
Abstract
High-pressure delivery devices for paint and other substances can lead to severe injuries of the hand without immediate surgical debridement. We present a case of a high-pressure paint gun injury treated surgically with full resolution of function. A systematic review of the literature details outcomes of similar injuries.
Introduction
Injections from high-pressure, airless paint-guns are uncommon industrial accidents that may result in acute injuries, usually to the nondominant hand [Citation1]. They may appear innocuous because of the small size of the entrance wound. These injuries commonly require emergent management including immediate surgical debridement to avoid tissue necrosis and loss of hand function [Citation2]. Successful treatment of this injury hinges on early recognition and intervention [Citation3]. Delayed treatment can result in irreversible soft tissue damage, lifelong morbidity, and even amputation. Rarely oleogranulomas, fibrohistiocytic tumours and squamous cell carcinoma have been described as late complications [Citation1,Citation4–7]. We present a case of paint gun injury that was successfully debrided and managed with full return of function.
Illustrative case
A healthy 57 year-old-male painter presented to urgent-care with a pinpoint entrance wound () on the radial aspect of the right long finger middle phalanx from a pressurised latex paint sprayer. Radiographs were obtained (). Operative exploration involved exposure of the neurovascular bundles and flexor sheath of the finger () and debridement. The fresh paint was removed with saline irrigation and skin loosely closed. IV antibiotics and pain control with an infraclavicular block permitted bedside soap and water soaks for 48 h postoperatively. He had complete return of sensation with normal range of motion post latex paint evacuation. Skin edges were loosely approximated, and the finger healed by secondary intention. Hand therapy was performed as per institutional protocol.
Figure 1. Entrance wound on the radial aspect of the right long finger middle phalanx.

Figure 2. Radiograph demonstrating foreign material in the volar aspect of the right long finger, extending far beyond the injection site, lateral (left) and AP (right) views.

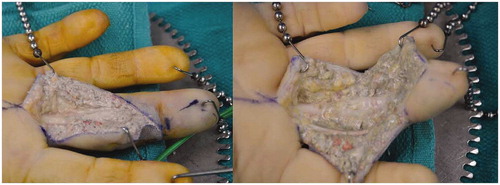
Figure 3. (left) Operative exploration with exposure of the neurovascular bundles and flexor sheath of the finger. The fresh white paint is clearly visible; (right) After extensive washout and initial debridement.
Methods
A review of the pertinent literature was performed using a search on the National Institute of Health’s PubMed database using the key phrases “high-pressure injection injury”, “paint gun injury”, or “pressure gun injury”, inclusive of “hand”. The initial search yielded 205 articles. Further inclusion criteria consisting of case reports available in the English language narrowed the search to 83 articles. Additional eligibility criteria including high-pressure injection and injuries pertaining to the hand reduced the available articles to 61 [Citation3–63]. Previous reviews have noted that high-pressure injection of air and water were not associated with the same complications as the injection of other substances and did not generally require surgical treatment, so articles detailing air or water injections were further excluded [Citation8]. This left 49 articles with 115 cases for review. We present a summary of these case reports, as well as an overview of recent developments in the literature.
Results
Although a rare occurrence, high-pressure injections of the hand have been frequently reported throughout the literature. The population included in our review was predominantly young men, with an average age of 33% and 96% male. Many described occupations that required usage of high-pressure equipment. The injured hand in the prototypical case is often the patient’s non-dominant hand, usually the left hand, due to the gun being operated in the patient’s dominant hand. Instances such as leaks along the hose of a high-pressure system caused high-pressure injection to either hand. A unique cohort noted an accidental injection while injecting high-pressure vaccines into livestock, which were to the dorsum of the hand [Citation9].
The most common material injected was paint, in 42% of cases, followed by hydraulic fluid in 17%. The type of paint was not always disclosed, but previous reports have noted an increasing incidence of complications with oil-based paint, rather than water-based [Citation8,Citation10]. Latex paints are increasing more widely used and would demonstrate a lower risk of amputation than other paints. We recorded a 17% amputation rate of paint injection, which was lower than other caustic substances, but a 35% rate of necrosis. Hydraulic fluid presented a higher infection rate at 50% but a lower amputation and necrosis rate. The most necrotic substances were noted to be dry cleaning solvent, gasoline, and petroleum ().
Table 1. Number of cases of each type of injected material.
The pressure of injection was not widely reported but ranged from 1800 psi to 4350. A pressure of only 100 psi is necessary to penetrate the skin [Citation11]. These pressures can avulse tendons, destroy vasculature, and cause significant neuropathy. Of the 17 cases that noted the injection pressure, pressures over 2500 psi had higher rates of necrosis and neuropathy but resulted in comparable amputation rates with lower pressures. Interestingly, half of the cases with pressures under 2500 psi developed infections, compared to 14% and no instances in pressures over 2500 and over 3500, respectively.
The index finger was the most common site of injection, followed by the long finger. This correlates with the standard mechanism of injury being an accidental discharge of the pressure gun while having one’s fingers over the nozzle. While a small number of cases were associated with the thumb, they described higher rates of complications, including infection, neuropathy, and the necessity of a subsequent graft, as well as persistent functional impairment. Index finger injuries reported similar instances of necrosis and amputation as thumb injuries but were less likely to report functional impairment, particularly after amputation. The material injected has been noted to follow the neurovascular structures when injected into the digits.
The time between injury and surgery has been known to correlate with severity of symptoms. Within the reviewed cases, time at presentation varied from within 1 h–6 years. When the outliers of 6 months, 2 years, and 6 years were omitted from the calculation, the average time of presentation was 34 h. Often, the patients complained of little to no pain upon injection, with a small injection injury. Several presented to the emergency room and were discharged with antibiotics and tetanus boosters without recognition of the need for surgical debridement. These patients generally develop more severe symptoms within 24 h that prompt them to return to the emergency room, at which point the urgency for debridement is recognised, and many can receive digit-preserving treatment.
After debridement, one-third of the patients experienced necrosis, a natural progression of the injury pattern, and one-third exhibited signs of infection. High-pressure injuries often require multiple debridements, which is further complicated by the need to treat infection or necrosis. Neuropathy was associated in fewer cases but with all of the reported injection areas in the hand, and often with residual pain or strength impairment. Grafts were warranted in 17% of cases to restore perfusion to the affected area. We report an overall amputation rate of only 13%, indicating that amputation may be less common than previously reported. Index finger and thumb injuries were associated with the highest rates of amputation at 34% and 38%, respectively. Patients reported resolution of symptoms and adequate functionality of the hand in 42% of cases ().
Table 2. Rate of complications of each case and the resulting outcomes.
While few cases reported long-term follow-up, several cases involved long-term complications of high-pressure injuries. Three reports included cases of fibrohistiocytic tumour and three detailed granuloma formation. Two of the patients reported adequate surgical debridement within a couple of days after injury, but the rest did not seek or receive proper treatment at the time. All of these patients reported increasing pain and swelling at the site of injury, and the masses were excised under surgical exploration of the site. Some patients that had long-term follow up also reported a residual loss of strength in the affected hand.
Discussion
High-pressure injection injuries are catastrophic due to both the mechanical force of injection and the introduction of caustic substances into the tissue. Those operating these types of high-pressure delivery devices are often those working in painting, mechanics, and farming [Citation12]. The population affected is predominantly young men who accidentally discharge a pressure gun while cleaning the equipment or test the gun by placing a finger in front of the nozzle, as commonly practiced with low-pressure equipment [Citation12]. Most patients describe a benign presentation with little pain or indication of severe trauma. This can lead to dangerous delaying of medical treatment, either by the patient themselves not seeking treatment or the dismissal of patients from the emergency room by providers not familiar with this type of injury.
Of additional concern is the ability of the substance, combined with the subsequent oedema and swelling, to cause a compartment-like syndrome of the affected space, leading to increased pain and impaired functionality of the hand over time without treatment. This can result in further damage from resulting vasospasm, thrombosis, and ischaemia [Citation13]. The more caustic substances have the potential to raise a stronger inflammatory response, further increasing the depth of injury to the tissue.
The standard of care for high-pressure injection injuries includes administration of antibiotics, tetanus prophylaxis, and immediate recommendation for surgical debridement. Third generation cephalosporins are often commonly administered [Citation14]. Radiographs can be helpful in located the foreign material in some circumstances, and patients may demonstrate an elevated white blood cell count a few hours after injury [Citation11]. As stated earlier, air and water injection injuries can be treated conservatively without immediate surgical debridement but should be monitored closely to avoid progression to compartment syndrome or other emergent complications [Citation8]. Injuries from animal vaccine injection can also be monitored without immediate surgical intervention if the doses are less than 0.5 mL. These injuries are specifically at risk for developing infections and inflammatory response to the vaccine components, so they must be monitored appropriately [Citation15]. Corticosteroids have been utilised to dampen the inflammatory response after high-pressure injection injuries with varied results and no clear consensus on its efficacy, warranting further investigation [Citation11]. Additionally, a recent cohort utilised vacuum therapy to treat high-pressure injection injuries and found positive results in decreasing tissue oedema and the further spread of injected substances throughout the tissue [Citation16].
Wong et al. suggested a treatment plan based on the severity classification of the high-pressure injection. Mild cases with low-risk factors can be observed closely with antibiotics, while moderate risk cases should proceed directly to surgical debridement with delayed closure. Severe cases included injection of paint or caustic substances, very high-pressure injections, injuries with loss of sensation or circulation, and delayed patient presentation. In these cases, repeated debridements staged amputations, and flap reconstruction should all be considered as potential treatment options [Citation17]. A wide incision upon debridement is generally recommended to remove all necrosed tissue and as much of the foreign substance as possible, then to observe the patient radiographically and symptomatically to determine if further surgical exploration is warranted [Citation16]. Patients should be educated on the potential of amputation and late complications that may present after this type of injury.
Previous cohort studies with significant follow up have noted diminished sensation and two-point discrimination at the fingertips in all patients with digital injuries. Patients often heal gradually with significant flexion impairment and necessitate physiotherapy [Citation19]. While manageable functionality and return to work are undoubtedly possible after high-pressure injuries, patients should be aware of the long recovery process and risk of persistent complications. It should be expected that patients will exhibit some residual strength impairments in the affected hand or digit. In one cohort, only 43% of followed patients were able to return to their previous employment [Citation20]. Proper education on the safe operative usage of high-pressure equipment and the need for immediate medical treatment upon injury is imperative, as it could decrease the rates of injury and cases of delayed presentation. As providers are increasingly more aware of proper management in the emergency room and upon surgical intervention, patients may more commonly recover without significant long-term repercussions from high-pressure injection injuries.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Saadat P, Turla S, Vadmal M, et al. Fibrohistiocytic tumor of the hand after high-pressure paintgun injury: 2 case reports. J Hand Surg Am. 2005;30:404–408.
- Collins M, McGauvran A, Elhassan B. High-pressure injection injury of the hand: peculiar MRI features and treatment implications. Skeletal Radiol. 2019;48(2):295–299.
- Ryan AT, Johnstone BR. High-pressure injection injury: benign appearance belies potentially devastating consequences. Med J Aust. 2017;11:477.
- Bean B, Cook S, Loeffler BJ, et al. High-pressure water injection injuries of the hand may not be trivial. Orthopedics. 2018;41:e245–e251.
- Mauzo SH, Swaby MG, Covinsky MH, et al. Tumefactive foreign body giant cell reaction following high-pressure paint injection injury: a case report and review of literature. J Cutan Pathol. 2017;44:474–476.
- Hayes CW, Pan HC. High-pressure injection injuries to the hand. South Med J. 1982;75:1491–1516.
- Vasilevski D, Noorbergen M, Depierreux M, et al. High-pressure injection injuries to the hand. Am J Emerg Med. 2000;18:820–824.
- Hogan CJ, Ruland RT. High-pressure injection injuries to the upper extremity: a review of the literature. J Orthop Trauma. 2006;20:503–511.
- Couzens G, Burke FD. Veterinary high pressure injection injuries with inoculations for larger animals. J Hand Surg Br. 1995;20:497–499.
- Lozano-Calderon SA, et al. Latex paint-gun injuries of the hand: are the outcomes better? Hand (NY). 2008;3:340–345.
- Rosenwasser MP, Wei DH. High-pressure injection injuries to the hand. J Am Acad Orthop Surg. 2014;22:38–45.
- Hart RG, Smith GD, Haq A, et al. Prevention of high-pressure injection injuries to the hand. Am J Emerg Med. 2006;24:73–76.
- Cannon TA. High-pressure injection injuries of the hand. Orthop Clin North Am. 2016;47:617–624.
- Amsdell SL, Hammert WC. High-pressure injection injuries in the hand: current treatment concepts. Plast Reconstr Surg. 2013;132:586e–591e.
- Robertson CE, Ackerman NA, Burke FD, et al. Sharps and high-pressure injection injuries in veterinary and animal workers. Eur J Emerg Med. 2016;23:8–11.
- Temiz G, Şirinoğlu H, Güvercin E, et al. A useful option to obtain maximal foreign body removal and better prognosis in high-pressure injection injuries: negative pressure wound therapy with installation. J Plast Reconstr Aesthet Surg. 2016;69:570–572.
- Wong TC, Ip FK, Wu WC, et al. High-pressure injection injuries of the hand in a Chinese population. J Hand Surg Br. 2005;30:588–592.
- Pappou IP, Deal DN. High-pressure injection injuries. J Hand Surg Am. 2012;37:2404–2407.
- Bekler H, Gokce A, Beyzadeoglu T, et al. The surgical treatment and outcomes of high-pressure injection injuries of the hand. J Hand Surg Eur Vol. 2007;32:394–399.
- Wieder A, Lapid O, Plakht Y, et al. Long-term follow-up of high-pressure injection injuries to the hand. Plast Reconstr Surg. 2006;117:186–189.
- Agha FP. High-pressure paint gun injuries of hand: clinical and roentgen aspects. N Y State J Med. 1978;78:1955–1956.
- Apfelberg DB, Lash H, Maser MR, et al. High-pressure silicone injection injury of the hand. J Trauma. 1975;15:922–925.
- Barr ST, Wittenborn W, Nguyen D, et al. High-pressure cement injection injury of the hand: a case report. J Hand Surg Am. 2002;27:347–349.
- Beguin JM, Poilvache G, Van Meerbeeck J, et al. Hand injuries caused by high-pressure injection. Contribution of loco-regional anaesthesia. Ann Chir Main. 1985;4:37–42.
- Booth CM. High pressure paint gun injuries. Br Med J. 1977;2:1333–1335.
- Bourget DM, Perrone J. High-pressure decisions: recognition and management of uncommon hand injuries. J Med Toxicol. 2011;7:162–163.
- Burke PJ, Conolly WB. Paint gun injection injury of the hand: a surgical emergency. Med J Aust. 1973;2:276–278.
- Chan BK, Tham SKY, Leung M, et al. Free toe pulp transfer for digital reconstruction after high-pressure injection injury. J Hand Surg Br. 1999;24:534–538.
- Chaudhry S, Gould S, Gupta S, et al. High-pressure paint gun injection injury to the palm. Am J Orthop (Belle Mead NJ). 2013;42:379–382.
- Childress MH. High pressure injection injury of the hand . J Natl Med Assoc. 1977;69:663–664.
- Craig EV. A new high-pressure injection injury of the hand. J Hand Surg Am. 1984;9:240–242.
- del Pinal F, Herrero F, Jado E, et al. Acute thumb ischemia secondary to high-pressure injection injury: salvage by emergency decompression, radical debridement, and free hallux hemipulp transfer. J Trauma. 2001;50:571–574.
- Dickson RA. High-pressure injection injuries of the hand. A clinical, chemical and histological study. Hand. 1976;8:189–193.
- Engel J, Lin E, Tsur H, et al. Neurovascular island flap reconstruction following high-pressure injection injuries of the hand. Injury. 1981;13:181–184.
- Eroglu O, Sari E, Vural S, et al. Warning: this may be as dangerous as firearm injuries; “grease-gun injury”: a case report. Pan Afr Med J. 2015;20:40.
- Flotre M. High-pressure injection injuries of the hand. Am Fam Physician. 1992;45:2230–2234.
- Foran I, Oak NR, Meunier MJ, et al. High-pressure injection injury caused by electronic cigarette explosion: a case report. JBJS Case Connect. 2017;7:e36
- Foresman-Capuzzi J, Tadduni GT, Callahan T, et al. A 56-year-old man sustains high pressure injection trauma to his hand. J Emerg Nurs. 2006;32:310–312.
- Gutowski KA, Chu J, Choi M, et al. High-pressure hand injection injuries caused by dry cleaning solvents: case reports, review of the literature, and treatment guidelines. Plast Reconstr Surg. 2003;111:174–177.
- Herrick RT, Godsil RD, Widener JH, et al. High-pressure injection injuries to the hand. South Med J. 1980;73:896–898.
- Jebson PJ, Sanderson M, Rao VK, et al. High-pressure injection injuries of the hand. Wis Med J. 1993;92:13–16.
- Kamrani RS, Mehrpour SR, Aghamirsalim MR, et al. High-pressure plastic injection injury of the hand: case report. Occup Med (Lond). 2011;61:518–520.
- Karaharju EO, Par S. Angiography after paint-gun injury of the hand: a case report. Injury. 1977;9:66–67.
- Karlbauer A, Gasperschitz F. High-pressure injection injury: a hand-threatening emergency. J Emerg Med. 1987;5:375–379.
- Kendrick RW, Colville J. Conservative management of a high pressure injection injury to the hand. Hand. 1982;14:159–161.
- LeBlanc JV. High pressure petroleum injection injuries. J Occup Med. 1977;19:276–277.
- Lilis R, Green SM, Field J, et al. Paint spray gun injury of the hand. Report of an unusual source of lead poisoning. Jama. 1981;246:1233–1235.
- Locker J, Carstens A. High pressure injection of silica-based paint into a finger. N Z Med J. 2010;123:104–106.
- Luber KT, Rehm JP, Freeland AE, et al. High-pressure injection injuries of the hand. Orthopedics. 2005;28:129–132.
- Maxwell RJ, Dixon PL. High-pressure injection injuries of the hand: a report of three cases. ANZ J Surg. 1988;58:344–346.
- Oktem F, Oçgüder A, Altuntaş N, et al. High-pressure paint gun injection injury of the hand: a case report. J Plast Reconstr Aesthet Surg. 2009;62:e157–159.
- O’Sullivan ST, O’Donoghue JM, O’Connor TP, et al. Occupational high-pressure injection injury of the hand. Dermatology (Basel). 1997;194:311.
- Phelps DB, Hastings H, Boswick JA, et al. Systemic corticosteroid therapy for high-pressure injection injuries of the hand. J Trauma. 1977;17:206–210.
- Pinto MR, Turkula-Pinto LD, Cooney WP, et al. High-pressure injection injuries of the hand: review of 25 patients managed by open wound technique. J Hand Surg Am. 1993;18:125–130.
- Puhaindran ME, Chong AKS, Chew WYC, et al. Flap reconstruction following high-pressure injection injuries of the hand: a report of three cases. Hand Surg. 2004;09:211–219.
- Schoo MJ, Scott FA, Boswick JA, et al. High-pressure injection injuries of the hand. J Trauma. 1980;20:229–238.
- Silsby JJ. Pressure gun injection injuries of the hand. West J Med. 1976;125:271–276.
- Sirinoglu H, Ersoy B, Bayramiçli M. Late presentation of a case of high-pressure cement injection injury to the hand. J Plast Surg Hand Surg. 2013;47:331–333.
- Stiles NA. High-pressure injection injury of the hand: a surgical emergency. J Emerg Nurs. 1994;20:351–354.
- Tanaka Y, Tajima S, Yamamoto Y, et al. Successful reconstruction of a high-pressure injection injury of the hand using a first web flap of the foot. J Reconstr Microsurg. 1993;9:55–59.
- Utrobicic I, Pogorelić Z, Druzijanić N. High-pressure injection injuries of the hand–report of two cases. Acta Chir Belg. 2011;111:46–50.
- Vente JP, Bolhuis RJ. Airless paint-gun injuries of the hand: a report of three cases. Injury. 1984;16:91–93.
- Vilke GM, Snyder B. High pressure paint spray gun injury. J Emerg Med. 2002;23:203–204.