
ABSTRACT
The thermosensory system is relevant to both the conceptualization and treatment of depression. There is evidence that depression is associated with changes in thermoregulatory functioning, and that thermosensory pathways can be recruited to influence affect and reduce depressive symptoms. In this study, we investigated the relationship between severity of depressive symptoms and changes to measures of subjective experiences associated with thermoregulatory processes as well as the relationship between severity of depressive symptoms and affective responses to warm stimuli, specifically frequency of warmth-seeking behavior. Participants (N = 529) completed measures of depressive symptoms, subjective experiences associated with thermoregulatory processes (i.e., perceived sweating and preferred ambient temperature) and frequency of warmth-seeking behavior (e.g., long hot baths, saunas, etc.). We demonstrate that, controlling for age and gender, greater severity of depressive symptoms is associated with greater perceived sweating and lower preferred ambient temperature. Furthermore, we demonstrate that greater severity of depressive symptoms is associated with more frequent warmth-seeking behavior, and that something other than thermal preference (i.e., stated preference for warmer temperature) is driving this behavior. These data highlight the importance of incorporating the thermoregulatory system in our conceptualization of the pathophysiology of depression and support the potential to recruit thermosensory pathways to target depressive symptoms.
Introduction
There is emerging evidence that investigating thermosensory systems may help better understand the biology of depression and identify novel antidepressant treatments. Depression is associated with altered thermosensory functioning and thermosensory responses (for review, see [Citation1]). There is also evidence that thermosensory pathways can be recruited to influence affect and target depressive symptoms. Most notably, several clinical trials have shown that exposure to whole-body hyperthermia or hyperthermic baths that elevates core body temperature into a “fever” range (i.e., 38.5 °C) results in a large antidepressant effect that lasts for several weeks [Citation2–5]. The relationship between exposure to warm stimuli, affect, thermoregulation, and depression has been an emerging area of focus in clinical research over recent years [Citation1].
There are multiple factors that contribute to the relationship between warm stimuli and affect. An important influence on the affective response to a warm stimulus is how useful the stimulus is for the body’s thermoregulatory processes, a phenomenon early researchers termed “thermal alliesthesia” [Citation6]. So, as a person’s core body temperature increases, the affective value of warm thermal stimuli decreases, while cool stimuli are experienced as more pleasant [Citation7]. However, non-noxious warm stimuli also influence affect far beyond a simple determination as to whether a stimulus is beneficial for thermoregulatory purposes. For example, non-noxious local skin warming (e.g., via a heat pack or warm cup), has been reported to increase feelings of closeness [Citation8], and prosocial behavior [Citation9] and reduce self-reported negative affect after stressor exposure [Citation10,Citation11]. There is some evidence that warm stimuli directly influence cortical structures involved in affective processing. For instance, skin warming has been shown to inhibit markers of sympathetic activity following stressor exposure [Citation11,Citation12], and to activate neural circuits associated with positive affective responses [Citation13]. Similarly, preclinical research has shown activation of regions of the brain implicated in the inhibition of sympathetic activity following whole-body heating [Citation14].
Depression is associated with altered thermosensory functioning, including changes to thermoregulation and affective responses to warm stimuli. There is a well-established association between depression and elevated core body temperature [Citation15–17]. While the causes of elevated core body temperature are not established, it is likely that depressed individuals are experiencing alterations in the relationship between heat transfer processes and other elements such as thermoregulatory effectors (e.g., sweating), resulting in the “balance-point” for their core body temperature being higher (i.e., resulting in fever [Citation18]). Interestingly, a common side-effect of antidepressant medications, increased sweating [Citation19], also implicates thermoregulatory effectors in the actions of antidepressant drugs. In contrast to physiological changes, there is comparatively little research on the subjective experience of altered thermoregulatory processes associated with depression. A previous study by von Salis, Ehlert, and Fischer [Citation20] found no difference between depressed individuals and healthy controls in terms of perceived sweating and self-reported thermoregulatory behaviors (i.e., removing clothing) in response to increases in ambient warmth. There is also very little research exploring the impact of depression on subjective affective responses to non-noxious warm stimuli. Previous laboratory studies have shown what appears to be an “affective bias” against warm stimuli amongst individuals with depression, including a tendency to rate warm stimuli as more unpleasant [Citation21], and a lower threshold for experiencing warm stimuli as noxious [Citation22].
In contrast to the findings of an affective bias against warm stimuli, a number of observations have indicated that warm stimuli may in fact have particular affective benefits for people with depression. Multiple studies have demonstrated that elevating core body temperature in depressed individuals into a “fever” range (described as elevating to 38.5 °C) results in an antidepressant effect that lasts for at least several weeks (for review, see [Citation23]). The stimuli used to elevate core body temperature have included a form of infrared sauna (e.g [Citation3]., and hot baths (e.g [Citation5]. Further to these clinical trials, there is some research in naturalistic settings showing mood disturbance is associated with an increase in warmth-seeking behavior, such as having hot baths [Citation24] and long hot showers [Citation25]. It is worth noting that replications of the study by Bargh and Shalev [Citation25] have shown variable results, with either no association between mood disturbance and warmth-seeking [Citation26] or successful replication of the initial findings [Citation27]. There is some evidence that a specific symptom profile of depression, namely symptomatology consistent with “atypical depression,” is associated with higher frequency of warmth-seeking behavior [Citation24]. There is also research showing that there is a lower prevalence of selective serotonin reuptake inhibitor (SSRI)-treated mental disorders, including depression, amongst people living in climates with greater ambient temperatures and solar insolation [Citation28], although other studies have shown mixed results regarding the link between mood and weather conditions [Citation29].
In this study, we investigate the relationship between the severity of depressive symptoms (using specific symptom profiles), two measures of subjective experiences associated with thermoregulatory processes (i.e., perceived levels of sweating and preferred ambient temperature), and frequency of warmth-seeking behavior (e.g., accessing sauna, long hot baths, showers, etc.). While we used a non-clinical sample, considering the high prevalence of depression in the global population [Citation30], we expected the sample to include individuals with levels of depressive symptoms consistent with a diagnosis of a mood disorder.
Methods
Participants and procedure
Participants were recruited via e-mail and text via the university research participant database, and via social media more broadly. Participants were provided a link to the online questionnaire, and, upon completion, were provided with a summary of their depression levels based on pre-established clinical cutoffs (i.e., for nil to mild, moderate, and severe). If a participant reported symptoms showing “moderate” to “severe” levels of depressive symptoms, they were provided with an automated message encouraging them to discuss treatment options with a healthcare provider and indicating that there are effective treatment options for depression. After removing incomplete response the sample consisted of N = 529 participants (377 female, Mage = 25.96 years, SDage = 0.33, age range = 18–52 years). Participant gender was identified by self-report questionnaire, with the question “Do you identify as male, female or other,” with a short-response option if the participant allocated “other.” Eligibility criteria included being 18 years old or older and proficiency in English (in order to complete the self-report questionnaires accurately and to provide informed consent). Institutional ethics approval was granted from the La Trobe University Human Ethics Committee (HEC18122) and consent was obtained by participants prior to commencement of the questionnaire.
Measures
Assessment of severity of depressive symptoms
The Centre for Epidemiological Studies – Depression Scale Revised 14-item Version (CES-D-14) is a 14-item measure of symptoms associated with depression that have been experienced over the past week [Citation31]. The CES-D-14 proposes to improve on the original CES-D measure by removing items that inflate scores in women, and by presenting a 3-factor structure (negative affect, anhedonia, and somatic symptoms) that are more appropriate for current diagnostic criteria for depression [Citation31–33]. Previous research has indicated a score of 16 on the CES-D-14 as the optimal cutoff to identify individuals at risk of clinical depression, with good sensitivity and specificity [Citation32]. Cronbach’s alpha for the present study was .87 for the Negative Affect subscale, and .86 for the Anhedonia subscale, both showing high internal consistency, and .78 for the somatic subscale, showing adequate internal consistency.
Assessment of subjective experiences associated with thermoregulatory processes
We generated an 8-item Likert measure (see ) assessing subjective experiences associated with thermoregulatory processes. This included perception of thermoregulatory effectors [Citation18], namely perceived sweating, and an indirect measure of thermoregulatory behavior, namely preferred ambient temperature. We also asked participants to report on their perceived body temperature. Questions assessed perceived sweating, preferred ambient temperature, and perceived body temperature at nighttime, during the day and during exercise. We conducted an exploratory factor analysis on the scale to identify latent constructs in the measure (psychometrics described below in section 3.2).
Table 1. Summary of exploratory factor analysis results for the measure of subjective experiences associated with thermoregulatory processes.
Assessment of frequency of warmth-seeking behaviour
Participants were asked how many warming activities they engaged in, on average, per month. Activities included saunas, long hot baths, and hot showers (over 10 min), steam room, and other activities. Participants indicated frequency using a Likert scale ranging from 0 (none) to 28 (daily). If participants indicated they engaged in multiple warming activities, these were combined to create an average frequency of overall warming activities per month (e.g., if sauna was accessed once per month, and long hot baths were accessed once per month, frequency of warming activities would be twice per month).
Statistical method
All data were analyzed using IBM SPSS Statistics version 27.0 [Citation34] (IBM Corp., Armonk, NY, USA). Data were checked for outliers, missing data, multicollinearity and violation of normality. Outliers, identified as z scores exceeding 3.29 [Citation35] p. 107), were windsorized to the next highest score + 1, or the next lowest score −1 in order to reduce their disproportionate influence on inferential analyses [Citation35] p. 111). Due to the need to control for the known influence of sex on thermoregulation, [Citation36] the 5 participants who selected non-binary, transgender or agender for the gender item were not included in the inferential analysis, but their descriptive data are included in the descriptives section below. Participants were excluded if they had completed less than 75% of the questionnaire (n = 44) as completion needed to be above this cutoff for all variables relevant for analysis to be completed. The age variable was found to have a negative skew and the frequency of warmth-seeking behavior measure had a positive skew. Attempts to use common transformations to correct the distributions were unsuccessful so we proceeded with untransformed data, considering that large samples are robust to violations of normality [Citation37] p. 184). The Kaiser-Meyer-Olkin (KMO) measure and Bartlett’s test of sphericity were used to confirm the data were suitable for factor analysis.
Power analysis (G * Power [Citation38]; for a moderated regression with 5 predictors, with a statistical power of 80%, α = .05 and a small effect size of f2 = .02, showed that a sample size of 395 would be sufficient to detect relationships between severity of depressive symptoms and measures of subjective experiences associated with thermoregulatory processes and, separately, frequency of warmth-seeking behavior, while controlling for age and gender.
Pearson’s correlation coefficients were calculated to determine associations between key variables. Principal axis factoring was the method used for factor extraction. The direct oblimin rotation method was used, as the factors were unlikely to be independent of each other [Citation37] p. 681). Kaiser’s criterion of eigenvalues over 1 was used to identify factors. Hierarchical regressions that controlled for age and gender were used to determine the relationship between severity of depressive symptoms and measures of subjective experiences associated with thermoregulatory processes (i.e., perceived sweating and preferred ambient temperature), and to determine the relationship between severity of depressive symptoms and frequency of warmth-seeking behavior. A moderated regression was conducted using the macro-program PROCESS 3.4.1 [Citation39] with bootstrapping (N = 5000) to determine whether subjective experiences associated with thermoregulatory processes influenced the relationship between severity of depressive symptoms and frequency of warmth-seeking behavior. To explore the findings from the moderated regression, we used a cluster analysis to identify subgroups (clusters) of participants who had a similar pattern of scores across the preferred ambient temperature and somatic depressive symptoms measures. As we did not have a clear expectation of the number of clusters that may emerge, we used a two-step cluster analysis. Unlike some forms of cluster analysis, two-step cluster analysis does not rely on the subjective assessment of visual information to identify clusters, it uses a log-likelihood distance measure to identify distinctiveness between individuals and then a probabilistic approach and silhouette statistics to identify and classify, respectively, the optimal subgroup model. Two-step cluster analysis performs well when all variables are continuous, has appropriate sensitivity to subgroups, and has ease of use and interpretability compared to other clustering techniques [Citation40]. We then used a one-way analysis of variance (ANOVA) followed by post hoc tests to identify differences in the frequency of warmth-seeking behavior between the subgroups. Based on previous research identifying that age and sex can impact on thermosensory functioning [Citation36,Citation41], these variables were included as covariates for all regression analyses.
Figures were generated using Jamovi software package [Citation42] along with the JJStatsPlot module [Citation43–46].
Results
Descriptives
Based on the recommended cutoff score of 16 on the CES-D-14, 73% of the sample reported levels of depressive symptoms that indicated they were at risk of clinical depression (M = 21.95, SD = 9.46, see ). The majority of participants (79.4%) engaged in some kind of warming activity at least once a month (Mfrequency = 12.80 times per month, SDfrequency = 11.74, range = 0–52 times per month).
Figure 1. Graph showing individual data points for CES-D-14 scores. The dashed line indicates the clinical cutoff for depression of 16 using the CES-D-14. Abbreviations: CES-D-14, Center for Epidemiological Studies – Depression Scale Revised 14-item Version.
Exploratory factor analysis on measures of subjective experiences associated with thermoregulatory processes
A principal axis factor analysis was conducted on the eight items of the scale measuring subjective experiences associated with thermoregulatory processes with oblique rotation (direct oblimin). The Kaiser-Meyer-Olin measure indicated the data were suitable for the analysis (KMO = .70). Three factors had eigenvalues over 1, and the scree plot also showed an inflexion at 3 factors. However, inspection of factor loadings after rotation showed that one factor had only a single item loading on it (“Compared to other people, what does your body temperature feel like at night?”), and so it was removed. The items that clustered on the remaining two factors suggested one represented perceived level of sweating, and the other preferred ambient temperature. One item on the perceived sweating factor was excluded due to its low factor loading. shows factor loadings after rotation and Cronbach’s α for the subscales, showing that both had adequate reliability.
Validation of the measure of the preferred ambient temperature subscale
Consistent with established gender and age differences in thermoregulation (Kim et al., 1998 [Citation41], female gender and greater age were associated with a preference for higher ambient temperature. A one-way ANOVA demonstrated that female participants reported a preference for higher ambient temperature than male participants, after controlling for age differences, F(1, 526) = 7.12, p < .01, ηp2 = .01. A hierarchical linear regression showed that age explained preferred ambient temperature, after controlling for gender differences. After step 1, with gender entered, R = .10, R2 = .01, F(1, 527) = 5.80, p = .02. After step 2, with age entered into the equation, R = .18, R2 = .03, ΔR2 = .02, F(2, 526) = 11.41, p < .001, indicating that age uniquely explained 2% of the variance in preferred ambient temperature, with greater age predicting higher preferred ambient temperature. Together, these findings support the criterion validity of the preferred ambient temperature subscale. There was no influence of gender nor age on perceived level of sweating. See for correlation coefficients between study variables.
Table 2. Pearson correlation coefficients for the study variables.
What is the relationship between severity of depressive symptoms and subjective experiences associated with thermoregulatory processes?
The combination of depressive symptom measures entered at Step 2 were significantly associated with both measures of subjective experiences associated with thermoregulatory processes (see ). Specifically, greater severity of depressive symptoms was associated with lower preferred ambient temperature and greater perceived sweating. After controlling for the influence of age and gender, severity of depressive symptoms explained a significant additional 2% of the variance in each measure of subjective experiences associated with thermoregulatory processes. None of the individual subscales were associated with either perceived sweating or preferred ambient temperature.
Table 3. Hierarchical regression analyses assessing the relationship between subscales of depressive symptoms and perceived sweating and preferred ambient temperature, after controlling for age and gender.
Is there a positive association between severity of depressive symptoms and frequency of warmth-seeking behaviour?
We used a hierarchical regression to assess if the association of each depressive symptom measure (or their combined association) were positively associated with the frequency of warmth-seeking behavior.
The cumulative association of depressive symptom measures at Step 2 with the frequency of warmth-seeking behavior was significant, with higher scores on the Somatic subscale associated with a higher frequency of warmth-seeking behavior. The items that comprise the Somatic subscale for the CES-D-14 are outlined in , below. Overall, the severity of depressive symptoms on the subscales together explained 2% of the variance in frequency of warmth-seeking behavior after controlling for the influence of age and gender. Only the Somatic subscale, with a β of .17, uniquely explained variance in frequency of warmth-seeking behavior, with greater severity of symptoms associated with greater frequency of warmth-seeking behavior (see ).
Table 4. Items comprising the somatic subscale for the CES-D-14.
Table 5. Hierarchical regression analysis assessing the relationship between subscales of depressive symptoms and frequency of warmth-seeking behavior, after controlling for age and gender.
Do measures of subjective experiences associated with thermoregulatory processes moderate the relationship between severity of somatic depressive symptoms and frequency of warmth-seeking behaviour?
Preferred ambient temperature moderated the impact of severity of somatic depressive symptoms on frequency of warmth-seeking behavior (b = −.02, t(520) = −2.00, p = .046), indicating that the positive association between somatic depressive symptoms and frequency of warmth-seeking behavior was observed amongst participants reporting a preference for low to moderate ambient temperature (see ). Perceived level of sweating did not moderate the relationship between somatic depressive symptoms and frequency of warmth-seeking behavior (b = .00, t(520) = .50, p = .623). A direct effect of somatic depressive symptom scores on the frequency of warmth-seeking behavior also emerged (b = .44, t(520) = 3.49, p < .001), showing greater severity of somatic depressive symptoms predicted greater frequency of warmth-seeking behavior. Similarly, there were direct effects of the preferred ambient temperature (b = .15, t(520) = 3.13, p = .002), and perceived sweating (b = −.02, t(520) = −2.76, p = .006), showing that the frequency of warmth-seeking behavior was higher as the preferred ambient temperature was higher, and perceived sweating lower.
Figure 2. Graph showing that preferred ambient temperature moderated the relationship between severity of somatic depressive symptoms and frequency of warmth-seeking behavior. Abbreviations: CES-D-14, center for epidemiologic studies depression scale revised 14-item version. Note: CES-D-14-somatic scores, preferred ambient temperature and perceived sweating were mean-centered to perform the moderated regression.
Are there subgroups of people organized around the domains of severity of somatic depressive symptoms and preferred ambient temperature?
To better understand the findings from the moderated regression, we conducted a two-step cluster analysis, and a five-cluster solution was found to be the best fit for the data. The silhouette measure of cohesion and separation was .40, suggesting the five-factor solution was a fair quality solution. The five-clusters that were identified within the data, derived from patterns of responses on the somatic depressive symptom subscale and preferred ambient temperature measure, were: “High-depression desiring cool ambient temp” (Cluster 1, n = 150); “High depression desiring warm ambient temp” (Cluster 2, n = 75); “High depression desiring cold ambient temp” (Cluster 3, n = 67); “Low depression desiring cool ambient temp” (Cluster 4, n = 103); and “Low depression desiring warm ambient temp” (Cluster 5, n = 134). Cluster 1 (High-depression desiring cool ambient temp) and cluster 3 (High depression desiring cold ambient temp) were differentiated by the fact that, while the mean preferred ambient temperatures in both clusters were lower than the “warm temp” clusters, there was a significant difference in mean preferred temperature between the clusters, with cluster 3 showing a mean 16.34 points lower than cluster 1. The “preferred ambient temperature” measure was a composite measure (i.e., based on the subscales identified in the Exploratory Factor Analysis). Hence, “points” here are not simple units of temperatures (e.g., °C), but represented a participant’s score on the combined items (i.e., a combination of preferred ambient temperature at night, during the day and while exercising). Mean scores and standard deviations for each cluster are presented in .
Table 6. Means of somatic depressive symptoms and thermoregulatory measures for sample and clusters.
Do these subgroups differ in their frequency of warmth-seeking behaviour?
A one-way between-subjects ANOVA showed that the frequency of warmth-seeking behavior differed between clusters (). Post hoc comparisons demonstrated that, after Holm adjustment to correct for familywise error, participants in cluster 4 (“low depression desiring cool ambient temp”) attended warming activities less than those in cluster 2 (“high depression desiring warm ambient temp”), with no difference in frequency between other clusters (see ).
Figure 3. Plots showing means and distributions for frequency of warmth-seeking behavior across clusters. Note: p value is after Holm adjustment to correct for familywise error.
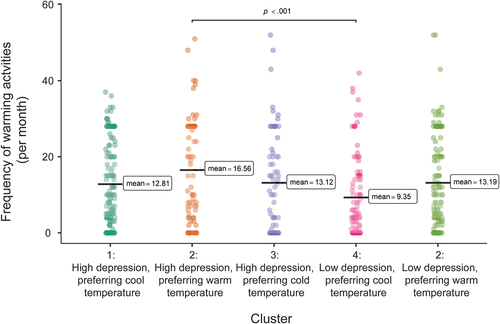
Table 7. Frequency of warmth-seeking behaviour - means and standard deviations by cluster.
Discussion
The findings demonstrated a relationship between severity of depressive symptoms, measures of subjective experiences associated with thermoregulatory processes and self-reported frequency of warmth-seeking behavior. There was a positive association between the frequency of warmth-seeking behavior and the severity of somatic depressive symptoms. Greater severity of depressive symptoms was also associated with differences in measures of subjective experiences associated with thermoregulatory processes, namely greater perceived sweating and lower preferred ambient temperature. A relationship between measures of subjective experiences associated with thermoregulatory processes and the frequency of warmth-seeking behavior emerged, with lower preferred ambient temperature and greater perceived sweating both associated with lower frequency of warmth-seeking behavior. However, moderation analysis showed that participants reporting higher levels of somatic depressive symptoms accessed warming activities more frequently, even when reporting a preference for lower ambient temperature. We identified five clusters or subgroups in the data, which differed in patterns of responses on the preferred ambient temperature and somatic depressive symptom measures. Participants belonging to a subgroup in the sample with low levels of depressive symptoms and a preference for cooler temperatures accessed warming activities less frequently than participants in a subgroup with high levels of depressive symptoms and a preference for warmer temperatures. However, participants belonging to subgroups with high levels of depressive symptoms who also expressed a preference for cooler temperatures accessed warming activities at the same frequency as participants expressing a preference for warmer temperatures. Together, these data suggest that participants with greater severity of somatic depressive symptoms accessed warming activities more frequently, and that this positive association held even when there was a stated preference for cooler temperatures, suggesting something other than thermal preference may be driving their behavior.
Our results show an increase in warmth-seeking behavior as the severity of somatic depressive symptoms increases. Our observations, in a naturalistic setting, support the hypothesis that warm stimuli may have specific benefits for individuals with depression [Citation1]. Interestingly, the somatic subscale of the CES-D-14 is characterized by changes in appetite and fatigue, symptoms that are also consistent with “atypical depression,” which has been previously linked to greater frequency of warmth-seeking behavior [Citation24]. Similarly, previous research has shown that repeated exposure of depressed inpatients to infrared sauna led to specific reductions in somatic complaints, including appetite and fatigue [Citation47]. Possible explanations for greater frequency of warmth-seeking behavior amongst individuals with greater severity of somatic depressive symptoms are explored below.
Our findings suggest a link between the severity of depressive symptoms and changes to measures of subjective experiences associated with thermoregulatory processes. Greater severity of depressive symptoms was associated with lower preferred ambient temperature, and greater perceived sweating. The relationship between depressive symptoms and measures of subjective experiences associated with thermoregulatory processes is consistent with research showing a link between depression and elevated core body temperature [Citation15,Citation16]. Greater perceived sweating is likely a function of elevated core body temperature, as sweating increases as core body temperature increases [Citation48]. Similarly, a preference for lower ambient temperature would be expected if core body temperature was elevated, as seeking cooler temperature is a thermoregulatory behavior used to defend against heat [Citation6,Citation18].
To our knowledge, this is the first time an association between depressive symptoms and differences in measures of subjective experiences associated with thermoregulatory processes has been identified. A previous study by von Salis et al. [Citation20] identified impairments in vigilance (e.g., reduced concentration) in warm environments in depressed individuals, but no difference in subjective experiences related to thermoregulatory effectors (i.e., perceived sweating) nor self-reported thermoregulatory behaviors (i.e., changing clothing). Our sample included individuals with greater severity of depressive symptoms (i.e., 73% at risk of depression in our study, 15% at risk in the von Salis et al. [Citation20] study), which may have increased our ability to identify differences in measures of subjective experiences associated with thermoregulatory processes. The relatively high proportion of participants reporting depressive symptoms above the clinical cutoff in the current study may have resulted from the fact that participants received a summary of their levels of depressive symptoms following completion of the questionnaire. People experiencing mood disturbance may have been more likely to participate in order to get feedback on their level of depressive symptoms. Beyond the greater severity of depressive symptoms in our sample, using continuous measures of depression afforded us with more statistical power than similarly sized studies that used binary classifications of depression [Citation20]. This design choice may explain the difference in findings between studies.
Our findings show a link between measures of subjective experience associated with thermoregulatory processes and the frequency of warmth-seeking behavior. The findings show a tendency for people with a preference for warmer ambient temperature and lower perceived level of sweating to access warming activities more frequently. It is unsurprising that an association between these variables was observed, if they are all viewed as mechanisms to defend against heat and cold. For example, if a person was needing to defend against heat, they are likely to experience increased sweating, have a preference for cooler ambient temperature, and would be unlikely to seek warm stimuli such as hot baths or sauna. Conversely, if a person was defending against cold, they would experience a lack of sweating, have a preference for warmer ambient temperature and be more likely to seek warm stimuli.
The findings from both the moderated regression and the cluster analysis showed that participants reporting higher severity of somatic depressive symptoms accessed warming activities more frequently, even if they reported a preference for cooler temperatures. This suggests that the function of warmth-seeking behavior amongst individuals with high levels of somatic depressive symptoms is beyond just defending against cold (i.e., as they are reporting greater warmth-seeking behavior even when reporting a preference for cooler ambient temperature). The fact that perceived sweating did not influence the relationship between the severity of depressive symptoms and warmth-seeking behavior is consistent with contemporary understanding of thermoregulatory effectors being relatively independent [Citation49].
While it appears that something other than thermoregulatory requirements may be driving the warmth-seeking behavior of participants with greater severity of somatic depressive symptoms, it is unclear what specific benefits individuals were experiencing from accessing the warming activities. There is some evidence that exposure to warm stimuli inhibits sympathetic nervous system activity [Citation11,Citation12,Citation14], and that depression is associated with sympathetic nervous system hyper-reactivity [Citation50]. Furthermore, warm cutaneous stimulation activates hedonic circuits in association with perceived pleasantness of warm stimuli [Citation13]. Perhaps participants with higher levels of somatic depressive symptoms access warming activities more frequently in an attempt to downregulate sympathetic nervous system overactivation.
In the context of research showing an antidepressant effect of whole-body hyperthermia and hyperthermic baths [Citation2–5], our findings raise the possibility that individuals with high levels of depressive symptoms may be accessing warming activities such as sauna and long hot baths or showers in an attempt to alleviate symptoms associated with depression. However, the fact that there was a positive association between depressive symptoms and warmth-seeking behavior suggests that there was no lasting antidepressant effect resulting from the warming activities that participants accessed in our study, although it is feasible that their scores may have been higher if they had not been engaged in warming activities. Elevating core body temperature into a fever range (i.e., defined as 38.5 °C in whole-body hyperthermia studies) is difficult to achieve, due to the body’s thermoregulatory cooling processes. For example, a previous study using hyperthermic baths required participants to remain in a 40 °C bath for half an hour, followed by another half hour wrapped in blankets and two hot water bottles, to raise core body temperature to the required level [Citation4]. Thus, the warming activities participants accessed in the current study may not have sufficiently elevated core body temperature to elicit the antidepressant effect seen in the whole-body hyperthermia clinical trials. So, it may be that individuals with high levels of depressive symptoms are self-administering whole-body heating and possibly experiencing some acute affective benefits (e.g., in the form of inhibited sympathetic nervous system activity or activation of hedonic circuits) but failing to experience a lasting antidepressant effect due to a lack of sufficient elevation of core body temperature.
We did not analyze the specific type of warming activity that participants were engaged in, and it is possible that different activities have different relationships with depressive symptoms. For example, previous research has demonstrated improved mood resulting from long hot baths but not long hot showers [Citation51,Citation52]. Our research was cross-sectional, and causality regarding the relationships between the variables cannot be determined. Our assessment of depressive symptoms was limited to self-report, and it was not possible to determine which participants were clinically depressed. We did not assess for comorbid psychopathology and cannot rule out possible confounding disorders influencing our results. For example, the somatic subscale of the CES-D-14 includes items that may be influenced by conditions such as chronic pain or insomnia (e.g., “everything I did was an effort,” “my sleep was restless”). While there is comorbidity between depression and these conditions [Citation53], they are nonetheless distinct phenomena [Citation54]. If participants reporting greater somatic depressive symptoms were actually suffering from chronic pain or insomnia, they may have been accessing warming activities to alleviate these conditions rather than mood disturbance. Overall, participants in our sample were relatively young and, while we controlled for the influence of age in our analyses, future research with older populations would help clarify if there are age-related differences in the relationships between the variables. Finally, we did not assess antidepressant use, and so could not control for the influence of medication on the relationship between the variables. In particular, the finding that the greater severity of depressive symptoms was associated with greater perceived sweating is complicated by the fact that increased sweating is also a common side effect of antidepressant medication [Citation19]. Future research is needed to clarify any role of antidepressant medication on subjective experiences associated with thermoregulatory processes.
Conclusions
In summary, our study provides evidence that severity of depressive symptoms is associated with changes to thermosensory processes, namely subjective experiences associated with thermoregulatory processes and affective responses to warm stimuli. The finding that depressive symptoms were associated with changes to subjective experiences associated with thermoregulatory processes (i.e., perceived sweating and preferred ambient temperature) reinforces the importance of including the thermosensory system (incorporating both peripheral and central nervous system processes) in our conceptualization of depression. The positive association between somatic depressive symptoms and the frequency of warmth-seeking behavior identified in our study supports the hypothesis that the thermosensory system can be recruited to target depressive symptoms. While it appears that something other than thermoregulatory demands (i.e., defense against cold) is driving greater frequency of warmth-seeking behavior in individuals with high levels of somatic depressive symptoms, future research is needed to investigate exactly what is driving this association. The link between non-noxious warming and the inhibition of sympathetic nervous system activity [Citation11,Citation12,Citation14] may provide one explanation worth testing. Activation of positive affective circuits by warm stimuli is another [Citation13]. Qualitative research may also clarify the specific benefits of warmth exposure for individuals with high levels of somatic depressive symptoms. Controlling for the influence of comorbid pathology (e.g., insomnia and chronic pain), and medication use in future studies would help identify the specific influence of depressive symptoms on warmth-seeking behavior and subjective experiences associated with thermoregulatory processes. While our sample included a large proportion of individuals with depressive symptoms consistent with a diagnosable disorder, it remains to be tested whether these findings translate to a clinical population.
Our results suggest that individuals with high levels of a somatic subtype of depressive symptom can access warming activities for some affective benefit. Our findings provide support from a naturalistic setting for the hypothesis that thermoregulatory pathways can be recruited to target depressive symptoms. Interventions such as whole-body hyperthermia, which use warmth exposure for antidepressant effect, are relatively novel in the scientific literature [Citation55]. However, our findings suggest that individuals in the community with high levels of depressive symptoms may already be self-administering warmth exposure for some affective benefit.
CRediT author statement
Mark Tyler: Conceptualization, Methodology, Formal analysis, Investigation, Writing – Original Draft, Visualization, Project administration. Bradley Wright: Methodology, Formal analysis, Writing – Review & Editing. Charles Raison: Conceptualization, Writing – Review & Editing. Christopher Lowry: Conceptualization, Writing – Review & Editing. Lynette Evans: Conceptualization, Writing – Review & Editing. Matthew Hale: Conceptualization, Methodology, Writing – Review & Editing, Supervision, Project Administration.
List of abbreviations
| ANOVA | = | analysis of variance |
| CES-D-14 | = | Centre for Epidemiological Studies – Depression Scale Revised 14-item Version |
| SD | = | standard deviation |
| SSRI | = | selective serotonin reuptake inhibitor |
Disclosure statement
MPT, BJW, RB, KM, LE and MWH report no financial relationships with commercial interests. CAL is Cofounder, Board Member, and Chief Scientific Officer of Mycobacteria Therapeutics Corporation, and is a member of the faculty of the Integrative Psychiatry Institute, Boulder, Colorado, the Institute for Brain Potential, Los Banos, California, and Intelligent Health, Reading, UK. CLR serves as a consultant to Usona Institute, Novartis, Biogen/Sage, and Emory Healthcare.
References
- Raison CL, Hale MW, Williams L, et al. Somatic influences on subjective well-being and affective disorders: the convergence of thermosensory and central serotonergic systems. Front Psychol. 2015;5:1580. doi: 10.3389/fpsyg.2014.01580
- Hanusch K-U, Janssen CH, Billheimer D, et al. Whole-body hyperthermia for the treatment of major depression: associations with thermoregulatory cooling. AJP. 2013;170(7):802–804. doi: 10.1176/appi.ajp.2013.12111395
- Janssen CW, Lowry CA, Mehl MR, et al. Whole-body hyperthermia for the treatment of major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2016;73(8):789–795. doi: 10.1001/jamapsychiatry.2016.1031
- Naumann J, Grebe J, Kaifel S, et al. Effects of hyperthermic baths on depression, sleep and heart rate variability in patients with depressive disorder: a randomized clinical pilot trial. BMC Complement Altern Med. 2017;17(1):172. doi: 10.1186/s12906-017-1676-5
- Naumann J, Kruza I, Denkel L, et al. Effects and feasibility of hyperthermic baths in comparison to exercise as add-on treatment to usual care in depression: a randomised, controlled pilot study. BMC Psychiatry. 2020;20(1):1–13. doi: 10.1186/s12888-020-02941-1
- Cabanac M. Physiological role of pleasure. Science. 1971;173(4002):1103–1107. doi: 10.1126/science.173.4002.1103
- Mower GD. Perceived intensity of peripheral thermal stimuli is independent of internal body temperature. J Prof Nurs. 1976;90(12):1152. doi: 10.1037/h0077284
- Inagaki TK, Ross LP. A body-to-mind perspective on social connection: physical warmth potentiates brain activity to close others and subsequent feelings of social connection. Emotion. 2021;21(4):812. doi: 10.1037/emo0000749
- Williams LE, Bargh JA. Experiencing physical warmth promotes interpersonal warmth. Science. 2008;322(5901):606–607. doi: 10.1126/science.1162548
- IJzerman H, Gallucci M, Pouw WT, et al. Cold-blooded loneliness: social exclusion leads to lower skin temperatures. Acta Psychol. 2012;140(3):283–288. doi: 10.1016/j.actpsy.2012.05.002
- Kober A, Scheck T, Tschabitscher F, et al. The influence of local active warming on pain relief of patients with cholelithiasis during rescue transport. Anesth Analg. 2003;96(5):1447–1452. doi: 10.1213/01.ane.0000056825.55397.1f
- Hornstein EA, Fanselow MS, Eisenberger NI. Warm hands, warm hearts: an investigation of physical warmth as a prepared safety stimulus. Emotion. 2022;22(7):1517. doi: 10.1037/emo0000925
- Rolls ET, Grabenhorst F, Parris BA. Warm pleasant feelings in the brain. Neuroimage. 2008;41(4):1504–1513. doi: 10.1016/j.neuroimage.2008.03.005
- Hale MW, Dady KF, Evans AK, et al. Evidence for in vivo thermosensitivity of serotonergic neurons in the rat dorsal raphe nucleus and raphe pallidus nucleus implicated in thermoregulatory cooling. Exp Neurol. 2011;227(2):264–278. doi: 10.1016/j.expneurol.2010.11.012
- Avery D, Shah S, Eder D, et al. Nocturnal sweating and temperature in depression. Acta Psychiatr Scand. 1999;100(4):295–301. doi: 10.1111/j.1600-0447.1999.tb10864.x
- Mason AE, Kasl P, Soltani S, et al. Elevated body temperature is associated with depressive symptoms: results from the TemPredict study. Sci Rep. 2024;14(1):1884. doi: 10.1038/s41598-024-51567-w
- Rausch JL, Johnson M, Corley K, et al. Depressed patients have higher body temperature: 5-HT transporter long promoter region effects. Neuropsychobiology. 2003;47(3):120–127. doi: 10.1159/000070579
- Romanovsky AA. The thermoregulation system and how it works. Handb Clin Neurol. 2018;156:3–43.
- Marcy TR, Britton ML. Antidepressant-induced sweating. Ann Pharmacother. 2005;39(4):748–752. doi: 10.1345/aph.1E564
- von Salis S, Ehlert U, Fischer S. Altered experienced thermoregulation in depression—no evidence for an effect of early life stress. Front Psychiatry. 2021;12. doi: 10.3389/fpsyt.2021.620656
- Strigo IA, Simmons AN, Matthews SC. Increased affective bias revealed using experimental graded heat stimuli in young depressed adults: evidence of “emotional allodynia”. Psychosom Med. 2008;70(3):338. doi: 10.1097/PSY.0b013e3181656a48
- Ushinsky A, Reinhardt LE, Simmons AN, et al. Further evidence of emotional allodynia in unmedicated young adults with major depressive disorder. PLOS ONE. 2013;8(11):e80507. doi: 10.1371/journal.pone.0080507
- Hanusch K-U, Janssen CW. The impact of whole-body hyperthermia interventions on mood and depression–are we ready for recommendations for clinical application? International J of Hyperthermia. 2019;36(1):572–580. doi: 10.1080/02656736.2019.1612103
- Parker G, Crawford J. Chocolate craving when depressed: a personality marker. Br J Psychiatry. 2007;191(4):351–352. DOI:10.1192/bjp.bp.106.033746
- Bargh JA, Shalev I. The substitutability of physical and social warmth in daily life. Emotion. 2012;12(1):154–162. doi: 10.1037/a0023527
- Donnellan MB, Lucas RE, Cesario J. On the association between loneliness and bathing habits: nine replications of bargh and shalev (2012) study 1. Emotion. 2015;15(1):109. doi: 10.1037/a0036079
- Shalev I, Bargh J. On the association between loneliness and physical warmth-seeking through bathing: reply to Donnellan et al.(2014) and three further replications of Bargh and Shalev (2012) study 1. Emotion. 2015;15(1):120–123. doi: 10.1037/emo0000014
- Wortzel J, Norden J, Turner B, et al. Ambient temperature and solar insolation are associated with decreased prevalence of SSRI-treated psychiatric disorders. J Psychiatr Res. 2019;110:57–63. doi: 10.1016/j.jpsychires.2018.12.017
- Keller MC, Fredrickson BL, Ybarra O, et al. A warm heart and a clear head: the contingent effects of weather on mood and cognition. Psychol Sci. 2005;16(9):724–731. doi: 10.1111/j.1467-9280.2005.01602.x
- World Health Organization (2017). Depression and other common mental disorders: global health estimates. Available from https://www.who.int/publications/i/item/depression-global-health-estimates
- Carleton RN, Thibodeau MA, Teale MJ, et al. The center for epidemiologic studies depression scale: a review with a theoretical and empirical examination of item content and factor structure. PLOS ONE. 2013;8(3):e58067. doi: 10.1371/journal.pone.0058067
- Jiang L, Wang Y, Zhang Y, et al. The reliability and validity of the center for epidemiologic studies depression scale (CES-D) for Chinese university students. Front Psychiatry. 2019;10:315. doi: 10.3389/fpsyt.2019.00315
- Yang L, Jia C-X, Qin P. Reliability and validity of the center for epidemiologic studies depression scale (CES-D) among suicide attempters and comparison residents in rural China. BMC Psychiatry. 2015;15(1):1–8. doi: 10.1186/s12888-015-0458-1
- IBM Corp. IBM SPSS statistics for windows, version 27.0 (released). Armonk, NY: IBM Corp; 2020.
- Tabachnick BG, Fidell LS, Ullman JB. Using multivariate statistics. Vol. 6. Boston, MA: Pearson Education; 2014.
- Kim H, Richardson C, Roberts J, et al. Cold hands, warm heart. The Lancet. 1998;351(9114):1492. doi: 10.1016/S0140-6736(05)78875-9
- Field A. Discovering statistics using IBM SPSS statistics. London, UK: SAGE; 2013.
- Faul F, Erdfelder E, Buchner A. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi: 10.3758/BRM.41.4.1149
- Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York, NY, USA: Guilford Press; 2017.
- Kent P, Jensen RK, Kongsted A. A comparison of three clustering methods for finding subgroups in MRI, SMS or clinical data: SPSS TwoStep cluster analysis, latent gold and SNOB. BMC Med Res Methodol. 2014;14(1):1–14. doi: 10.1186/1471-2288-14-113
- Van Someren EJ. More than a marker: interaction between the circadian regulation of temperature and sleep, age-related changes, and treatment possibilities. Chronbiol Int. 2000;17(3):313–354. doi: 10.1081/CBI-100101050
- The jamovi project (2022). jamovi. (Version 2.3) Computer software. https://www.jamovi.org
- Patil I (2018). ggstatsplot: ‘ggplot2’ based plots with statistical details. [R package]. https://CRAN.R-project.org/package=ggstatsplot
- R Core Team (2021). R: A language and environment for statistical computing. (version 4.1) [Computer software]. https://cran.r-project.org ( R packages retrieved from MRAN snapshot 2022–01-01).
- Balci S (2022). ClinicoPath jamovi Module. [R Package]. https://github.com/sbalci/ClinicoPathJamoviModule
- Wickham H, Chang W, Henry L, et al. (2018). ggplot2: create elegant data visualisations using the grammar of graphics. [R package]. https://CRAN.R-project.org/package=ggplot2
- Masuda A, Nakazato M, Kihara T, et al. Repeated thermal therapy diminishes appetite loss and subjective complaints in mildly depressed patients. Psychosom Med. 2005;67(4):643–647. doi: 10.1097/01.psy.0000171812.67767.8f
- Osilla E, Marsidi J, Shumway K, et al. (2018). Physiology, temperature regulation. StatPearls. Treasure Island, FL, USA.
- McAllen RM, Tanaka M, Ootsuka Y, et al. Multiple thermoregulatory effectors with independent central controls. Eur J Appl Physiol. 2010;109(1):27–33. doi: 10.1007/s00421-009-1295-z
- Hu MX, Lamers F, de Geus EJ, et al. Differential autonomic nervous system reactivity in depression and anxiety during stress depending on type of stressor. Psychosom Med. 2016;78(5):562–572. doi: 10.1097/PSY.0000000000000313
- Goto Y, Hayasaka S, Kurihara S, et al. Physical and mental effects of bathing: a randomized intervention study. Evid Based Complement Alternat Med, 2018. 2018;2018:1–5. doi: 10.1155/2018/9521086
- Tai Y, Obayashi K, Yamagami Y, et al. Association between passive body heating by hot water bathing before bedtime and depressive symptoms among community-dwelling older adults. Am J Geriatr Psychiatry. 2022;30(2):161–170. doi: 10.1016/j.jagp.2021.06.010
- Steffen A, Nübel J, Jacobi F, et al. Mental and somatic comorbidity of depression: a comprehensive cross-sectional analysis of 202 diagnosis groups using German nationwide ambulatory claims data. BMC Psychiatry. 2020;20(1):1–15. doi: 10.1186/s12888-020-02546-8
- Lerman SF, Rudich Z, Shahar G. Distinguishing affective and somatic dimensions of pain and depression: a confirmatory factor analytic study. J Clin Psychol. 2010;66(4):456–465. doi: 10.1002/jclp.20674
- Knobel A, Hanusch K, Auen N, et al. Whole-body hyperthermia (WBH) in psychiatry. In: Vaupel P, editor. Water-filtered Infrared A (wIRA) irradiation. Cham: Springer; 2022. p. 155–164.