Public health spending, governance and child health outcomes: revisiting the links. J Hum Dev Capabil. 2013;14(2):285–311. [accessed 2023 Jan 18]. doi:10.1080/19452829.2013.765392.