
Abstract
ACL reconstruction is the recommended surgery for young, physically active persons with complete ACL rupture. This study has MAHE, Manipal ethics committee clearance. This research is a case study on AMP and TT techniques of ACL reconstruction. The two techniques of Reconstruction of ACL undertaken on different subjects are compared with the healthy knee joint and Reconstructed-ACL (R–ACL) which have undergone simulation, based on the stress induced. This research paper is based on a retrospective study that utilizes image data from previously carried–out surgery on patients and does not cause any harm to the living condition of the patients. Computer Tomography (CT) image of the human knee joint of a person who had undergone ACL reconstruction by Anteromedial Portal (AMP) technique and another person who had undergone ACL reconstruction by Traditional Transtibial (TT) technique were considered for this study. A 3-dimensional (3D) geometry of the reconstructed ACL is generated from the CT images of human knee joints of both persons. A Magnetic Resonance Image (MRI) of a healthy human knee joint is considered. A 3-D geometric image of this healthy human knee joint is considered. It is discretized into a finite element model. The healthy ACL was replaced by a reconstructed ACL in the healthy human knee joint. The loads and boundary conditions corresponding to the Lachman test were applied to the human knee joint. In this study, equivalent stress (Von-Mises) in the ACL reconstructed by the AMP technique was found to be 16.07 MPa, whereas the equivalent stress in the ACL which has undergone TT technique of ACL reconstruction was 36.73 MPa. The equivalent stress distribution in the model was assessed and compared with earlier studies. Based on the analysis, it was found that the AMP technique is better than the TT technique of ACL reconstruction.
1. Introduction
ACL reconstruction is surgical procedure in which the torn ACL is replaced by a graft. If the graft is taken from another person it is known of allograft. If it is taken from the same person it is known as autograft. If it is taken from another person it is known as allograft. Van Ek et al. (Charles Brown, Citation2014) define anatomic ACL reconstruction as the process of restoring ACL to its native site and orientation. There are three conditions for anatomic ACL reconstruction. First, the graft should replicate the size, shape and location of native ACL. Secondly, it should replicate the two functional bundles of native ACL. The tertiary condition is it should replicate the tensional pattern of native ACL. Finally, it should be individualized for every person as a every person has a different anatomical configuration when compared with another person. In Anteromedial Portal (AMP) technique an anteromedial portal is drilled in the femur. But, in the Traditional Transtibial (TT) technique this feature is absent. Knee joint which is considered for this study includes bones such as Tibia, Femur, and Fibula; stabilising ligaments like anterior cruciate ligament (ACL), articular cartilages, posterior cruciate ligament (PCL), medial collateral ligament (MCL), lateral collateral ligament (LCL); Femoral and Tibial cartilages, Menisci. The comparison between Traditional Transtibial and Anteromedial Portal techniques is shown in .
Figure 1. (a)Tunnel position in transtibial technique (Charles Brown, Citation2014).
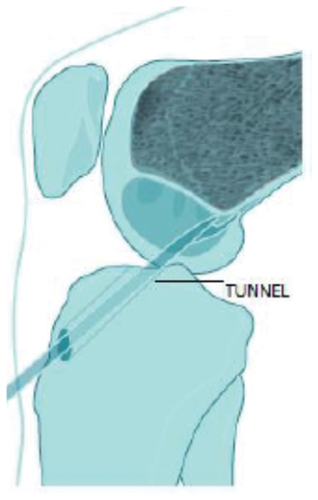
Figure 1. (b) Tunnel position in anteromedial technique (Charles Brown, Citation2014).
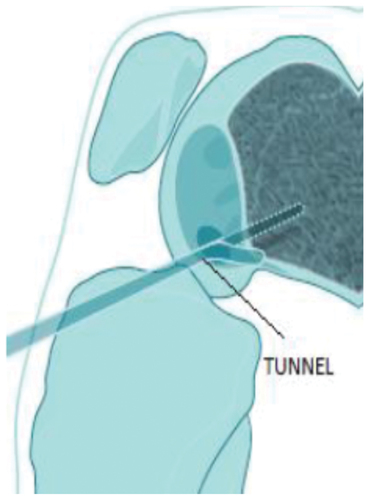
An Anterior Cruciate Ligament femoral tunnel is drilled through a tibia tunnel positioned in the posterior half of the native Anterior Cruciate Ligament tibial attachment site. The ability of the Transtibial technique to recreate the anatomy and function of the Anterior Cruciate Ligament was questioned by many researchers which led to the use of the Anteromedial Portal Technique. The comparison between Traditional Transtibial and Anteromedial Portal Techniques is shown in .
Not much literature is available in this area of study. However, among the ones that are available Kim et al. (Kim et al., Citation2021) have undertaken experimental studies in which they have compared Anteromedial Portal (AMP) and Traditional Transtibial (TT) techniques pertaining to footprint in the femur. They have concluded that the TT technique produced more stress when compared to the AMP technique of ACL reconstruction at the femoral footprint. Trofa et al. (Trofa et al., Citation2020) have undertaken their study by using a hybrid TT technique which involved procedures of both AMP and TT techniques of ACL reconstruction. They have concluded that their technique was better able to achieve the anatomical position of ACL reconstruction. Mehta et al. (Mehta et al., Citation2019) have studied contact characteristics of tibial tunnel aperture for both Anteromedial and Traditional techniques of ACL and have found that the Anteromedial technique may produce graft failures when compared to the TT technique owing to a high contact pressure of the graft. Liu et al. (Liu et al., Citation2018) have undertaken studies in which they have tabulated tibiofemoral contact stress for both Anteromedial and Traditional transtibial techniques. They have concluded that the AMP technique closely restores the human knee joint close to the ACL intact knee. Franceschi et al. (Franceschi et al., Citation2013) have retrospectively studied clinical, functional, and radiographic outcomes of ACL reconstruction by comparing AMP and TT techniques of ACL reconstruction with data on femoral tunnel position. They have concluded that the AMP technique better restores the reconstructed ACL to its native location and orientation than the TT technique. Sila et al. (Silva et al., Citation2011) studied femoral and tibial tunnel position along with orientation for both the AMP and TT technique of ACL reconstruction. They have concluded that the AMP technique better restores the reconstructed ACL to its native site location and orientation. Sim et al. (Sim et al., Citation2011) have experimentally compared AMP and TT techniques of ACL reconstruction. They have concluded that AMP and modified TT technique produce ACL to its native site and orientation. Bedi et al. (Bedi et al., Citation2011) have studied femoral tunnel location, and orientation for AMP and TT techniques of ACL reconstruction. They have concluded that results eccentric positioning of reconstructed ACL results in iatrogenic re-reaming of the tibial tunnel and significant intra-articular aperture expansion. Liu et al. (Liu et al., Citation2018) have studied tibiofemoral contact area and stresses after single bundle ACL reconstruction with femoral tunnels with respect to AMP and TT techniques. They have concluded from their study that ACL reconstruction by AMP and TT technique alter the contact area and stresses when compared to intact human knee joint. From their study they have concluded that AMP technique restores more closely the native ACL contact area and stresses when compared to TT technique. Kim et al. (J. Kim et al., Citation2021) have studied contact stress at single bundle and transportal double bundle ACL reconstruction. The total graft and total contact stresses after double bundle ACL reconstruction are higher than those after single bundle ACL reconstruction from 0° to 30° and 0° to 90° knee flexion, respectively. But, the stresses in each graft of double bundle ACL reconstruction are half those of single-bundle ACL reconstruction. Kim et al. (S. Kim et al., Citation2021) have studied contact stress around femoral footprint for anteromedial and central footprint. They have concluded from their study that contact stresses around femoral tunnel opening is higher for central footprint technique when compared to anteromedial footprint technique.
From the literature review, it is observed thought there are clinical/experimental and finite element studies in which numerous researchers have compared AMP and TT techniques of ACL reconstruction. Not many authors have used the finite element method to compare the stress in the bundle of single-bundle ACL reconstruction by both AMP and TT techniques of ACL reconstruction. However, some authors have compared stress at femoral footprint for AMP and TT technique of ACL reconstruction. These authors have concluded that stress at femoral footprint for AMP technique produces less stress when compared to TT technique of ACL reconstruction. Some authors have compared stress in single-bundle ACL reconstruction to double-bundle ACL reconstruction. They have concluded that stress in single-bundle ACL reconstruction is less when compared to double-bundle ACL reconstruction. This research paper claims novelty in comparing these two techniques of ACL reconstruction by using the finite element method for Lachman test loading condition. The objective of this paper is to compare the two techniques of ACL reconstruction which is done by a single surgeon. It is a retrospective study wherein readily available Magnetic Resonance Imaging (MRI) and Computed Tomography data is used for the study.
2. Materials and methods
The linear elastic isotropic material property was considered for all the parts of the joint. In this study, the loading time considered was 1s which is far less than the cartilages’ viscoelastic time constant of the 1500s (Bhat et al., Citation2018). Quasi-static implies that the linear elastic material property holds good up to 1500s. Beyond this, the material property of living tissues would become viscoelastic. Here, the 1500s is a viscoelastic time constant. The load applied is for 1s which is far less than the viscoelastic time constant of the 1500s.
Therefore, the cartilages were isotropic linear elastic in behavior. For the same reason menisci and stabilizing, ligaments were also considered to be linear. Hence, the linear elastic material properties considered in the analysis are quasi-static and are higher than equilibrium values (Bhat et al., Citation2018). The material properties used in the present work are as in .
Table 1. Material property (Bhat et al., Citation2018)
2.1. Grid Independence test
The maximum von–Mises stress induced in the knee joint was taken as the reference for deciding the appropriate number of elements for the analyses. The von–Mises stress at 12.52 lakh elements is 12.483 MPa which is 13.81% more than the stress in the finite element model of the knee joint at 16.96 lakh elements. A percentage change of 1.7% is observed in the von–Mises stress in the finite element model of the human knee joint from 16.96 lakh to 23.97 lakh elements. Similarly, a percentage change of 1.2% is observed when elements are increased from 23.97 lakh to 35.24 45 lakh. It is observed that von–Mises stress at 23,96,584 elements is 10.571 MPa and at 35,42,527 elements is 9.883 MPa, the difference between these two is about 5%. It is observed that the best results are obtained at 23,96,584 elements. Hence, the subsequent analyses are undertaken with models having 23,96,584 or more number of elements. The same has been shown in . Further, the meshed human knee joint is shown in , this is similar to the ACL reconstructed knee joint.
Figure 2. Results of grid independence test.
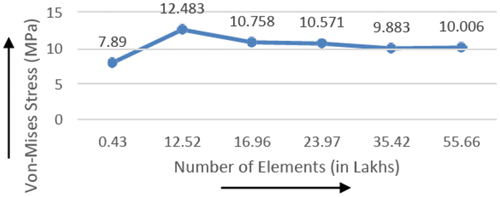
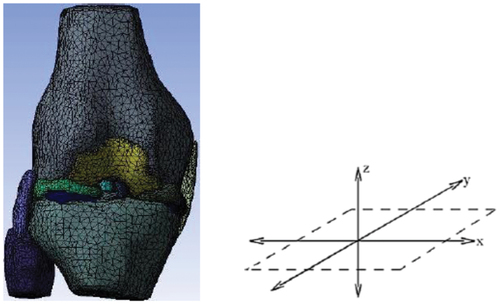
Figure 3. Finite element mesh with corresponding co-ordinate system.
The 3D model of the knee joint with reconstructed ACL is meshed using 10–node tetra hadron (second-order) elements having three degrees of freedom in translation. This is done using 3–Matic (Materialise Inc., Leuven, Belgium) software. The meshed knee joint parts were then exported into the ANSYS workbench (ANSYS Inc., USA). The loads and boundary conditions of the Lachman test are applied as discussed further in this paper.
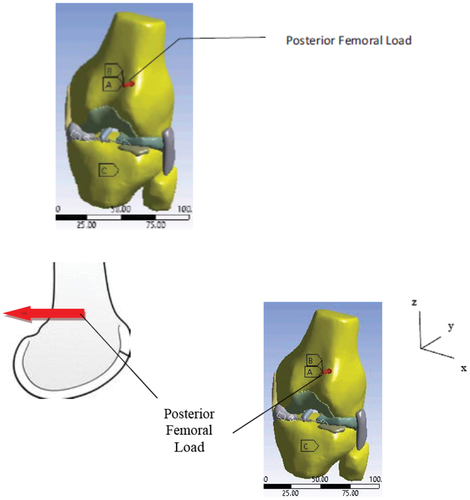
Verification of intactness of ACL is done by the Lachman test (S. Kim et al., Citation2021). In this test, the ATT of the tibia is observed in the supine position of the body when a 134 N (Trofa et al., Citation2020 and Wan et al., Citation2017) load is applied to the tibia in the anterior direction. The same is shown in . In the present study, the Lachman test was simulated using the Finite Element analysis approach on healthy human knee joints of five subjects for statistical significance of the results. Finite Element models of one subject with healthy knee joints in full-extension position were considered.
Figure 4. Loads and boundary conditions in a human knee joint subjected to Lachman test.
2.2. Modeling and load application
The full-extension position of the knee joint is considered for this study. An MRI with a slice thickness of 2 mm and pixel size of 1 mm was utilized. The stacked MRI of a 31 year–the old male subject was loaded into MIMICS (Materialise Inc., Leuven, Belgium) software in Digital Imaging and Communications in Medicine (DICOM) format. The stacked DICOM images were collated so that 3-dimensional (3D) geometry can be generated.
The first step in the process is the generation of a 2-dimensional surface called “Mask” on each slice of the MRI. From these “Masks” the individual parts of the knee joint were generated. For each of these subjects, MRI considered had a slice thickness of 2 mm and a pixel size of 1 mm. Subsequently, the surfaces of the knee joint parts are “smoothed” and “wrapped” so that holes in the geometry are reduced. shows masks as seen in MIMICS software. The geometric model of the joint was exported to 3–Matic (Materialise Inc., Leuven, Belgium) software where it was converted into a finite element model using 10-node second-order tetrahedral element with three degrees of freedom at each node. Firstly, the surface mesh was carried out followed by the volume mesh of the individual parts of the knee joint. Each part of the human knee joint was imported separately and assembled in ANSYS–workbench (ANSYS Inc., USA) respectively. The spatial position of each part corresponds to the MRI. A finite element model of the human knee joint along with its appropriate coordinate system is shown in .
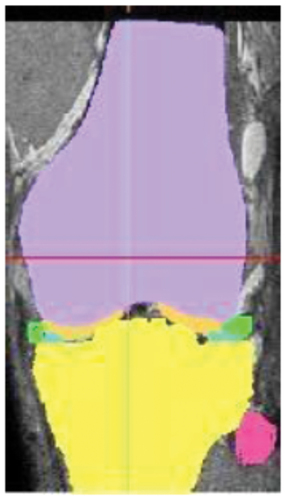
Figure 5. Mask as seen in MIMICS.
Computed Tomography (CT) images of knee joints of patients who had undergone ACL reconstruction by AMP and TT techniques by a single surgeon were utilized to generate a 3D model of reconstructed ACL. For this purpose, the data pertaining to footprint positions, tunnel dimensions, and angle of orientations in those knee joints were extracted using MIMICS (Materialise Inc., Leuven, Belgium) software. Upon obtaining these details, the reconstructed ACL for both AMP and TT techniques were modeled in the 3D model of the human knee joint of a 31-year-old subject from the digital repository of a hospital using 3–Matic (Materialise Inc., Leuven, Belgium) software. This is inevitable because the CT images of the subjects who had undergone ACL reconstruction according to AMP and TT techniques do not have the data of soft tissues. The load application is shown in a meshed model of a healthy human knee joint. This is similar to the one applied on a knee joint with a reconstructed ACL.
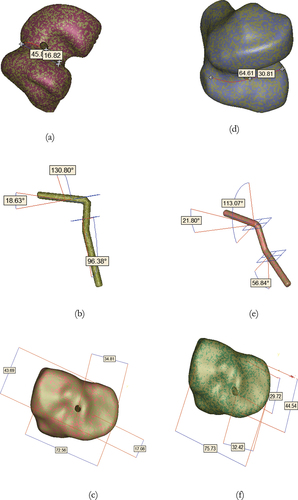
The MRI data used for generating the 3D model of this human knee joint is the same as the one used for modeling in the research paper by Bhat et al. (Bhat et al., Citation2018) as stated earlier in this research paper. The number of elements was chosen from the grid-independence test in this research paper. The 3D model of the knee joint considered for the purpose has all other parts of the joint except the ACL which needs to be modeled using the data extracted from the knee joint subjected to ACL reconstruction. The diameter of reconstructed ACL as extracted from the subjects who have undergone ACL reconstruction is 6 mm. Even though the diameter of this reconstructed ACL is lesser by 3 mm when compared to the R–ACL mentioned in Bhat et al. (Bhat et al., Citation2018), it is still within the recommended range of 6–10 mm (J. Kim et al., Citation2021). The geometric models of reconstructed ACL, femoral and tibial tunnels are generated by AMP and TT techniques as shown in . The constructed geometry of ACL is incorporated into the 3D knee joint model (as discussed above) at the appropriate locations.
Figure 6. AMP technique: (a) Femur with foot print location (b) reconstructed ACL (c)* Tibia with foot print; TT technique: (d) Femur with foot print location (e) reconstructed ACL (f)* Tibia with foot print.
3. Results
The stress and displacement results obtained in the knee joint in supine position for the AMP technique are presented in and the TT technique is shown in . The von-Mises stress has been plotted human knee joint for both AMP and TT techniques of ACL reconstruction. Further, stress implies Von-Mises stress in this research paper.
Figure 7. AMP technique: (a) Displacement in the knee joint, (b) Stress in the knee joint, (c) Stress in the R—ACL.
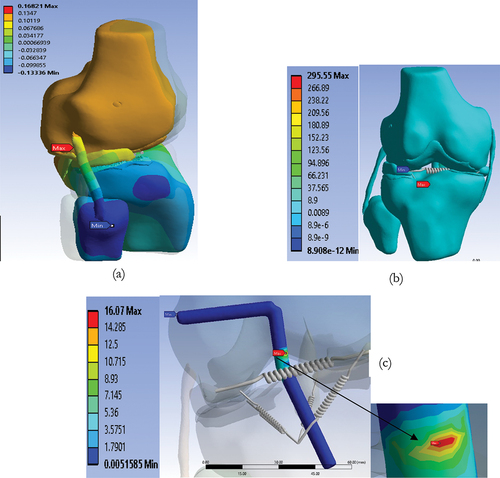
Figure 8. TT technique (a) Displacement in the knee joint, (b) Stress in the knee joint, (c) Stress in the R—ACL.
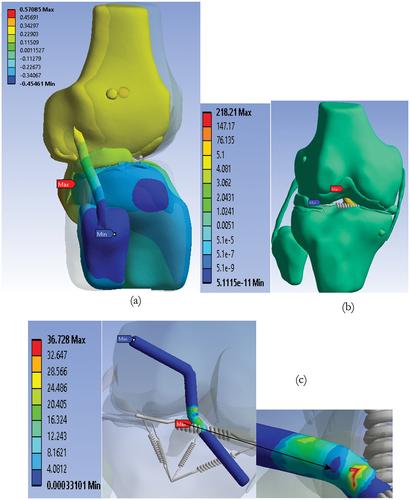
The posterior femoral displacement the knee joint with ACL reconstruction by the AMP technique is 0.168 mm as seen in . The maximum stress in this knee joint is 295.55 MPa, as shown in . The reconstructed ACL shows the stress of 16.07 MPa in its articular region as represented in .
Posterior femoral displacement in the knee joint with ACL reconstruction by TT technique is 0.5708 mm as seen in . The maximum stress in this knee joint is 218.21 MPa as presented in . The reconstructed ACL shows the stress of 36.73 MPa in the region of articulation of the knee joint as evident in .
4. Discussion
During the comparison of the recommended footprint location and angle of orientation (J. Kim et al., Citation2021) of the ACL with the reconstructed ACL, the method of measurement of femoral and tibial footprints used is the same as in Bhat et al. (Bhat et al., Citation2018). From , the recommended values for femoral footprint locations 38 ± 2.7%of articulating region measured from posterior margin for both AMP and TT techniques of ACL reconstruction. In the knee joint subjected to ACL reconstruction by AMP technique, the footprint is located at 36.7% of articulating region measured from the posterior margin which is within the recommended range. But, in the knee joint subjected to the TT technique of ACL reconstruction, the footprint is located at 47.67%measured from the posterior margin which is outside the recommended range. In the tibia, the recommended location of the tibial footprint is at 44.6 ± 2.5% from the anterior margin for both AMP and TT techniques of ACL reconstruction. In the knee joint subjected to the AMP technique, the footprint of reconstructed ACL is located at 39.09% from the anterior margin which is outside the recommended range. Similarly, in the knee joint subjected to the TT technique of ACL reconstruction, the femoral footprint is at 65.26% from the anterior margin of the tibia which is very much outside the recommended range. Further, as per the recommendation, the footprint is to be located at 48 ± 3 % from the medial margin for both AMP and TT techniques of ACL reconstruction. In the case of the knee joint subjected to the AMP technique, the tibial footprint is at 47.97% from the medial margin which is within the recommended range. In the case of the TT technique, the tibial footprint is located at 42.81% from the medial margin. This is outside the recommended range. In general, it is found that for the AMP technique the femoral and tibial footprints located by the surgeon are in the recommended range with an exception in locating the tibial footprint from the anterior margin, as shown in . It can also be seen from that, for the TT technique, the femoral and tibial footprints located during surgery are not in the recommended range. Hence, it may be noted that the TT technique implemented by the surgeon did not abide by the anatomic method of ACL reconstruction.
Table 2. Recommended and as reconstructed knee joint foot ‒print location/angle of orientation
The recommended range of values of ACL orientation for femoral insertion in the human knee joint subjected to the AMP technique is 69 to 76 degrees in the coronal plane measured from the tibial plateau (Bhat et al., Citation2018). In the knee joint subjected to the AMP technique, this angle is at 18.63 degrees. In the knee joint which has undergone the TT technique the femoral orientation of the reconstructed ACL, the recommended angle is in the range of 72 to 78 degrees in the coronal plane measured from the tibial plateau (Bhat et al., Citation2018). In the knee joint where ACL is reconstructed by TT technique, the coronal obliquity is found to be 21.8 degrees. In the sagittal plane, the angle of obliquity of ACL for femoral insertion recommended angle is in the range of 52 to 58.5 degrees (Bhat et al., Citation2018 and Vermesan et al., Citation2015).
In the knee joint where ACL is reconstructed by the AMP technique, this angle of projection on a sagittal plane is found to be 130.8 degrees from the tibial plateau. In the knee joint where ACL is reconstructed by TT technique, the sagittal obliquity is recommended to be in the range of 59 to 69.5 degrees. Further, in the knee joint reconstructed by the TT technique, this angle of projection is found to be at 113.07 degrees from the tibial plateau. The tibial obliquity of reconstructed ACL observed in the sagittal plane is 45 degrees for AMP and TT techniques as recommended (Bhat et al., Citation2018). But, in the knee joints which have undergone AMP and TT techniques of ACL reconstruction, this angle is found to be 96.38 degrees and 56.64 degrees respectively. For both AMP and TT techniques of ACL reconstruction sagittal, coronal and tibial obliquities are outside the recommended range.
The stress in reconstructed ACL through the AMP technique is 16.07 MPa, as represented in , which is comparable with the mean stress of 17.74 ± 3.01 MPa obtained from the four subjects on which the AMP technique of ACL reconstruction is simulated. This mean value of stress is in turn compared with the mean stress of 13.934 ± 5.1 MPa obtained from the five healthy subjects. From these results, it could be interpreted that the femoral angle of orientation of ACL does not have much significance on the stress-induced in ACL. Therefore, the surgeon has the freedom of selecting the angle of orientation of ACL in the tibia as per the need of the subject undergoing ACL reconstruction. Further, it could be understood that the AMP technique would restore the anatomic position of the native ACL site. The stress-induced in reconstructed ACL through the TT technique is 36.728 MPa, as represented in , which is not comparable with the mean stress obtained from the five healthy subjects as discussed above. Therefore, it could be interpreted that the TT technique of ACL reconstruction does not guarantee the restoration of ACL to its native site.
The results show that the AMP technique produces lesser stress on the reconstructed ACL than the TT technique as seen in , even though the stresses in the knee joint by both the methods are comparable as represented in . Moreover, it is also observed that the stress of 16.07 MPa induced in reconstructed ACL through the AMP technique is within the range of 17.74 ± 3.01 MPa. Whereas, the stress of 36.728 MPa obtained through the TT technique is outside this range. It is observed by Bhat et al. (Bhat et al., Citation2018) that the TT technique produces inconsistent results in terms of stress in different subjects when compared to the AMP technique which produces more or less consistent stress in all the subjects. Given these, it would be understood that the AMP technique could be preferred over the TT technique for ACL reconstruction.
The posterior femoral displacement in the ACL reconstructed knee joint by AMP is 0.168 mm which is lesser than the femoral displacement of 0.5708 mm produced by the TT techniques seen in . As per the study by Mehta et al. (Mehta et al., Citation2019) the anteromedial technique more circular tibial tunnel, showed a smaller, and a greater peak contact pressure at the tibial tunnel aperture under various loading conditions. The peak contact pressure is 869.1 ± 164.1 MPa for AMP technique and 564.6 ± 108.8 MPa for TT technique. Increased peak contact pressure on the graft at the tibial aperture may increase the stress on the graft and possibly lead to failure following ACL reconstruction with the anteromedial technique. This may be because of not considering other stabilizing ligaments for the experimental study. Further, increased peak contact pressure at the tibial tunnel may indicate that AMP firmly holds the reconstructed ACL to its site and location when compared with TT technique. Liu et al. (Liu et al., Citation2018) have shown that contact stress is higher for TT technique when compared to AMP technique. In this study it has been shown that the knee joint could become more flexible when subjected to the TT technique of ACL reconstruction when compared with the AMP technique. This flexibility is not desirable as it may lead to functional instability of the knee joint. This study is limited to Lachman test loading condition. However, there is future scope in using other loading conditions pertaining to the human knee joint.
5. Conclusion
ACL reconstruction by the AMP technique produces lesser stress in the reconstructed ACL than the TT technique.
The stress in reconstructed ACL and displacement in the knee joint using AMP technique methods are compared with the simulation results of ACL reconstruction presented.
From the results, it is found that the AMP technique is better than a technique for ACL reconstruction.
Ethics clearance
This study is cleared by MAHE, Manipal ethics committee with certificate bearing the number: Registration No. ECR/146/Inst/KA/2013.
Acknowledgements
The authors would like to thank the Manipal Academy of Higher Education, Manipal for providing the opportunity and support to pursue this research and attend the conference.
Some content has been taken from the author’s previously published articles. The authors wish to thank the publishers for allowing the reproduction of the content under an open-access license: under the terms of the Creative Commons Attribution 4.0 International Public License (CC-BY 4.0), a copy of which is available at: (https://creativecommons.org/licenses/by/4.0/legalcode). This license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Bhat, B., Adhikari, R. and Acharya, K. (2018). A Numerical Investigation of Anatomic Anterior Cruciate Ligament Reconstruction. The Open Bioinformatics Journal, 11(1), pp.259-274.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Bedi, A., Musahl, V., Steuber, V., Kendoff, D., Choi, D., Allen, A. A., Pearle, A. D., & Altchek, D. W. Transtibial versus anteromedial portal reaming in anterior cruciate ligament reconstruction: An anatomic and biomechanical evaluation of surgical technique. (2011). Arthroscopy: The Journal of Arthroscopic & Related Surgery, 27(3), 380–13. Available: 10.1016/j.arthro.2010.07.018. https://doi.org/10.1016/j.arthro.2010.07.018
- Bhat, B., Adhikari, R., & Acharya, K. (2018). A numerical investigation of anatomic anterior cruciate ligament reconstruction. The Open Bioinformatics Journal, 11(1), 259–274. https://doi.org/10.2174/1875036201811080259
- Charles Brown, J. (2014). Anatomical ACL reconstruction. Aspetar.com, 2022. [Online]. Available:https://www.aspetar.com/journal/viewarticle.aspx?id=94#.YtEqlnZBzIU
- Franceschi, F., Papalia, R., Rizzello, G., Del Buono, A., Maffulli, N., & Denaro, V. (2013). Anteromedial portal versus transtibial drilling techniques in anterior cruciate ligament reconstruction: Any clinical relevance? a retrospective comparative study. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 29(8), 1330–1337. https://doi.org/10.1016/j.arthro.2013.05.020 Available
- Kim, J., Kang, K., & Wang, J. Biomechanical difference between conventional transtibial single-bundle and anatomical transportal double-bundle anterior cruciate ligament reconstruction using three-dimensional finite element model analysis. (2021). Journal of Clinical Medicine, 10(8), 1625. Available: 10.3390/jcm10081625. https://doi.org/10.3390/jcm10081625
- Kim, S., Song, S., Kim, T., Kim, Y., Jang, S., & Seo, Y. (2021). Creating a femoral tunnel aperture at the anteromedial footprint versus the central footprint in ACL reconstruction: Comparison of contact stress patterns. Orthopaedic Journal of Sports Medicine, 9(4), 232596712110018. https://doi.org/10.1177/23259671211001802 Available
- Liu, C., Wang, Y., Li, Z., Li, J., Zhang, H., Fu, Y., & Zhang, K. (2018). Tibiofemoral joint contact area and stress after single-bundle anterior cruciate ligament reconstruction with transtibial versus anteromedial portal drilling techniques. Journal of Orthopaedic Surgery and Research, 13(1). Available. https://doi.org/10.1186/s13018-018-0956-1.
- Mehta, A., Lin, C. C., Campbell, R. A., Chin, G., McGarry, M. H., Lee, T. Q., & Adamson, G. J. (2019). Effects of anteromedial portal versus transtibial ACL tunnel preparation on contact characteristics of the graft and the tibial tunnel aperture. Clinics in Orthopedic Surgery, 11(1), 52. https://doi.org/10.4055/cios.2019.11.1.52 Available
- Silva, A., Sampaio, R., & Pinto, E. (2011). ACL reconstruction: Comparison between transtibial and anteromedial portal techniques. Knee Surgery, Sports Traumatology, Arthroscopy, 20(5), 896–903. https://doi.org/10.1007/s00167-011-1645-3 Available
- Sim, J., Gadikota, H., Li, J., Li, G., & Gill, T. Biomechanical evaluation of knee joint laxities and graft forces after anterior cruciate ligament reconstruction by anteromedial portal, outside-in, and transtibial techniques. (2011). The American Journal of Sports Medicine, 39(12), 2604–2610. Available: 10.1177/0363546511420810. https://doi.org/10.1177/0363546511420810
- Trofa, D., Saltzman, B., Corpus, K., Connor, P., Fleischli, J., & Piasecki, D. A hybrid transtibial technique combines the advantages of anteromedial portal and transtibial approaches: A prospective randomized controlled trial. (2020). The American Journal of Sports Medicine, 48(13), 3200–3207. Available: 10.1177/0363546520956645. https://doi.org/10.1177/0363546520956645
- Vermesan,D., Inchigolo,F., Patrascu,J.M., Trocan,I., Prejbeanu,R., Florescu,S., Damian,G., Benagiano,V., Abbinante,A., Caprio, M., Cagiono,R., &Haragus,H. (2015). Anterior cruciate ligament reconstruction and determination of tunnel size and graft obliquity. European Review for Medical and Pharmacological Sciences,19,357―364.
- Wan, C., Hao, Z., Li, Z., & Lin, J. (2017). Finite element simulations of different hamstring tendon graft lengths and related fixations in anterior cruciate ligament reconstruction. Medical and Biological Engineering and Computing, (June), 19(3), 357-364.