
ABSTRACT
The OECD’s 2016 ‘Neurotechnology and Society: Strengthening Responsible Innovation in Brain Science’ International Workshop drew together scientists, policy-makers, industries, regulators, and academics for the purpose of discussing the present state of neurotechnology and exchanging ideas on how RRI can, and should, play a role in the rapidly evolving field. A myriad of technologies and devices were discussed during the workshop, but one area of neurotechnology received considerable attention: transcranial direct current stimulation (tDCS). In this discussion piece, I describe what tDCS technology is, give a brief overview of its history, introduce a number of scientific studies that suggest the efficacy of the technology and, most importantly, set out some of the concerns I have for its use. The piece concludes by making the argument that we, members of the neuroscience community, have an ethical duty to become more involved in this community so that we may help guide these people and potentially prevent any unintended brain damage.
In September 2016, I attended the OECD’s ‘Neurotechnology and Society: Strengthening Responsible Innovation in Brain Science’ International Workshop, held at the National Academy of Sciences, Engineering and Medicine, Washington, DC. This high-level, international workshop drew together scientists, policy-makers, industries, regulators, and academics for the purpose of discussing the present state of neurotechnology, and exchanging ideas on how RRI can, and should, play a role in the rapidly evolving field.
While a myriad of technologies and devices were discussed during the 1.5 days, one area of neurotechnology that received considerable attention was transcranial direct current stimulation (tDCS). Though tDCS has been used for the last 200 years to probe the inner mechanisms of the central nervous system and alleviate the pressures of various neurological disorders (Sarmiento, San-Juan, and Prasath Citation2016), it is still a highly debated, and contentious, topic for a good reason.
Discussion at the OECD workshop was, for the most part, focused on the potential benefits that tDCS could offer the individual, their families, and population health more generally. Within this framing, unknown consequences and long-term side effects of tDCS were also canvassed; it quickly became clear that the potential risks are not well understood nor are they likely to be in the near future. As a student studying in the field of neurotechnology, such uncertainties were particularly unsettling to me. This is especially unsettling given that some members of the general public have taken tDCS neurotechnology research into their own hands and are actively deploying the technology on themselves.
A quick search online shows that there are, quite literally, thousands of citizen scientists communicating with each other for the purposes of exchanging information on how to use tDCS to alter their brain activity.Footnote1 Massive discussion platforms, such as the website Reddit.com, host a wide variety of conversations centered on tDCS. These citizen scientists are attempting to take healthcare into their own hands, and some are even attempting to – wait for it – enhance their own intelligence.
As much as this sounds like the plot of a futuristic cyborgian novel, I can assure you that this is a reality we face today. These citizen scientists are experimenting with their own brains and trading information with each other online on how to build, and use, these devices. More recently, companies have begun to specifically market tDCS devices to this population.Footnote2 Companies, such as Foc.us, suggest that their devices have the ability to enhance alertness, boost focus, and even increase the capacity to learn (). They advertise tDCS as a technology that works by placing the user’s neurons ‘in a heightened state of excitement that are primed to fire more rapidly’. This statement concerns me. And I am sure that I am not the only one. It makes it sound like all neurons in the brain are the same, react to similar levels of stimulation, and produce the same outcome. I am sure that you can understand my concern with this statement, especially considering that there are literally hundreds of different neuronal subtypes in the cerebral cortex alone (Molyneaux et al. Citation2007).
Figure 1. Foc.us tDCS headset.
In this discussion piece, I describe what tDCS technology is, give a brief overview of its history, introduce a number of scientific studies that suggest the efficacy of the technology and, most importantly, sets out some of the concerns I have for its use. The piece concludes by making the argument that we, members of the neuroscience community, have an ethical duty to become more involved in this community so that we may help guide these people and potentially prevent any unintended brain damage.
Transcranial current direct stimulation: What is it?
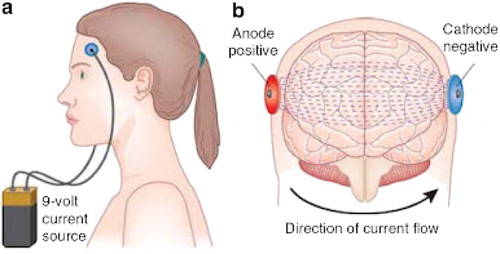
tDCS is a form of neurostimulation that involves the placement of electrodes on the human scalp for the purpose of stimulating specific brain regions (). With the electrodes in place over the area of interest, low levels of current (1–2 mA) are sent through the skull for certain durations (≤30 min) and work to alter the membrane potential of neurons either through depolarization or hyperpolarization (Woods et al. Citation2016). In layman’s terms, the neurons are either activated or suppressed. To achieve these desired results, the tDCS electrodes are either anodal or cathodal. Anodal stimulation works by depolarizing the membrane potential of neurons, which makes neurons more likely to fire. Cathodal stimulation works by hyperpolarizing the membrane potential of neurons, which decreases the likelihood that neurons will fire.
Figure 2. A simple diagram illustrating the basics of tDCS. Two electrodes, cathodal or anodal, are hooked up to a battery and placed on certain regions of the skull. Current is then applied through the electrodes to alter neural activity. Source: George and Aston-Jones (Citation2010).
The specific parameters of tDCS devices are typically controlled through a control panel that allows the user to set the strength and duration of the current. Being able to modify all the parameters of the tDCS device allows the user for greater control over all aspects of their treatment.
Origins of tDCS
Stimulating the brain as a therapeutic strategy was first imagined during the time of Luigi Galvani. During the eighteenth century, Galvani created the Galvanic Battery, which would go on to be the basis of the batteries we use today ((A)). It was Galvani’s nephew Giovanni Aldini who first employed his uncle’s battery in the clinical setting. The best-written account of Aldini utilizing this battery on humans comes from his own notes, in which Aldini describes how he attached the battery to the scalp of a 27-year-old farmer suffering from ‘melancholy madness’ ((B)) (Parent Citation2004). Aldini reported that the farmer’s mood progressively improved and, after several weeks of treatment, was completely cured.
Figure 3. (A) Schematic for Luigi Galvani’s eighteenth-century Galvanic Battery. (B) Details from plate V in Aldini (Citation1804). Sources: A, The Popular Science Monthly, Volume 12, 1877; B, Parent (Citation2004).
For almost 200 years after Aldini first applied electrical currents to the human brain, tDCS technology has been studied by doctors, researchers, and therapists alike as a potential treatment strategy for neurological and psychological conditions (Sarmiento, San-Juan, and Prasath Citation2016). Generally, inconclusive results and variation of procedures (Parent Citation2004) stifled interest in the technology and areas of clinical application. This all changed, however, in 1998 with the publication of a seminal study by Priori et al. In their study, Priori et al. (Citation1998) were able to show that tDCS application on the human skull could significantly alter neuronal excitability of the human motor cortex. The researchers ran a series of 4 experiments with 15 healthy volunteers in which they exposed the subjects to a variety of stimulation conditions. The results of these experiments demonstrated that weak (<0.5 mA, 7 s) stimulation was sufficient enough to cross the skull and influence brain activity. Given the known effects of CNS polarization in animal experiments, the researchers proposed that the technology could be used as a therapy for disorders that involve altered neuronal excitability. Before this study, there existed only indirect evidence based on reaction studies and animal models that showed any support for the technology being able to alter cortical excitability. The results of this experiment have, once again, spawned great interest in tDCS as a ‘safe’ form of non-invasive brain stimulation and a potential treatment strategy for numerous neurological disorders.
As sophisticated as this sounds, what evidence – if any – exists to suggest that the technology can be used to treat a range of neurological disorders?
Evidence for tDCS efficacy
A number of published and peer-reviewed studies now exist to suggest that tDCS is safe and effective when used for therapeutic purposes. This body of literature is growing and providing healthcare providers a valuable insight into the non-invasive ways to treat neurological disorders. In this section, I provide a summary of key areas of investigations and research results.
Treatment for stroke
In a Citation2013 study conducted by Khedr et al., 40 patients with ischemic stroke were placed into anodal, cathodal, or control tDCS treatments. The anodal group (N = 14) had an anode placed over the M1 region of the motor cortex of the damaged hemisphere and the remaining electrode placed on the contralateral supraorbital region. The cathodal group (N = 13) had the electrodes placed in the same areas as the anodal group except on the unaffected hemisphere. The control group (N = 13) had the electrodes placed on the same areas as the anodal/cathodal group, but the frequency was much lower and only applied to mimic the feeling of having the device on the head. The treatment groups were stimulated at a frequency of 2 mA for 25 min/day for 6 days. All three groups exhibited increased cortical excitability and improvements in muscular strength over the course of rehabilitation; the anodal and cathodal groups exhibited significant increases over the control group when assessed using the functional ability test (Two main clinical rating scales: OMCAS, P = .02; BI, P = .002). The authors concluded that the use of either anodal or cathodal stimulation was superior to control stimulation in enhancing the effects of rehabilitation. While the study suffers from a number of limitations, including sample size, it does suggest that tDCS has the potential to enhance the effects of rehabilitation, decrease recovery time, and ultimately improve motor recovery after stroke.
Treatment for depression
In Citation2012, Loo et al. conducted a study on 64 participants with depression in which they used tDCS on the subjects for the purposes of alleviating their depressive symptoms. The researchers applied anodal stimulation to the left dorsolateral prefrontal cortex and cathodal stimulation to the lateral aspect of the contralateral orbit. This stimulation was applied at a voltage of 2 mA for 20 min. The control group for the study had the same arrangement of electrodes, but the applied stimulation was at a voltage of 1 mA for 30 s to give the subject the sensation of stimulation. Both groups were treated every weekday for 3 weeks (15 treatments in total). Although the effects were not seen early on, after 6 weeks the stimulated group had statistically significant (P < .05) improvements in mood when compared to the control group. The researchers found tDCS to be more effective than antidepressants for this group of people. This research suggests that tDCS had the potential to help those who suffer from depression.
Enhance intelligence
One of the major claims made by companies selling tDCS devices including, for example, Foc.us, is that stimulation of certain regions of the brain can increase learning capacity. Evidence for this sort of claim can be found from a 2014 published study in which researchers were able to successfully use tDCS to induce neuroplasticity in subjects and improve learning capacity (Meinzer et al. Citation2014).
With a sample size of 40 adult patients, researchers stimulated the subject’s posterior temporoparietal junction at 1 mA for 20 min while they were tasked with memorizing novel vocabulary. This was repeated once a day over 5 consecutive days. Each day after the acquisition phase was completed and the tDCS had been turned off, subjects were asked to recall the novel vocabulary. When tested for memory acquisition against a control group (N = 20), the tDCS subjects (N = 20) were able to recall more words. These findings suggest that this technology has the capacity to enhance a human’s ability to acquire new knowledge under certain conditions.
A 2010 study utilized tDCS to produce long-lasting changes in numerical competence (Cohen Kadosh et al. Citation2010). Here, Cohen Kadosh et al. (Citation2010) applied tDCS to the left and right parietal lobe of subjects for 20 min at 1 mA while they learned artificial digits. The subjects were placed into one of three conditions: right parietal anodal-left parietal cathodal (RA-LC), right parietal cathodal-left parietal anodal (RC-LA), and control. The subjects in the RA-LC group (N = 5) consistently outperformed both the RC-LA (N = 5) and control group (N = 5) in numerical tasks. While these data are interesting, I personally found it much more perplexing that the RC-LA group performed statistically worse than the control group. This demonstrates that while tDCS may have potential benefits, it may also pose a risk to those who use it.
Possible risks of tDCS
As discussed above, there is evidence for the efficacy of tDCS in regard to alleviating both the symptoms of certain medical conditions (in certain patients) and enhancing human intelligence. But this does not mean that tDCS is 100% safe and/or effective. I have a number of specific concerns about this technology, especially when used in a nontherapeutic setting.
(1) tDCS technology has been marketed as a non-invasive device, but I argue that it is invasive
The term ‘non-invasive’ is used by physicians to describe treatment strategies that are not as invasive as traditional methods including, for example, surgery. I think it is time that we update the way we describe these methods in line with the technological advances that have occurred over the last few decades. The term ‘neuron-altering’ is, I would argue, more appropriate for describing the nature of tDCS technology and better informs consumers as to its mechanisms of action. We need to be able to emphasize that these devices are capable of depolarizing and hyperpolarizing the neurons in your brain; that the electrical current stemming from the tDCS device is capable of altering the very ionic concentration that controls the membrane potential of the neurons in one’s brain. Marketing these devices as ‘non-invasive’ may mislead consumers into believing that these devices are 100% safe and effective. When, in actuality, they are not. I argue that if we start referring to these devices as being neuron-altering, people are more likely to understand what the risks of using these devices are and may either reconsider their use or learn more about them prior to use.
(2) Stimulating areas that are part of a neural network
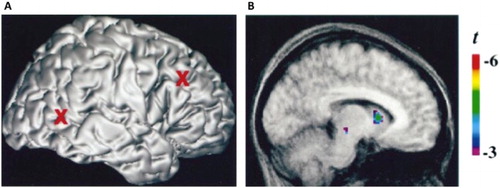
Part of the allure of tDCS is its seemingly ease of use. People believe that the technology is straightforward and will allow you to stimulate only the areas that you choose to stimulate. But that is just not the case. In a 2013 study, researchers were able to remotely activate the ventral midbrain of 19 subjects through direct current stimulation of the prefrontal cortex for 15 min at 2mA () (Chib et al. Citation2013) They hypothesized that due to the midbrain’s highly interconnected nature with the prefrontal cortex that stimulation in one part of the pathway should be able to activate other parts of the pathway. Another study conducted in Citation2001 by Strafella et al. demonstrated the ability to induce dopamine release in the caudate nucleus of eight subjects through repetitive stimulation of the prefrontal cortex (). This study utilized a similar form of brain stimulation called transcranial magnetic stimulation (TMS). TMS is a circular coil that is held over the subject’s head and electrical pulses are sent across the skull.
Figure 4. Electrical stimulation of the ventral medial prefrontal cortex caused activation of the ventral midbrain. Source: Chib et al. (Citation2013).
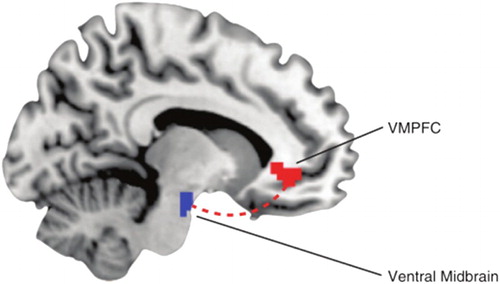
Figure 5. (A) Electrical stimulation of the cortex. (B) Induced dopamine release in the caudate nucleus due to stimulation of the cortex. Source: Strafella et al. (Citation2001).
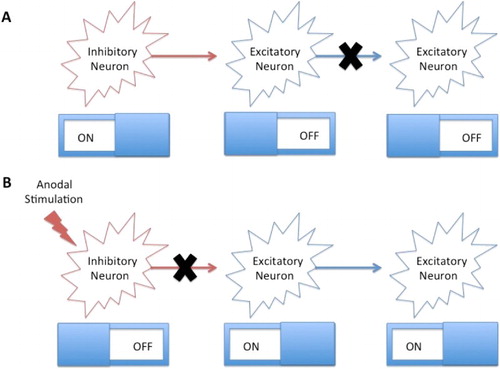
To stimulate one part, a neural network runs the risk of altering the activity of anything connected to it. The danger lies within the unintended consequences of indirectly exciting, or inhibiting, other parts of the brain. Think of a neural network like a series of switches (). The position of each switch plays a major role in the position of the other switches on the board. Imagine one switch is tasked with inhibiting the activity of an excitatory switch. This inhibitory switch is preventing the excitatory switch from activating another excitatory switch. What happens if you apply cathodal stimulation to this inhibitory switch? You will release the excitatory switch from its inhibition and allow it to excite another excitatory switch. As I am sure you can imagine this analogy can be made much more complicated if you added 86 billion more switches!
Figure 6. (A) An inhibitory neuron is inhibiting the firing on the excitatory neuron. This is in turn in preventing the firing of another excitatory neuron. (B) Cathodal stimulation is inhibiting the inhibitory neuron (disinhibition), which allows the excitatory neuron to fire and activate another excitatory neuron. Source: Author generated.
(3) Unintentional stimulation of regions near the targeted area due to the misplacement of the electrodes and/or the other region being in close proximity
To properly utilize tDCS technology, the user has to be sure of where to put the electrodes. Placing them in the correct location on the skull is challenging at the best of times. Even more so if you are not well versed in the brain’s anatomy. It gets even more complicated when you are doing it on your own head. Even a small misplacement of the electrodes may stimulate unintended areas. If you were to choose, for example, to stimulate the dorsolateral prefrontal cortex so that you can increase your working memory but instead place the electrodes a little further back than you should, you will be directly stimulating Broca’s area (). This section of the brain is important as it mediates speech and language production. Unintentional stimulation of this brain region could possibly alter your ability to form coherent speech and may lead to irreparable damage. It is exceedingly hard to imagine that use outside of the clinical setting is going to involve the level of rigor found within the clinical setting. This is highly problematic.
Figure 7. Broca’s area (represented by the circle) is within close proximity of the dorsolateral prefrontal cortex (represented by the triangle). Unintentional stimulation of either area may occur while attempting to use tDCS. Source: Author generated.
(4) Stimulation of excitatory and inhibitory neurons at the same time
The human brain is composed of vast networks of neurons that work together to perform crucial functions. Among these neurons are many different subsets that can either be excitatory or inhibitory, depending on the neurotransmitter they secrete. What this means is that when you stimulate a certain brain region you will not only be activating the excitatory neurons, but also the inhibitory neurons. Our brains are composed of a multitude of neural networks that must have specific coordination and timing between these different subsets of neurons.
To apply tDCS to any area of the brain is to create artificial-like activity. My argument here is that when you stimulate all of the neurons in one area of the brain, you are not emulating something that would occur naturally. Also, depending on the type of current you are exposing the brain to, cathodal or anodal, there will be a different outcome. Such considerations need to be taken into account before an individual uses such a device, especially when it is in the absence of an individual properly trained to use, and apply, the tDCS device.
(5) Altering the developing brain
tDCS has been marketed as a technology that may enhance different aspects of an individual’s life. But what about their athletic abilities? Companies are marketing tDCS devices toward athletes by stating that the technology has the ability to increase your reaction speed and overall athletic abilities (see note 2). This is seriously concerning to me. To begin with, a significant portion of people participating in athletic events are children and young adults whose brains are yet to be fully developed. The frontal lobes of the brain are among the last regions to mature (Sowell et al. Citation1999). Though the maturation rate of the frontal lobes differs among people, it is thought that this development can continue up until the mid-twenties. Since the frontal lobes are the home of executive functions such as planning, impulse control, and judgment, it is crucial that this brain region’s developmental trajectory goes unabated. If we wish for our children and young adults to develop into mature adults capable of sound moral judgment, then we need to pose stricter regulations on these devices. Since athletes typically fall into this age category, I worry that the use of these devices will alter the patterning of their still developing brains and cause long-term side effects. I also worry that given the competitive nature of today’s sporting events and the enormous amount of pressure that parents place on children to do well in sports that parents may subject their children to these devices to gain a ‘competitive edge’.
(6) tDCS may lead to addiction
While my argument here may be considered somewhat outlandish, I do believe that the question of addiction needs to be explored. And sooner rather than later. In Citation2012, DosSantos et al. showed that a single session of tDCS, 2 mA for 20 min, over the M1 region of the motor cortex of a 62-year-old woman was sufficient to decrease binding of an exogenous mu-opioid ligand. The researchers believed that this was due to a direct increase in endogenous opioid binding. While the research has yet to be duplicated, the research team have stated that they plan to perform future studies with a larger cohort of subjects.
The results of this study immediately made me think of the possibility of people using tDCS to get high. Wouldn’t it be interesting if people were able to use tDCS as a substitute for recreational drugs? It could eliminate the need for people to use harmful drugs such as cocaine and heroin. How could it be bad?
The reason I believe that this could lead to dangerous outcomes is because the ‘high’ achieved from tDCS may be due to neural mechanisms of action similar to that of recreational drugs. Is it likely that long-term use of tDCS to increase endogenous opioid binding will be sufficient enough to create an addictive behavior? I am sure at this point you are wondering why this would be of any concern, especially considering it is just a device you put on your head and it is not causing any harm. But take into consideration the entirety of this article. There are many unintended consequences of exposure to tDCS devices, and there can be little doubt that prolonged exposure to their use is going to cause problems. If a person develops, for example, an addiction to tDCS, we may see a similar trajectory as in addiction where a person begins to take more and more just to achieve the same effect. I argue that the longer the device is applied, and the more frequently it is used, the higher the chance it is that problems will begin to arise. Not only will this have serious negative effects for the individual and their family, but it has the potential to give rise to a myriad of larger public health problems. All the while being a drain on the already overstretched healthcare system.
Conclusion
The research that has been done on tDCS is persuasive in terms of its therapeutic uses and efficacy. Whether or not the positive results outweigh the unknown negative side effects is yet to be determined. Nonetheless, studies have provided evidence of its efficacy for the treatment of various physical and psychological disorders including, in particular, certain types of depression. I believe that this is why citizen scientists are experimenting with this technology. For some they see tDCS as an opportunity to take their healthcare into their own hands. For others they see it as an opportunity to increase their own intelligence. And some are likely to see both. At the end of the day, they ultimately want to better themselves.
Knowing what we know about the brain, I wonder whether we, members of neuroscientist community, have an ethical or moral responsibility to actively engage with the citizen scientists who are using the technology. Can we, those educated in the science and the technology, use our knowledge and expertise to counter the false assertions being put out by the companies selling tDCS devices? The promises that these companies are making are outlandish and I believe that it is our duty to help guide these citizen scientists. They do not have the same level of knowledge about the anatomy and physiology of the brain that we do. With our knowledge and intuition about the brain, does that make it our ethical or moral responsibility to get involved with this community? Yes, I believe so. Can we possibly guide their usage of tDCS and help them understand what the possible ramifications are? Absolutely.
There was once a time where it was acceptable for scientists and academics to wall themselves in their academic fortresses, bury their noses in dense research literature, and live in their intellectual bubbles. This is no longer that time. As neurotechnology advances, we are more likely to see people harming themselves in the pursuit to take control of their own brains, whether that be through electrical stimulation or experimental nootropic smart drugs. We neuroscientists need to become the voice of reason during this highly experimental time. This will involve a concerted effort by not only neurologists, but the basic neuroscience researcher as well. It is impossible for one field of neuroscience to predict all of the possible benefits and side effects of these upcoming neurotechnologies. The people of this world, and the healthcare system for that matter, can only stand to benefit if we work together with multiple fields of neuroscience to begin crafting policy that addresses the concerns I have laid out in this discussion piece. Given the complexity of the brain, crafting policy will be no easy task. I am sure that if neuroscientists and policy-makers work together to become the voice of reason behind the safe use of this technology that we will be able to prevent people from unintentionally damaging themselves. And who knows, maybe we can help guide people in safely accomplishing what they set out to do with this technology.
Disclosure statement
No potential conflict of interest was reported by the author.
Notes on contributor
Colton D. Smith is a graduate student at Arizona State University studying neuroscience. The lab that he was conducting research in utilizes transgenic organisms and high-end microscopy to elucidate the role that the MAP Kinase signaling cascade has in proper neural development. Alongside his research as a biologist, he was also involved in the discussion of policy and ethics in the neurosciences.
Notes
References
- Aldini, G. 1804. Essai théorique et expérimental sur le galvanisme. Paris: Fournier Fils.
- Chib, V. S., K. Yun, H. Takahashi, and S. Shimojo. 2013. “Noninvasive Remote Activation of the Ventral Midbrain by Transcranial Direct Current Stimulation of Prefrontal Cortex.” Translational Psychiatry 3: e268. doi:10.1038/tp.2013.44.
- Cohen Kadosh, R., S. Soskic, T. Iuculano, R. Kanai, and V. Walsh. 2010. “Modulating Neuronal Activity Produces Specific and Long-lasting Changes in Numerical Competence.” Current Biology 20: 2016–2020. doi: 10.1016/j.cub.2010.10.007
- DosSantos, M., T. Love, I. Martikainen, T. Nascimento, F. Fregni, C. Cummiford, M. Deboer, J. Zubieta, and A. DaSilva. 2012. “Immediate Effects of tDCS on the µ-opioid System of a Chronic Pain Patient.” Frontiers in Psychiatry. doi:10.3389/fpsyt.2012.00093.
- George, M. S., and G. Aston-Jones. 2010. “Noninvasive Techniques for Probing Neurocircuitry and Treating Illness: Vagus Nerve Stimulation (VNS), Transcranial Magnetic Stimulation (TMS) and Transcranial Direct Current Stimulation (tDCS).” Neuropsychopharmacology 35 (1): 301–316. doi:10.1038/npp.2009.87.
- Khedr, E., O. Shawky, D. El-Hammady, J. Rothwell, E. Darwish, O. Mostafa, and A. Tohamy. 2013. “Effect of Anodal Versus Cathodal Transcranial Direct Current Stimulation on Stroke Rehabilitation: A Pilot Randomized Controlled Trial.” Neurorehabilitation and Neural Repair 27 (7): 592–601. doi:10.1177/1545968313484808.
- Loo, C., A. Alonzo, D. Martin, P. Mitchell, V. Galvez, and P. Sachdev. 2012. “Transcranial Direct Current Stimulation for Depression: 3-Week, Randomised, Sham-controlled Trial.” The British Journal of Psychiatry 200: 52–59. doi:10.1192/bjp.bp.111.097634.
- Meinzer, M., S. Jahnigen, D. Copland, R. Darkowa, U. Grittner, A. Kevirame, A. Rodriguez, R. Lindenberg, and A. Floel. 2014. “Transcranial Direct Current Stimulation Over Multiple Days Improves Learning and Maintenance of a Novel Vocabulary.” Cortex 50: 137–147. doi: 10.1016/j.cortex.2013.07.013
- Molyneaux, B. J., P. Arlotta, J. R. L. Menezes, and J. D. Macklis. 2007. “Neuronal Subtype Specification in the Cerebral Cortex.” Nature Reviews Neuroscience 8 (6): 427–437. doi:10.1038/nrn2151.
- Parent, A. 2004. “Giovanni Aldini: From Animal Electricity to Human Brain Stimulation.” The Canadian Journal of Neurological Sciences 31 (4): 576–584. doi:10.1017/S0317167100003851.
- Priori, A., A. Berardelli, S. Rona, N. Accornero, and M. Manfredi. 1998. “Polarization of the Human Motor Cortex through the Scalp.” Neuroreport 13 (9): 2257–2260. doi: 10.1097/00001756-199807130-00020
- Sarmiento, C. I., D. San-Juan, and V. B. S. Prasath. 2016. “Letter to the Editor: Brief History of Transcranial Direct Current Stimulation (tDCS): From Electric Fishes to Microcontrollers.” Psychological Medicine 46 (Aug.): 1–3. doi:10.1017/S0033291716001926.
- Sowell, E., P. Thompson, C. Holmes, T. Jernigan, and A. Toga. 1999. “In Vivo Evidence for Post-Adolescent Brain Maturation in Frontal and Striatal Regions.” Nature Neuroscience 2 (10): 859–861. doi: 10.1038/13154
- Strafella, A., T. Paus, J. Barrett, and A. Dagher. 2001. “Repetitive Transcranial Magnetic Stimulation of the Human Prefrontal Cortex Induces Dopamine Release in the Caudate Nucleus.” The Journal of Neuroscience 21: RC157.
- Woods, A. J., A. Antal, M. Bikson, P. S. Boggio, A. R. Brunoni, P. Celnik, L. G. Cohen, et al. 2016. “A Technical Guide to tDCS, and Related Non-invasive Brain Stimulation Tools.” Clinical Neurophysiology 127 (2): 1031–1048. doi:10.1016/j.clinph.2015.11.012.
