
Abstract
Dementia-related stigma is a key barrier to people living well with dementia, leading to social isolation and poor well-being. Adolescents represent an under-researched group that will become future carers and healthcare workers for the estimated 83.2 million people who will be living with dementia by 2030. Understanding the factors involved in dementia attitude formation in adolescents is useful for the development of evidence-based anti-stigma initiatives. This study aims to identify predictors of dementia attitudes in adolescents. This is a cross-sectional study using secondary data analysis. 470 participants aged 12–15 years old from secondary schools in the Southeast of England, United Kingdom completed validated questionnaires relating to dementia attitudes (KIDS and Brief A-ADS) as well as demographic information. Multiple regressions were employed as well as a path analysis via a structural equation model to test for direct and mediatory effects. Multiple regression models revealed that being female, having higher levels of contact with dementia, and higher levels of empathy are positively associated with dementia attitudes in adolescents (p<0.05). Within the accepted structural equation model, empathy was a key mediator between contact and dementia attitudes. This study highlights the pivotal role that contact with dementia can have in influencing dementia attitudes in adolescents with empathy serving as a mediator between contact and dementia attitudes. Interventions that use contact should consider how to stimulate empathetic responses to ultimately shape dementia attitudes.
Keywords:
1. Background
There is a need to tackle the challenges faced by the estimated 55.2 million people currently living with dementia globally (Kim et al., Citation2022). Stigma towards people with dementia is widespread and has a profound impact on their lives including leading to barriers in accessing support and impacting the quality of life and well-being (O’Connor, Citation2019). A policy priority outlined by Alzheimer’s Disease International is the need to tackle dementia-related stigma (Prince et al., Citation2016). One such strategy is through anti-stigma and dementia education initiatives designed to improve attitudes in the community (Baker et al., Citation2019; Mukadam & Livingston, Citation2012; World Health Organization, Citation2017). However, before designing evidence-based initiatives, we need to understand what factors are driving dementia-related stigma in the first instance.
Dementia-related stigma refers to the ideology of “public stigma” (Nguyen & Li, Citation2020) and encompasses related terms such as “attitudes”, “stereotypes”, “perceptions”, “beliefs”, and “discrimination” (Corrigan et al., Citation2005). Public stigma can be described as a collection of negative attitudes and beliefs that lead to discrimination and avoidance behaviours towards a group of people and is often interlinked with attitudes (Cheng et al., Citation2011). There are some limited attitude theoretical frameworks applied to dementia-related stigma research (Hebditch et al., Citation2020). One such framework commonly applied in the dementia-related stigma literature is the tripartite model (Pryor & Reeder, Citation2011). The model consists of three main constructs; cognitive (belief), affective (feelings and emotions), and behavioural responses (actions) (Eagly & Chaiken, Citation1995; Pryor & Reeder, Citation2011). These constructs are viewed as what is best captured by attitude measures (Eagly & Chaiken, Citation1993).
There are several factors suggested to be implicated with dementia-related stigma that have been identified within the general public with limited knowledge, limited contact, and being male as some examples (Adefila et al., Citation2015; Cheston et al., Citation2019; Herrmann et al., Citation2018; Werner et al., Citation2013). However, the association between such factors and public attitudes toward dementia (Kim et al., Citation2022) has mostly focused on those above 18 years old. Yet, it is important to recognise that adolescents are also part of the wider society. Not only do adolescents also hold some negative attitudes towards dementia (Farina, Hughes, et al., Citation2020) they also are ideal targets for interventions given theoretical frameworks (e.g., “impressionable year’s hypothesis”) highlighting that the adolescent stage has a key role in attitude formation (Krosnick & Alwin, Citation1989). The impressionable years hypothesis suggests that the period of adolescence is a critical stage in personal and social development with respect to adolescents forming their beliefs. Relationships and social networks experienced during adolescence can impact their own attitudes and beliefs and shape their worldviews (Krosnick & Alwin, Citation1989).
One key gap in the literature is the lack of consensus over factors associated with dementia-related stigma in adolescents. For example, some evidence shows that males hold more negative attitudes toward dementia than females (Farina, Hughes, et al., Citation2020; Lo et al., Citation2020) but this has not always been reported (Cheston et al., Citation2016; Felc et al., Citation2021; Shulman & Adams, Citation2002). These differences could be attributed to mediating factors, such as empathy, which develops later in males than females (Herrmann et al., Citation2018; Lo et al., Citation2020). However, our understanding of such associations is limited due to a lack of data and the tendency to adopt unvalidated outcome measures (Felc et al., Citation2021; Isaac et al., Citation2017). Understanding the factors associated with dementia-related stigma in adolescents allows us to better identify at-risk groups such as those most likely to hold stigmatizing attitudes, whilst also allowing stakeholders to deploy evidence-based interventions in the community that are more cost and time effective. For example, the widespread roll-out of dementia awareness programmes (e.g., Dementia Friends) in adolescents can be seen as inherently good, despite evidence of lack of efficacy (Farina, Hughes, et al., Citation2020).
In this study, we aimed to take an exploratory approach to identify what factors are associated with dementia attitudes in an adolescent cohort. In a novel component, we developed a structural equation model (SEM) to ascertain what factors may mediate relationships with attitudes. The adoption of mediation analysis via SEM serves the purpose to ascertain whether factors such as empathy (an underexplored variable quantitatively in the adolescent/dementia-related stigma literature) has a mediatory role in other variables such as contact, a predictor variable. Moreover, to address the under-utilisation of validated outcome measures, this study adopted only measures that have been psychometrically tested in those under 18-year-olds.
2. Methods
2.1. Study design
This is a secondary data analysis of the baseline cross-sectional data collected by Farina, Hughes, et al. (Citation2020).
2.2. Study setting and sample
Participants were required to be between 12–15 years old. There were no formal exclusion criteria. Participants were recruited from three secondary schools geographically close to Brighton and Hove (England). Schools were identified on the basis that they had previously expressed interest in being involved in dementia awareness initiatives.
2.3. Procedure
Schools’ senior staff provided consent for the research to occur within the school and indicated which classes/pupils should be approached for participation. All potential participants were provided with information about the study, and an opportunity to opt-out of participation. All participants received a standard set of measures related to demographic information, experience and knowledge of dementia, and dementia attitudes. Further details about the full procedure are published elsewhere (Farina, Hughes, et al., Citation2020).
2.4. Measures
Demographic variables: Age was assessed as a continuous variable as participants had a narrow age range. Categorical variables such as ethnicity and gender was recoded into dummy variables (ethnicity dichotomized into White British = 1, Non-white British = 0 whilst gender was dichotomized as 0 = female, 1 = male).
Single item about whether participants have heard of the word’s dementia or Alzheimer’s disease before. This consists of the responses: they have heard of either dementia or Alzheimer’s disease, have heard of both terms or have heard of neither.
Level of Contact: Adolescent Level of Contact of Dementia Questionnaire (ALOCD) is a validated measure on the level of contact adolescents have with dementia (Parveen et al., Citation2020). The scale consists of 11 items rated on a 5-point Likert scale that ranges from “1 – Never” to “5 – A great deal”. Higher scores indicate more contact with people with dementia. The measure as a total score demonstrates good internal consistency (α = 0.80) (Parveen et al., Citation2020).
Empathy: The Empathy Questionnaire for Children and Adolescents (EmQue-CA) (Overgaauw et al., Citation2017) is a validated measure of adolescent empathy made up of three subscales; “affective empathy” (ability to be sensitive and derivatively experience the feelings of others), “cognitive empathy” (ability to construct a working model of other individuals’ emotional states) (Reniers et al., Citation2011) and “intention to comfort” (prosocial motivation). The measure consists of 18 items (i.e., “If a friend is sad, I also feel sad”) with each item on a 3-point Likert response scale that ranges between “not true”, “sometimes true” and “often true”. As the three subscales are highly correlated (see supplementary material A for inter-correlation matrix and Cronbach’s Alpha for reliability checks), empathy was computed as a total score. Higher scores indicate higher level of empathy. The scale demonstrated good internal consistency (α = .86). Totals were scored adhering to the guidance of the EmQue-CA syntax (Rieffe et al., Citation2010).
2.5. Outcome variables
The Brief version of the Adolescent Attitudes towards Dementia Scale (brief A-ADS): a shortened version (13 items) (Farina, Griffiths, et al., Citation2020) of the 23-item version of the A-ADS (Griffiths et al., Citation2018). The brief version was selected due to displaying more comprehensive psychometric properties than the 23-item measure. Items (i.e., people with dementia can be creative) are rated on a 5-point Likert scale with the responses ranging between “1 – strongly disagree” and “5 – strongly agree”. Higher scores indicate more positive attitudes towards dementia. The measure has good internal consistency (α = 0.82) (Griffiths et al., Citation2018). Reverse scoring was applied to two items of the measure with scoring calculated in accordance with the brief A-ADS syntax.
The Kids Insight into Dementia Survey (KIDS): a validated measure that measures children’s perceptions of dementia through 14 items that capture three constructs “personhood”, “stigma” and “dementia understanding” (Baker, Low, et al., Citation2018). Each item (i.e., spending time with people with dementia can be fun) is on a 5-point Likert scale with the response scale ranging between “5 – agree a lot” to “1 – disagree a lot”. Higher scores indicate more positive attitudes and understanding of dementia. The KIDS demonstrated good internal consistency (α = 0.77). Reverse scoring was applied to six items of the measure with scoring calculated in accordance with the KIDS syntax.
2.6. Data analysis
SPSS (version 26) (IBM, New York, USA) was used to analyse the data. Insufficient error responding (IER) was handled using the maximum Longstring index. This is where the maximum number of consecutive values were calculated for items within the KIDS and brief A-ADS. All cases two standard deviations above the mean were excluded from the analysis (Meade & Craig, Citation2012).
The brief A-ADS and the KIDS underwent reverse coding for negatively worded items and then the total scores for these measures were summed. The ALOCD items were summed into a total score as was the case for the EmQue-Ca. A missing values analysis was used to detect whether data were missing at random (p > 0.05). Extreme outliers were excluded if they fell outside the interquartile ranges of −1.5 and + 1.5. Multiple imputation (MI) was used to handle missing data and was selected to retain statistical power of the sample size (Harel et al., Citation2014). Descriptive statistics, checks for normality and cross-tabulations were obtained. Categorical variables were recoded into dummy variables (e.g. White British = 1, Non-white British = 0).
A multivariate linear regression was used to assess which variables (age, gender, contact, empathy, ethnicity, and whether participants have heard of dementia or Alzheimer’s disease before) were associated with dementia attitudes. The variables were entered simultaneously into the models with the Brief A-ADS or KIDS as the dependent variable. Assumptions to run the regression were met (Durbin-Watson statistic values were all between 1.5 and 2.5, plots and multicollinearity were checked with the VIF values less than ten). An alpha of 0.05 was used to denote statistical significance.
To build an exploratory model to determine model fit (Grønneberg & Foldnes, Citation2018), a non-recursive path analysis via a SEM using the maximum likelihood estimation (CB-SEM) was used to explore direct and indirect (mediation) effects between factors. The exploratory model incorporates the empathy-altruism hypothesis (Batson et al., Citation1991) in which empathy towards a stigmatized group may change attitudes (Batson et al., Citation2002).
The SEM had four stages. This included, testing a measurement model to optimize and check for misspecifications of the model, model identification to assess initial model fit modifications to the preliminary model, model fitting and checking for directionality (direct effects), and lastly, obtaining specific indirect effects by creating parameter paths. The factors included in the model building were decided by the factors that were the strongest predictors in the regressions as well as the wider theorised relationships in the literature. The data were analysed on the IBM SPSS Amos Graphics (version 28) (IBM, New York, USA). See supplementary material B for further methodology details relating to the SEM. A bootstrapping procedure (100,000 samples) was applied due to having non-normal data (Nevitt & Hancock, Citation2001). Standardizing coefficients can be misleading when distributions vary between variables (Wang et al., Citation2019; Willett et al., Citation1998). Therefore, unstandardized coefficient betas as well as standardized coefficients, standard error (s.e.) and bias corrected CI (95%) are reported. Bias corrected confidence intervals (BsCI) were obtained (100,000 samples at 95% CI) (Efron, Citation1987) for the direct and indirect effects for the CB-SEM (Cheung & Lau, Citation2008) and to obtain more accurate estimations of the lower and upper limits of the CI (Wagstaff et al., Citation2009). A Bollen-Stine bootstrap was also utilised to obtain a goodness-of-fit statistic to provide the model fit (p value above 0.05 indicates good fit) (Corrêa Ferraz et al., Citation2022). Supplementary material C outlines the indexes used as indicators of the model fit (Resnick et al., Citation2022).
3. Results
There were 470 students recruited at baseline with 432 students remaining in the analysis after data cleaning. The Little’s MCAR test (missing values analysis) found that data was missing at random, χ2 (170) = 166.158, p > 0.05. Participants were on average 12.6 years old (SD. = 0.78), female (55.6%) and predominantly White British (75.7%). See Table for further details.
Table 1. Descriptive statistics of participants (n = 432)
3.1. Regression models: dementia attitudes
Six variables were entered into the multivariate regression model (empathy, age, ethnicity, contact, whether participants have heard of Alzheimer’s disease or dementia before, and gender). The model revealed a significant fit where the brief A-ADS was the outcome, F(6, 425) = 16.176, p < 0.001. A small but significant amount of variance in the brief A-ADS scores was explained by the model fit, R2 adjusted = .174. Within the model, increased empathy (β = .21, p < .001), higher levels of contact (β = .32, p < 0.001) and being female (β = −.12, p = .02) significantly predicted the brief A-ADS scores. Within the model, males denoted significantly poorer attitudes.
In the case of the KIDS scores as the outcome, the model also fitted significantly, F(6, 425) = 18.660, p < 0.001. A small but significant amount of variance in the KIDS scores was explained by the model fit, R2 adjusted = .197. Within the model, higher levels of contact (β = .39, p < 0.001) and increased empathy (β = .13, p = .00) significantly predicted KIDS scores. Table provides the multivariate linear regression for the brief A-ADS and the KIDS.
Table 2. Multiple linear regression for variables predicting Brief A-ADS and the KIDS attitude scores
Comparison between imputed data versus the raw data are provided in supplementary material D.
3.2. Structural equation model
Due to the lack of support for the factors, age, ethnicity and whether participants have heard of dementia or Alzheimer’s disease, these variables were not included in the SEM. The measurement SEM and its specifications are reported in supplementary materials E and F.
The exploratory SEM suggested the overall fit of the model was very good with several indicators of a very close fit, χ2(2) = 3.999, p = .14, CMIN/DF = 2.00, CFI = .99, GFI = 1.00, AGFI = .97, TLI = .97, RMSEA = .05, Pclose = .41. The Bollen-Stine (p = .21) suggested that goodness of fit of the model was good. Figure displays the accepted model.
Figure 1. SEM exploratory model (accepted model) with standardized coefficients.
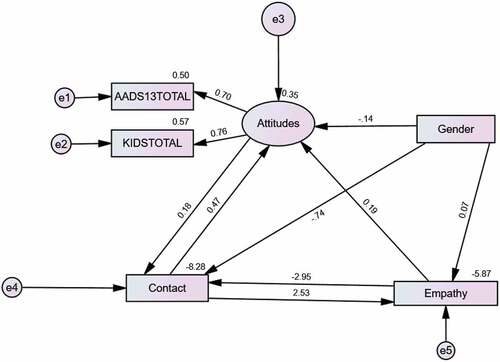
There was a significant direct effect observed between all paths: gender on attitudes (p = .01), gender on empathy (p = .00), gender on contact (p = .00), empathy on attitudes (p < .001), contact on attitudes (p < .001), contact on empathy (p = .00) and empathy on contact (p = .00). Table reports the coefficients and confidence intervals.
Table 3. Direct effects of the accepted model
All indirect pathways were statistically significant (p = .00): attitudes was a mediator between empathy and contact (empathy > attitudes > contact), contact was a mediator between gender and attitudes (gender > contact > attitudes), contact was a mediator between attitudes and empathy (attitudes > contact > empathy), contact was a mediator between empathy and attitudes (empathy > contact > attitudes), and empathy was a mediator between contact and attitudes (contact > empathy > attitudes). Table reports the coefficients for the mediation effects.
Table 4. Mediation effects of the accepted model
4. Discussion
This is the first study to explore factors associated with dementia related stigma outcomes in adolescents using SEM. This study highlights that empathy, gender and contact are potential contributors to dementia attitudes. Whilst the data highlights some potential contributors to dementia attitudes, causality cannot be obtained due to the cross-sectional and observational nature of the analyses and data. The SEM further provides us with a better understanding about how these factors may interact together in influencing dementia attitudes in adolescents.
Several findings from this study are also consistent with what is reported in the adolescent literature and our broader understanding of dementia attitudes, mental illness and aging. As such, our findings revealed that males displayed significantly poorer attitudes towards dementia than females, which concur with other research (Blay & Peluso, Citation2010; Farina, Hughes, et al., Citation2020; Lo et al., Citation2020). A possible explanation for these findings draws on the potential developmental and empathetic maturity differences between males and females at various stages of adolescence (Van der Graaff et al., Citation2018). Our findings suggest that gender may have a direct effect on empathy which supports this explanation. Research also suggests that more contact with people with dementia amongst female adolescents may improve attitudes (Isaac et al., Citation2017). Evidence from studies have found that female adolescents have higher levels of contact with people with dementia than males (Cheston et al., Citation2019; Farina, Hughes, et al., Citation2020). Our indirect pathway (gender > contact > attitudes) was statistically significant, thus indicating that the gender effect on dementia attitudes may be driven, in part, by increased contact.
The study provides an early indication that modifiable factors such as contact with people with dementia are potential useful targets for anti-stigma initiatives. Increased contact and education are common anti-stigma approaches within the broader stigma literature (Cook et al., Citation2014). Our findings are in line with other studies that report an association between contact and dementia-related stigma, quantitatively (Cheston et al., Citation2016; Werner et al., Citation2017) and qualitatively (Baker, Jeon, et al., Citation2018; Felc et al., Citation2021). The SEM demonstrates that empathy likely has an important mediating role in adolescents’ dementia attitudes. As there are a limited number of quantitative studies on the association between empathy and dementia attitudes in adolescents, this study addresses this gap, further consolidating our notion that adolescents may be an ideal age group to target for initiatives. This is supported by adolescent developmental theory that suggests components of empathy such as prosocial development is at a peak between the ages of 13 and 16 years old (Eisenberg et al., Citation2016; Silke et al., Citation2018).
Whilst our findings indicate the potential role of contact on dementia attitudes, our findings do not indicate whether it is direct contact or indirect contact that is most important in its influence amongst adolescents. Future work could investigate how these components of contact influence the model. Furthermore, research has suggested that quality over quantity of contact may be more important in changing stereotypes (Brouwer & Boros, Citation2010). However, the quality of contact is not captured in this study.
In our study, we found that empathy and contact both had a mediatory effect on attitudes. It is therefore reasonable to suspect that initiatives employing one without the other may not be strong enough by itself to change stereotypes. This is supported by Allport (1954) who argued that contact alone may not be enough to change stereotypes with evidence from the broader adolescent disability literature finding that greater empathy was a partial mediator between contact and attitudes and that empathy was an important factor to consider when developing interventions based on contact (Armstrong et al., Citation2015). While prior research has questioned to what extent the relationship between contact and empathy is reciprocal (Barbot & Kaufman, Citation2020), there is evidence from intervention studies where contact has the potential to enhance empathy in a dementia virtual reality program (Adefila et al., Citation2015). Likewise, intergroup contact led to increased empathy in another program, supporting the stance that empathy may be malleable in nature (Barbot & Kaufman, Citation2020). Pragmatically, facilitating meaningful contact between people with dementia and young people may be difficult due to red tape. Virtual reality (VR) could be one way to tap into empathy (Schutte & Stilinović, Citation2017) without having direct contact with a person with dementia. A positive impact on attitudes may be possible through challenging stereotypes of dementia within the VR (e.g., inter-generational video gaming) (Makri & Tsolaki, Citation2022) which foster positive portrayals of dementia. Adopting VR would be appealing to young populations (Hicks et al., Citation2021) but would come at the cost of losing the voice of people with dementia.
The WHO’s global action plan on the public health response to dementia 2017–2025 outlines the need to tackle the stigma towards dementia among the general population by improving the societal conditions for those living with dementia (O’Connor, Citation2019). Our findings provide a mechanism to tackle stigma towards dementia in adolescents, enabling for an evidence-based anti-stigma policy and interventions to be developed. Whilst our research was focussed on an adolescent sample, we should also be aware that in improving attitudes in young people may ultimately have a more widespread benefit to society. Adolescents engaging with their parents could act as a catalyst to change parental values (Knafo & Galansky, Citation2008) or improve knowledge through intergenerational learning (Soto‐Perez‐de‐Celis et al., Citation2017). However, further research is needed to understand the efficacy of such transmission. The translational implications of this study include providing a foundation to develop effective initiatives that is rooted in evidence in our public health efforts to reduce dementia-related stigma in the general population.
There are some limitations to consider for this study. First, the cross-sectional nature of the study limits what causal inferences we can make about the data with statistical associations not necessarily equating to meaningful associations (Kafadar, Citation2021). As all the data are cross-sectional, it is difficult to truly identify how variables influence each other. The cross-sectional design is however useful in the context of this study as it enabled the exploratory establishment of relatedness of several variables (Spector, Citation2019). Second, inclusion of the independent variables within the model only accounted for 17–20% percent of the variance of dementia attitudes, indicated that there are other unobserved variables. Future work will be needed to establish more complex models that include other variables such as quality of contact and level of knowledge. Third, participants in our study are relatively homogenous in terms of ethnicity (75% white British). Our findings indicate that there was no association between ethnicity and dementia attitudes, which differs from previous literature (Cheston et al., Citation2016; Werner et al., Citation2017). A more granular focus on different ethnic groups could help better understand these findings. It is also worth noting that the sample may not wholly represent older adolescents’ attitudes given the mean age of participants was 12.6 years old. Lastly, the conceptual development of the brief A-ADS and KIDS are different, and therefore may capture slightly different underlying factors. For example, items on the brief A-ADS appear to capture elements of prosocial responding and empathetic concern (i.e., “If I saw someone with dementia struggling to do something, I would help them”) whilst the KIDS items capture more affective elements (i.e., “I would feel a bit scared if I met someone with dementia on the street”). The consistency of strength and direction of associations across the brief A-ADS and KIDS, however, provides reassurance that they capture overlapping domains.
5. Conclusion
The purpose of this study was to determine what factors are associated with dementia attitudes in adolescents and establish a model fit to the data in an exploratory capacity. Empathy and contact both appear to be key mediators of dementia attitudes within the SEM. These factors should be explored in more heterogenous samples, whilst longitudinal research will better allow for us to interpret the temporal nature of empathy development and attitude change. At present, it appears that empathy and contact are factors that may be useful targets for anti-stigma and dementia awareness initiatives for adolescents.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Esra Hassan
Esra Hassan is a PhD student at Brighton and Sussex Medical School with her research on the determinants of dementia attitudes in young people. With an MSc in Clinical Neuroscience, Esra’s research background spans across memory and neuropsychology, molecular cancer biology, and neuroimaging techniques. Esra has worked closely with schools and young people in recent years through outreach and public engagement work on brain health and dementia and developing her expertise in delivering tailored interventions to young people.
Ben Hicks
Dr Ben Hicks is a Research Fellow and the Co-ordinator of the ESRC/NIHR funded DETERMIND research programme. This is a 5-year longitudinal study, led by BSMS, that seeks to examine and address the inequalities and inequities in the post-diagnostic care pathway for newly diagnosed people with dementia and their care partners. Dr Hicks research concerns supporting quality of life and social inclusion in people with dementia by exploring their differing lived experiences of the condition and addressing the inequalities that may arise in the dementia care pathway.
Naji Tabet
Professor Naji Tabet, Professor in Dementia and Old Age Psychiatry, is the Director of the Centre for Dementia Studies (CDS). Prof Tabet also leads the Dementia Theme at the NIHR Applied Research Collaboration (ARC) KSS. Prof Tabet is also the Dementia Speciality Co-Lead for NIHR Clinical Research Network (CRN) KSS. Prof Tabet has also been the Principal and UK Chief Investigator on over 35 Phase II-IV therapeutic and diagnostic clinical trials in dementia.
Nicolas Farina
Dr Nicolas Farina is an associate Professor at the University of Plymouth. Dr Farina has a PhD in psychology from the University of Sussex, in which he explored the effects of physical activity on the executive decline of people with dementia. Dr Farina has a wide range of research interest areas that seek to improve the lives of people with dementia and their carers. Dr Farina whilst at the Brighton and Sussex Medical School as a senior research fellow, developed an expertise in dementia-related stigma, working both within the UK and internationally and co-ordinating two work packages on the STRiDE project.
References
- Adefila, A., Graham, S., Clouder, L., Bluteau, P., Ball, S., & Basset, T. (2015). myShoes–the future of experiential dementia training? The Journal of Mental Health Training, Education and Practice, 11(2), 91–12. https://doi.org/10.1108/JMHTEP-10-2015-0048
- Armstrong, M., Morris, C., Abraham, C., Ukoumunne, O. C., & Tarrant, M. (2015). Children’s contact with people with disabilities and their attitudes towards disability: A cross-sectional study. Disability and Rehabilitation, 38(9), 879–888. https://doi.org/10.3109/09638288.2015.1074727
- Baker, J. R., Goodenough, B., Jeon, Y.-H., Bryden, C., Hutchinson, K., & Low, L.-F. (2019). The Kids4Dementia education program is effective in improving children’s attitudes towards dementia. Dementia, 18(5), 1777–1789. https://doi.org/10.1177/1471301217731385
- Baker, J. R., Jeon, Y.-H., Goodenough, B., Low, L.-F., Bryden, C., Hutchinson, K., & Richards, L. (2018). What do children need to know about dementia? The perspectives of children and people with personal experience of dementia. International Psychogeriatrics, 30(5), 673–684. https://doi.org/10.1017/S1041610217002022
- Baker, J. R., Low, L.-F., Goodenough, B., Jeon, Y.-H., Tsang, R. S. M., Bryden, C., & Hutchinson, K. (2018). The Kids Insight into Dementia Survey (KIDS): Development and preliminary psychometric properties. Aging & Mental Health, 22(8), 947–953. https://doi.org/10.1080/13607863.2017.1320703
- Barbot, B., & Kaufman, J. C. (2020). What makes immersive virtual reality the ultimate empathy machine? Discerning the underlying mechanisms of change. Computers in Human Behavior, 111, 106431. https://doi.org/10.1016/j.chb.2020.106431
- Batson, C. D., Batson, J. G., Slingsby, J. K., Harrell, K. L., Peekna, H. M., & Todd, R. M. (1991). Empathic joy and the empathy-altruism hypothesis. Journal of Personality and Social Psychology, 61(3), 413. https://doi.org/10.1037/0022-3514.61.3.413
- Batson, C. D., Chang, J., Orr, R., & Rowland, J. (2002). Empathy, attitudes, and action: Can feeling for a member of a stigmatized group motivate one to help the group? Personality and Social Psychology Bulletin, 28(12), 1656–1666. https://doi.org/10.1177/014616702237647
- Blay, S., & Peluso, E. T. P. (2010). Public stigma: The community’s tolerance of Alzheimer disease. The American Journal of Geriatric Psychiatry: Official Journal of the American Association for Geriatric Psychiatry. https://doi.org/10.1097/JGP.0b013e3181bea900
- Brouwer, M. A., & Boros, S. (2010). The influence of intergroup contact and ethnocultural empathy on employees’ attitudes toward diversity. Cognition, Brain, Behavior, 14(3), 243–260.
- Cheng, S. T., Lam, L. C., Chan, L. C., Law, A. C., Fung, A. W., Chan, W. C. & Chan, W. M. (2011). The effects of exposure to scenarios about dementia on stigma and attitudes toward dementia care in a Chinese community. International Psychogeriatrics, 23(9), 1433–1441. https://doi.org/10.1017/S1041610211000834
- Cheston, R., Hancock, J., & White, P. (2016). A cross-sectional investigation of public attitudes toward dementia in Bristol and South Gloucestershire using the approaches to dementia questionnaire. International Psychogeriatrics, 28(10), 1717–1724. https://doi.org/10.1017/S1041610216000843
- Cheston, R., Hancock, J., & White, P. (2019). Does personal experience of dementia change attitudes? The bristol and South Gloucestershire survey of dementia attitudes. Dementia, 18(7–8), 2596–2608. https://doi.org/10.1177/1471301217752707
- Cheung, G. W., & Lau, R. S. (2008). Testing mediation and suppression effects of latent variables: Bootstrapping with structural equation models. Organizational Research Methods, 11(2), 296–325. https://doi.org/10.1177/1094428107300343
- Cook, J. E., Purdie-Vaughns, V., Meyer, I. H., & Busch, J. T. (2014). Intervening within and across levels: A multilevel approach to stigma and public health. Social Science & Medicine, 103, 101–109. https://doi.org/10.1016/j.socscimed.2013.09.023
- Corrêa Ferraz, R., Maydeu-Olivares, A., & Shi, D. (2022). Asymptotic is better than bollen-stine bootstrapping to assess model Fit: The effect of model size on the chi-square statistic. Structural Equation Modeling: A Multidisciplinary Journal, 29(5), 731–743. https://doi.org/10.1080/10705511.2022.2053128
- Corrigan, P. W., Kerr, A., & Knudsen, L. (2005). The stigma of mental illness: Explanatory models and methods for change. Applied and Preventive Psychology, 11(3), 179–190. https://doi.org/10.1016/j.appsy.2005.07.001
- Eagly, A. H., & Chaiken, S. (1993). The psychology of attitudes. Harcourt brace Jovanovich college publishers.
- Eagly, A. H., & Chaiken, S. (1995). Attitude strength, attitude structure, and resistance to change. Attitude Strength: Antecedents and Consequences, 4(2), 413–432.
- Efron, B. (1987). Better bootstrap confidence intervals. Journal of the American Statistical Association, 82(397), 171–185. https://doi.org/10.1080/01621459.1987.10478410
- Eisenberg, N., VanSchyndel, S. K., & Spinrad, T. L. (2016). Prosocial motivation: Inferences from an opaque body of work. Child Development, 87(6), 1668–1678. https://doi.org/10.1111/cdev.12638
- Farina, N., Griffiths, A. W., Hughes, L. J., & Parveen, S. (2020). Measuring adolescent attitudes towards dementia: The revalidation and refinement of the A-ADS. Journal of Health Psychology, 27(2), 374–385. https://doi.org/10.1177/1359105320953479
- Farina, N., Hughes, L. J., Griffiths, A. W., & Parveen, S. (2020). Adolescents’ experiences and perceptions of dementia. Aging & Mental Health, 24(7), 1175–1181. https://doi.org/10.1080/13607863.2019.1613343
- Farina, N., Hughes, L. J., Jones, E., Parveen, S., Griffiths, A. W., Galvin, K., & Banerjee, S. (2020). The effect of a dementia awareness class on changing dementia attitudes in adolescents. BMC Geriatrics, 20(1), 188. https://doi.org/10.1186/s12877-020-01589-6
- Felc, B., Leskošek, V., & Felc, Z. (2021). Teaching dementia in secondary schools to create dementia friendly generation. International Journal of Psychiatry Research, 4(1), 1–9. https://doi.org/10.33425/2641-4317.1088
- Griffiths, A. W., Parveen, S., Shafiq, S., & Oyebode, J. R. (2018). Development of the Adolescent Attitudes towards Dementia Scale (A-ADS). International Journal of Geriatric Psychiatry, 33(8), 1139–1145. https://doi.org/10.1002/gps.4907
- Grønneberg, S., & Foldnes, N. (2018). Testing model fit by bootstrap selection. Structural Equation Modeling: A Multidisciplinary Journal, 26(2), 182–190. https://doi.org/10.1080/10705511.2018.1503543
- Harel, O., Perkins, N., & Schisterman, E. F. (2014). The use of multiple imputation for data subject to limits of detection. Sri Lankan Journal of Applied Statistics, 5(4), 227. https://doi.org/10.4038/sljastats.v5i4.7792
- Hebditch, M., Daley, S., Wright, J., Sherlock, G., Scott, J., & Banerjee, S. (2020). Preferences of nursing and medical students for working with older adults and people with dementia: A systematic review. BMC Medical Education, 20(1), 1–11. https://doi.org/10.1186/s12909-020-02000-z
- Herrmann, L. K., Welter, E., Leverenz, J., Lerner, A. J., Udelson, N., Kanetsky, C., & Sajatovic, M. (2018). A systematic review of dementia-related stigma research: Can we move the stigma dial? The American Journal of Geriatric Psychiatry: Official Journal of the American Association for Geriatric Psychiatry, 26(3), 316–331. https://doi.org/10.1016/j.jagp.2017.09.006
- Hicks, B., Konovalova, I., Myers, K., Falconer, L., & Board, M. (2021). Taking ‘A walk through dementia’: Exploring care home practitioners’ experiences of using a virtual reality tool to support dementia awareness. Ageing & Society, 43(5), 1042–1067. https://doi.org/10.1017/S0144686X21000994
- Isaac, M., Isaac, M., Farina, N., & Tabet, N. (2017). Knowledge and attitudes towards dementia in adolescent students. Journal of Mental Health, 26(5), 419–425. https://doi.org/10.1080/09638237.2016.1207234
- Kafadar, K. (2021). Editorial: Statistical significance, P-values, and replicability. The Annals of Applied Statistics, 15(3), 15(3. https://doi.org/10.1214/21-AOAS1500
- Kim, S., Anstey, K. J., Mortby, M. E., & Williams, K. N. (2022). Who displays dementia-related stigma and what does the general public know about dementia? Findings from a nationally representative survey. Aging & Mental Health, 1–10. https://doi.org/10.1080/13607863.2022.2126819
- Knafo, A., & Galansky, N. (2008). The influence of children on their parents’ values. Social and Personality Psychology Compass, 2(3), 1143–1161. https://doi.org/10.1111/j.1751-9004.2008.00097.x
- Krosnick, J. A., & Alwin, D. E. (1989). Aging and susceptibility to attitude change. Journal of Personality & Social Psychology, 10(3), 416–425. https://doi.org/10.1037/0022-3514.57.3.416
- Lo, I., Zeng, W., Lei, C. I., Lam, C., & Lou, H. L. (2020). Knowledge, attitude and preventive practice on dementia care among primary health professionals in Macao. The Journal of Prevention of Alzheimer’s Disease. https://doi.org/10.14283/jpad.2020.10
- Makri, M., & Tsolaki, M. (2022, June). Innovative Serious Games for people with dementia developed through intergenerational interventions The “Bridge” project: A European Innovative Approach. Proceedings of the 15th International Conference on PErvasive Technologies Related to Assistive Environments, Corfu, Greece (pp. 678–682).
- Meade, A. W., & Craig, S. B. (2012). Identifying careless responses in survey data. Psychological Methods, 17(3), 437. https://doi.org/10.1037/a0028085
- Mukadam, N., & Livingston, G. (2012). Reducing the stigma associated with dementia: Approaches and goals. Aging Health, 8(4), 377–386. https://doi.org/10.2217/ahe.12.42
- Nevitt, J., & Hancock, G. R. (2001). Performance of bootstrapping approaches to model test statistics and parameter standard error estimation in structural equation modeling. Structural Equation Modeling, 8(3), 353–377. https://doi.org/10.1207/S15328007SEM0803_2
- Nguyen, T., & Li, X. (2020). Understanding public-stigma and self-stigma in the context of dementia: A systematic review of the global literature. Dementia (London, England), 19(2), 148–181. https://doi.org/10.1177/1471301218800122
- O’Connor. (2019). Alzheimer’s disease international world alzheimer report 2019: attitudes to dementia. 14–17.
- Overgaauw, S., Rieffe, C., Broekhof, E., Crone, E. A., & Güroğlu, B. (2017). Assessing empathy across childhood and adolescence: Validation of the Empathy Questionnaire for Children and Adolescents (EmQue-CA). Frontiers in Psychology, 8, 870. https://doi.org/10.3389/fpsyg.2017.00870
- Parveen, S., Griffiths, A. W., & Farina, N. (2020). The development and validation of the adolescent level of contact with dementia scale. International Journal of Geriatric Psychiatry, 35(10), 1134–1140. https://doi.org/10.1002/gps.5335
- Prince, M., Bryce, R., Albanese, E., Wimo, A., Ribeiro, W., & Ferri, C. P. (2016). The global prevalence of dementia: A systematic review and metaanalysis. Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, 9(1), 63–75.e2. https://doi.org/10.1016/j.jalz.2012.11.007
- Pryor, J. B., & Reeder, G. D. (2011). HIV-related stigma. In B. Hall, J. Hall, & C. Cockerell (Eds.), HIV/AIDS in the Post-HAART Era: Manifestations, Treatment and Epidemiology (pp. 790–806). Shelton, Connecticut: PMPH-USA, Ltd.
- Reniers, R. L., Corcoran, R., Drake, R., Shryane, N. M., & Völlm, B. A. (2011). The QCAE: A questionnaire of cognitive and affective empathy. Journal of Personality Assessment, 93(1), 84–95. https://doi.org/10.1080/00223891.2010.528484
- Resnick, B., Galik, E., Kolanowski, A., VanHaitsma, K., Boltz, M., Zhu, S., & Dorsey, S. G. (2022). The relationship between pain, function, behavioral, and psychological symptoms of dementia and quality of life. Pain Management Nursing, 23(1), 55–61. https://doi.org/10.1016/j.pmn.2021.07.001
- Rieffe, C., Ketelaar, L., & Wiefferink, C. H. (2010). Assessing empathy in young children; construction and validation of an Empathy Questionnaire (EmQue). Personality and Individual Differences, 49(5), 362–367. https://doi.org/10.1016/j.paid.2010.03.046
- Schutte, N. S., & Stilinović, E. J. (2017). Facilitating empathy through virtual reality. Motivation and Emotion, 41(6), 708–712. https://doi.org/10.1007/s11031-017-9641-7
- Shulman, N., & Adams, B. (2002). A comparison of Russian and British attitudes towards mental health problems in the community. International Journal of Social Psychiatry, 48(4), 266–278. https://doi.org/10.1177/002076402128783307
- Silke, C., Brady, B., Boylan, C., & Dolan, P. (2018). Factors influencing the development of empathy and pro-social behaviour among adolescents: A systematic review. Children and Youth Services Review, 94, 421–436. https://doi.org/10.1016/j.childyouth.2018.07.027
- Soto‐Perez‐de‐Celis, E., Smith, D. D., Rojo‐Castillo, M. P., Hurria, A., Pavas‐Vivas, A. M., Gitler‐Weingarten, R., Mohar, A., & Chavarri-Guerra, Y. (2017, October). Implementation of a school‐based educational program to increase breast cancer awareness and promote intergenerational transmission of knowledge in a Rural Mexican community. The Oncologist, 22(10), 1249–1256. https://doi.org/10.1634/theoncologist.2017-0063
- Spector, P. E. (2019). Do not cross me: Optimizing the use of cross-sectional designs. Journal of Business and Psychology, 34(2), 125–137. https://doi.org/10.1007/s10869-018-09613-8
- Van der Graaff, J., Carlo, G., Crocetti, E., Koot, H. M., & Branje, S. (2018). Prosocial behavior in adolescence: Gender differences in development and links with empathy. Journal of Youth and Adolescence, 47(5), 1086–1099. https://doi.org/10.1007/s10964-017-0786-1
- Wagstaff, D. A., Elek, E., Kulis, S., & Marsiglia, F. (2009). Using a nonparametric bootstrap to obtain a confidence interval for Pearson’sr with cluster randomized data: A case study. The Journal of Primary Prevention, 30(5), 497–512. https://doi.org/10.1007/s10935-009-0191-y
- Wang, L., Zhang, Q., Maxwell, S. E., & Bergeman, C. S. (2019). On standardizing within-person effects: Potential problems of global standardization. Multivariate Behavioral Research, 54(3), 382–403. https://doi.org/10.1080/00273171.2018.1532280
- Werner, P., Goldberg, S., Mandel, S., & Korczyn, A. (2013). Gender differences in lay persons’ beliefs and knowledge about Alzheimer’s Disease (AD): A national representative study of Israeli adults. Archives of Gerontology and Geriatrics, 56(2), 400–404. https://doi.org/10.1016/j.archger.2012.11.001
- Werner, P., Jabel, H. A., Reuveni, Y., & Prilutzki, D. (2017). Stigmatic beliefs toward a person with Alzheimer’s Disease among high-school students: Does majority-minority status make a difference? Educational Gerontology, 43(12), 609–618. https://doi.org/10.1080/03601277.2017.1376461
- Willett, J. B., Singer, J. D., & Martin, N. C. (1998). The design and analysis of longitudinal studies of development and psychopathology in context: Statistical models and methodological recommendations. Development and Psychopathology, 10(2), 395–426. https://doi.org/10.1017/S0954579498001667
- World Health Organization. (2017). Global action plan on the public health response to dementia 2017–2025. Alzheimer's Disease International.