
Abstract
Carney complex is a rare autosomal dominant familiar multiple neoplasia syndrome combined with cardiocutaneous manifestations. Our report describes a Carney complex case with bilateral myxoid fibroadenomas that led to a bilateral mastectomy. An 18-year-old female patient presented at our clinic with complaints of multiple palpable lumps in her breasts bilaterally. On physical examination the patient had also multiple pigmented lentiginous lesions on her face, body and her sclerae, blue nevi on her trunk and upper extremities and a round moon-shaped face. The diagnosis of Carney syndrome was decided upon imaging, biopsies and genetic analysis. The patient underwent a bilateral mastectomy as a prophylactic treatment plan with tissue expanders’ placement. Breast myxomatosis due to Carney complex is a common characteristic in female patients. Prophylactic mastectomy must be considered as a therapeutic intervention in these cases since it provides a definite treatment, with minimal side effects and excellent outcomes.
Introduction
Carney complex is a rare disorder firstly described by J. Aidan Carney in 1985. It is a rare autosomal dominant familiar multiple neoplasia syndrome combined with cardiocutaneous manifestations. It is characterized by a complex of multiple myxomas, skin pigmentation (both pigmented like lentigines and blue nevi and non-pigmented like cutaneous myxomas) and/or, endocrine overactivity [Citation1].
Heterozygous inactivating mutations of PRKAR1A on chromosome 17q22-24 and CNC2 gene on chromosome 2p16 have been associated with this complex [Citation2,Citation3].
According to NORD (National Organization for Rare Disorders) approximately only 750 patients have been registered with Carney complex since its identification, due to the complexity and rarity of the disease [Citation4]. Epidemiologically, 70% of them have a familiar history, whereas the remaining 30% presented with a de novo germline mutation. Two thirds are female patients and there is also no predilection according to ethnicity [Citation5].
Case report presentation
An 18-year-old Caucasian, female patient presented at our clinic with complaints of multiple palpable lumps in her breasts bilaterally. On physical examination the patient had multiple pigmented lentiginous lesions on her face, body and her sclerae bilaterally, blue nevi on her trunk and upper extremities and a round moon-shaped face.
Upon ultrasonographic evaluation multiple compact nodules-fibroadenomas were found in both breasts, with the largest being in the upper outer quadrant of the left breast with diameter of 7.8 cm.
She had previously undergone total thyroidectomy in 2018 with the diagnosis of follicular adenoma and a removal of a large nodule of the left breast, due to its large size and pain, with a histopathology report suggesting fibroadenoma with myxoid stroma.
An excision biopsy of two nodules of the right breast was performed with myxoid fibroadenoma diagnosis, supporting our diagnosis of Carney complex.
On magnetic resonance imaging, multiple compact fibroadenomas were found on bilateral breasts, with high signal intensity on T2 and T2/FS images, with internal septations without restriction of diffusion, compatible with multiple myxoid fibroadenomas.
Furthermore, there were a couple of axillary lymph nodes and prominent internal mammary lymph nodes bilaterally.
In addition, there was an abnormality of soft tissue density at the anterior mediastinum, measuring 11 mm in maximum thickness, suggesting a prominent thymus.
All the above findings suggested a possibility of Carney complex. Further laboratory evaluation took place. Hormonal testing showed no abnormalities in testosterone, prolactin, PTH and DHEA-S levels.
Gene analysis was then performed with findings of PRHAR1A gene mutation, heterozygous for a missense variant of uncertain significance in exon 3 of this gene. This mutation has never been reported in the gnomAD database.
Genetic testing was performed to the parents as well, finding only the father positive to the same gene mutation.
Various conservative treatment plans were discussed with the patient, but none proved to provide a definite solution/treatment. Excision of big lobules was performed in the past with temporary alleviation of the patients’ pain symptoms and the recurrent surgeries were affecting her quality of life. The patient had also several sessions with our clinic psychologist and was assessed thoroughly before deciding upon the final solution of a bilateral mastectomy.
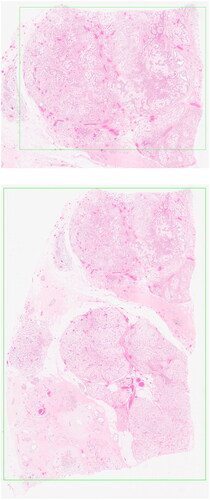
The patient underwent a bilateral skin-sparing mastectomy and placement of tissue expanders (smooth, Motiva Flora®) subcutaneously. Histopathology reported multiple myxoid fibroadenomas in both breasts, compatible with Carney complex syndrome, with disruption of normal breast parenchyma architecture. and show macroscopically and histologically the fibroadenoma.
Figure 1. Macroscopic image of myxoid fibroadenoma.

Figure 2. Histology slides with hematoxylin & eosin staining of myxoid fibroadenoma.
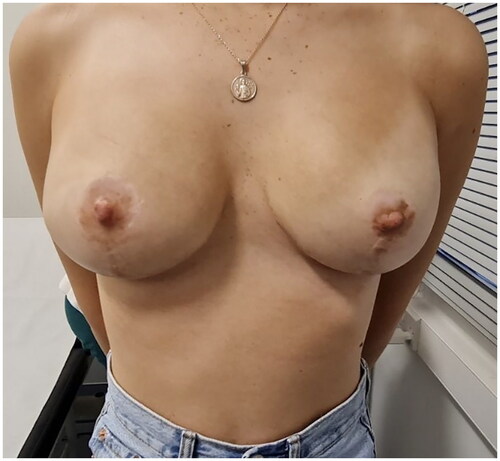
Wound care was minimal, the patient was advised to wear a medical bra and regular visits to the outpatient clinic for follow-up and further filling of the tissue expanders at regular intervals until the desired size was achieved. and show the patient prior and post-mastectomy. After one year a second surgery took place and the expanders were replaced with permanent silicone implants (smooth, Motiva Ergonomic®) submuscular, with again the same minimal wound care requirements and bra placement ().
Figure 3. Patient before surgery.

Figure 4. Patient one-month post-mastectomy surgery and placement of tissue expanders.

Figure 5. Patient one month after silicone implant placement.
Discussion-conclusion
Carney complex is a rare autosomal dominant multiple neoplasia syndrome. Identification of this rare disorder is difficult therefore registered cases are minimal.
Diagnosis of Carney complex is made according to a list of major and minor criteria, presented in . The list was revised in 2001 and has a sensitivity of 98%.
Table 1. Diagnosis criteria for Carney complex.
For the diagnosis to be established, two major criteria need to be fulfilled by imaging, histologically or biochemically, or one major and one minor criterium [Citation6].
Our case was unique with findings of PRHAR1A gene mutation, heterozygous for a missense variant of uncertain significance in exon 3 of this gene, never registered in the gnomAD database before. This supports the complexity of the disorder itself both in diagnosis and follow-up management.
Various conservative treatment plans were discussed about the patient, but none proved to provide a definite solution/treatment. Excision of big lobules was performed in the past with temporary alleviation of the patients’ pain symptoms.
Choice of breast implants is a big and important chapter in both esthetic and reconstructive breast surgeries. Regarding our case, the selection of the specific tissue expander was done on its unique feature of being MRI compatible (non-magnetic port), compared to the rest and wouldn’t intervene with any possible follow-up MRI that may have been required. They have a smooth surface, giving them the advantage to reduce inflammation and formation of a thinner capsule compared to the conventional tissue expanders [Citation7,Citation8].
Breast implants were again chosen due to their smooth surface, decreasing inflammation and pain from capsule formation. Ergonomic shape was chosen to mimic the shape, movement as well as the feel of the natural breast.
Another major factor for the selection of smooth implants compared to textured ones is that they provoke less pro-fibrotic inflammation that in turn minimizes foreign body immune-related seromas, capsular contracture, malposition as well as the occurrence of BIA-ALCL.
Breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) is a rare yet treatable T-cell lymphoma that develops around breast implants and not on the breast tissue itself. Incidence rate ranges from 1:2207 to 1:86000 depending on the implant used. No cases have yet been reported of this kind of cancer with smooth implants, that is mainly hypothetical due to the larger surface area of textured, hence more exposure [Citation9]
Bilateral mastectomy was performed as a prophylactic modality in treating this rare disorder, with excellent post-surgical results. Prophylactic mastectomy may be considered as a last treatment option of carney complex patients with breast myxomatosis since it provides a definite solution with minimal side effects and excellent outcomes, especially in multiple and large fibroadenomas that cause pain and discomfort to the patient, cannot be relieved with any of the conservative methods and affect the patient’s everyday life. Homologous breast reconstruction modalities, using a DIEP flap for example, could have been considered in this case but weighing the advantages vs the disadvantages of the two procedures, bilateral prophylactic mastectomy is similar carney syndrome cases should be considered as a definite treatment modality of breast myxomatosis.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Patient consent
Consent for publication of recognizable patient photographs or other identifiable material was obtained by the authors and included at the time of submission to the journal stating that the patient gave consent with the understanding that this information may be publicly available.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Carney JA, Gordon H, Carpenter PC, et al. The complex of myxomas, spotty pigmentation, and endocrine overactivity. Medicine. 1985;64(4):1–5. doi: 10.1097/00005792-198507000-00007.
- Kirschner LS, Carney JA, Pack SD, et al. Mutations of the gene encoding the protein kinase a type I-alpha regulatory subunit in patients with the carney complex. Nat Genet. 2000;26(1):89–92. doi: 10.1038/79238.
- Matyakhina L, Pack S, Kirschner LS, et al. Chromosome 2 (2p16) abnormalities in Carney complex tumours. J Med Genet. 2003;40(4):268–277. doi: 10.1136/jmg.40.4.268.
- National Organization for Rare Disorders; Carney JA. Quincy-Massachusetts: Carney complex; 2011 [cited 2023 Nov]. NORD. Available from: https://rarediseases.org/rare-diseases/carney-complex/
- Espiard S, Bertherat J. Carney complex. Front Horm Res. 2013;41:50–62. doi: 10.1159/000345669.
- Stratakis CA, Kirschner LS, Carney JA. Clinical and molecular features of the carney complex: diagnostic criteria and recommendations for patient evaluation. J Clin Endocrinol Metab. 2001;86(9):4041–4046. doi: 10.1210/jcem.86.9.7903.
- Doloff JC, Veiseh O, R de M, et al. The surface topography of silicone breast implants mediates the foreign body response in mice, rabbits and humans. Nat Biomed Eng. 2021;5(10):1115–1130. doi: 10.1038/s41551-021-00739-4.
- Establishment Labs. Post market surveillance report Q4 December. Costa Rica: Establishment Labs; 2020 [cited 2023 Nov]. Available from: https://establishmentlabs.com/wp-content/uploads/2022/12/Post-Market-Surveillance-Report-2022.pdf
- Clemens MW, Brody GS, Mahabir RC, et al. How to diagnose and treat breast implant-associated anaplastic large cell lymphoma. Plast Reconstr Surg. 2018;141(4):586e–599e. doi: 10.1097/PRS.0000000000004262.