
Abstract
An interventional pre-post study was conducted to evaluate rural women’s insights on anaemia and the effects of nutritional training on the knowledge and haemoglobin (Hb) levels among women of reproductive age (19–45 years) in Dodoma, Tanzania. The respondent was the mother/woman or any other person responsible for food preparation and serving in the household. Baseline and endline data on demographic and socioeconomic information, women’s insights on anaemia, knowledge gaps of mothers’/caregivers’ in nutrition, iron deficiency and iron-rich foods were collected using a face to face interviewer-administered questionnaire. Haemoglobin concentration of the women was measured at baseline and endline using a portable battery-operated electronic HemoCue Hemoglobinometer. Training was done once every month for three months consecutively. A total of 350 women were involved at baseline and 260 women at endline. Among all respondents, only 18% of women had baseline knowledge regarding the causes of anaemia which was increased significantly to 72% after the intervention. At baseline, 19% of women had haemoglobin levels of below 12.0 g/dl this number decreased to 13% during the endline survey. The results indicated a significant association between a woman having consumed green leafy vegetables in the previous 24 hours preceding the survey and haemoglobin levels during the endline period. The findings of this study indicate that the nutrition education given directly to rural women could have some impact in improving women’s knowledge and haemoglobin status.
PUBLIC INTEREST STATEMENT
Hidden hunger or micronutrient deficiency is a major problem in developing countries. In Tanzania, vitamin and mineral deficiencies are high; about 58% and 34% of children below five years are iron and vitamin A deficient, respectively. The rural underprivileged residents depend on staple foods which lack diversity; increasing the risk of insufficient intake of vitamins and minerals. This article enlightens opinions of rural women on anaemia and assesses the effect of educating women on nutritional matters on the knowledge, practices and haemoglobin status in rural settings. It was found that before the nutrition education was given to women, the majority lacked information regarding anaemia and its various aspects, but the knowledge of these women greatly increased after the education was given. It was also found that the haemoglobin level of women increased after the education programme. It is therefore recommended that education interventions should be done regularly to women which will, in turn, motivate them to practice health eating and improve their nutrition status.
1. Introduction
Micro-nutrient deficiencies inflict significant public health problems in many developing countries affecting especially women of childbearing age and children. Dietary intake has a key effect on nutritional status, making essential the revealing of both nutritional insufficiencies and extremes that would have detrimental outcomes on health (Alao, Citation2015). According to the Tanzania Demographic and Health Surveys (TDHS), about 34% of children aged 6–59 months and 37% of women of reproductive age (15–49 years) were vitamin A deficient (National Bureau of Statistics (NBS) and ICF Macro, 2010) and about 58% of children below five years of age suffered from anaemia (MoHCDGEC et al., Citation2016). About 33% of women of age 15–49 years were iron deficient and about 45% had anaemia.
As indicated above, in Tanzania, the most prevalent micronutrient deficiency is anemia and the rates are worsened for women. Anaemia is a problem of public health significance in developing countries with the main implications for economic, human health and social development (Chaparro & Suchdev, Citation2019). Iron deficiency and other micronutrients are the major causes of anaemia throughout the world and it is common in women of reproductive age where these deficiencies may lead to various effects including birth defects, preterm labour, low birth weight and an increase in perinatal death (Black et al., Citation2013; Scott et al., Citation2014).
Anaemia is defined by the World Health Organization (WHO) as “a condition in which the number of red blood cells (RBCs) or their oxygen-carrying capacity is inadequate to meet physiologic demands in the body, in which the haemoglobin level may vary by age, sex, altitude, smoking, and pregnancy status” (Gogoi & Prusty, Citation2013).
Many factors can cause anemia including several micronutrient deficiencies, blood loss, and hookworms (Chaparro & Suchdev, Citation2019). Iron is one of the micronutrient deficiencies that can cause anaemia. Iron deficiency anemia, which is the most common form of anemia, is principally dangerous because iron is crucial for the production of hemoglobin (Hb), a molecule that carriages oxygen through the body. Therefore, iron deficiency anemia will just be referred to as “anaemia” in this study.
In Tanzania, the prevalence of anaemia among women of reproductive age is estimated to be 29% (MoHCDGEC et al., Citation2018). Even though for a long time anaemia has been recognized as a public health problem worldwide, there has not been an observable fast improvement, and its prevalence is still high globally (Ghislain & Manfred, Citation2012). The WHO and the United Nations Children’s Fund (UNICEF) declared an immediate need to reduce the prevalence of anaemia and underlined the importance of recognizing its numerous causes so as to reach the global nutrition targets of 50% ‘reduction of anaemia in women of reproductive age by 2025ʹ (WHO, Citation2014).
Dietary practices are an essential determinant of anaemia, and the extensiveness of anaemia in Tanzania is a reflection of poor nutritional knowledge and dietary intake (MoHCDGEC et al., Citation2018). Moreover, poor knowledge is a direct consequence of poor nutritional education. Past research has indicated that knowledge is one of the initial stages to changing behaviour. Nutrition knowledge is thus an important foundation for good dietary practices (Alderman, Citation2007; Jalambo et al., Citation2017). Equally, a lack of knowledge is a risk factor for undernutrition (Ryoo, Citation2011). Nutrition education programmes are required to intensify awareness in women of reproductive age about anaemia (Weise, Citation2012). Furthermore, health education has demonstrated to be very effective and has resulted in a considerable improvement in haemoglobin levels and nutrition knowledge (Jalambo et al., Citation2017). The aim of this study was therefore to evaluate women’s insights on anaemia and the effects of nutritional training on the knowledge and haemoglobin (Hb) levels in women of reproductive age (19–45 years) in Dodoma, Tanzania.
2. Methodology
2.1. Study area
The study was conducted in two villages from the semi-arid Dodoma region in Tanzania. Ilolo and Idifu villages were selected from Chamwino district. Food production in Dodoma is predominantly rain fed. Dodoma region receives rainfall in one season with an average of 350–500 mm rainfall per annum. Dodoma is characterized by a prevalence of highly food-insecure areas. Crops produced include cereals (sorghum, pearl millet and maize), roots/tubers (cassava and sweet potato), legumes (cowpea, pigeon pea, bambara nut, groundnut, chickpea, green gram and lablab bean), oil crops (sunflower, sesame, groundnuts) and fruits (pawpaw, guava, mango, grape, lemon and dates). There is also widespread collection of edible wild fruits and vegetables. The food system in Dodoma is mainly based on cereals with pearl millet as the preferred staple. Groundnuts are normally mixed in most relishes that are used with the main dish. Edible wild products, particularly vegetables and fruits, are important in local food menus (Mutabazi Citation2013). The Chamwino district imports food crops from other regions during deficit months. These foods include maize, beans and pigeon peas. During deficit months imported food such as maize and pearl millet is sold at a price more than three times its price during the months of plenty. This is because there are no structured local markets in the study villages, only small grain and pulse traders. The two villages together account for 70–80% of the types of farming system found in semi-arid areas in Tanzania (Ronner & Giller, Citation2013).
2.2. Study design and sampling procedure
The study was interventional with pre and post-tests. The population was comprised of women or caregivers in the sampled households. The respondent was the mother/woman or any other person responsible for food preparation and serving in the household who was between 19 and 45 years of age. The households were randomly selected from village household lists provided by the Agricultural Research Institutes (ARI) Hombolo. The lists contained names of the household heads and names of hamlets (hamlets) they live in. After sorting the lists alphabetically for each hamlet, a total of 350 households were randomly selected to be included in the study. All hamlets were equally represented according to size or number of households. The household representatives were required to sign the form or apply a thumbprint (in ink), marking their consent to participating in the study. Permission to conduct the study was granted by the District Commissioners’ Offices and Ethical clearance was obtained from the Tanzania National Institute for Medical Research (NIMR/HQ/R.8a/Vol.IX/2226).
2.3. Baseline and endline surveys
A face to face interviewer-administered questionnaire was used to collect demographic and socioeconomic information, women’s insights on anaemia and to identify knowledge gaps of mothers’/caregivers’ in nutrition, iron deficiency and iron-rich foods in the selected households. The results of the baseline survey indicated that nutrition knowledge, practices and attitudes particularly those related to general nutrition, nutrition requirements for specific groups, preparation and preservation were poor. These areas were identified as those that required the most improvement (Mbwana et al., Citation2016). The face to face interviews principally informed the results of the study and were used together with other literature information to enrich the content of the nutrition training. The study found the nutritional knowledge of women to be relatively limited. Post-intervention knowledge of the women was assessed after training by the same questionnaire.
2.4. Biochemical measurements (haemoglobin concentration)
Haemoglobin concentration of the women was measured using a portable battery-operated electronic HemoCue Hemoglobinometer (HemoCueHb 201+, Angelhom). A capillary blood sample was obtained from a finger prick of each participant using a sterile lancet. A drop of blood was placed in a single-use Hemocue micro-cuvette and inserted in the machine for immediate reading in g/dL. Anaemia in non-pregnant women was defined as haemoglobin concentration <12.0 g/dL (World Health Organization [WHO], Citation2011). Haemoglobin measurements were done at baseline and endline periods. After the intervention, the haemoglobin levels were compared at baseline and endline to establish if there was any change.
2.5. Nutrition training program
The household nutrition training materials were developed based on the knowledge gaps and needs identified from the baseline survey conducted in the study areas. One training module with five topics was developed. The topics included: General nutrition and consumption of micronutrient-rich foods within households, nutrition requirements for specific groups: preparation and preservation of food, improving nutrition through kitchen gardens and tips for improving health through nutrition. Content validity of the materials developed was done by a panel of five experienced nutritionists who are researchers and academicians. The experts validated the accuracy of the information presented and the cultural sensitivity of the materials. The materials were also presented to project members during a meeting. The meeting participants were requested for general comments and suggestions which were later incorporated to improve the materials. Training was done once every month for three months consecutively. Two training sessions per day were done at the central demonstration household. Vegetable cooking demonstrations included actual cooking and eating. One training session lasted for about 3 hours. A total of 15 hours were used to cover the whole module of training.
3. Data analysis
Baseline and endline assessments were done by scoring method. All analyses were performed using IBM SPSS Statistics for windows, Version 21 (IBM Corp., Armonk, New York, USA). Data were presented using frequencies, percentages frequencies, means and standard deviations. The dichotomous categorical data for assessing differences in responses to nutritional knowledge in the baseline and endline time points were analysed using Mc Nemar test. The marginal homogeneity test was used for categorical variables with more than two responses to assess the marginal frequencies. Significance was considered when p < 0.05. The McNemar-Bowker’s test was used to calculate the changes in the Hb level categories before and after the nutrition education intervention.
4. Results
A total number of 350 women were involved at baseline and 260 women at endline. The mean age of women was 34 ± 0.9 years. Household size ranged between 6 and 8 persons at baseline and endline. The proportion of female-headed households was 15% at baseline and 23% at endline. The respondents who had not attained any formal education were 33% and 32% at baseline and endline respectively.
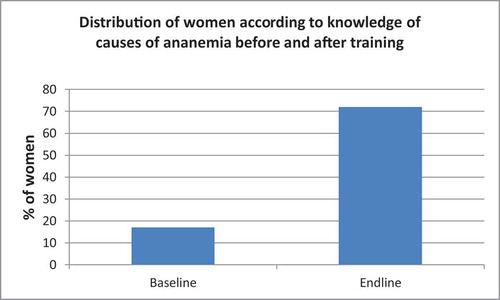
Among all respondents, only 18% of women had baseline knowledge regarding the causes of anaemia. The same knowledge was increased to 72% after the intervention and the increase in the knowledge was significant (p < 0.05) ().
Figure 1. Distribution of women according to knowledge of causes of anaemia before and after training
Women were asked about signs and symptoms of anaemia; in the baseline only about 24% of women were knowledgeable on this while during the endline, this knowledge increased significantly to 68% (P < 0.05). When asked about dietary sources of iron, 26% of women at baseline were aware about this, this knowledge increased significantly to 81% during the endline survey (P < 0.05).
About 21% of women had baseline knowledge about factors that inhibit the absorption of iron. When assessed in the endline, this knowledge increased to 68% and the increase was significant at 0.05. Regarding treatment of anaemia, 26% of women had baseline knowledge, which was increased to 74% in the endline.
4.1. Mean haemoglobin levels before and after intervention
At baseline, 19% of women had a haemoglobin level of below 12.0 g/dl this number decreased to 13% during the endline survey. shows changes in mean haemoglobin levels of the women before and after intervention. Distinguished differences were observed in mean Hb levels of women between the two points in time.
Table 1. Mean haemoglobin levels of the women before and after intervention
The results indicate a significant association (P < 0.05) between a woman having consumed green leafy vegetables in the previous 24 hours preceding the survey and haemoglobin levels during the endline period. The other selected nutrition knowledge themes were not significantly associated with haemoglobin level (p > 0.05), but the associations were stronger at endline for all themes except the question on factors inhibiting iron absorption. displays the relationship of nutrition knowledge and some selected themes and haemoglobin levels at baseline and endline.
Table 2. Relationship of nutrition knowledge on particular themes and haemoglobin levels
5. Discussion
This study informs on the level of knowledge regarding iron deficiency anaemia and haemoglobin status of women of reproductive age in rural areas in Tanzania.
Interventions on nutrition education to improve knowledge and dietary practices that support healthy eating to address iron deficiency are obligatory in any given population. Results of the baseline study indicated a substantial lack of knowledge about anaemia among the women. This lack of knowledge about various aspects of anemia is similar to other studies which reported low nutrition knowledge before educational interventions. For instance, a study by Daba et al. (Citation2013) in Ethiopia reported that the majority of women did not know the main food groups to form a balanced diet and more than half did not even know the meaning of food. Another study in Egypt reported that about half of the women did not have enough knowledge regarding the significance, the importance, and the elements of a well-balanced diet (Latifa et al., Citation2012). Poor knowledge is among the risk factors to develop malnutrition (Ryoo, Citation2011).
As it was observed in this study, after the intervention the average mean of nutrition knowledge improved considerably in all aspects that were assessed. The improvement may have been caused by the information during the training and women may have inclined to recall their responses during the endline survey. The findings of the current study demonstrate the affirmative outcome of nutrition education on knowledge and attitudes of women in agreement with other studies (Gupta & Kochar, Citation2009; Moore et al., Citation2009; Rani et al., Citation2013). Preceding studies reported that acquiring knowledge is one of the initial phases of an interchange towards a modification of behavior. Nutrition knowledge is therefore an important foundation for noble dietary practices (Alderman, Citation2007; Spendlove et al., Citation2012).
Hemoglobin levels were lower before the interventions but improved though not significantly after the intervention. This may be due to increased intake of iron-rich foods such as green leafy vegetables after the education which may have led to diet modification. These results advocate the shielding outcome of nutrition education on hemoglobin status. Nutrition education was effective since it improved the knowledge and attitudes of the participating women. These results are supported by numerous studies indicating nutritional education is effective in improving hematocrit, hemoglobin and serum ferritin levels among adolescents (Khoshnevisan et al., Citation2004; Moore et al., Citation2009). For instance, in Nicaragua, a study to examine the effect of a community‐based nutrition education program on the nutritional knowledge, hemoglobin levels, and nutritional status of adolescent girls and the nutritional knowledge of their mothers reported a significant increase in the nutritional knowledge of the girls and their mothers after participation in the nutrition education intervention program.
The increased nutritional knowledge in various aspects was significantly associated with increase in haemoglobin levels after intervention.
6. Conclusions and recommendations
The findings of this study clues to the supposition that the nutrition education intervention given directly to rural women could have some impact in improving women’s knowledge and haemoglobin status and therefore it may be an effective approach to combat iron deficiency and anaemia and promote good health and well-being of the women. Such interventions are recommended to be done regularly to improve women’s knowledge and to inspire them to embrace healthy lifestyles which averts anaemia and other micronutrient deficiencies.
Acknowledgements
The author gratefully acknowledges the funding source that allowed her to write this paper. This study was funded by the Innovating Strategies to Safeguard Food Security using Technology and Knowledge Transfer: A people-centred Approach Project (acronym ‘Trans-SEC’). The Trans-SEC project was financially supported by the German Federal Ministry of Education and Research (BMBF) and co-financed by the Federal Ministry for Economic Cooperation and Development (BMZ).
Disclosure statement
The author declares no conflict of interest.
Additional information
Funding
Notes on contributors
Hadijah Ally Mbwana
Dr Hadijah Mbwana is a lecturer and researcher at Sokoine University of Agriculture in the area of Human Nutrition and Consumer Studies. She holds PhD in Nutritional Sciences from Sokoine University of Agriculture, an MSc in Human Nutrition from Massey University, New Zealand and BSc in Home Economics and Human Nutrition from Sokoine University of Agriculture, Tanzania. She started as a tutorial assistant in 2008, and is now a lecturer in Human Nutrition and Consumer Studies since 2014. Dr Mbwana has worked in several research involving dietary practices and patterns of the vulnerable groups and exploring the potential of indigenous and locally produced foods throughout the food value chain in mitigating hunger, malnutrition; particularly micronutrient deficiencies nationally, regionally and internationally. She has competence in planning and executing quantitative and qualitative research and monitoring and evaluation of nutrition and health projects.
References
- Alao, M. (2015). Dietary intake and nutritional status of the elderly in Osun State. Journal of Nursing and Health Science, 4(1), 32–8.
- Alderman, H. (2007). Improving nutrition through community growth promotion: Longitudinal study of the nutrition and early child development program in Uganda. World Development, 35(8), 1376–1389. https://doi.org/10.1016/j.worlddev.2007.04.003
- Black, R. E., Victora, C. G., Walker, S. P., Bhutta, Z. A., Christian, P., de Onis, M., Ezzati, M., Grantham-McGregor, S., Katz, J., Martorell, R., & Uauy, R. (2013). Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet, 382(9890), 427–451. https://doi.org/10.1016/S0140-6736(13)60937-X
- Chaparro, C. M., & Suchdev, P. S. (2019). Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Annals of the New Yok Academy of Sciences, 1450(1), 15–31. Annals of the New York academy of sciences. https://doi.org/10.1111/nyas.14092.Anemia
- Daba, G., Beyene, F., Fekadu, H., & Garoma, W. (2013). Assessment of knowledge of pregnant mothers on maternal nutrition and associated factors in Guto Gida Woreda, East Wollega Zone, Ethiopia. Journal of Nutrition and Food Science, 3, 235.
- Ghislain, K., & Manfred, M. (2012). Prevalence and risk factors in a malaria-endemic Area in Benin. The American Journal of Tropical Medicine and Hygiene, 87(3), 418–424. https://doi.org/10.4269/ajtmh.2012.11-0706
- Gogoi, M. & Prusty, R. (2013). Changing patterns of social inequalities in anemia among women in India: cross-sectional study using nationally representative data. Journal of North east India Studies, 3(1), 75–84.
- Gupta, N., & Kochar, G. K. (2009). Role of nutrition education in improving the nutritional awareness among adolescent girls. International Journal of Nutrition and Wellness, 7(1), 1-4.
- Jalambo, M. O., Sharif, R., Naser, I. A., & Karim, N. A. (2017). Improvement in knowledge, attitude and practice of iron deficiency anaemia among iron-deficient female adolescents after nutritional educational intervention. Global Journal of Health Science, 9(7), 15. https://doi.org/10.5539/gjhs.v9n7p15
- Khoshnevisan, F., Kimiagar, M., Kalantaree, N., Valaee, N., & Shaheedee, N. (2004). Effect of nutrition education and diet modification in iron depleted preschool children in nurseries in Tehran: A pilot study. International Journal for Vitamin and Nutrition Research, 74(4), 264–268. https://doi.org/10.1024/0300-9831.74.4.264
- Latifa, M. F., Manal, H. A., & Nihal, S. S. (2012). Nutritional awareness of women during pregnancy. The Journal of American Science, 8(7), 494–502.
- Mbwana, H. A., Kinabo, J., Lambert, C., & Bielsalski, H. K. (2016). Determinants of household dietary practices in rural Tanzania. Implications for nutrition interventions. Cogent Food and Agriculture, 13, 1–13
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), and ICF. 2016. Tanzania demographic and health survey and malaria indicator survey (TDHS-MIS) 2015–16. Dar es Salaam, Tanzania, and Rockville, Maryland, USA: MoHCDGEC, MoH, NBS, OCGS, and ICF.
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], Tanzania Food and Nutrition Centre (TFNC), National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS) [Zanzibar] and UNICEF. 2018. Tanzania national nutrition survey using SMART methodology (TNNS) 2018. Dar es Salaam, Tanzania: MoHCDGEC, MoH, TFNC, NBS, OCGS, and UNICEF.
- Moore, J., Pawloski, L., Rodriguez, C., Lumbi, L., & Ailinger, R. (2009). The effect of a nutrition education program on the nutritional knowledge, hemoglobin levels, and nutritional status of Nicaraguan adolescent girls. Public Health Nurtirion, 26(2), 144–152.
- Mutabazi, K. D. (2013). Identifying, Defining and Typologizing Food Value Chanis and Upgrading Strategies, 50. A Trans-SEC document, Morogoro.
- Rani, M. A., Shriraam, V., Zachariah, R., Harries, A. D., Satyanarayana, S., Tetali, S., Anchala, R., Muthukumar, D., & Sathiyasekaran, B. (2013). Does a nutrition education programme change the knowledge and practice of healthy diets among high school adolescents in Chennai, India? Health Education Journal, 72(6), 733–741. https://doi.org/10.1177/0017896912461093
- Ronner, E. & Giller, K. E. (2013). Background information on agronomy, farming systems and on going projects on grain legumes in Tanzania. (Milestone; No. S. 1. 2. 2). N2Africa
- Ryoo, E. (2011). Adolescent nutrition: What do pediatricians do? Korean Journal of Pediatrics, 54(7), 287–291. https://doi.org/10.3345/kjp.2011.54.7.287
- Scott, S. P., Chen-Edinboro, L. P., Caulfield, L. E., & Murray-Kolb, L. (2014). The impact of anemia on child mortality: An updated review. Nutrients, 6(12), 5915–5932. https://doi.org/10.3390/nu6125915
- Spendlove, J. K., Heaney, S. E., Gifford, J. A., Prvan, T., Denyer, G. S., & O’Connor, H. T. (2012). Evaluation of general nutrition knowledge in elite Australian athletes. British Journal of Nutrition, 107(12), 1871–1880. https://doi.org/10.1017/S0007114511005125
- Weise, A. (2012). WHA global nutrition targets 2025: Low birth weight policy brief. W.H.O Publication (pp. 1–7). https://doi.org/WHO/NMH/NHD/14.3
- WHO. (2011). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and mineral information system. Geneva, WHO. (WHO/NMH/NHD/11.1)
- WHO. (2014). Global nutrition targets 2025, anaemia policy brief, targets 50% reduction of anaemia in women of reproductive age.