
Abstract
We report the case of a HIV-seronegative 57 year-old man, with known classic Kaposi’s disease and in whom a secondary localization in the upper left limb led to carpal and metacarpal lysis in the left hand. This unfavorable local evolution led to left transhumeral amputation.
Introduction
Kaposi sarcoma (KS) was first described by the Hungarian dermatologist Moritz Kaposi in 1872. It is a slow-growing rare cancer characterized by generally asymptomatic purplish, pink or blue macular lesions of the skin and mucous membranes. It is defined as an angio-proliferative mesenchymal disorder that affects blood and lymphatic endothelial cells, and that is induced by viral growth factors, such as interleukin 6, and human herpesvirus-8 (HHV8) [Citation1].
HHV8 is therefore considered as the etiological agent of not only KS but also other diseases including multicentric Castleman disease or primary effusion lymphoma [Citation2]. KS came to the forefront of public attention during the acquired immunodeficiency syndrome (AIDS) epidemic when it was commonly found in severely immunodepressed patients co-infected with human immunodeficiency virus (HIV) and the opportunistic HHV8. KS in HIV-patient could lead to fatal complications specially with the Kaposi Sarcoma Immune Reconstitution Syndrome [Citation3].
In total there are four forms of KS: the classic form (or Mediterranean/Eastern European endemic), the African endemic form, the iatrogenic form occurring in immunodepressed patients, and the epidemic form (associated with AIDS) also known as HIV-associated KS. KS occurring in its endemic form is referred to as Kaposi’s disease, one of which affects generally the aging population living in the Mediterranean basin.
The dermatological lesions are similar in all these forms but differ in terms of their severity. The diagnosis is obtained by histology of lesion biopsies and immunolabeling of HHV8 or seropositivity for HHV8 antibodies [Citation4]. We report a case of classic Kaposi’s disease leading to osteolysis of the bones in the hand.
Case report
A 57 year-old HIV-seronegative patient of Northwest African origin was first diagnosed with classic KS in 2009 upon discovery of erythematous macular lesions on the right leg. A first line treatment with vinblastine was initiated but stopped 8 months later due to inefficacy and skin toxicity. A change of treatment to doxorubicin was well tolerated and permitted a good initial response. However, a recurrence of the lesions 3 years later required a change in treatment to etoposide which the patient took for 2 more years and which permitted a good response.
A further recurrence of the lesions occurred 3 years later on the right lower limb but was accompanied this time by the appearance of a lesion on the left upper limb. Treatment with doxorubicin was initiated for 7 months and initially worked well with a favorable response of lesions on the upper left limb. However, a worsening of lesions at this site one year later required new therapeutic options including radiotherapy with no success.
An X-ray showed local worsening of the Kaposi’s disease leading to osteolysis at the base of the 3rd and 4th metacarpal bones (). A bone biopsy and CT scan were performed () showing the evolution of the disease with carpal bone involvement. In view of the successive failed treatment attempts and the unfavorable disease evolution (), the decision was made to perform a transhumeral amputation. The computed tomography shows that tumor has spread in the soft tissue up to the distal third of the forearm without osteolytic lesions at that level. Skin was red, swollen with induration up to the elbow. Transhumeral amputation was chosen over elbow disarticulation to better accommodate future upper extremity prothesis. Immunohistochemical investigations found cells positive for ERG (clone EP111) and HHV8 (clone 13B10). Successful resection with healthy margins was confirmed by analyses of the amputated limb-part. The amputation stump healed well () and no local recurrence had occurred at the six month follow-up but a progression of the disease was found at other sites: sub-diaphragmatic, small intestinal and multifocal bone (). The patient experienced no phantom limb pain and was still alive one year after surgery.
Figure 1. X ray of the left hand showing complete lysis of the Fourth metacarpal bones.

Figure 2. CT Scan with bone and vascular reconstruction.
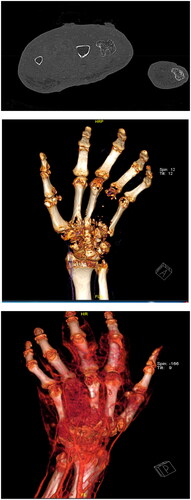
Figure 3. Lesions of the hand with a lateral view before surgery.

Figure 4. Lesions of the hand with a dorsal view before surgery.

Figure 5. Lesions of the hand with a palmar view before surgery.

Figure 6. Appearance of the amputation stump at 6-month follow-up.

Figure 7. PET-SCAN 6 months after surgery showing sub-diaphragmatic, small intestinal and multifocal bone lesions. There was no recurrence on the upper-limb.

Discussion
Kaposi sarcoma (KS) is a malignant vascular tumor characterized by fusiform and dilated mesenchymal cells. The dermatological lesions are characterized by purplish red erythematous macules that evolve, mainly slowly, towards plaques or nodules. The disease classically first appears in the lower limb, as in the case presented here. It is generally characterized into four groups. A new category has been evoked to group together KS occurring in patients negative for HIV but having had homosexual contact [Citation5, Citation6]. Our patient did not report having male partners. The so-called classic form of KS affects the aging population originating in the Mediterranean basin, or Central and Eastern Europe. Most reported cases involve patients over 75 years of age and classic KS affecting patients below 50 years of age is rare with an incidence of between 4 and 8% [Citation7].
Bone involvement, while rare with a frequency of 4.5% according to Ritz Quillac et al. [Citation8, Citation9], can occur in all forms of KS but is most frequent in classic KS with a prevalence up to 1 in 3 patients with Kaposi’s disease. It generally arises through contiguity with a soft tissue lesion, as reported in the present case. The bone lesions are generally osteolytic with complete destruction of the bone.
To our knowledge, our case represents a rare example of classic Kaposi’s disease not only affecting the upper limb but also involving osteolysis in the hand. In one review of the literature, Caponetti and al. reported 66 cases of KS with musculoskeletal system involvement [Citation10]. Involvement of the upper limb remains rare. Only few cases of classic Kaposi’s disease with metacarpal involvement have previously been reported [Citation11]. One case of classic KS affecting the hand but with no bone involvement was previously reported in a 68 year-old woman [Citation12]. More recently, Bas et al. reported a case of Kaposiform hemangioendothelioma in the upper limb of a newborn baby [Citation13]. Aim and al. reported a patient with isolated KS in the finger with bone involvement but no cutaneous lesion upon clinical examination [Citation14]. One report did concern classic KS leading to osteolysis in the hand that required amputation, however the patient was over 100 years of age and of Moroccan origin [Citation15]. Classic Kaposi’s disease, unlike the endemic form, does generally occur in older patients (more than 75 years of age), and yet our patient developed the disease in early age.
Involvement of the upper limb in KS, particularly when leading to osteolysis, remains therefore rare, especially in Europe. Amputation remains an efficient solution for local control and sepsis prevention but drug therapies should be pursued to stop dissemination.
Ethical approval
Written informed consent was obtained from the patient to participate in this study for the publication of this case report and accompanying images. A copy of the written consent form is available for review on request.
Disclosure statement
The authors declare having no competing interests.
References
- Marrigio G et al. Kaposi sarcoma herpesvirus pathogenesis. Phil Trans R Soc B Biol Sci. 2017;372(1732):20160275.
- Cesarman E, Chadburn A, Rubinstein PG, et al. KSHV/HHV8 mediated hematologic diseases. Blood. 2022;139(7):1013–1025. DOI: 10.1182/blood.2020005470.
- Dumic I, Radovanovic M, Igandan O, et al. A fatal case of Kaposi sarcoma immune reconstitution syndrome (KS-IRIS) complicated by kaposi sarcoma inflammatory cytokine syndrome (KICS) or multicentric castleman disease (MCD): a case report and review. Am J Case Rep. 2020;21:e926433. DOI: 10.12659/AJCR.926433.
- Dupin N et al. Update on oncogenesis and therapy for Kaposi sarcoma. Curr Opin Oncol. 2020;32(2):122–128. DOI: 10.1097/CCO.0000000000000601.
- Swali et al. Kaposi sarcoma of the medial foot in an MSM, HIV-negative man: a fifth clinical variant. J Clin Aesthet Dermatol. 2020;13(10):42–44.
- Lanternier F, Lebbé C, Schartz N, et al. Kaposi’s sarcoma in HIV-negative men having sex with men. AIDS. 2008;22(10):1163–1168. DOI: 10.1097/QAD.0b013e3283031a8a.
- Lorenzo et al. Update on classic Kaposi sarcoma therapy: new look at old disease. Crit Rev Oncol/Hematol. 2008;68(3):242–224.
- Ritz-Quillac L, Machet L, Machet MC, et al. Bone involvement in a case of Kaposi’s sarcoma. Dermatology. 1999;198(1):73–74. DOI: 10.1159/000018069.
- Pantanowtiz et al. Kaposi sarcoma in unsual locations. BMC Cancer. 2008;8:190.
- Caponetti et al. Kaposi sarcoma of the musculoskeletal system. A review of 66 patients. Cancer. 2007;109(6):15.
- Morgan L et al. Kaposi’s sarcoma in bone: a case report with unsual radiographic findings and an abnormal radioisotope scan. Rev Interarm Radiol. 1976;1(2):37–41.
- Kaposi’s sarcoma of the hand mimicking squamous cell carcinoma in a woman with no evidence of HIV infection: a case report. J Med Case Rep. 2008;2:213.
- Kosmidis Bas et al. Upper arm life-saving amputation of a 12-day-old neonate due to extensive vascular tumor of the upper extremity. Acta Orthop Traumatol Turc. 2020;54(1):114–117.
- Aïm F, Rosier L, Dumontier C, et al. Isolated kaposi sarcoma of the finger pulp in AIDS patient. Orthop Traumatol Res. 2012;98(1):126–128. DOI: 10.1016/j.otsr.2011.09.017.
- Sbiyaa M, Alaoui AE, Bardai ME, et al. L’atteinte osseuse dans le sarcome de kaposi classique et agressif: à propos d’un cas. Pan Afr Med J. 2016;23:196. DOI: 10.11604/pamj.2016.23.196.8632.