
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Many factors influence the utilization of reproductive healthcare services in Kenya. Despite the effort by the government and other stakeholders to improve access and utilization of these services, there remains a major challenge in reaching out to marginalized segments of society. The study aims to examine the factors affecting the utilization of modern contraceptives by homeless women in Nairobi, Kenya, and draw policy recommendations based on the findings. The study utilized the logit model to analyze determinants of contraceptive utilization by homeless women in Nairobi using primary data collected from 196 households within Nairobi. The number of children per woman, age at first birth, living with a partner, drug abuse by the respondent, drug abuse by respondents’ partner, poverty, child planning, health facility delivery, neonatal death incidence, knowledge of male sterilization, never attending school, primary school attendance, secondary school attendance, operating of small business and contraceptive spending significantly affect the utilization of modern contraceptives by homeless women in Nairobi, Kenya. The majority of homeless women in Nairobi utilized injectibles (26.63%) and implants (24.07%) as a form of contraception. The government should therefore provide a contraceptive mix that incorporates these forms of contraception to ensure maximum utilization.
1. Introduction
1.1. Demand for contraceptives
Contraceptives have consistently been used all over the world leading to an improvement in contraceptive prevalence (United Nations, Department of Economic and Social Affairs, Population Division, Citation2015) Contraceptives have been credited to prevent unplanned pregnancies (Barden O’Fallon et al., Citation2018). However, despite the governments’ effort to provide subsidized contraception, many homeless women still do not utilize contraceptives. Hence, the interest in understanding the determinants of contraceptive use among homeless women in Kenya.
Contraceptive use has played a huge role in assisting women to plan the number of children they would want and the spacing they desire. Davanzo et al. (Citation2004) noted that women who had short intervals between pregnancies have a greater risk of pre-eclampsia, premature rupture of membranes, and high blood pressure. Globally, child spacing achieved through the use of modern contraceptives has been found to save the lives of more than 2 million newborns each year (Collumbien et al., Citation2004). The unmet need for contraception among homeless women should therefore be an area of interest to help reduce mortality and morbidity. Choosing to have smaller families has been found to impact the quality of children (Pailhé et al., Citation2019). Pailhe’ noted that investment per child decreases with an increase in the number of children in a household.
Homeless women also face challenges providing basic needs for their families and majority depend on social assistance to meet their daily needs (Karabanow, Citation2008). Women with lesser children, therefore, have a chance to provide sustainably for their families than women with larger families. In the labor market, homeless women face few options when it comes to job opportunities (Hossain & Alam, Citation2016). Homeless women work long hours and are often paid low wages and since they have no formal educations, chances of getting well-paying jobs are slim (Milaney et al., Citation2020). Early use of contraception improves a woman’s human capital investment and changes a woman’s career path as chances of unplanned pregnancies are eliminated (Bailey, Citation2006; Goldin & Katz, Citation2000). Contraceptive use improves the economic prospects of a woman leading to an increase in overall family income (Canning & Paul Schultz, Citation2012). Smaller family sizes have also been found to break cycles of poverty and reduce dependency on the government (Wang & Sun, Citation2016). Wang and Sun (Citation2016) argued that women with smaller families are more capable of caring for their families as they achieve more economic stability. Good spacing and smaller family sizes have also been found to affect the quality of children. Pailhé et al. (Citation2019) argue that income and family time are easily depleted when caring for a large family. Olinto et al. (Citation2013) noted a direct relationship between poverty and household size. The burden of caring for street children mainly lies with the government. The Kenyan government has over the years played an important role in rehabilitating street families (National Authority for the Campaign Against Alcohol and Drug Abuse NACADA, Citation2017) through the provision of safety nets, shelter, rehabilitation centers, etc (Embleton et al., Citation2020). The Kenyan government despite running eight rehabilitation centers for wayward kids (Consortium for Street Children, Citation2011), has also established and gazetted the Street Families Rehabilitation Fund of 2003 which aims at mobilizing funds, rehabilitating, and fertility of homeless women allowing them to care for children they can afford.
Homeless women also face inequality in access and utilization of contraceptives. Street women are characterized by low literacy levels and poor productivity, which leads to lesser social inclusion (OECD, Citation2013). A study by Grotluschen et al. (Citation2016) noted a link between low literacy and poor social outcomes. Homeless women battle stress and mental health issues that affect their productivity (Glomm & John, Citation2002) leading to high rates of unemployment (Gould & Williams, Citation2010). Homeless women do not invest in skill development for their children because of their low income (Heckman & Mosso, Citation2014) leading to a generation of street children with low productivity and life skills. Subsidized contraceptives will therefore cushion homeless women from the burden of unwanted pregnancies thereby reducing the burden of caring for many children using little resources. Street women have a difficult time getting formal employment. Many are forced to do illegal work or be part of the informal sector (Dachner & Tarasuk, Citation2002). With economic restructuring from unskilled- to skilled-based labor (Pratschke & Morlicchio, Citation2012) street women are unable to get employed as they lack legal identification documents, good education, and good housing (Karabanow, Citation2004).
Homeless women are characterized by unique reproductive health needs which include mistimed pregnancies, abortions and miscarriages, rape, survival sex, etc (Gelberg et al., Citation2001). Street women who sleep outside risk physical and sexual abuse (Wenzel et al., Citation2000). Homeless women also engage in sexually exploitative relationships where they have little power to negotiate contraceptive use leading to high incidences of untimed pregnancies (Conde Agudelo et al., Citation2006). Homeless women like other women need to utilize family planning services to space and time births as well as prevent pregnancies (Kennedy et al., Citation2014). However, homeless women encounter several barriers in access to reproductive health services (Gelberg et al., Citation2001). The majority of homeless women rarely visit healthcare centers due to fear of stigmatization by healthcare providers (Ayaya & Esamai, Citation2001). Homeless women cite a lack of respect and lack of trust in healthcare workers (Gelberg et al., Citation2004). The majority of women practicing survival sex are often ashamed of discussing their sexual behaviors with healthcare providers (Oliver & Cheff, Citation2012). Homeless women who abuse drugs often suffer low self-esteem and are unable to keep appointments (Pleace et al., Citation2000). Healthcare providers have also cited mistrust and lack of sufficient training as major setbacks in providing reproductive health services to homeless women (Dasari et al., Citation2016). Housing is important for a woman’s well-being. Research has shown that housing controls alcohol use and HIV infections as well as improve overall well-being and community functioning (Buchanan et al., Citation2009). Street women are unable to hold formal employment as they lack adequate and safe housing to operate from (Karabanow et al., Citation2010).
Housing challenge also affects a street woman’s ability to store drugs that need daily administration leading to incidences of stolen or misplaced drugs (Whitney & Glazier, Citation2004) Contraceptive utilization by homeless women is influenced by several socio-economic and demographic factors. Mass media, for example, is a mode of communication widely used in both developing and developed countries. Viewers are exposed to new information and new ways from different parts of the world. Media exposure has been found to significantly improve a woman’s autonomy and reduce overall fertility (Jensen, Citation2012).
A woman’s education also impacts contraceptive utilization. Education is believed to give a woman autonomy which acts as a link between education and contraception (Jejeebhoy & Sathar, Citation2001). More educated women are more likely to use contraception than the less educated, Studies carried out in Ghana by Achana et al. (Citation2015), collaborates this argument when he discovered that women with secondary or higher levels of education utilize contraception more than women with a primary level of education or lower. Withers et al. (Citation2010) further noted that women from a higher socio-economic background were more likely to utilize contraception than women from poor households. Studies from India have revealed that women who are employed are more likely to utilize contraception than women without employment (Islam et al., Citation2016). Marital status and number of children have been found to inform contraceptive utilization decisions among women. Studies have shown that single women are more likely to use contraception than married women as they desire to prevent pregnancy than married women (Agyemang et al., Citation2019). The quality of children is believed to impact on contraceptive behaviors of women. Economic development has led to greater investments in human capital, therefore shifting societies’ focus to quality rather than quantity (Heckman & Mosso, Citation2014). A drop in fertility in the late 20th century has been attributed to decreased mortality (Meltzer , Citation1992). Meltzer (Citation1992) noted that a reduction in mortality increases demand for surviving children. In developed nations, social security paid by the young is used to support the older generation. Since the retired are often covered by social security, the young generation may not desire to have more children for future security, therefore, reducing the need for parents to stay with their children (Barr & Diamond, Citation2006). When intergenerational transfers like public debt and social security payments are to be paid by the younger generation, the cost of having children for the younger generation becomes high. The high cost of children increases the demand for contraception (Lee, Citation2008).
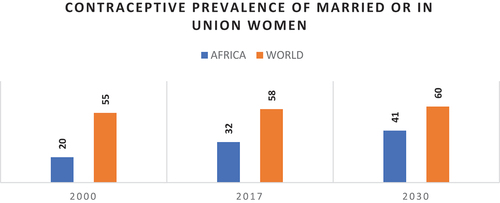
Globally fertility rates have declined from 3.2 children per woman to 2.5 children per woman. However, Africa continues to lag in fertility management which has led to low savings, low literacy levels, and low foreign direct investments (Cleland & Machiyama, Citation2017). To speed up Africa’s economic development contraceptive utilization should be adopted to reduce fertility (Moultrie et al., Citation2012). In most regions of the world, contraceptive use has widely been adopted by women of reproductive age to delay births or prevent unwanted pregnancies. In 2017, 78% of women globally had their contraceptive needs met a. However, only 56% of women in need of contraception in Africa had their needs met. In the case of married or in-union women, 63% used contraception globally, while only 36% used contraception in Africa as shown in Figure below. Married women or in-union women utilizing contraception contributed a proportion of 92% of the global contraceptive prevalence (United Nations, Department of Economic and Social Affairs, Population Division, Citation2017).
Figure 1. Contraceptive Prevalence for women between 15–49 Years (Married or in a union).
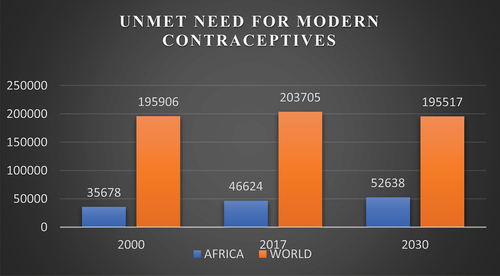
Women often have an unmet need for contraception when they desire to stop births for 2 years or more but are unable to access any form of contraception (Machiyama et al., Citation2017). With 1.9 billion women of reproductive age (15–49 years) globally, 842 million were utilizing modern contraceptives and as of 2019 while 190 million women had an unmet need for contraception as highlighted in Figure below (United Nations, Department of Economic and Social Affairs, Population Division, Citation2017).
Figure 2. Unmet need for contraception among women between 15–49 years.
Kenya has made tremendous progress in improving contraceptive access and use. In 2019 contraceptive prevalence in Kenya rose to 59.7% (United Nations, Department of Economic and Social Affairs, Population Division, Citation2019). Despite this progress, there still exist disparities in contraceptive use across counties in Kenya (Kenya National Bureau of Statistics, Citation2014). Women living in rural areas and women from poor backgrounds utilize contraception at lower proportions than the rest of the population (Ross & Goldner, Citation2009). Kenya when compared to the rest of Africa has performed exceedingly well with a gradual but consistent improvement in contraceptive utilization (Kenya National Bureau of Statistics (KNBS) and ICF Macro, Citation1998, Citation2003).
Improving access to contraceptives will not only assist the government meet one of its Big four agendas on Universal Health Coverage by 2022 but will also ensure every individual access needed healthcare services without incurring financial hardships (WHO, Citation2010).
This study, therefore, examined the factors affecting the utilization of modern contraceptives in Nairobi, Kenya. Several policy recommendations can be drawn from the findings of the study on population control of street children in Kenya by ensuring that homeless women can space and delay birth at will thus promote good health for both mothers and their children.
2. Literature review
2.1. Theoretical review
The demand for healthcare theory by Grossman (Citation1972a) was utilized to explain the demand for contraceptives. The Social Capital theory by Bourdieu (Citation1985) was used to explain the importance of social capital in knowledge exchange and information flow within social networks.
2.1.1. New home economics theory
The new home economics theory by Becker was adopted to give insights into how the utility preferences of parents determine fertility (Becker & Barro, Citation1988). According to this theory, a parent’s utility is determined by utility derived from consumption, i.e., having children. In his work, Becker noted that household heads seek to maximize utility subject to the benefits of an additional child in comparison to the cost of raising that child. Becker notes that the cost of raising a child is dependent on the change in interest rates, degree of altruism, time preference, and increase in the net cost between generations. The theory further notes that the economic roles of women and level of education affect their reproductive health behaviors where young adults will tend to reduce births to improve their living standards (Ferber & Birnbaum, Citation1977)
According to Gary Becker (Citation1960), when positive yields are derived from the net investments in children, the positive psychic income derived has the ability to offset the cost of having an extra child. Becker further noted that if there results a negative cost of children, since children are treated as a production good they will generate monetary returns for their parents in future. The formula developed by Becker to calculate the cost of raising a child is as follows:
Net cost of children =Present value of expected outlays + Inputed value of parent’s services -Present value of expected money return + inputed value of child services.
2.1.2. Social capital theory
The social capital theory was first defined by Bourdieu (Citation1985) as a combination of all potential and actual resources that are linked to lasting networks that provide mutual benefits to members and can access social resources available within the network. Access improves decision-making and affects behaviors. Chiu et al. (Citation2006) and Hazen et al. (Citation2016) argue that interactions within a social network led to a standard of acceptable social norms which have an impact on health behaviors, such as substance abuse, alcoholism, prostitution, etc. Social capital enhances access to healthcare through lobbying while providing psychosocial support networks important for the physical and mental well-being of members. There exist two elements of social networks
Social relations (Portes, Citation1998)
Quantity and quality of resources available within a network (Bourdieu, Citation1985)
Kankanhalli et al. (Citation2005) highlight the importance of social capital in the creation of a conducive environment for knowledge exchange and information flow. The latent constructs of social capital can be developed using the principal concept analysis to reduce the set of related variables to a smaller number of underlying components. For example, given a set of j response variables, x (i.e., our proxy variables, like participation in group activities) , we can estimate a set of k latent components
, where k, that contain similar information, so that
. This can be expressed as:
where is the correlation between variable and factor of the
latent factors
for each individual
, derived from
number of explanatory variables,
. The correlations are represented by:
The eigenvalue is useful in measuring the variance of all explanatory variables, which is accounted for by that factor (Pugno & Verme, Citation2011). A factor with the larger eigenvalue is said to have the most variance. To further explore the validity of the factors that emerge from the principal concept analysis (PCA), we consider the impact of some health and well-being measures. The equation can be estimated as follows:
where represents each of the k latent factors of social capital
are a set of
control variables and (ε) is the error term. In this literature, models of individual health status are derived from the Grossman (Citation1972b) model of demand for health capital.
2.2. Empirical literature
Contraceptive use among homeless women is an area of study that is yet to be fully studied. Alkema et al. (Citation2013) in their research on contraceptives found that contraceptive prevalence globally had increased from 54.8% in the early 1990s to about 63.3% by 2010. Alkema et al. (Citation2013) further noted that Central America, parts of Eastern Europe East, North, and Southern Africa had shown an increase in the utilization of contraception. Moreover, the sum of women with unmet needs for family planning had reduced from a high of 15.4% in the early 1990s to 12.3% by 2010. In the United States, United Kingdom, and Canada, it was discovered that 70% of contraceptive preference achieved was consistent with a balanced distribution of modern contraceptives (Biddlecom and Kantorova, Citation2013). United Nations Department for Economic and
Social Affairs (2019) noted that sub-Saharan Africa had the least contraceptive prevalence at 31% as of 2017.
Arab Countries followed with a contraceptive prevalence of 47%. More developed regions like North America recorded the highest contraceptive prevalence at 76% while Kenya had a contraceptive prevalence of 61% as of 2017.
The United Nations population division (Citation2009) report revealed that the contraceptive prevalence among women living in the sub-Saharan region of Africa ranges from a high of 60.3% (South Africa) to 1.2% in South Sudan. Countries in the Southern parts of Africa recorded high usage of modern family planning than countries in East Africa. The West African and Central African countries reported very low rates of family planning use. Contraceptive use in Africa can be traced to the 1980s when fertility rates began to drop. In the 1970s South Africa recorded a high contraceptive prevalence relative to the rest of Africa (Lucas, Citation1992)
In Kenya, the contraceptive prevalence was estimated to be around 46% with a fertility rate of 4.6 in 2009. Kenya National Bureau of Statistics (Citation2014) estimated the contraceptive preference among women in Kenya to be around 58% and unmet need was at 17.5%. Between the late 1989s and late 1990s, the proportion of married women using contraceptives increased by over two times. Results from Kenya Demographic and Health Survey suggest that by the year 2014 over 60% of unmarried women were using contraceptives.
Several studies on homeless women, their challenges, and reproductive health have widely been carried out. The street is deemed a place of survival without parental guidance and supervision. Street families rely on the streets for the provision of social, physical, and psychological support (Sorber et al., Citation2014). However, the streets are not friendly and initiate street families into a hostile environment of sexual abuse, drug, and substance abuse as well as physical injuries. This makes this group of people very vulnerable (Kudrati et al., Citation2008). The hostile street environment also tends to favor boys than girls. This is because boys are deemed more aggressive and dominate than their female counterparts. Sorber et al. (Citation2014) in their research on street families in Kenya noted that 73% of homeless women were members of a gang, whereas 98% of men in the streets were members of a gang. Male street children, therefore, engage in crimes to get a livelihood whereas the females turn to prostitution putting themselves at a high risk of unplanned pregnancies. It’s estimated that female sex workers in Ethiopia had a 28.6% incidence of unplanned pregnancies, whereas 69% of females in Cote d’Ivoire had unplanned pregnancies (Sorber et al., Citation2014).
A study carried out in the city of Los Angeles reveal that 28% of homeless women were pregnant and 78% of these pregnant women had unplanned pregnancies (Gelberg et al., Citation2001) Factors contributing to unplanned pregnancies among homeless women practicing prostitution include drug abuse and being unmarried (Kudrati et al., Citation2008). In Kenya research by Rescue dada, a non-Governmental organization found that 20% of women in the streets engage in commercial sex, whereas the remaining 80% are often raped and abused by other street boys leading to incidences of unwanted pregnancies and HIV and Aids. Apart from the risk of STD’s homeless women are often exposed to other dangerous viral infections like Hepatitis A. Research carried out in Iran and Brazil among the youth in the street population revealed that between 80% and 92.2% had hepatitis A virus (Queiróz et al., Citation1995). In Ethiopia 40% of homeless women live alone while over 35% women abused drugs. 79% of street girls knew about contraceptives and had had coition in the past 12 months while 83% of homeless girls had more than two sexual partners with a mean number of sexual partners being 2.85 (Ababor et al., Citation2019). A study by Embleton et al. (Citation2018) on causes factors that influence survival and death found that incidences of death were high among those street people above 18 years than those below 18 years. Embleton found that of the deaths recorded in 2018, 37% occurred in the population below 18 years. Of the total deaths, 37% was caused by HIV/Aids, 36% by assault, and 10% was caused by accidents. The education level among homeless women is also very low.
2.3. Data sources
Data collected for the study was primary data from Nairobi CBD alleys and off slum settlements of Kibra, Korogocho, Mathare, Mukuru kwa Reuben, Majengo, Kawangware, and Huruma. The sample size used during the study was determined using Gill et al. (Citation2010) formula of sample size selection based on the desired accuracy with a confidence level of 95%. According to Bartlett et al. (Citation2001), the percentage of occurrence in the primary survey is expected to yield maximum variance and the maximum sample size is estimated to be 50%. The population of homeless women in Nairobi was estimated to be greater than 10,000 and the level of confidence needed was 95% which corresponds to a Z value of 1.96. Using the Gills formula, we estimated the sample size as follows:
Where:
n= size of the sample needed for the study
z = standard normal deviate with an expected confidence level of 1.96.
p = Percentage occurrence of a state/heterogeneity of the population.
ε = percentage maximum error required which is at 5%
= 384.16. Rounding off to the nearest figure = 384
Using this estimate the number of homeless women interviewed was 384 plus an
additional 38 persons from the pilot study. The data collection exercise is expected to be carried out between
the 21st of November 2019 and the 5th of December 2019.
3. Methodology
Grossman (Citation1972b) classifies health as a durable capital stock and a consumer good. Heath, as a consumer good, derives direct utility when one is healthy. Health can be a capital good that can be increased through investment in health. Investment can be done through exercise, eating healthy, and regular medical checkups. Health as a capital stock can also be depreciated with time as one ages and healthy days meant to develop economic resources are decreased. Health can be utilized by an individual as an investment good or consumption good.
3.1. Theoretical framework
A household will seek to maximize its utility subject to a budget constraint and the health production function (Grossman, Citation1972b). The household utility maximization function is given as
where;
: Is the utility of the household
: Family Health
: The consumption of other market goods.
The budget constraint is stated as:
where:
M: The income of the household
: Cost of using family planning
: Cost of inputs like knowledge of contraceptives
: Cost of other consumption goods consumed by the household
Moreover, the health production function is given as follows:
where:
H: Health
: Methods of family planning
: Other inputs in the market
: Other household consumption
Using the equations 1 and 2, we form the following Langrage function:
Solving Equationequation 4(4)
(4) we shall have the following reduced demand function for the use of family planning:
where:
V: other variables
: Cost of using family planning
: Cost of inputs like knowledge of contraceptives
: Cost of other consumption goods consumed by the household
Y: household income
The household utility function described in EquationEquation 5(5)
(5) above applies to homeless women. Homeless women like other individuals seek to maximize their utility. To achieve this homeless woman, engage in income generating activities like begging, others, i.e.,, prostitution and small businesses. Street women work with a budget that is subject to the price of contraception, price of knowledge, and the price of other commodities. EquationEquation 6
(6)
(6) points to the fact that keeping the income constant, an increase in the price of contraception will reduce consumption of contraception or reduced consumption of other goods consumed by a household.
EquationEquation 7(7)
(7) outlines the relevance of family planning on family health and wellbeing. From this equation, underutilization of family planning leads to poor health.
EquationEquation 8(8)
(8) shows that increasing the price of family planning will reduce or increase quantity demand. Moreover, increasing the prices of other household consumables reduces or increases the demand for family planning services.
3.2. Empirical model
3.2.1. Logistic regression model
The logistic model was used since the dependent variable in the study is a binary. The logistic model was therefore used to combine the covariate values and convert them into a probability scale of between 0 and 1.
The logit analysis is an extension of the linear probability regression model that expresses the dependent variable Y as a non-linear function of the explanatory variable X.
The general linear regression model is often expressed as follows:
where;
is the intercept
‘s is the slope between Y and the
that is needed
is the error term
The linear Equationequation 6(6)
(6) above can be interpreted as the probability that a homeless woman uses contraceptives or not, given the independent variables in the model. The logit model was used to analyze the first objective that estimated factors affecting contraceptive usage among homeless women in Nairobi. The dependent variable takes the form of value 1 if contraceptives are used and 0 if contraceptives are not used. The model is simplified such that:
where X represents all the explanatory variables in the study (respondent’s age, education, age at first birth, drug abuse by the respondent and partner, miscarriage/stillbirth/abortion incidences, living with a partner, child planning, neonatal death incidences, knowledge on female sterilization, knowledge on male sterilization, income source contraceptive spending and visit by a healthcare worker in the past 12 months).
In our example, Pi is the probability of using or not using contraceptives, and x represents the explanatory variables. Therefore, the parameter β0 gave the log odds of a Street woman having not used contraceptive (when) and
shows how these odds differ (when
) when a street woman was using contraceptives. The study, therefore, describes the model in terms of odds as follows:
(
+
) and in terms of the probability of the outcome (e.g., use or not using Contraceptives) occurring as:
4. Results & discussions
4.1. Descriptive statistics
Age was found to be an important explanatory variable in the study and the descriptive statistics indicated the average age of women in the streets to be 27 years. The study also found the average age of childbearing in the streets to be 19 years as shown in Table below. The average number of children per woman in the streets was found to be three children which was slightly lower than the national fertility rate of 3.9 (Kenya National Bureau of Statistics, Citation2014).
Table 1. Descriptive Statistics
4.2. Demographic analysis of the respondents
A demographic analysis on homeless women in Nairobi county found the average age of a homeless woman in Nairobi county to be 28 years. The study further found that homeless women had an average of two children. Moreover, the average age at first birth for homeless women in Nairobi was found to be 19 years. A qualitative analysis on homeless women has revealed that the majority of homeless women in Nairobi county had walked out of their matrimonial home as a result of domestic violence and others had joined their partners in the search for employment in the city and were either unemployed, beggars, small business owners, casual workers, or generated income from other means not mentioned above. The study found over 10% of homeless women to be beggars and majority small business owners.
The study further found that over 34% of homeless women were born and raised in Nairobi County. The remaining 66%, had emigrated from various counties in Kenya which includes Homabay, Kiambu, Kisumu, Kwale, Machakos, Meru, Moyale, Nyandarua, Siaya, Uasin Gishu, and Wajir. Kakamega recorded the highest level of immigration at 9.84%. The study further noted that 54.87% of homeless women had emigrated from the rural areas while 45.13% had either been born in Nairobi or emigrated from an urban area.
Education attainment among homeless women in Nairobi, Kenya was also analyzed. The study found that majority of homeless women were well educated and a some had tertiary level of education. Majority of these women had attained primary-level education while less than 10% had never attended school. An increase in primary school attainment by homeless women can be attributed to the free primary education introduced in Kenya in 2003 by the National Rainbow Coalition Party (Republic of Kenya ROK, Citation2003). A higher enrollment in secondary schools is as a result of subsidized secondary school tuition fees (for Day schools) and the introduction of adult education centers. Kenya has continued to position adult education as part of its long-term strategy to bring balanced development across regions of the country (UNESCO, Citation2007).
5. Discussion
Findings from this study reveals an interesting phenomenon where homeless women behave just like other sheltered women in decision-making and sometimes act differently due to challenging socio-economic and psychological challenges. It is to be noted that homeless women face life challenges quite differently than sheltered women. Homeless women often deal with emotion stress, low self-esteem, violence, drug abuse and rape (Volpi, Citation2002). Most DHS data estimate the childbearing age of a woman to be between 15 and 49 years. However, the dynamics facing women in the streets is different as their childbearing age can be as low as 13 years. Majority of street children are emancipated minors who lack parental supervision and are often exposed to the risk of prostitution and sexual abuse earlier in their development (Woan et al., Citation2013).
As illustrated in table , findings from this study revealed that, the more a street woman delays her first birth the more she uses contraception. These results collaborate findings by Sedekia et al. (Citation2017). In their research on contraceptive use among women in southern Tanzania, these researchers found the odd ratio of using contraceptives to be higher among women with higher age at first birth that those who got pregnant earlier.
Table 2. Estimates of contraceptive use among homeless women in Kenya
Findings from the research has revealed that giving birth in a health facility increases a street woman’s predicted probability of contraceptive use by over 20%. These results collaborate findings from research by Lasong et al. (Citation2020) who found that women who give birth in a health facility were 1.73 times more likely to use contraception than women who gave birth away from a health facility. These findings point to the importance of healthcare facilities as center of reproductive health utilization.
The study further revealed that an additional incidence of miscarriages, abortions, and still births increased the predicted probability of contraceptive use by over 7%. These findings are in line with Singh et al. (Citation2017) who noted that, the use of modern contraceptives in sub-Saharan Africa averted 12.6 million unintended pregnancies with 64% of the unplanned pregnancies averted likely to occur in the southern part of Africa.
The study further found that increasing contraceptive spending by KES 1 increases the predicted probability of contraceptive use by over 2000%. These findings are in line with findings by a number of researchers. Weinberger et al. (Citation2021) noted that the private out of pocket expenditure on family planning in 2019 increased to $2.73 billion in 113 middle- and low-income economies. Of these budgets 29% was mainly used to purchase pills. Brant et al. (Citation2022) further noted that from 2013 to 2016, 38% of women who spent on contraceptives from out of pocket used on average $216. The study further reveals that 98% of women who spent from out of pocket consistently utilized contraceptives.
The research also found that being assisted by a midwife during delivery increases the predicted probability of contraceptive use by over 7%. These results collaborate findings from qualitative research collected during the study A few women gave their view on mistreatment by midwives from public hospitals who look down upon them. The midwives we meet at the Kibera hospital look down upon us. They say we are dirty and we smell like dogs. They however give us lessons on family planning and sometimes carry some pills as they come (Midred, 31, Kibera off slum settlement)
The research also found women who had knowledge on contraceptive methods like lactational amenorrhoea to more likely to utilize contraception. These findings collaborate the work of Alemu et al. (Citation2020) who found the odds of contraceptive use among women with knowledge on contraceptive methods like lactational amenorrhea to be 3.9.
The research also found that attending school improved the predicted probability of contraceptive use by over 30%. This collaborates findings by Bbaale and Mpuga (Citation2011) who noted that 16.1% and 24.7% of women with primary and secondary education utilized modern contraceptives, while only 9.7% of women who had never attended school utilized modern contraceptives. Other studies from rural Zambia found that women with secondary school level of education were 7.61 times more likely to use contraception while women with higher level of education where 2.39 times more likely to use contraception than women with secondary school level of education (Lasong et al., Citation2020)
The study further found that an additional year unemployed or practicing begging reduces contraceptive use. These findings collaborate finding by studies carried out in Ghana in 2008 by Justice and Novignon (Citation2014) who found that women in the richest quantiles of Ghana’s economy were 2.6 times more likely to utilize contraception while women in the poorest quantiles were 1.14 times more likely to utilize contraception. These findings reveal that poor women will less likely utilize contraception than richer women.
The study also found that an additional year living with a partner increased the predicted probability of contraceptive use by over 25%. These findings collaborate studies that point to the use of contraceptives for purposes of spacing and delaying births (Zewude et al., Citation2019). Studies that collaborate these findings include studies by Akoth et al. (Citation2021) who noted that one-fifth of married women in developing countries were using contraceptives due to increased sexual frequency necessitated by living with a partner. They further noted that 0–4% of married women in 52 developing countries lacked knowledge on contraceptives while 20–33% continue contraceptive use despite suffering adverse effects.
The study also found that spending a year as a beggar or as an unemployed person reduced the predicted probability of contraceptive use. The county government in collaboration with the National government can set up a fund to finance business start-ups for homeless women. Business professions can also be recruited to give advice and help street women nurture their businesses into maturity. The National government through the affirmative fund can assist businesses owned by street funding through increased funding to the affirmative fund. The affirmative fund currently caters for the needs of youths, women and people living with disabilities. Homeless women should be included as a special group and be given more allocation in the funds (Lavagna et al., Citation2019).
Further probing during the interview pointed out the important role the government has played to provide free contraception to all the needy women in society. Some women in the off-slum settlements of Kibera, Mathare, and Mukuru as well as the CBD Alleys pointed to free contraception being offered in public hospitals. Free contraception was offered at Kibera south hospital but sometimes residents were charged a small fee of $1 (Joan, 27, Kibera). More probing on why homeless women choose to use contraceptives pointed out the need to space children or stop childbearing at all costs. Other women desired to offer their children a quality life since life was already hard on them. With homelessness women lacked jobs and sources of income to purchase contraceptives or visit health facilities.
6. Conclusions
The study found homeless women to be rational in decision-making. However, some behavioral and environmental factors affect the way they make some decisions, especially on issues of family health. The research found that even though homeless women utilize contraception when they visit a health clinic during delivery, lessons on family planning done in health centers to benefit only those who can be physically present. More community health volunteers should be recruited and assigned to villages, slums, and the streets to give lessons to women who can’t access health facilities during birth. Mobile clinics should also be increased in slum areas and street alleys to reach every homeless woman in need of reproductive health services. The study through qualitative research found that homeless women were reluctant to go back to healthcare facilities after unfair treatment by healthcare workers. The government should ensure that healthcare workers are trained on care for the vulnerable. Furthermore, homeless women were found to be unable to meet their contraceptive needs using out of pocket expenditure. The government is therefore tasked with the responsibility of providing a wide range of free or subsidized contraceptives to all.
The study noted attending school highly increases the odds of contraceptive use. This finding is important since education is expected to impart knowledge on modern contraceptives. Lessons on family planning should therefore be introduced early on in primary and secondary school curricula to reach out to all men and women in that level of education. Bursary funds can also be set up by the county government of Nairobi to aid in education for children residing in the streets. Streets campaigns on family planning should also be introduced to reach out to all homeless women. In agreement with Kenya’s government vision 2030 that seeks to provide universal health coverage to all by 2030, homeless women should also have access to reproductive healthcare. Community health workers and outreach programs should expand their jurisdiction to homeless women all over the country such that all women regardless of their socio-economic backgrounds have access to affordable contraception. The government should also offer financial safety nets for the homeless women who are not able to work due to physical disability and offer free rehabilitation to those struggling with substance abuse. Homeless women should also be considered for employment especially casual labor, while those operating small business should be exempted from municipal rates and provided subsidized business premises to boost their businesses.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors

Lydia Cheruto Pkaremba
Lydia Pkaremba is a PhD. Student at the University of Nairobi’s school of Economics doing a doctorate course in Economics. She is a graduate of the University of Nairobi having completed a Masters in Economics and policy management course. She also holds a bachelors in Economics and Finance degree from Kenyatta University, Kenya. Ms. Pkaremba, is a beneficiary of the African Economic Research Consortium scholarship (AERC) that aims to incubate scholars and researchers to accomplished economists in sub-Saharan Africa. Ms. Pkaremba is an entrepreneur in charge of Linkstakes consultancy limited, a consultancy firm that deals with capacity building and performance assessment. She has extensive experience in lecturing, consultancy and management. Her recent activities include working with public officials and county government of Kenya’s legislative assemblies and executive governments to improve capacity of counties in service delivery.
Ms. Pkaremba currently lectures at the University of Nairobi and Zetech University. Her areas of specialization include: Health economics, international economics, development economics, statistics and econometrics.
Ms. Pkaremba is a frequent speaker at municipal finance functions and is a member of the Institute of Economic affairs as well as the chair of the Linkstakes Fund Board. She lives in Nairobi, Kenya, and campaigns to eradicate female genital mutilation in Kenya in collaboration with the US Network against FGM.
Education & Credentials
PhD., University of Nairobi, 2017 to Date
M.A, (Economics), University of Nairobi, 2016
B.A., Kenyatta University.
References
- Ababor, A. A., Tesso, D. W., & Cheme, M. C. (2019). Addressing the deprived: Need and access of sexual reproductive health services to street adolescents in Ethiopia. The case of Nekemte town: Mixed methods study. BMC Research Notes, 12(1), 827. https://doi.org/10.1186/s13104-019-4850-7
- Achana, F. S., Bawah, A. A., Jackson, E. F., Welaga, P., Awine, T., Asuo-Mante, E., Oduro, A., Awoonor-Williams, J. K., & Phillips, J. F. (2015). Spatial and socio-demographic determinants of contraceptive use in the Upper East region of Ghana. Reproductive Health, 12(1). https://doi.org/10.1186/s12978-015-0017-8
- Agyemang, J., Newton, S., Nkrumah, I., Tsoka-Gwegweni, J. M., & Cumber, S. N. (2019). Contraceptive use and associated factors among sexually active female adolescents in Atwima Kwanwoma District, Ashanti region-Ghana. The Pan African Medical Journal, 32, 182. https://doi.org/10.11604/pamj.2019.32.182.15344
- Akoth, C., Oguta, J. O., & Gatimu, S. M. (2021). Prevalence and factors associated with covert contraceptive use in Kenya: A cross-sectional study. BMC Public Health, 21(1), 1316. https://doi.org/10.1186/s12889-021-11375-7
- Alemu, L., Ambelie, Y. A., & Azage, M. (2020). Contraceptive use and associated factors among women seeking induced abortion in Debre Marko’s town, Northwest Ethiopia: A cross-sectional study. Reproductive Health, 17(1), 97. https://doi.org/10.1186/s12978-020-00945-4
- Alkema, L., Kantorova, V., Menozzi, C., & Biddlecom, A. (2013). National, regional and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: A systematic and comprehensive analysis. Lancet (London, England), 381(9878), 1–19. https://doi.org/10.1016/S0140-6736(12)62204-1
- Ayaya, S. O., & Esamai, F. O. (2001). Health problems of street children in Eldoret, Kenya. East African Medical Journal, 78(12), 624–629. https://doi.org/10.4314/eamj.v78i12.8930
- Bailey, M. J. (2006). More power to the pill: The impact of contraceptive freedom on women’s life cycle labor supply. Quarterly Journal of Economics, 121(1), 289–320. https://doi.org/10.1162/qjec.2006.121.1.289
- Barden O’Fallon, J., Speizer, I. S., & Calhoun, L. M. (2018). Women’s contraceptive discontinuation and switching behavior in urban Senegal,2010–2015. BMC Women’s Health, 18, 35. https://doi.org/10.1186/s12905-018-0529-9
- Barr, N., & Diamond, P. (2006). The Economics of Pensions. Oxford Review of Economic Policy, 22(1), 15–39. https://doi.org/10.1093/oxrep/grj002
- Bartlett, J. E., Kotrlik, J. W., & Higgins, C. C. (2001). Organizational research: Determining appropriate sample size in survey research. Learning and Performance Journal, 19(1), 43–50. http://api.semanticscholar.org/corpusID:142302922
- Bbaale, E., & Mpuga, P. (2011). Female Education, Contraceptive Use, and Fertility: Evidence from Uganda. Consilience, 6, 1–23. https://doi.org/10.7916/consilience.v0i6.4570
- Becker, G. (1960). An Economic Analysis of Fertility (Vol. 1, pp. 209–240). Columbia University and National Bureau of Economic research. 0870143036. http://www.nber.org/chapters/c2387
- Becker, G. S., & Barro, R. J. (1988). A reformulation of the economic theory of fertility. Quarterly Journal of Economics, 103(1), l–25. https://doi.org/10.2307/1882640
- Biddlecom and Kantorova. (2013). Global trends in contraceptive method mix and implications for meeting the demand for family planning. United Nations.
- Bourdieu, P. (1985). The forms of capital. Handbook of theory and research for the sociology Bronx. Journal of the National Medical Association, 91(4), 195–200. PubMed: 10333668.
- Brant, A. R., Batur, P., Arrigain, S., Lopez, R., & Farrell, R. M. Out-of-pocket expenditures for contraceptives during state medicaid expansion, 2013-2016. (2022). Obstetrics & Gynecology, 139(4), 622–625. April 2022. https://doi.org/10.1097/AOG.0000000000004721
- Buchanan, D., Kee, R., Sadowski, L. S., & Garcia, D. (2009). The health impact of supportive housing for HIV-positive homeless patients: A randomized controlled trial. American Journal of Public Health, 99(S3), sup. 3), S675–S680. https://doi.org/10.2105/AJPH.2008.137810
- Canning, D., & Paul Schultz, T. (2012). The economic consequences of reproductive health and family planning. The Lancet, 380(9837), 165–171. https://doi.org/10.1016/S0140-6736(12)60827-7
- Chiu, C. M., Hsu, M. H., & Wang, E. T. Understanding knowledge sharing in virtual communities: An integration of social capital and social cognitive theories. (2006). Decision Support Systems, 42(3), 1872-1888, ISSN 0167–9236. 2006. https://doi.org/10.1016/j.dss.2006.04.001
- Cleland, J., & Machiyama, K. (2017). The challenges posed by demographic change in sub Saharan Africa: A concise overview. Population and Development Review, 43, 264–286. https://doi.org/10.1111/padr.170
- Collumbien, M., Gerressu, M., & Cleland, J. (2004). Non-use and use of ineffective methods of contraception. Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors Geneva: World Health Organisation, 1, 1255–1320. 9241580313. http://researchonline.Ishtm.ac.uk/id/eprint/17866
- Conde Agudelo, A., Rosas-Bermudez, A., & Kafury-Goeta, A. C. (2006). Birth spacing and risk of adverse perinatal outcomes: A meta-analysis. Journal of the American Medical Association, 295(15), 1809–1823. https://doi.org/10.1001/jama.295.15.1809
- Consortium for street children. (2011). Street children: A mapping & gapping review of the literature 2000 to 2010 London. Street Children Literature Review, 2, 3–75. http://childhub.org/sites/default/files/library/attachments/1307
- Dachner, N., & Tarasuk, V. (2002). Homeless “squeegee kids”: Food insecurity and daily survival. Social Science & Medicine, 54(7), 1039–1049. https://doi.org/10.1016/S0277-9536(01)00079-X
- Dasari, M., Borrero, S., Akers, A. Y., Sucato, G. S., Dick, R., & Hicks, A. (2016). Barriers to long-acting reversible contraceptive (LARC) uptake among homeless women young women. J Pediatr Adolesc Gynecol. 29:104–110.
- Davanzo, J., Abdur, R., Mizanaur, R., Lauren, H., Kapil, A., Mehrab, A., Golam, M., & Kaniz, G. (2004). The effects of birth spacing on infant and child mortality, pregnancy outcomes and maternal morbidity and mortality in Matlab, Bangladesh, and Labor and Population. Working Paper
- Embleton, L., Ayuku, D., Makori, D., Kamanda, A., & Braitstein, P. (2018). Causes of death among street-connected children and youth in Eldoret, Kenya. BMC International Health and Human Rights, 18(1), 19. https://doi.org/10.1186/s12914-018-0160-8
- Embleton, L., Shah, P., Gayapersad, A., Kiptui, R., Ayuku, D., & Braitstein, P. (2020). Characterizing street-connected children and youths’ social and health inequities in Kenya: A qualitative study. International Journal for Equity in Health, 19(1). https://doi.org/10.1186/s12939-020-01255-8
- Ferber, M. A., & Birnbaum, B. G. (1977). The “new home economics”: Retrospects and prospects. Journal of Consumer Research, 4(1), 19. https://doi.org/10.1086/208675
- Gelberg, L., Browner, C. H., Lejano, E., & Arangua, L. (2004). Access to women’s health care: A qualitative study of barriers perceived by homeless women. Women & Health, 40(2), 87–100. https://doi.org/10.1300/J013v40n02_06
- Gelberg, L., Leake, B. D., Lu, M. C., Andersen, R. M., Wenzel, S. L., Morgenstern, H., Koegel, P., & Browner, C. H. (2001). Use of contraceptive methods among homeless women for protection against unwanted pregnancies and sexually transmitted diseases: Prior use and willingness to use in the future. Contraception, 63(5), 277–281. https://doi.org/10.1016/S0010-7824(01)00198-6
- Gill, J., Johnson, P., & Clark, M. (2010). Research Methods for Managers. SAGE Publications. SBN, 1847870945, 9781847870940; Length.
- Glomm, G., & John, A. (2002). Homeless women and Labor Markets. Regional Science and Urban Economics, 32(5), 591–606. https://doi.org/10.1016/S0166-0462(01)00097-7
- Goldin, C., & Katz, L. F. (2000). Career and Marriage in the Age of the Pill. American Economic Review, 90(2), 461–465. https://doi.org/10.1257/aer.90.2.461
- Gould, T., & Williams, A. R. (2010). Family Homelessness: An Investigation of Structural Effects. Journal of Human Behaviors in the Social Environment, 20(2), 170–192. https://doi.org/10.1080/10911350903269765
- Grossman, M. (1972a). The demand for health: A theoretical and empirical investigation. NBER New York, 45(1), 23–34.
- Grossman, M. (1972b). On the concept of health capital and the demand for health. Journal of Political Economy from. 80(2), 223–255. Retrieved July 4, 2020 www.jstor.org/stable/1830580 https://doi.org/10.1086/259880
- Grotluschen, A., Mallows, D., Reder, S., & Sabatini, J. (2016). Adults with low proficiency in Literacy or Numeracy. OECD. SSN: 19939019. https://doi.org/10.1787/19939019
- Hazen, B. T., Skipper, J. B., Ezell, J. D., & Boone, C. A. (2016). Big data and predictive analytics for supply chain sustainability. Computers & Industrial Engineering, 101, 592–598. C (November 2016). https://doi.org/10.1016/j.cie.2016.06.030
- Heckman, J. J., & Mosso, S. (2014). The economics of human development and social mobility. Annual Review of Economics, 6, 689–733. https://doi.org/10.1146/annurev-economics-080213-040753
- Hossain, S. A., & Alam, M. A. (2016). Socio-economic status of the street children. International Journal of Social Work, 3(1), 42–49. https://doi.org/10.5296/ijsw.v3i1.8668
- Islam, A. Z., Mondal, M. N., Khatun, M. L., Rahman, M. M., Islam, M. R., Mostofa, M. G., & Hoque, M. N. (2016). Prevalence and determinants of contraceptive use among employed and unemployed women in Bangladesh. International Journal of MCH and AIDS, 5(2), 92–102. https://doi.org/10.21106/ijma.83
- Jejeebhoy, S. J., & Sathar, Z. A. Women’s autonomy in india and Pakistan: The influence of religion and region. (2001). Population & Development Review, 27(4), 687–712. 00687.x. https://doi.org/10.1111/j.1728-4457.2001
- Jensen, R. (2012). Do labor market opportunities affect young women’s work and family decisions? Experimental evidence from India. The Quarterly Journal of Economics, 127(2), 753–792. https://doi.org/10.1093/qje/qjs002
- Justice, N., & Novignon, J. (2014). Trend and determinants of contraceptive use among women of reproductive age in Ghana. African Population Studies, 28, 956. Supplement July 2014. https://doi.org/10.11564/28-0-549
- Kankanhalli, A., Tan, B., & Wei, K. K. (2005). Contributing knowledge to electronic knowledge repositories: An empirical investigation. MIS Quarterly, 29(1), 113–143. https://doi.org/10.2307/25148670
- Karabanow, J. (2004). Making organizations work: Exploring characteristics of anti-oppressive organizational structures in street youth shelters. Journal of Social Work, 4(1), 47–60. https://doi.org/10.1177/1468017304042420
- Karabanow, J. (2008). Getting off the street: Exploring the processes of young people’s street exits. American Behavioral Scientist, 51(6), 772–788. https://doi.org/10.1177/0002764207311987
- Karabanow, J., Hughes, J., Ticknor, J., Kidd, S., & Patterson, D. (2010). The economics of being young and poor: How homeless youth survive in neo-liberal times. Journal of Sociology & Social Welfare, 37(4), Article 4. https://doi.org/10.15453/0191-5096.3560
- Kennedy, S., Grewal, M., Roberts, E. M., Steinauer, J., & Dehlendorf, C. (2014). A qualitative study of pregnancy intention and the use of contraception among homeless women with children. Journal of Health Care for the Poor and Underserved, 25(2), 757–770. https://doi.org/10.1353/hpu.2014.0079
- Kenya National Bureau of Statistics. (2014). Kenya Demographic and Health Survey 2014. KNBS, 1, 6–8. 3317623. http://dhsprogram.com/pubs/pdf/fr308
- Kenya National Bureau of Statistics (KNBS) and ICF Macro. (1998). Kenya demographic and health survey 1998 (Vol. 2). KNBS and ICF Macro.
- Kenya National Bureau of Statistics (KNBS) and ICF Macro. (2003). Kenya demographic and health survey 2003 (Vol. 1). KNBS and ICF Macro.
- Kudrati, M., Plummer, M. L., & NDEH, Y. (2008). Children of the sug: A study of the daily lives of street children in Khartoum, Sudan, with intervention recommendations. Child Abuse & Neglect, 32(4), 439–448. https://doi.org/10.1016/j.chiabu.2007.07.009
- Lasong, J., Zhang, Y., Gebremedhin, S. A., Opoku, S., Abaidoo, C. S., Mkandawire, T., Zhao, K., & Zhang, H. (2020). Determinants of modern contraceptive use among married women of reproductive age: A cross-sectional study in rural Zambia. Zambia BMJ Open, 10(3), e030980. https://doi.org/10.1136/bmjopen-2019-030980
- Lavagna, G., Salcedo, J., Alessandro, E., Lionetti, F., Valenzuela, L., Mugo, A., & Prigov, A. (2019). Expert group meeting on affordable housing and social protection systems for all to address homelessness. United Nations Human Settlements Programme (UN-Habitat), 8–144. https://unhabitat.org/sites/default/files/2020/10/final_for_publication_homelesness_egm_proceedings_report_1.pdf
- Lee, J. (2008). Sibling size and investment in children’s education: An Asian instrument. Journal of Population Economics, 21(4), 855–875. https://doi.org/10.1007/s00148-006-0124-5
- Lucas, D. (1992). Fertility and family planning in Southern and Central Africa. Studies in Family Planning, 23(3), 145–158. https://doi.org/10.2307/1966724
- Machiyama, K., Casterline, J. B., Mumah, J. N., Huda, F. A., Obare, F., Odwe, G., Kabiru, C. W., Yeasmin, S., & Cleland, J. (2017). Reasons for unmet need for family planning, with attention to the measurement of fertility preferences: Protocol for a multi-site cohort study. Reproductive Health, 14(1), 2017. https://doi.org/10.1186/s12978-016-0268-z
- Meltzer, D. (1992). Mortality decline, the demographic transition and economic growth, University of Chicago, School of Economics, 1, 146. 32053. http://books.google.co.ke/books?id=Ix9tHAAACAAJ
- Milaney, K., Williams, N., Lockerbie, S. L., Dutton, D. J., & Hyshka, E. Recognizing and responding to women experiencing homelessness with gendered and trauma-informed care. (2020). BMC Public Health, 20(1), 397. 2020. https://doi.org/10.1186/s12889-020-8353-1
- Moultrie, T. A., Sayi, T. S., & Timaeus, I. M. (2012). Birth intervals, postponement, and fertility decline in africa: A new type of transition? population studies. A Journal of Demography, 66(3), 241–258. https://doi.org/10.1080/00324728.2012.701660
- National Authority for the Campaign Against Alcohol and Drug Abuse (NACADA). (2017). Rapid situation assessment of drug and substance abuse in Kenya. AJADA Journal, 1–36. 133. http://nacada.go.ke/node/133
- OECD. (2013). OECD Skills Outlook 2013: First Results from the Survey of Adult Skills. of education. Greenwood.
- Olinto, P., Beegle, K., Sobrado, C., & Uematsu, H. (2013). The State of the Poor: Where are the poor, Where is extreme poverty harder to end, and what is the current profile of the world’s poor? Economic Premise Note, 135(289469850), 3–16. http://www.researchgate.net/publication/289469850
- Oliver, V., & Cheff, R. (2012). Sexual health: The role of sexual health services among homeless women young women living in Toronto, Canada. Health Promotion Practice, 13(3), 370–377. https://doi.org/10.1177/1524839912437369
- Pailhé, A., Solaz, A., & Tanturri, M. L. (2019). The time cost of raising children in different fertility contexts: Evidence from France and Italy. European Journal of Population, 35(2), 223–261. https://doi.org/10.1007/s10680-018-9470-8
- Pleace, N., Jones, A., & England, J. (2000). Access to general practice for people sleeping rough. Department of Health/University of York.
- Portes, A. (1998). Social capital: Its origins and applications in modern sociology. Annual Review of Sociology, 24(1), 1–24. https://doi.org/10.1146/annurev.soc.24.1.1
- Pratschke, J., & Morlicchio, E. (2012). Social polarization, the labour market and economic restructuring in Europe: An urban perspective. Urban Studies, 49(9), 1891–1907. https://doi.org/10.1177/0042098012444885
- Pugno, M., & Verme, P. (2011). Life satisfaction, social capital and the bonding-bridging nexus. World Bank policy research working paper 5945
- Queiróz, D. A., Cardoso, D. D., Martelli, C. M., Martins, R. M., Porto, S. O., Azevedo, M. S., Borges, A. M., & Daher, R. R. (1995). Soroepidemiologia da infecção pelo vírus da hepatite A em “meninos de/na rua de” Goiânia-Goiás. Rev Soc Bras Med Trop, 28(3), 199–203. https://doi.org/10.1590/S0037-86821995000300006
- Republic of Kenya (ROK). (2003). Report of the task force on implementation of free primary education. Jomo Kenyatta Foundation. http://www.google.co.ke/books/edition/report-of-the-taskforce-on-implementation
- Ross, C. A., & Goldner, E. M. (2009). Stigma, negative attitudes and discrimination towards mental illness within the nursing profession: A review of the literature. Journal of Psychiatric & Mental Health Nursing, 16(6), 558–567. https://doi.org/10.1111/j.1365-2850.2009.01399.x
- Sedekia, Y., Jones, C., Nathan, R., Schellenberg, J., & Marchant, T. (2017). Using contraceptives to delay first birth: A qualitative study of individual, community and health provider perceptions in southern Tanzania. BMC Public Health, 17(1). https://doi.org/10.1186/s12889-017-4759-9
- Singh, S., Bankole, A., & Darroch, J. E. (2017). The impact of contraceptive use and abortion on fertility in Sub-Saharan Africa: Estimates for 2003–2014. Population & Development Review, 43(Suppl 1), 141. https://doi.org/10.1111/padr.12027
- Sorber, R., Winston, S., Koech, J., Ayuku, D., Hu, L., Hogan, J., & Braitstein, P. (2014). Social and Economic characteristics of street youth by gender and level of street involvement in Eldoret Kenya. PLoS ONE, 9(5), e97587. https://doi.org/10.1371/journal.pone.0097587
- UNESCO. (2007). Education for all global monitoring report 2008: Education for All by 2015.Will we make it? UNESCO.Pp1–Pp23
- United Nations, Department of Economic and Social Affairs, Population Division. (2015). Trends in contraceptive use worldwide. ST/ESA/SER.A/349
- United Nations, Department of Economic and Social Affairs, Population Division. (2017). Model-based estimates and projection of family planning indicators 2017. United Nations.
- United Nations, Department of Economic and Social Affairs, Population Division. (2019). Contraceptive Use by Method 2019: Data Booklet (ST/ESA/SER.A/435). United Nations. 978-92-1-148329-1. http://www.un.org/development/desa/pd
- United Nations Population Division. (2009). World contraceptive use. New York; United Nations department of economic and social affairs ventures. The Academy of Management Journal, 46(3), 374–384.
- Volpi, E. (2002). Street Children: Promising practice and Approaches. World Bank Institute, 1, 2–7 37196. http://ovcsupport.org/wp-content/uploads/documents/street-children-promising-practices-andApproaches-1.pdf
- Wang, Q., & Sun, X. (2016). The role of socio-political and economic factors in fertility decline: A cross-country analysis. World Development, 87, 360–370. https://doi.org/10.1016/j.worlddev.2016.07.004
- Weinberger, M., Bellows, N., & Stover, J. (2021). Estimating private sector out-of-pocket expenditures on family planning commodities in low-and-middle-income countries. BMJ Global Health, 6(4), e004635. https://doi.org/10.1136/bmjgh-2020-004635
- Wenzel, S., Koegel, P., & Gelberg, L. (2000). Antecedents of physical and sexual victimization among homeless women: A comparison to homeless women men. American Journal of Community Psychology, 28(3), 367–390. https://doi.org/10.1023/A:1005157405618
- Whitney, M., & Glazier, R. (2004). Factors affecting medication adherence among the homeless: A qualitative study of patient’s perspectives. University of Toronto Medical Journal, 82(1), 6–9.
- WHO. (2010). Global Recommendations on Physical Activity for Health. https://www.who.int/publications/i/item/9789241599979
- Withers, M., Kano, M., & Pinatih, G. N. (2010). Desire for more children, contraceptive use and unmet need for family planning in a remote area of Bali, Indonesia. Journal of Biosocial Science, 42(4), 549–562. https://doi.org/10.1017/S0021932010000052
- Woan, J., Lin, J., & Auerswald, C. (2013). The health status of street children and youth in low- and middle-income countries: A systematic review of the literature. Journal of Adolescent Health, 53(3), 314–321.e12. https://doi.org/10.1016/j.jadohealth.2013.03.013
- Zewude, B., Biru, D., & Tesfaye, A. (2019). Pregnancy and child-bearing practices outside the home setting: The case of on-homeless women in Shashemene Town, West Arsi Zone, Ethiopia. Science Journal Womens Health Care, 3(1), 001–007.