
Abstract
3D deformity of the spine-like scoliosis is commonly assessed using stereo-radiographic technique. The Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) modelling fail in this case, as they are obtained with the patient in sleeping position. Also, they are associated with heavy cost and radiation hazards. We have developed two models namely, feature-based model and a Combined Stereo-Corresponding Point And Geometric (CSCPG) model for 3D spine reconstruction using biplanar x-rays. The spinal disorder is quantified using two parameters, namely axial vertebral rotation and spinal curvature using both these methods. Their performance is compared by considering Non-Stereo-Corresponding Point (NSCP) model as the gold standard method. The feature-based model is less accurate compared to the CSCPG model. The performance of the feature-based model is also poor in the case of deformity quantification. A statistical significance test is conducted in order to verify its suitability in diagnosis of the spinal disorders. The accuracy of feature-based model can be improved by incorporating additional landmark features from the biplanar radiographs. The proposed CSCPG model has accuracy closer to the gold standard technique and can be used a diagnostic tool for the spinal disorders.
PUBLIC INTEREST STATEMENT
The human spine is made up of complex anatomical structures. Therefore, pathological deformations of the spine are difficult to diagnose using x-rays. The advanced 3D imaging modalities like CT and MRI have limitations on assessment of 3D spinal deformities as they are obtained in supine position. The supine position can change the actual deformation. Although CT can provide more information for the deformity assessment, the subjects are exposed to higher levels of radiation. Since the subjects with spinal deformities may have implants and corrective tools, MRI cannot be used. Hence, stereo-radiography is the most widely used technique for 3D reconstruction of the human spine. We have developed two stereo-radiographic methods, namely, Feature-based Model and Combined Stereo-Corresponding Point and Geometric (CSCPG) model. The performance of these methods is compared with respect to a gold standard method. The proposed CSCPG model has accuracy closer to the gold standard technique and can be used a diagnostic tool for the spinal disorders.
1. Introduction
The deformities of the human spine are three dimensional (3D) in nature. They are diagnosed wrongly using biplanar x-rays which give only a projection of the actual deformation (Boisvert, Cheriet, & Pennec, Citation2008). The advanced diagnostic methods like Computed Tomography (CT) or Magnetic Resonance Imaging (MRI) has limited application in the case of spinal disorders. This is due to the fact that they are acquired from the subject in sleeping position (Seoud, Cheriet, Labelle, & Dansereau, Citation2011). Since the patient has to undergo repeated follow-up examinations, CT scans cannot be used due to the radiation hazards (Aubin et al., Citation1997). The MRI scan cannot be used in the post-surgery examinations due to the presence of metal implants (Dumas et al., Citation2008). Hence, stereo-radiographic reconstruction is used in which 3D spinal models are developed using biplanar x-rays (Zhang et al., Citation2013). Numerous stereo-reconstruction approaches are proposed in the literature (Daniel, Boisvert, Jorge, Labelle, & Joao Manuel, Citation2011, Mitulescu, Skalli, Mitton, & De Guise, Citation2002; Pomero, Mitton, Laporte, De Guise, & Skalli, Citation2004). Non-stereo-corresponding point (NSCP) reconstruction is considered as the gold standard (Moura & Barbosa, Citation2014). We have developed NSCP models from 10 scoliotic subject data using the method mentioned in Mitton, Landry, Véron, & Skalli (Citation2000). This is used as a reference model for future validation. The subjects used in this study are of the age group 12–16 having an S-shaped scoliotic curves. We have developed feature-based models and combined stereo-corresponding point and geometric (CSCPG) models for these 10 subjects. Feature-based models are obtained by deforming the CAD-based generic models according to the stereo-corresponding point (SCP) reconstruction, whereas the CSCPG models are obtained by deforming biomedical spine models according to SCP reconstruction and the features extracted automatically from the x-rays. The accuracy of reconstruction is measured by back projecting these models on to the radiographs. The spinal curvature and axial vertebral rotation (AVR) of these models are also computed from these models which quantifies the spinal deformities. The accuracy along with the spinal parameters is statistically compared. The accuracy of CSCPG model is closer to the gold standard technique, whereas the accuracy of feature-based model is poor and can be increased by incorporating additional landmarks from the biplanar x-rays. Thus, the most accurate CSCPG model can be used to develop a diagnostic tool for spinal disorders.
2. Methodology
2.1. Feature-based model for spine 3D reconstruction
Feature-based 3D spine model is developed using CATIA V5 software using the data available from a known database (Tan, Teo, & Chua, Citation2004). The parameters used from this database are shown in Figure .
Figure 1. Parameters considered from the standard database (Tan et al., Citation2004 ).
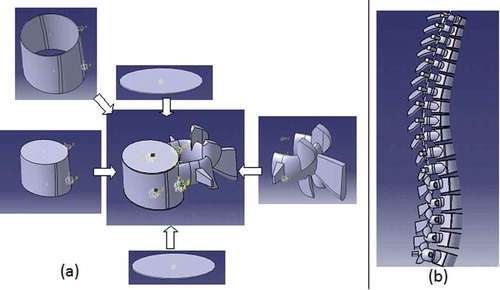
Each vertebra is modelled as an assembly of five parts, namely cancellous core, cortical shell, upper and lower endplate, and posterior elements (Jones & Wilcox, Citation2008) using the specifications given by Tan et al. (Citation2004). The cross-sectional shape of vertebrae is estimated to be elliptical rather than the kidney shape or heart shape. The thickness of cancellous core was taken as 0.40 mm. The cortical shell that covers the cancellous core is approximated to be 0.40 mm. The endplate was also considered to have an elliptical shape with 0.40 mm thickness. In posterior elements, the pedical cross-section was elliptical in nature. The thoracic and lumbar posterior elements were designed separately. The articular process, spinous process, transverse processes is developed using standard specifications. The integration of these parts results in a vertebra. The thoracic and the lumbar vertebral assembly are integrated separately. Then they are integrated together to form the generic spine model. They are assembled using the connectors. This helps to call the endplate of the vertebra using the code and used it as reference. This can be used to set the orientation of that vertebra. They retain continuity of vertebral column when the orientation of vertebra changes. The connectors are the line segments which passes through the endplate centres. Figure ) shows the feature-based model of a lumbar vertebra of the generic model. The assembled generic spine model is shown in Figure ).
Figure 2. Feature-based model (a) L1 vertebra (b) Generic model.
The vertebral orientation features are extracted automatically from biplanar radiographs through several image processing steps. This involves enhancement of the x-rays using multiscale morphological image enhancement technique (Mukhopadhyay & Chanda, Citation2002). Then the contours of the vertebral body are identified automatically using Gradient Vector Flow Snake algorithm (Kass, Witkin, & Terzopoulos, Citation1998). Because of the convergent properties, this algorithm is used. The curve z(s), s ԑ [0, 1] moves according to the Equation (1) using energy minimization function.
Here, β and α are parameters for controlling tension and rigidity, z′ and z″ are first and second derivatives of z. Eext is the external GVF force “u” derived from the image. It is given as solution diffusion equation given in Equation (2).
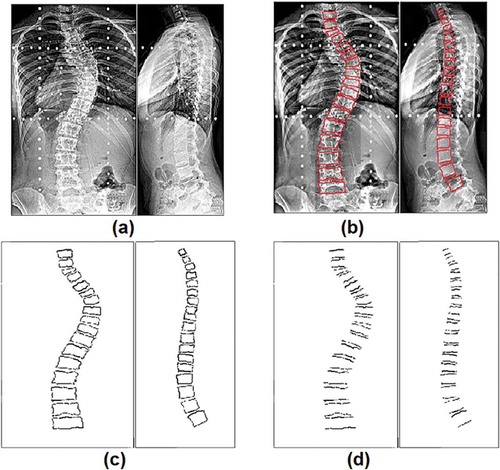
Here, μ is for regulation, k is the edge map image, and δ is the gradient. The Gradient Vector Flow (GVF) snake is capable of convergence. The image is then converted to grayscale using morphological operators. Then the horizontal edges are extracted using a Sobel operator. The orientation of each vertebra is computed using Hough transform (Hough, Citation1962). All these steps are depicted in Figure .
Figure 3. Subject-1 (a) Enhanced x-ray (b) Segmentation (c) Morphological operation (d) Edge extraction.
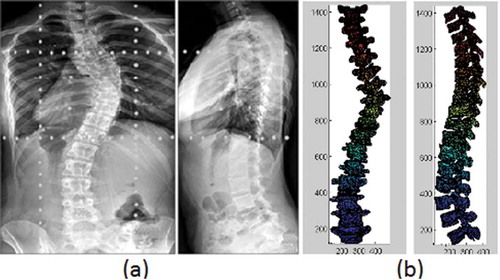
The vertebral orientations are given as an input to the interface which produces subject-specific 3D spine model. This interface is developed using VBA in CATIA. This procedure is described in our earlier work (Kumar, Nayak, & Hareesha, Citation2016). The subject-specific model for subject-1 and corresponding biplanar x-rays are shown in Figure . Similarly, feature-based models are obtained from all the 10 scoliotic subjects.
Figure 4. Subject-1 (a) Biplanar x-rays (b) Feature-based model.
2.2. CSCPG 3D spine modelling
The steps involved in the CSCPG reconstruction are shown in Figure . Using the coronal and sagittal radiographs obtained on a calibration apparatus, this technique performs the 3D modelling of the human spine. The calibration apparatus helps in computing the geometrical parameters of the room in which x-rays are acquired. The acquired images are enhanced using multiscale mathematical morphology (Mukhopadhyay & Chanda, Citation2002). Then pedicle boundaries as well as the vertebral contours are extracted automatically using an active contour modelling technique (Kass et al., Citation1998). From this, vertebral features are semi-automatically extracted using Hough transform (Hough, Citation1962). These features used to deform the SCP model to get the custom-made models of the spine. This process is called a CSCPG reconstruction method. The SCP model is attained using deformation of the generic spine model according to the SCPs available on the biplanar x-rays using the technique suggested by Andre, Dansereau, & Labelle (Citation1994). This method involves identification of six SCPs. The manual identification results in inter- as well as intra-observer variability. To eliminate this error, the identification process is made automatically. The six points to be identified are the extremities of the pedicles and the centres of superior and inferior vertebral endplates. The automatic landmark identification procedure is described in our earlier work (Kumar, Nayak, & Hareesha, Citation2017b). Using six corresponding points, their 3D location is computed using the direct linear transformation (DLT). The DLT method results in large 3D reconstruction errors. To reduce these errors, an optimization technique is used for triangulation to get the 3D spine model. The 3D model thus obtained is a wireframe structure. The analysis of spinal deformities is very difficult using this structure. To improve the visibility, a morphorealistic generic spine model is prepared using the CT scan slices of a cadaveric spine (Kumar, Nayak, & Hareesha, Citation2014). This involves several image processing steps. The CT scan slices of 1 mm thickness are obtained from T1 to L5 vertebrae of the cadaveric spine in DICOM format with dimension 512 × 512 and 12 bit resolution. They are enhanced and segmented using the multilevel thresholding technique. For each vertebra, the segmented slices are stacked one above the other and volumerendering technique is used for the 3D reconstruction. It is obtained by modelling isosurfaces as the polygon meshes. The isosurface represents a region of specific density. The isosurfaces are extracted using the marching cubes algorithm also known as connecting cubes algorithm (Cline and Lorensen, Citation1987). The vertebrae are stacked one above the other with normal kyphotic and lordotic angles to obtain the generic model. This generic model is deformed according to the SCP wireframe structure to obtain the SCP model. Dual kriging, a free form deformation technique, is used for this purpose (Trochu, Citation1993). This model is more realistic in nature.
Figure 5. CSCPG spine modelling procedure.
The SCP spine model is further deformed using the automatically extracted features like orientations and positions of the pedicle. By retro-projecting the SCP-reconstructed model on to the frontal and lateral planes, the vertebral features are also computed. The transformations are applied to each vertebra of the spine in the SCP-reconstructed model till it matches with the computed orientation features. The projection of the pedicles is also used for accurate alignment of these features. This procedure is applied to all the 17 vertebrae to get the CSCPG reconstruction.
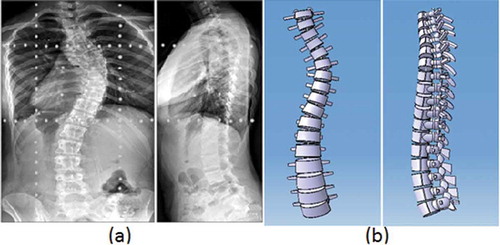
The CSCPG reconstruction obtained from subject-1 radiographs are shown in Figure . Similarly, CSCPG models are obtained from 10 scoliotic subjects. The accuracy of 3D reconstruction is measured by back projection technique. The reference NSCP models, feature-based models, and CSCPG models are back projected onto the x-rays in both the planes. The accuracy is computed by determining the least square distance between the six SCPs present in the x-rays and corresponding back projections. The orientation accuracy is computed by measuring the Cobb angle in the plane at which maximum curvature is observed. The plane of maximum curvature is obtained by rotating the frontal plane by an amount equal to the AVR, which is discussed in the next section.
Figure 6. Subject-1 (a) Biplanar x-rays (b) CSCPG model.
2.3. Deformity quantification
The spinal deformity is quantified by measuring the spinal curvature and AVR. This technique is described in detail in our earlier work (Kumar, Nayak, & Hareesha, Citation2017a). A semi-automatic technique is suggested to measure AVR of each vertebra. It involves identification of only two points on the pedicles of the 3D vertebral model to generate the vertebral vector to compute AVR. Then, the plane of maximum curvature is obtained using the most laterally deviated vertebra known as apical vertebra. Cobb angle measured in this plane gives the actual spinal curvature. A semi-automated procedure of calculating AVR is presented here. The most recent method followed to measure AVR in 3D (used in EOS systems) (Dubousset, Charpak, & Dorion, Citation2005) needs an exact location of the acetabulum. As the EOS system performs full body scanning, acetabula are clearly seen. The line joining centres of the acetabulum is considered as x-axis of the coordinate system (Illés, Tunyogi-Csapó, & Somoskeöy, Citation2011). Imaging the acetabulum along with the full spine is not possible in the normal clinical environment due to the restricted size of radiographic films and ethical issues. Hence, in this method, the positioning system of the calibration apparatus is used to align the subject along the x-axis. The positioning system is adjusted using the rotary platform to align the patient acetabula along the x-coordinate. The perpendicular line drawn to the inter-pedicular line is taken as a reference. The angle made by vertebral vector of the apical vertebra with respect to this line, gives the AVR.
To compute the spinal curvature, first, the 3D model is projected onto the frontal plane and converted to a grayscale image. The grayscale model projection is subject to thresholding in order to get the binary image. The thresholding operation is the first segmentation step. It separates the two classes in the grayscale image. In the present algorithm, the thresholding separates the vertebral segments from the background. Then the gradient edge detection is performed using the Sobel operator. It decides the vertebral edges in the binary image. Now, the edge region of the end vertebra is cropped using the selection tool. The edges of the transverse process and the vertebral endplate are extracted using the Hough transform. The complete algorithm is shown in Figure . The AVR and spinal curvature are computed for all the 10 subjects for both feature-based and CSCPG models.
3. Results
The NSCP models of 10 scoliotic subjects are considered as the gold standard for performance comparison of the proposed models. The standard 3D reconstruction methods like CT/MRI cannot be used as the reference as they are obtained in supine position which alters the spine anatomy. The mean reconstruction accuracies of the reference NSCP model, feature-based model, and CSCPG model of 10 scoliotic subjects is listed in Table . The accuracies are compared both in terms of location and orientation.
Table 1. The mean accuracies of different reconstruction techniques obtained from 10 scoliotic subjects
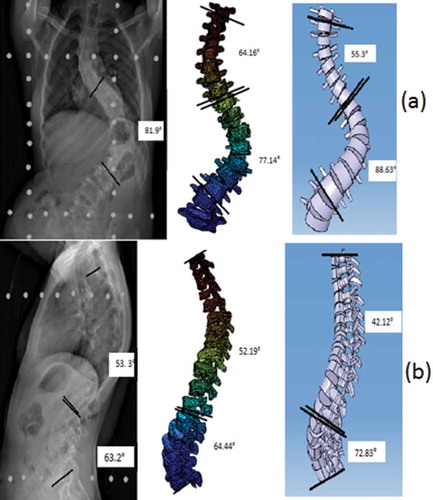
The AVR and spinal curvature of scoliotic subjects are measured from both feature-based and CSCPG models using semi-automatic methods explained in the previous section. These measurements are repeated for all the 10 subjects. An example of subject-2 measurements is shown in Figure .
Figure 7. Steps involved in spinal curvature measurement.
Figure 8. Spinal curvature of subject-2 using both the models (a) Frontal plane (b) Lateral plane.
In order to validate, the NSCP model is rotated manually by an angle equal to AVR. The spinal curvature is computed at this plane. This data are taken as a reference to validate the quantitative results obtained from the proposed model. The error between the quantitative results of the reference NSCP model and the proposed models are computed of all the 10 subjects. Then, the Wilcoxon test is performed to find if the differences between these results are statistically significant (p < 0.05). Table contains the summary of these results. From the table, it is clear that the difference between CSCPG model and the reference model is not significant. But, a significant difference is observed in the case of the feature-based model as the difference in both the clinical indices is large and p value is also less than 0.05.
Table 2. The mean differences between the quantitative results of proposed methods and NSCP reference method and corresponding pvalues of Wilcoxon signed rank test
4. Discussion and conclusion
The accuracy of CSCPG model is close to the gold standard NSCP model both in terms of location and orientation. The accuracy is slightly lesser due to the fact that only 6 SCPs are used in CSCPG modelling; whereas NSCP modelling uses 19 more SCPs for the reconstruction. Though the reconstruction accuracy is less, the CSCPG reconstruction completely eliminates inter- and intra-observer variability. It is due to the presence of automatic landmark identification procedure in the CSCPG reconstruction. The accuracy of feature-based modelling is poor, both in terms of location and orientation. This is due to the assumptions and approximations incorporated in the design of the generic spine model. Also, the features used for personalizing the spine models are limited in numbers. Only vertebral orientation features from the radiographs are automatically extracted to deform the generic model. The accuracy can be increased by incorporating other features like pedicle contours, and vertebral endplate centres.
The statistical significance test for the difference in clinical indices also shows that CSCPG modelling is closer to the gold standard model. Hence, it can be used in any clinical set-up for diagnosing the scoliotic subjects.
Acknowledgements
The authors would like to acknowledge the support from the department of radio-diagnostics and the department of orthopedics, Kasturba Medical College, Manipal in data acquisition and expert opinion.
Additional information
Funding
Notes on contributors
Hareesha KS
Our main focus is on 3D modelling of human body parts. We are also in to augmented reality and virtual reality related to the healthcare domain. The current project is 3D reconstruction of the human spine using two x-rays. This idea can also be extended to 3D reconstruction of teeth and jaw using x-rays. The product developed using this approach will be economical, at the same time less radiation hazardous.
Sampath Kumar
Our main focus is on 3D modelling of human body parts. We are also in to augmented reality and virtual reality related to the healthcare domain. The current project is 3D reconstruction of the human spine using two x-rays. This idea can also be extended to 3D reconstruction of teeth and jaw using x-rays. The product developed using this approach will be economical, at the same time less radiation hazardous.
Related Research Data
References
- Andre, B. , Dansereau, J. , & Labelle, H. (1994). Optimized vertical stereo base radiographic setup for the clinical three dimensional reconstruction of the human spine. JBio Mechanisms , 1 27, 1023–1035.
- Aubin, C. É. , Dansereau, J. , Aubin, C. É., Dansereau, J., Parent, F., Labelle, H., & de Guise J. A. (1997). Morphometric evaluations of personalized 3D reconstructions and geometric models of the human spine. Medical and Biological Engineering and Computing , 35, 611–618. doi:10.1007/BF02510968
- Boisvert, J. , Cheriet, F. , & Pennec, X. (2008). Articulated spine models for 3D reconstruction from partial radiographic data. IEEE Transactions on Biomedical Engineering , 55, 11. doi:10.1109/TBME.2008.2001125
- Cline, H. E. , & Lorensen, W. E. (1987). Marching cubes: A high resolution 3D surface construction. Computer Graphics , 21, 163–169. doi:10.1145/37402.37422
- Daniel, C. M. , Boisvert, J. , Jorge, G. B. , Labelle, H. , & Joao Manuel RST (2011). Fast 3D reconstruction of the spine from biplanar radiographs using a deformable articulated model. Medical Engineering and Physics , 33, 924–933. doi:10.1016/j.medengphy.2011.03.007
- Dubousset, J. , Charpak, G. , & Dorion, I. (2005). A new 2D and 3D imaging approach to musculoskeletal physiology and pathology with low-dose radiation and the standing position: The EOS system. Bulletin De l’Academie Nationale De Medecine , 189, 287–297.
- Dumas, R. , Blanchard, B. , Carlier, R. , De Loubresse, C. G. , Le Huec, J.-C. , Marty, C. , … Vital, J.-M. (2008). A semi-automated method using interpolation and optimization for the 3D reconstruction of the spine from bi-planar radiography. Journal of Medicine Biology Engineering Computations , 46, 85–92. doi:10.1007/s11517-007-0253-3
- Hough . (1962). Method and means for recognizing complex patterns . Patent 3069654, USA.
- Illés, T. , Tunyogi-Csapó, M. , & Somoskeöy, S. (2011). Breakthrough in three-dimensional scoliosis diagnosis: Significance of horizontal plane view and vertebra vectors. European Spine Journal , 20(1), 135–143. doi:10.1007/s00586-010-1566-8
- Jones, A. C. , & Wilcox, R. K. (2008). Finite element analysis of the spine: Towards a framework of verification, validation and sensitivity analysis. Medical Engineering and Physics , 30, 1287–1304. doi:10.1016/j.medengphy.2008.09.006
- Kass, M. , Witkin, A. , & Terzopoulos, D. (1998). Snakes: Active contour models. International Journal of Computer Vision , 1, 321–331. doi:10.1007/BF00133570
- Kumar, S. , Nayak, K. P. , & Hareesha, K. S. (2014). 3D Biomedical modelling of human vertebrae and its deformation. In J. Stephen & R. K. Bhatia (Eds.), Advances in information technology and power electronics (pp. 325–336). McGraw-Hill publishing.
- Kumar, S. , Nayak, K. P. , & Hareesha, K. S. (2016). Improving visibility of stereo-radiographic spine reconstruction with geometric inferences. Journal of Digital Imaging , 29, 226–234. doi:10.1007/s10278-015-9841-1
- Kumar, S. , Nayak, K. P. , & Hareesha, K. S. (2017a). Quantification of spinal deformities using combined SCP and geometric 3D reconstruction. Biomedical Signal Processing and Control , 31, 181–188. doi:10.1016/j.bspc.2016.08.004
- Kumar, S. , Nayak, K. P. , & Hareesha, K. S. (2017b, April 7–8). Effect of automatic landmark identification on CSCPG reconstruction . 2nd international conference on communication systems, computing and IT applications (CSCITA - 2017), St. Francis Institute of Technology, Mumbai. doi: 10.1109/CSCITA.2017.8066571
- Mitton, D. , Landry, C. , Verson, S. , Skalli, W. , Lavaste, F. , & de Guise, J. A. (2000). 3D reconstruction method from biplanar radiography using non-stereo corresponding points and elastic deformable meshes. Medica Biologic Engineering Computation , 38, 133–139. doi:10.1007/BF02344767
- Mitulescu, A. , Skalli, W. , Mitton, D. , & De Guise, J. (2002). Three-dimensional surface rendering reconstruction of scoliotic vertebrae using a non-stereo-corresponding points technique. European Spine Journal , 11(4), 344–352. doi:10.1007/s00586-002-0432-8
- Moura, D. C. , & Barbosa, J. G. (2014). Real-scale 3D models of the scoliotic spine from biplanar radiography without calibration objects. Computerized Medical Imaging and Graphics , 38(7), 580–585. doi:10.1016/j.compmedimag.2014.05.007
- Mukhopadhyay, S. , & Chanda, B. (2002). An edge preserving noise smoothing technique using multiscale morphology. Journal of Signal Processing , 82, 527–544. doi:10.1016/S0165-1684(01)00143-8
- Pomero, V. , Mitton, D. , Laporte, S. , De Guise, J. A. , & Skalli, W. (2004). Fast accurate stereo-radiographic 3-D reconstruction of the spine using a combined geometric and statistic model. Clinical Biomechanics , 19, 240–247. doi:10.1016/j.clinbiomech.2003.11.014
- Seoud, L. , Cheriet, F. , Labelle, H. , & Dansereau, J. (2011). A novel method for the 3D reconstruction of scoliotic ribs from frontal and lateral ladiographs. IEEE Transactions on Biomedical Engineering , 58, 5. doi:10.1109/TBME.2009.2032530
- Tan, S. H. , Teo, E. C. , & Chua, H. C. (2004). Quantitative three-dimensional anatomy of cervical, thoracic and lumbar vertebrae of Chinese Singaporeans. European Spine Journal , 13, 137–146. doi:10.1007/s00586-003-0586-z
- Trochu, F. A. (1993). contouring program based on dual kiging interpolation. Engineering with Computers , 9, 160–177. doi:10.1007/BF01206346
- Zhang, J. , Lv, L., Shi, X., Wang, Y., Guo, F., Zhang, Y., & Li, H. (2013). 3D reconstruction of the spine from biplanarX-rays based on contour matching using the Hough transform. IEEE TransBiomed Engineering , 60, 7.