
Abstract
We report a case of post-traumatic trigger finger due to a partial longitudinal tear of the flexor digitorum superficialis. The suspect came from the clinical history and the young age of the patient. It was successfully treated with tendon flap suture and pulley A1 release.
Introduction
The trigger finger is in the clinical practice, frequently caused by stenosing tenosynovitis at the A1 pulley characterized by pain, swelling and a triggering sensation with the limitation of finger motion. The first treatment is conservative using anti-inflammatory drugs and steroid injection, but some resistant cases may need surgery.[Citation1]
Post-traumatic trigger finger is a rare case of resistant trigger finger that can be suspected recording an accurate clinical history and in case of resistant trigger finger after anti-inflammatory drugs therapy and steroid injection.[Citation2–6].
We report a case of post-traumatic trigger finger due to a partial longitudinal tear of the flexor digitorum superficialis.
Case report
A healthy 22-year-old Caucasian male referred to our department suffering from pain and limited range of motion (ROM) of the right ring finger. The patient sustained in August 2015 a penetrating injury on the palm of the right hand during his sport activity. He did not refer to any emergency department or general pratictioner, the wound was small and healed naturally. One month later pain started and limitation of ROM of the right ring finger gradually worsened. Because of his clinical disorders, a trigger finger was diagnosed by another orthopedic who performed a steroid injection. The treatment was ineffective, then he referred to our department in November 2015. The clinical examination showed a small scar on the palm, located proximally to the fourth metacarpophalangeal joint and the ROM of the proximal interphalangeal (PIP) joint of the ring finger was limited to 40 degrees of extension and complete (100 degrees) in flexion, both in passive and active motion. The feeling of numbness just under the scar, the first steroid injection that was not effective and the young age of the patient, led us to perform an ultrasound examination of the hand tendons (), which showed a suspect tear of the flexor digitorum superficialis tendon of the ring finger, proximally to the pulley A1 that appeared thickened. The surgical exploration of the tendon was the treatment of choice, which was performed 2 months and 10 days from the injury.
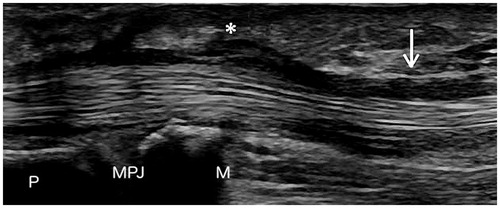
Figure 1. The ultrasounds examination shows an irregular region (arrow) of the flexor digitorum superficialis tendon suggestive of a partial rupture, accompanied by the thickening of the pulley A1 (asterisk). P: Proximal Phalanx; M: Metacarpus; MPJ: Metacarpo-Phalangeal Joint.
The incision was made at the pulley A1 and extended Brunner-like proximally in direction of the scar. A partial longitudinal flap-shaped tear was discovered, large approximately half of the entire tendon diameter, of the radial half of the flexor digitorum superficialis tendon that hooked at the entrance of the A1 pulley (). The flexor digitorum profundus tendon was intact. Because of the size of the flap-shaped tear, it was decided not to remove it, but it was sutured to the tendon in anatomic position with simple stitches (nylon 4-0) and the pulley A1 release completed the procedure to avoid risk of post-operative re-triggering. The examination during surgery showed the restoration of ring finger ROM (0–100 degrees) and the disappearance of the trigger, then the exploration of the distal pulleys (A2 and A3) was not necessary. Also, a capsulotomy of the PIP was not necessary because the limitation of ROM was not due to a capsular contracture. The patient was recommended to frequently move the fingers even with the bandage, to prevent the formation of adhesions. The cutaneous sutures were removed after 15 days. There was no need for physiotherapy as the ROM has been completely restored almost immediately. After 3 months of follow-up, no evidence of relapse was recorded and the ROM was 0–100 degrees.
Figure 2. The picture shows the longitudinal partial flap-shaped tear of the flexor digitorum superficialis.

Discussion
Most of the patients affected by trigger fingers are treated with anti-inflammatory drugs or steroid injection.[Citation1] The success rate of the single-dose of a steroid injection is reported to be 50% and when the conservative treatment fails, open A1 pulley release has a success rate of approximately 100%.[Citation7]
In literature some cases of resistant trigger finger caused by rare conditions, such as phalangeal osteochondroma,[Citation8] tendon sheets tumor (fibroma or giant cell tumor) [Citation9] or calcifying tenosynovitis [Citation10] have been reported. More frequent, but still rare in the clinical practice, is the trigger finger due to a partial tear of the flexor digitorum. To our knowledge, there are only few reports in literature.[Citation2–10] Previous reports advised the imaging support for the diagnosis of triggering after partial flexor tendon tear. Fujiwara reported a case that was diagnosed with the use of ultrasound.[Citation6] More recently, Okano and Couceiro in two different reports used MRI for the diagnosis.[Citation3,Citation5]
Our recent case, together with the other few reported in literature, demonstrates that the diagnosis of trigger finger, although does not present difficulties in the majority of the cases, have to be supported by an accurate clinical history and clinical examination, because in some cases it can be the consequence of rare clinical conditions. In selected cases, mostly if post-traumatic, the ultrasound imaging or the MRI can be used to perform a correct diagnosis, and subsequently a correct treatment.
Disclosure statement
The authors declares that there is no conflict of interest regarding the publication of this paper.
References
- Bonnici AV, Spencer JD. A survey of trigger finger in adults. J Hand Surg Br. 1988;13:202.
- Ceran F, Basat SO, Basaran K, et al. Five-years trigger finger due to partial flexor tendon laceration in a child. J Hand Microsurg. 2015;7:228–229.
- Couceiro J, Fraga J, Sanmartin M. Trigger finger following partial flexor tendon laceration: magnetic resonance imaging-assisted diagnosis. Int J Surg Case Rep. 2015;9:112–114.
- Seki Y, Kuroda H. Locking finger due to a partial laceration of the flexor digitorum superficialis tendon: a case report. Hand Surg. 2014;19:437–439.
- Okano T, Hidaka N, Nakamura H, Partial laceration of the flexor tendon as an unusual cause of trigger finger. J Plast Surg Hand Surg. 2011;45:248–251.
- Fujiwara M, A case of trigger finger following partial laceration of flexor digitorum superficialis and review of the literature. Arch Orthop Trauma Surg. 2005;125:430–432.
- Newport ML, Lane LB, Stuchin SA. Treatment of trigger finger by steroid injection. J Hand Surg (Am). 1990;15:748–750.
- Al-Harthy A, Rayan GM. Phalangeal osteochondroma: a cause of childhood trigger finger. J Plast Surg. 2003;56B:161–163.
- Oni OOA. A tendon sheath tumour presenting as trigger finger. J Hand Surg. 1984;9B:340.
- Seiler JG III, Kerwin GA. Adolescent trigger finger secondary to post-traumatic chronic calcific tendonitis. J Hand Surg. 1995;20A:425–427.