
Abstract
The ubiquitous nature of microorganism and its ability of being transmitted have raised serious concerns, particularly items/objects used by multiple people. The aim of this study is to assess the microbial quality of water-containing vessels/containers (kettles) for ablution in Nyankpala in the northern region of Ghana. Thirty ablution kettles from 10 mosques were sampled by taking 90 swab samples which were taken from the external surfaces of these kettles for laboratory analyses for four bacteria (Staphylococcus spp., Salmonella spp., Shigella spp. and Escherichia coli) known to majorly cause infectious diseases pertaining to hygiene and sanitation. Swabbed samples were spread-plated on various appropriate media and incubated. Viable colonies were then counted and recorded as colony-forming units (cfu/cm2). Confirmations of bacteria were done using citrate, urease, Triple Sugar Iron and catalase tests. A questionnaire was also administered to assess the knowledge of mosque management regarding bacterial contamination of surfaces as well as mosque management practices that influence it. Also, 70% of the mosque management in Nyankpala had no idea about microbial contamination of the ablution kettle, while 30% had fair knowledge about it. The study indicated that Staphylococcus spp. was the highest in occurrence (79.33%), followed by Shigella spp. (10.76%), E. coli (9.17%) and Salmonella spp. (0.75%). It was recommended that proper hand washing among ablution kettle users should be practiced as most contaminations were observed from contact with palms of handlers and avenues be created by stakeholders of hygiene and public health for educating mosque managements on the risk of microbial contamination as well.
PUBLIC INTEREST STATEMENT
The incidence of hygiene and sanitation has become a nationwide concern which Ghana in no exception. However, efforts have not been made with regard to sustainable strategies to curb and mitigate it. The article seeks to create awareness to make conscious efforts to prevent microbial contamination. Also, the work is to notify Government of Ghana and other stakeholders to take the issue serious. Consequently, this work sought to make available comprehensive information about the extent of microbial contamination of ablution kettles in selected mosque in the Nyankpala community. Also, 70% of mosque management in Nyankpala had no idea about microbial contamination of the ablution kettle, while 30% had fair knowledge about it. The study indicated that Staphylococcus spp. was the highest in occurrence (79.33%), followed by Shigella spp. (10.76%), E. coli (9.17%) and Salmonella spp. (0.75%). The study recommends cautiousness in the use of ablution kettles in public places.
Competing Interest
The authors declare no competing interest.
1. Introduction
Ablution is a general term used to describe ritual purification. Basically, ritual purification is a standard set by the Islamic religion to cleanse oneself prior to performing Islamic prayers or worship. It is a recognized ritual among at least four major religions of the world: Islam, Christianity, Judaism and Shintoism. In Islam, ablution (“Wuḍu” in Arabic) mainly denotes the Islamic established method for washing parts of the body. Wudu is an item of indulgence which has become an everyday inevitability for all Muslims as it is typically done in preparation for formal prayers (salat) and also before handling and reading the Qur’an (C. Glasse Citation2001).
The vessels/containers in which water can be held for use for ablution according to the Islamic tradition have not been specified. But evolutions in technology and civilization clearly have had tremendous impact on them when comparison is made between vessels used in recent times and what were conventionally used in the early ages of Islam. In the early Islam, quite apart from the use of water in their natural environments such as rivers, dams, springs, among others, it was much more common to find the use of bowls, gourds and buckets as containing vessels for ablution water. In recent times, due to technological advancement and changes in the social lives of Muslims, much more sophisticated ways have been developed to make performing ablution easier. Running taps, ablution bowls and water bottles are examples of such improvements in the developed Muslim world such as Saudi Arabia, United Arab Emirates, Qatar and most portions of the Middle East. In West Africa, however, as of now, such levels of advancement have not been reached on a large scale, but a few innovative trends have obviously taken place pertaining vessels for water for performing ablution in recent times as compared to the early days of Islam.
The ablution kettle “booter” has become the most pervasive water container for ablution in West Africa. It, therefore, comes as no surprise to see that many Ghanaian Muslims make optimum use of the ablution kettle in performing their religious rituals. The quality of hygiene exercised over these kettles is, however, always brought to question, especially with emphasis on the consequent effects on the health of its users.
Infectious diseases affect the world unequally. Sixty-two percent (62%) of all deaths in Africa and 31% of all deaths in Southeast Asia are caused by infection diseases (Global Health Council, Citation2005). About half of all the infant mortalities each year are due to diarrhea and acute respiratory infections, both of which are transmitted from person to person during everyday interaction, through droplet and airborne spread, through skin contact and through contamination of the environment (World Health Organization [WHO], Citation2002). However, many of these diseases are preventable as it is estimated that the global disease burden could be lessened by one-tenth simply by improving water quality, sanitation and personal hygiene (World Health Organization [WHO], Citation2014).
The worst perpetrators of infections on humans are microorganisms which are deemed ubiquitous; hence, despite the unique role of the ablution kettle in the daily lives of its users, can serve as reservoirs for microbes. They can help spread infectious diseases by recurrent contact with hands (L. H. Kilic, L. H. Kilic, et al. Citation2009), and as a matter of fact, several epidemiological studies have corroborated that surfaces play major roles in the spread of infectious diseases (J. Nobel Citation2001). By way of a disclaimer, however, the hygienic conditions of the vessels for ablution water such as the ablution kettle have not been specifically prescribed by the Islamic tradition. Hence, the hygiene exercised over these kettles varies from place to place, society to society, culture to culture and even from person to person. Again, there are varying levels of hygiene and sanitation ablution kettle users in the urban and rural areas or less endowed areas both in the field of knowledge and that of income.
Wudu involves washing the hands, mouth, nostrils, arms, head and feet with water and is an important part of ritual purity in Islam. However, all these serve as effective routes for disease transmission (Glasse, Citation2001). The Muslims of West Africa have taken up the use of ablution kettles to perform this all important ritual from the Islamic perspective. However, the major challenge is the quality of hygiene and the status of the ablution kettle and its consequent effects on the quality of water put in them as well as the health of its users. From the Muslim tradition, it is strongly encouraged to use water when one attends the restroom or the urinal to ease him/herself. Hence, most Muslims attend the restroom with water in ablution kettles which are some of the most contaminated areas where infectious diseases can be contracted (ESFJ, 2014).
Also, there has being limited research on the hygienic status of water-containing vessels for ablution among its users. Hence, this study therefore sought to assess the microbial quality of water-containing vessels/containers (kettles) for ablution in Nyankpala in the northern region of Ghana by detecting for Staphylococcus spp., Salmonella spp., Shigella spp. and Escherichia coli, which are known for causing infectious diseases.
2. Methodology
2.1. Study area
This study was conducted in Nyankpala, a suburb of the Tolon District in the northern region of Ghana. It is a community with about 2,000 natives and an influx of about a similar population coming into the University for Development Studies (UDS) situated in its environs. The dominant ethnic group in this area is Dagomba with the Dagbani language as the most widely spoken dialect. Being one of the communities of the Tolon District known to have about 94.1% of its inhabitants as Muslims, most of the people there as such make use of the ablution kettles mostly at the various mosques for their ritual purification (Ghana Statistical Service [GSS], Citation2014).
There are a total of about 29 public mosques in Nyankpala, about 18 of which provide ablution kettles for public use. Out of these, 10 were selected at random for this study (Figure ).
2.2. Sampling procedure
First of all, the study area (Nyankpala) was zoned into three sections, namely the eastern zone, western zone and the UDS campus area. The eastern and the western zones were determined by using the main road that leads into the township towards the Nyankpala market. Within each cluster/zone, mosques with ablution kettles were purposively targeted. Eighteen mosques in total (including mosques on the UDS campus) were discovered to have ablution kettles for public use at the mosques. Hence, using simple random sampling, 10 mosques were chosen to have samples taken from their ablution kettles for the laboratory analysis. The modal number of ablution kettles found in the mosques in Nyankpala was about 5 with the highest number of kettles in a mosque being about 17 and the least number of kettles being 3. Hence, simple random sampling was again employed to select three ablution kettles at each chosen mosque. A total of 30 ablution kettles were selected for the swab samples to be taken, and in the end, 90 swab samples were taken for laboratory analyses of the four strains of bacteria selected. This is because that one of the media for culturing the bacteria (Salmonella–Shigella Agar) can accommodate two strains of bacteria on the same plate (Salmonella spp. and Shigella spp.), and so instead of 120 swabs, 90 swabs were enough to accommodate the four strains.
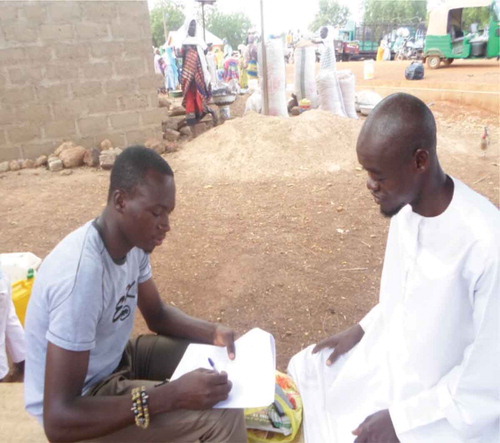
In addition, a semi-structured questionnaire was designed and administered to key informants (mosque management) for information on how ablution kettles were treated, the various demographics of mosques and the knowledge level of mosque management as far as microbial contamination of ablution kettles is concerned.
Plate 1. Taking swabs from ablution kettles.

Plate 2. Qualitative data collection.
2.3. Study design
The research was based on experimentation, observation and a field survey. Laboratory experiments were conducted at the Spanish Laboratory Complex in Ghana UDS Nyankpala campus while data concerning environmental, hygienic and sanitary conditions as well as the knowledge level of users of the ablution kettles about microbial contamination were taken by administering questionnaires and personal observation.
The experiment was done by culturing the various microorganisms (Staphylococcus spp., Salmonella spp., Shigella spp. and E. coli) using various appropriate media. Thus,
MacConkey Agar was used for culturing E. coli,
Mannitol Salt Agar for culturing Staphylococcus spp. and
Salmonella–Shigella Agar for culturing both Salmonella spp. and Shigella spp.).
Samples were picked up using swab sticks. Three swabs were used to swab the handles and external surfaces of each of the ablution kettles selected. Each of the swabs was, respectively, used to culture for the aforementioned bacteria. The swabs, however, under sanitized conditions were processed into a moist form by using (0.9%) saline solution so as to ease the process of swabbing. The swabbed samples were then transported to the lab in an ice chest filled with ice cubes to keep the tip of the swab moist.
The various culture media were prepared following the manufacturers’ instructions. Petri dishes, some of the culture media and other necessary glassware and equipment needed were sterilized by autoclaving at 121°C for about 15 min. After cooling the media, they were poured into 15–20-ml petri dishes. The swabs were spread-plated on the various media and incubated at temperatures based on the requirements of the bacteria cultured for. After the incubation period, plates were counted for colonies of bacteria. Confirmatory tests were done for all the colony-forming units (cfu/cm2) obtained.
2.4. Microbiological analyses
Microbial analyses with the aid of Laminar flow/Hood were carried out using the total plate count method. The total level of microbial contamination was determined. The media used were MacConkey agar, Salmonella–Shigella agar and Mannitol Salt agar for the culturing of E. coli spp., Salmonella spp., Shigella spp. and Staphylococcus spp., respectively, which were prepared in the laboratory according to the prescribed standard. Biochemical analysis for confirmation of the various bacteria were done using urease, citrate and Triple Sugar Iron agars as well as (H2O2) for catalase tests.
2.5. Statistical analyses
Statistical analyses of results were conducted using Genstat Discovery version 4.10. 3, IBM SPSS Statistics version 23 and Microsoft Excel to find means, standard deviations, frequencies and percentages and to produce tables and charts for the final results and conclusions.
3. Results and discussion
3.1. Results from questionnaire
Figure illustrates the educational status of respondents in the various mosques studied. The mosque management who responded to the questionnaire issued have gone through formal education to up to tertiary level, 30 (30%) of the respondents, however, have not in any way had the opportunity to go through formal education and 10 (10%) each of the respondents have been through formal education up to secondary education, respectively.
Figure 1. Map showing the study area.
Source: GSS, (Citation2014).
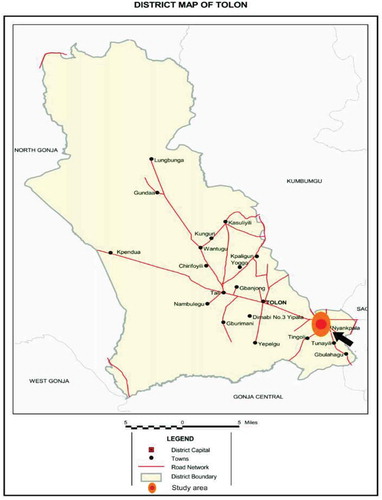
Figure 2. Level of education of respondents.
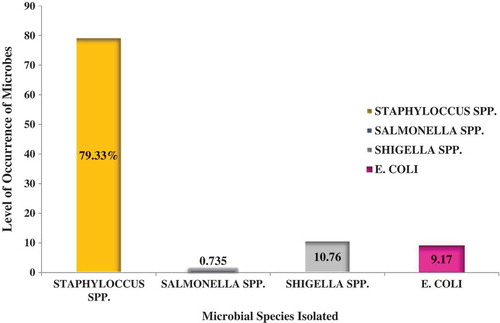
Figure illustrates the level of awareness of mosque management about bacterial contamination of surfaces. We observed that 70% of the respondents were unaware of ablution kettle contamination by bacteria, while 30% responded positively.
Figure displayed the knowledge of mosque management to prevent bacterial contamination.
Figure 3. Knowledge of mosque management about bacterial contamination.
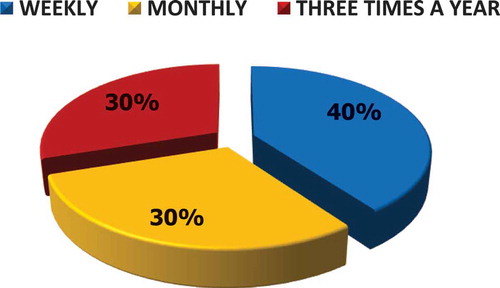
Interestingly, only 40% and 30% of the respondents clean their ablution kettles weekly and three times a year, respectively (Figure ).
Figure shows the percentage of mosques with racks to keep their ablution kettles or not. From the table, 80% of the mosques did not have racks, while 20% did.
Figure 4. How often mosque management wash their ablution kettles.
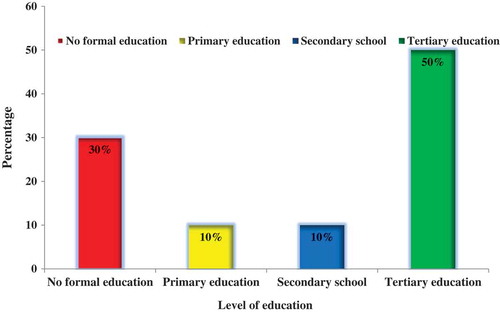
Figure 5. Storage of ablution kettles.
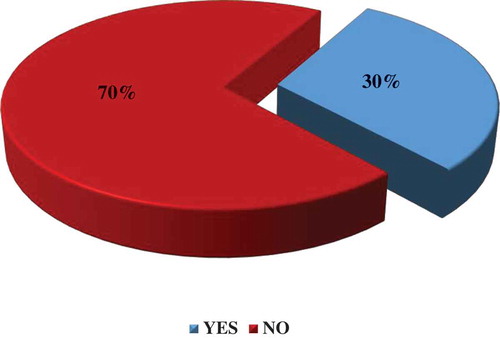
Table illustrates the main sources of water for ablution. Thirty percent of the mosques make optimum use of pipe-borne water for ablution, while 70% mostly make use of dam water. None of the mosques, however, made use of borehole or well water sources.
Table 1. Sources of water for ablution in Nyankpala mosques
3.2. Knowledge level of mosque management about microbial contamination
Contaminated surfaces when brought even into relatively brief contact with the fingers, palms or inanimate surfaces, significant number of organisms can be transferred (E. Scott and S. F. Bloomfield Citation2008). Inadequate knowledge about where germs/microbes lurk could result in the spread of health disorders such as intestinal tract infections as a result of the unhygienic use of artifacts such as the ablution kettle (P. Nancy, P. Nancy, et al. Citation2008). Awareness on contamination of surfaces and the likely microbial contamination of ablution kettle surfaces was very low on the part of mosque management in Nyankpala. This trend could be a very significant contributing factor to the ineffective management strategies put up in the mosques to maintain sanity, especially of the ablution kettles.
3.3. Microbial analyses
Different species of bacteria were isolated from the various samples that were collected from the various mosques. The bacteria genera that were isolated include Staphylococcus spp., Salmonella spp., Shigella spp. and E. coli. Table shows the various bacteria isolated from the ablution kettles of each of the sampled mosques within Nyankpala. Staphylococcus spp. and Shigella spp. were both identified in all the mosques. Salmonella spp. were found only in mosques A, F, G and H. E. coli, on the other hand, was found present in all the mosques except mosques A, B and J.
Table 2. The genera of bacteria isolated from the ablution kettles of the various mosques
Figure displayed the percentage contribution of various bacteria isolated from sampled ablution kettles. Staphylococcus spp. (79.33%) was the most dominant, next was Shigella spp. (10.76%), E. coli (9.17%) and Salmonella spp. (0.75%).
Figure 6. Bacteria isolated from the ablution kettles at various mosques in Nyankpala.
However, the analyses of variance (ANOVA) of occurrence of the various bacteria species in the various mosques in Nyankpala were not statistically significant in occurrence of any of the various bacteria between the various treatments (mosques) and the replications (sampled ablution kettles).
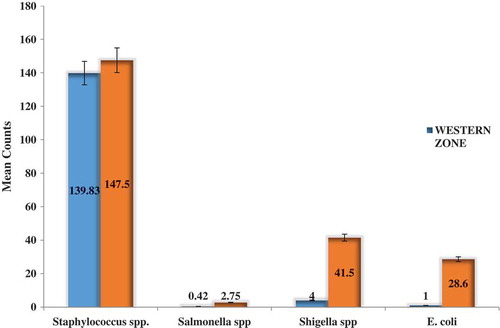
Figure illustrates a comparison of the mean level of occurrence of the various bacteria (Staphylococcus spp., Salmonella spp., Shigella spp. and E. coli) on ablution kettles of mosques within two zones of Nyankpala: the western and the eastern zones. The western plots of the various bacteria are represented by light blue bars, while the eastern plots are represented by orange bars. It was observed that the mean occurrence of Staphylococcus spp. in the eastern zone (147.5 cfu/cm2) was higher than the western zone (139.83 cfu/cm2). Also, for Salmonella spp., the eastern zone (2.75 cfu/cm2) yet again recorded a higher occurrence than in the western zone (0. cfu/cm2). Also, for Shigella spp., the eastern zone (41.5 cfu/cm2) once again had a higher recording than that of the western zone (4.00 cfu/cm2), and finally, for E. coli, the eastern zone (28.6 cfu/cm2) once again recorded the highest count than in the western zone (1).
Figure 7. Comparison of bacteria counts between the eastern and the western zones of Nyankpala.
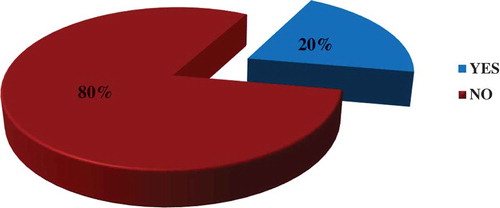
Table shows the total aerobic counts of the various bacteria on the surfaces of ablution kettles under study. The total aerobic counts ranged from 1.12 × 102 cfu/cm2 to 3.79 × 102 cfu/cm2 for the various mosques. The order of the viable bacteria were 3.79 × 102 cfu/cm2 (F) > mosque 2.36 × 102 cfu/cm2 (E) > 1.68 × 102 cfu/cm2 (B) > 1.48 × 102 cfu/cm2 (I) > 1.47 × 102 cfu/cm2 (D) > 1.46 × 102 cfu/cm2 (H) > 1.41 × 102 cfu/cm2 (C) > 1.24 × 102 cfu/cm2 (A) > 1.20 × 102 cfu/cm2 (G) > 1.12 × 102 cfu/cm2 (J).
Table 3. Mean viable count of bacteria in the various mosques in Nyankpala
3.4. Microbial load on ablution kettles
The level of microbial contamination of ablution kettles in mosques at Nyankpala was examined in this study. It was observed from the study that the ablution kettles were contaminated with Staphylococcus spp., Salmonella spp., Shigella spp. and E. coli. Using a keyboard in his study, R. Marsden Citation2009 posited that anytime an object, such as the ablution kettle in this case, is shared among two or more people, and it poses a risk of the spread of infectious agents.
Staphylococcus spp. was the most occurring species of bacteria observed on the ablution kettles with a percentage of 79.33% as shown above. This may be attributed to palm/hand contact with users. The human skin is a good habitat for Staphylococcus spp. because users of the ablution kettles have direct contact with its handle or upper surface (E. A. Grice, E. A. Grice, et al. Citation2009). Users of the ablution kettles’ palms/hands are in direct contact with the handle or upper surface of the ablution kettle. The palm is moist to varying degrees due to perspiration, the result of which makes the palms to be basic which is known for sustaining the growth of halophytic bacteria such as Staphylococcus spp. (T. Elliot, M. Hastings and U. Desselberger Citation2001).
Shigella spp. was the second most occurring bacteria species with 10.76% in the various mosques. This largely is attributed to the handling by users as Shigella spp. are found in the human intestines, thereby suggesting fecal sources of contamination of the ablution kettles. This is supported by the observation made in the mosque which recorded the highest count of this species (mosque F) having a toilet facility sited close to it and the locals making use of it by taking some of the ablution kettles to the facility to ease themselves.
The presence of E. coli being the third highest in occurrence (9.17%) indicated recent fecal contamination of ablution kettles. This may be attributed to contamination with feces after visiting the toilet, human sewage or contaminated water, fecal matter of animals and improper/inadequate hand washing as stated (D. H. Tambekar, S. D. Shirsat and S. B. Suradkar Citation2007). The source of contamination of E. coli is closely related to Shigella spp. as this species is known to be abundant in the gut of mammals. The mosque which recorded the highest count of this species (mosque E) was situated close to the abattoir as well as the market of the town and could be the source of contamination. Also, mosque F which recorded the second highest number of this species as already indicated had a toilet facility close by and could be the reason for the contamination. It was also observed in mosque I that bats were hanging up on a tree under which their ablution kettles were kept. These bats could drop their fecal matter on these ablution kettles which might have accounted for the presence of the species at that mosque. The presence of E. coli on the ablution kettle samples is an indication of fresh fecal contamination.
Salmonella spp. was the least because it thrives in a protein-rich medium which many of the respondents could not afford regularly. Nonetheless, mosque H and F located at the center of the town recorded the highest count of this species and could be attributed to the fact that the mosque were sited close to a protein source and the place was concentrated with food products. Also there are higher numbers of people with different levels of hygiene around the market who might be making use of the ablution kettle.
Not all the above-mentioned microbial species were found in each mosque. E. coli for instance was absent in mosques A, B and J. Salmonella spp. was also found to be absent in mosques B, C, D, E, I and J. It is worth noting that the level of microbial contamination varied from one mosque to the other with some recording high microbial presence while others recorded low microbial presence.
3.5. Factors that influenced microbial load and contamination of ablution kettles
All the microbial contamination of ablution kettles can be attributed to factors such as the location of the mosques, the mosque management strategies and also the demographics of the mosque attendees. Some of the mosques were located within the township, especially the market areas as well as the UDS campus, and are therefore easily accessed by numerous users, while others were found in very obscure locations where only few people had access to them. Generally speaking, the more accessible these mosques are, the more diverse the types of microbes present and hence the higher the level of microbial contamination (A. K. Al-Ghamdi, A. K. Al-Ghamdi, et al. Citation2011). In situations where there are a lot of people using the ablution kettles in mosques, there is likely to be a good number of sick people or people with varying hygienic conditions. Through them, new bacteria would settle on the ablution kettle, get release into the air or from physical contact (V. Lam, V. Lam, et al. Citation2011). This could account for the differences in microbial types and numbers among the different mosques that was observed. Also, the environmental conditions in the areas where these mosques were located played a very important role. Some of the mosques were located around areas where the environment was highly polluted with fecal matter, litter, other forms of excreta and some waste disposal areas. For instance, some of the mosques were located around the abattoir where the gut of slaughtered animals could serve as convenient sources of these bacteria strains, others around drainage gutters where liquid waste and others were discarded and others around toilet facilities. Others, however, were found in less polluted environments. J. Fleming Citation2007 posited that a variety of reservoirs in the environment can serve as sources of contamination.
Predominantly, hygiene levels influence the quantity of microbes on surfaces and thus the chance of transmission during handling of ablution kettles. Antimicrobial resistance has been observed to steadily be on the rise (H. Gedik, H. Gedik, et al. Citation2010), and contaminated surfaces such as the ablution kettle contribute to the spread of these multi-drug-resistant microbes among the public. One factor that had a significant influence on the microbial contamination of the ablution kettle in mosques is the management strategies put into play by mosque management. Generally, it was observed that microbial contamination in mosques which regularly washed their ablution kettles (e.g. mosques A, I and J) was found to be lower as compared to mosques which did not as regularly wash their ablution kettles (e.g. mosques E, F and H). Also, the fact that none of the mosques provided soap and antiseptic for use by the public after visiting urinals or toilets could be an accounting factor to the levels of microbial contamination on ablution kettles in mosques. Human hands and artifacts of public use/contact are prime sources of disease transmission, and the ablution kettle may serve as a key vehicle in the broadcast of diseases or disease-causing organisms (T. K. C. Pope, P. T. Ender and W. K. Woek Citation2002). Another contributing factor to microbial contamination of ablution kettles noticed in mosques due to mosque management strategies could be the inability to provide racks and proper storage facilities for keeping them, there by leaving them to the mercy of stray animals, rodents and other unfavorable environmental conditions.
3.6. Potential health hazards of contamination of ablution kettles
Staphylococcus spp. is a strain of bacteria usually found in large quantities in the environment and also found on the human body. Some strains of this species can be pathogenic and can cause serious infections in immunocompromised persons varying from urinary tract infections to osteomyelitis and valvular endocarditis (C. Mims, C. Mims, et al. Citation2004). Other popular infections caused by Staphylococcus spp. are boils, meningitis, bumble foo, arthritis, pneumonia, black pox, bronchitis, carbuncle, cystitis and scaled skin (B. Stuart Citation2005). Therefore, the high occurrence of Staphylococcus spp. on ablution kettles in mosques within the Nyankpala community is a major cause for concern.
Salmonella spp. belongs to the family Enterobacteriaceae. Salmonella spp. is facultative anaerobic, gram-negative, oxidase-negative and rod-shaped bacteria. Salmonellae cause diseases in both humans and animals. The serovar S. Typhi and most S. Paratyphi strains cause serious systemic infections in humans and are specific human pathogens. Salmonella cause a wide range of symptoms from diarrhea, cramping, vomiting and nausea to more serious complications and illness (P. N. Acha and B. Szyfres Citation1987).
E. coli is a gram-negative, facultative anaerobic and rod-shaped strain of bacteria which is usually found in the intestines of warm-blooded organisms. Most E. coli strains are known to be harmless, but some serotypes of which are also known to be pathogenic. E. coli (0157:H7) is a strain of this particular bacteria which can cause serious anemia or kidney failure and can eventually lead to death (www.webmd.com/a-to-Z guide/e. coli). Several laboratories have therefore characterized them as causing self-limiting diarrhea, hemorrhagic colitis, hemolytic uremic syndrome and thrombotic thrombocytopenic purpura in children and other susceptible groups of individuals (J. Meng, J. Meng, et al. Citation2001).
Shigella spp. is a genus of gram-negative, nonspore-forming, facultative anaerobic, nonmotile and rod-shaped bacteria which genetically has been observed to be closely related to another strain of bacteria known as E. coli (E. Yabuuchi Citation2002). Shigella is causative agent of human shigellosis; it causes disease in primate, but not in other mammals (K. J. Ryan and C. G. Ray Citation2004)
On a global scale, Shigella is one of the leading bacterial causes of diarrhea, resulting in an estimated 80–165 million cases (A. Bowen Citation2016). Annually, the number of deaths it causes is estimated between 74,000 and 600,000 deaths (Bowen, Citation2016; S. Mani, T. Wierzba and R. I. Walker Citation2016). It counts as part of the top four pathogens that are responsible for moderate-to-severe diarrhea in African and South Asian children (K. L. Kotlogg, J. P. Nataro and W. C. Blackwelder Citation2013).
The illustration shows the levels of contamination that are deemed acceptable as well as levels that are deemed contaminated according to BC CDC (Citation2010). From the above, swab samples which have <45 cfu/cm2 of bacteria on them are deemed clean enough for use by humans. However, even more specifically, if there is a specified area of 25 cm2 that is swabbed, then it is required that the number of cfu/cm2 of bacteria found should be <5. Contaminated levels are also said to range between 140 and 260 cfu/cm2, while any number >260 cfu/cm2 is deemed highly contaminated. From the experiment on swabs taken from ablution kettles at the various mosques as shown in Table , the mean total aerobic counts ranged from 1.12 × 102 to 3.79 × 102 cfu/cm2 which in essence showed that all the kettles from the mosques were either contaminated or very contaminated according to BC CDC (Citation2010) standards of swabbed surfaces.
Table 4. BC Centers for Disease Control (CDC) standard for swabbed surfaces
4. Conclusion and recommendation
The study assessed the microbial quality of ablution kettles used at mosques in Nyankpala by examining the level of occurrence of four strains of bacteria, namely Staphylococcus spp., Salmonella spp., Shigella spp. and E. coli. The study revealed the abundance of Staphylococcus spp. contamination of ablution kettles recorded 79.33%, Shigella spp. 10.76%, E. coli 9.17% and Salmonella spp. 0.75%. Ablution kettles no doubt have matchless importance to its users, but its multi-user nature poses a risk serving as reservoirs and vehicles for microbial contamination and transmission. Slight differences exists among the concentration of the bacteria studied; however, sources of contamination could be discovered to range from individuals who used these ablution kettles, the environment in which these ablution kettles were located as well as the various mosque management activities that were carried out in these mosques.
In general, the prevalent means of bacterial contamination are through palm contact with the kettles. It is therefore imperative that proper hand washing practices and decontamination of kettles should be adopted by mosque users.
The study therefore recommend that,
Avenues for education of mosque management and other ablution kettle users about microbial contamination should be taken up by stakeholders of hygiene and environmental safety.
Additional information
Notes on contributors
A. Waris Abu-Safianu
Mr. Abu-Safianu A. Waris holds a BSc Renewable Natural Resources (majored in Ecotourism and Environmental Management).
S. J. Cobbina
Dr. Cobbina S. J is a Senior Lecturer and Vice Dean of the Faculty of Natural Resources and Environment of the University for Development Studies. He has a PhD in Environmental Science and Engineering from Jiangsu University and an MPhil in Environmental Science. He has been the principal researcher in various projects such as the UNICEF-funded studies on hand washing with soap (HWWS) in basic schools in the northern region of Ghana and the CIDA-funded FARMER project on the quality of water in dugouts in northern Ghana. He is currently a member of a research team assessing the environmental and human health impacts of oil and gas activities on frontline communities in Ghana.
E. Yeleliere
Mr. Yeleliere E has a BSc Renewable Natural Resources and majored in Environmental management.
References
- Acha, P. N., & Szyfres, B. (1987). Zoonotic tuberculosis. Zoonoses and communicable diseases common to man and animals (2nd ed.). Washington, DC: Pan American Health Organization (PAHO)/World Health Organization, 503.
- Al-Ghamdi, A. K., Abdelmalec, S. M. A., Ashshi, A. M., Faidah, H., Shukri, H., & Jiman-Fatani, A. A. (2011). Bacterial contamination of computer keyboards and mice, elevator buttons and shopping carts. African Journal of Microbiology Research, 5(23), 3998–4003.
- BC Centre for Disease Control. (2010). Environmental hygiene monitoring. A guide for environmental health officers (3 ed., pp. 5–6).
- Bowen, A. (2016). Chapter 3: Infectious diseases related to travel. In The yellow book: Health information for international travel. CDC. ISBN 978-0-19-937915-6. Retrieved 16th May, 2017.
- Elliot, T., Hastings, M., & Desselberger, U. (2001). Lecture notes on medical microbiology (3rd ed.). Oxford: Blackwell Publishing, 20 [Google Scholar].
- Fleming, J. (2007). Computer keyboards, a new reservoir for infection transmission. Managing infection control.
- Gedik, H., Yahyaoglu, M., Yӧrük, G., & Fincanci, M. (2010). Extended-spectrum beta-lactamase production rates of Klebsiella spp. and Escherichia coli strains isolated from infections and faecal samples of healthy people. Infectious Diseases in Clinical Practice, 18, 104–106.
- Ghana Statistical Service. (2014). 2010 Population and housing census: District analytical report. Tolon District.
- Glasse, C. (2001). The new Encyclopedia of Islam (pp. 477). Walnut Creek, CA: Altamira Press.
- Global Health Council. (2005). Global health news. Initiative of University of Uta. Retrieved 10 June, 2017, from www.old.globalHealth.org.new/past-sear
- Grice, E. A., Kong, H. H., Conlan, S., Deming, C. B., Davis, J., Young, A. C., … Murray, P. R. (2009). Topographical and temporal diversity of the human skin microbiome, Science, 324(5931), 1190–1192. PMC 2805064. PMID 19478181.
- Kilic, L. H., Ozaslan, M., Karagoz, I. D., Zer, Y., & Davutoglu. (2009). The microbial colonization of mobile phones used by healthcare staff. Pak Journal Biologic Sciences, 12(11), 882–884.
- Kotlogg, K. L., Nataro, J. P., Blackwelder, W. C., Nasirin, D., Farag, T. H., Panchalingam, S., ... Breiman, R. F. (2013). Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study, The Lancet, 382(9888), 209–222. PMID 23680352.
- Lam, V., Chia-Wei, C., Aquino, E., & Han, Y. (2011). Computer keyboard. Retrieved 9 May, 2017, from http://microbewiki.kenyon.edu/index.php/ComputerKeyboard
- Mani, S., Wierzba, T., & Walker, R. I. (2016). Status of vaccine research and development for Shigella, Vaccine, 34(26), 2887–2894. PMID 23680352.
- Marsden, R. (2009). A solid-surfaced infection control computer keyboard (pp. 1–5). P Eng Clean key Inc.
- Meng, J., Doyle, M. P., Zhao, T., & Zhao, S. (2001). Enterohemorrhagic Escherichia coli O157: H7. In M. P. Doyle, L. R. Beuchat, & T. J. Montville (Eds.), Food microbiology: Fundamentals and frontiers (2nd ed., pp. 193–213). Washington, D.C: ASM Press.
- Mims, C., Dockrell, H., Goering, R., Roitt, I., Wakelin, D., & Zuckerman, M. (2004). Medical microbiology, Elsevier Mosby updated (3rd ed., pp. 287).
- Nancy, P., Moreno, P. D., Barbara, Z., Tharp, M. S., Deanne, B., Erdmann, M. S., … Denk, M. A. (2008). The science of microbes, microbes are everywhere. ISBN-13: 978-1-888997-54-5ISBN-10: 1-888997-54-0.
- Nobel, J. (2001). Text book of primary care medicine (3rd ed., pp. 8). St Louis, Mo: Mosby.
- Pope, T. K. C., Ender, P. T., Woek, W. K., et al. (2002). Bacterial contamination of paper currency. Southern Medica Journal, 95, 1408-1410.
- Ryan, K. J., & Ray, C. G. (2004). Sherries medical microbiology; an introduction to infectious diseases (4th ed.). Chapter 48, Candida albicans, pp. 661-663.
- Scott, E., & Bloomfield, S. F. (2008). The survival and transfer of microbial contamination via cloths, hands and utensil. Journal of Applied Microbiology, 68, 271–278.
- Stuart, B. (2005). Infrared spectroscopy. John Wiley & Sons, Inc. Kirk-Othmer Encyclopedia of Chemical Technology.
- Tambekar, D. H., Shirsat, S. D., & Suradkar, S. B. (2007). Prevention of transmission of infectious disease: Studies on hand hygiene in health-care among students in. Continental Journal of Biochemical Science, 1, 6–10.
- WHO. (2002). World Health Report. Geneva. doi:10.1044/1059-0889(2002/er01)
- WHO. (2014). Water. World Health Organization. Retrieved 17 May, 2017, from http://www.who.int/topics/water/en/
- Yabuuchi, E. (2002). Bacillus dysentericus (sic) 1897 was the first taxonomic rather than Bacillus dysenteriae 1898, International Journal of Systematic and Evolutionary Microbiology, 52(Pt 3), 1041. PDMID 12054222.
Appendix
University for Development Studies
Qualitative data for Nyankpala in the Tolon District
Questionnaire for mosque management regarding ablution kettle users''
This survey is aimed at collecting data for the assessment of microbial quality of ablution kettles in Ghana, a case study of Nyankpala in the Tolon District.
Please be assured that any information regarding this research obtained will remain confidential. This survey will take up to a maximum of 15 min.
Note: please provide all the relevant information required by either filling-in the spaces provided or by ticking the appropriate answer to the guided questions in the boxes provided.
1. Name of mosque __________________________________________________________________
2. Age of respondent
<20 □ 21–30 □ 31–40 □ 41–50 □ >51□
3. Sex
Male □ Female □
4. Educational status
Formal education □
No formal education □
Primary School □
Secondary school □
Tertiary □
5. What is your role in the mosque?
Muazzin □
Imam □
Care taker □
Others (Specify) _____________________
6. How long have you been praying in the said mosque
Less than 1 year □
1–3 years □
4–6 years □
7 years or more □
7. Do you provide ablution kettles for public use in your mosque?
Yes □ No □
8. How many ablution kettles do you have in your mosque for public use?
Specify: ____________________
9. a. Gender of users of the ablution kettles
Males □ Females □ Both □
b. Which of the following people make use of the ablution kettle?
Youth □ Children □ Aged □
c. Which of the above categories make the most use of the ablution kettle?
Youth □ Children □ Aged □
10. Approximately how many people pray in your mosque on a daily basis
<20 people □ 20 people □ 30 people □ others □
11. How frequently do people visit your mosque to make use of the ablution kettle?
Once a day □
Twice a day □
Thrice a day □
Four times a day □
Five times a day □
12. Do you observe Friday congregational prayers (Jumu’ah) in your mosque?
Yes □ No □
13. a. Do you normally wash your ablution kettles?
Yes □ No □
b. If YES, How often?
Specify ____________________
14. Do you have a rack on which you store or lock up your ablution kettles?
Yes □ No □
15. How often do you replace your old ablution kettles with new ones?
Thrice a year □
Twice a year □
Once a year □
More than a year □
Others (specify) ____________________
16. Which of the following supporting facilities for ablution do you have at your mosque?
Urinal □ Toilet □ Both □ None □
17. Do you provide any antiseptic or soap for public use in cleaning their hands after visiting any of the washrooms/toilets?
Yes □ No □
18. What is the main water source for your use for ablution in the mosque?
Pipe borne □
Borehole □
Well □
Dam □
Others (specify) _______________________
19. a. Where do you normally store water for public use for ablution?
Overhead tank □ Underground tank □ Barrel/drum □
Others (specify) ____________________
b. Does the water storage facility have a covering or it is always open?
Covered/closed □ Open □
20. a. Do you have any knowledge about bacterial contamination of surfaces?
Yes □ No □
b. If YES, by what means did you acquire that knowledge?
Formal education □
Non-formal education □
Seminar/forum □
Workshop □
Media broadcasts □
Friends and/or Family □
Others (specify) ____________________
21. a. Are you aware that one can contract pathogenic bacteria from the use of a contaminated ablution kettle?
Yes □ No □
b. If YES, Why do you think so?
…………………………………………………………………………………………… …………………………………………………………………………………………… …………………………………………………………………………………………… …………………………………………………………………………………………… …………………………………………………………………………………………… …………………………………………………………………………………………… …………………………………………………………………………………………… ……………………………………………………………………………………………