
Abstract
Objectives: To evaluate the micro-tensile repair bond strength between aged and new composite, using silane and adhesives that were cured or left uncured when new composite was placed.
Methods: Eighty Filtek Supreme XLT composite blocks and four control blocks were stored in water for two weeks and thermo-cycled. Sandpaper ground, etched and rinsed specimens were divided into two experimental groups: A, no further treatment and B, the surface was coated with bis-silane. Each group was divided into subgroups: (1) Adper Scotchbond Multi-Purpose, (2) Adper Scotchbond Multi-Purpose adhesive, (3) Adper Scotchbond Universal, (4) Clearfil SE Bond and (5) One Step Plus. For each adhesive group, the adhesive was (a) cured according to manufacturer’s instructions or (b) not cured before repair. The substrate blocks were repaired with Filtek Supreme XLT. After aging, they were serially sectioned, producing 1.1 × 1.1 mm square test rods. The rods were prepared for tensile testing and tensile strength calculated at fracture. Type of fracture was examined under microscope.
Results: Leaving the adhesive uncured prior to composite repair placement increased the mean tensile values statistically significant for all adhesives tested, with or without silane pretreatment. Silane surface treatment improved significantly (p < 0.001) tensile strength values for all adhesives, both for the cured and uncured groups. The mean strength of the control composite was higher than the strongest repair strength (p < 0.001).
Conclusions: Application of freshly made silane and a thin bonding layer, rendered higher tensile bond strength. Not curing the adhesive before composite placement increased the tensile bond strength.
Introduction
The philosophy and restorative approach to refurbish or repair defective restorations has gradually been adopted by most western dental schools and dental practitioners [Citation1–4]. In a recent survey among Norwegian dentists, it was found that almost eight out of nine dentists preferred repair of failed restorations when damage was small [Citation5].
New composite can be retained to old composite through macro-mechanical undercuts and micromechanical interlocking to irregularities in the prepared composite surface and through chemical bonding to filler particles and organic matrix, even though the latter bonding option is reduced by time [Citation6–9]. There is growing evidence that repairing composites increases the longevity of the restorations and methods to achieve the best repair have been explored in a number of investigations [Citation10–12]. The majority of these investigations deal with different types of adhesives and surface treatments of the composite to be repaired. In addition to roughening with diamond burs, sandblasting, etching with hydrofluoric acid, lasers and silane application have been suggested. To date, there appears to be no consensus for the most appropriate way to prepare the substrate [Citation12].
In an earlier report by us, silane surface treatment was found significantly to improve repair strength [Citation13]. This finding is supported by others while some recent papers report no benefit of silane [Citation14–21].
Because of the high viscosity and low wetting potential of composite materials, adhesive agents have been used to optimize the composite to composite bonding [Citation22,Citation23]. Lower micro-tensile bond strength was observed for Single Bond (3M ESPE) as the adhesive layer between dentin and composite was increased from one layer to three layers, whereas no correlation could be found for the more fluid Clearfil SE (Kuraray) [Citation24]. Dall'Oca et al. stated that the interface between the aged composite and fresh composite remains the weakest zone of the restoration [Citation25]. It must, therefore, be desirable to decrease the thickness of the adhesive layer as much as possible. We found that in general a thinner bonding layer rendered a stronger repair bond [Citation13]. It is therefore, postulated that further limiting the adhesive layer thickness could create more hermetic bond between new and old composite.
The main objective was to evaluate the repair bond strength, using micro-tensile testing and different adhesives that were either cured before repair, as recommended by manufacturers, or left uncured when repair composite was placed. Furthermore, the effect of silane surface treatment on micro-tensile bond strength was evaluated. The tested null hypotheses were (1) The repair bond strength is independent of whether the adhesive is cured or not before placement of repair composite. (2) The repair bond strength is independent of silane pretreatment of the substrate and (3) The repair bond strength is independent of the type of adhesive used.
Materials and methods
All the restorative materials used in this study are listed in . The procedure and preparation of the composite blocks are summarized in . Eighty, shade A1B Filtek Supreme XLT composite blocks, 10 mm × 6.2 mm wide and 8 mm high, were fabricated in Teflon molds in accordance with the manufacturer’s instructions. The composite blocks were incrementally built in four layers and each layer cured for 40 s with a Demetron A2 corded LED curing light (Kerr Corp., Orange, CA). Upon removal from the mold, the specimens were further cured for 20 s on the surfaces covered by the mold. The light output was measured at 1100 mW/cm2 (Norwegian Radiation Protection Authorities, Österaas, Norway). As a control group, four composite blocks of the same diameter and 12 mm in height were also incrementally fabricated.
Figure 1. Schematic procedure of the specimen preparation and the improved micro-tensile bond strength test procedure.
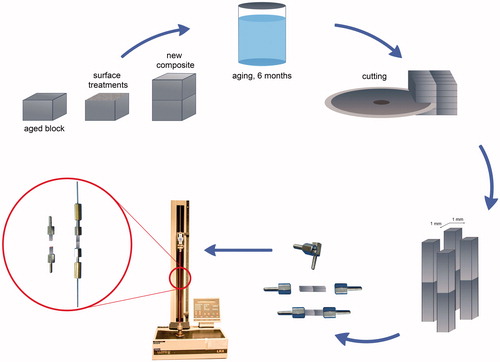
Table 1. Materials used in the investigation.
After polymerization, the composite blocks were immediately stored in distilled water for a total of two weeks [Citation26,Citation27]. The blocks were further aged by thermal cycling 5000 times between 5 and 55 °C, with a dwell time of 20 s and transfer time of 3 s. The eighty specimens were all surfaced on a 320 grit silicon carbide sandpaper disc (Struers, Copenhagen, Denmark) under running water for 5 s to obtain a flat surface with standardized roughness. For cleaning purposes, the test surfaces were acid etched with 37% phosphoric gel for 15 s and rinsed with water for another 15 s, also in the groups that received self-etching adhesives.
The 80 aged blocks were randomly divided into two experimental groups: Group A, no further surface treatment and Group B, the surface was coated with bis-silane, a two-part silane porcelain primer (BISCO Inc, Schaumburg, IL). The two parts were mixed and applied to the test surfaces with a small brush for 30 s and gently dried with air for 5–10 s to evaporate the solvent. Each experimental group (A and B) was further divided into subgroups, that each received different bonding systems for repair: (1) Adper Scotchbond Multi-Purpose (3M-ESPE), a three step etch and rinse adhesive. (2) Adper Scotchbond Multi-Purpose (3M-ESPE) Adhesive, where the primer was omitted and only the adhesive was used. (3) Adper Scotchbond Universal (3M-ESPE), a one-step self-etching adhesive. (4) Clearfil SE Bond (Kuraray America Inc, New York, NY), a two-step self-etching adhesive and (5) One Step Plus (BISCO Inc, Schaumburg, IL), a one-step self-etching adhesive. The adhesives were applied according to the manufacturer’s recommendations for placement of composite restorations except groups A2 and B2.
Each adhesive group was further divided into two subgroups; a and b. In groups a, the adhesive was cured according to the manufacturer’s suggestions, and in groups b, the adhesive was not cured before repair composite placement.
After surface treatment and adhesive application, the original mold was placed over the aged composite blocks and the first repair composite layer placed, using shade A3.5B to delineate the repair joint from the A1B substrate shade. To secure optimal adaptation of the repair material, the composite was placed to the middle of the specimen block to be repaired and adapted out to the margins with a small spatula. The second mold was then carefully fitted on the top and the composite further adapted and cured. The aged composite blocks were repaired in three approximately 2 mm incremental layers, the same way as the original aged specimen blocks, resulting in 14 mm high specimens. When the first composite repair layer was placed for the uncured group, the composite was also placed in the middle of the specimen and squeezed into the uncured adhesive and adapted to the sides. The uncured adhesive tended to be pushed to the side and was removed before placement of the second mold to avoid pooling or being mixed into the composite. After this, the cylinders were placed in distilled water for six months and thermo-cycled 5000 times. Control blocks (group C) were also thermo-cycled and stored for the same period of time.
The composite blocks were mounted on an automatic cutting machine (Metcon®, Miracut 201 Automatic Precision Cutter, Bursa, Turkey) equipped with a water cooled thin diamond blade. The specimens were serially sectioned perpendicular to the bonding surface both in the x and the y axis producing a number of square test specimen rods approximately 1.1 × 1.1 mm. Approximately 15 ± 3 test specimens were obtained from each composite block. The test specimens were cleaned ultrasonically in distilled water for 3 min. After the cleaning procedure, the test specimen rods were examined light microscopically at a magnification of 40× for voids and imperfections in the composite and the adhesive interphase and for evaluation of interphase thickness. Only flawless specimen rods were tested. The width and thickness of each test specimen was measured to the nearest 0.01 mm. using a calibrated digital caliber (Mitutoyo Co, Kawasaki, Japan).
Our recently published and much less time consuming method was used to attach the specimen rods to the bond testing machine [Citation13]. This attachment method was developed to secure more straight alignment of the specimen rods and, therefore, more uniform distribution of the tensile forces throughout the specimen. The 1.1 mm size of the test specimen rods was selected to fit into the female (hollow) end of 2 mm commercially available male/female extension screws (ELRA AS, Oslo, Norway) (). An extension screw was fitted to each end of the test specimen rods and secured with cyanoacrylate glue (Locktide 435, Hankel Norden, Gothenburg, Sweden). A special fitting mold was made to insure alignment of the screws to the long axis of the specimen.
Each test specimen was mounted in a calibrated Universal testing machine (Lloyd Instruments LTD, Model LRX, Fareham, England) using specially attached steel wires designed to transmit pure tensile forces to the specimen. The testing was conducted at a crosshead speed of 1 mm/min until fracture. The tensile bond strength of each test specimen was calculated in MPa, by dividing the imposed force (in Newtons) at fracture by the cross-sectional bond area (in mm2). The test specimens were maintained moist throughout the preparation and the test procedure.
The fracture surfaces were examined under a stereo microscope (American Optical, Buffalo, NY) at 40× magnification to determine if the failure region was within the adhesive zone or out of it. The adhesive zone was defined as the interphase between the old and the new composite. The failures were reported as cohesive or adhesive. Fracture in the adhesive zone was classified as adhesive failure.
Statistical calculations done were according to suggestions from ISO/TS 11405:2015 on treatment of results for testing of adhesion using Microsoft Excel 2010 [Citation27]. p values less than .05% were regarded as statistically significant.
Results
The results are presented in . All the repaired specimens in groups A1b and B1b, Scotchbond Multi-Purpose, uncured, failed in the adhesive layer when removed from the mold. A total of 51–66 usable specimen rods were obtained for each subgroup, a total of 1179 specimen rods for the whole study. The mean tensile strength of the control composite was 62.2 ± 5.29 MPa. The highest mean tensile strength in the repaired groups was for group B5b, One Step Plus, adhesive uncured (55.1 ± 10.12 MPa), and B3b, Scotchbond Universal, adhesive uncured (55.0 ± 8.71 MPa) closely followed by B4b, Clearfil SE, adhesive uncured (53.7 ± 9.10 MPa), all with mechanical roughening with sandpaper and silane surface treatments. This amounts to 88.6%, 88.4% and 86.3% of the strength of the control composite respectively. There was not statistically significant difference between these three groups (p > .05). The mean strength of the control composite was, however, significantly higher than the strongest repair strength (p < .001). The repair group that measured with the lowest mean tensile strength was group A1a, Scotchbond Multi-Purpose, mechanical roughening, adhesive cured, (27.8 ± 4.04 MPa). This amounts to 44.7% of the strength of the control composite.
Table 2. Results of micro-tensile testing in various groups of surface treatment and bonding systems.
Table 3. Group A, mechanical roughening with sandpaper. Results of statistical calculations evaluating the difference between sub-groups of adhesives.
Table 4. Group B, mechanical roughening with sandpaper and bis-silane treatment. Results of statistical calculations evaluating the difference between sub-groups of adhesives.
Table 5. The effects of silane treatment. Results of statistical calculations evaluating the difference between sub-groups of adhesives.
In general, leaving the adhesive uncured prior to composite repair placement increased the mean micro-tensile values statistically significantly for all adhesives, with or without silane pretreatment, except for group B2, Scotchbond Multi-Purpose, adhesive only, where it only showed a trend. For all adhesives in group A, mechanical roughening with sandpaper, the difference was highly significant (p < .001). In group B, mechanical roughening with sandpaper and bis-silane, the difference was highly significant for One Step Plus (p < .001), while somewhat less for Clearfil SE (p < .01) and Scotchbond Universal (p < .05). Furthermore, bis-silane surface treatment, in addition to mechanical roughening with sandpaper, improved significantly (p < .001) micro-tensile strength values for all adhesives, both for the cured and uncured adhesive groups. An exception is Scotchbond Multi-Purpose uncured both with and without silane application (groups A1b and B1b), where all specimen blocks failed adhesively when removed from the molds.
The thickness of the cured adhesive layer was approximately 5 μm for Clearfil SE and 20 μm for Scotchbond Universal and One Step. The thickness of the cured adhesive layer for Scotchbond Multi-Purpose varied more than for other adhesives, but it appeared mostly to be approximately 175 μm. For all the groups where the adhesive was left uncured before repair, the new composite seemed to be closely united with the substrate making the adhesive layer invisible to the eye.
The percentage of cohesive fractures is presented in . All the cohesive fractures occurred in the old composite. More cohesive fractures were found in the stronger repair groups. Most cohesive fractures were in groups B4b and B5b (19%), which also had the highest mean repair strength. In group A, mechanical roughening with sandpaper, all or almost all of the specimens failed adhesively where Scotchbond Multi-Purpose was used.
Discussion
Clinicians prefer the same procedure for both placing and repairing a restoration. The use of burs, followed by acid etching and application of a bonding agent, appeared to be used by over 80% of clinicians as a pretreatment for the old composite for repair [Citation5]. This was also the most commonly taught procedure for dental students in their curriculum [Citation2,Citation3,Citation23,Citation28].
The present study evaluated our assumption that the thinner the bond layers between two composites, the stronger the bond as suggested in an earlier study [Citation13]. The adhesive layer is regarded as the weakest part of the repair composite and by reducing this layer, the new and the old composite approach being one unit, similar to what was suggested for tooth fragment reattachment [Citation29]. By squeezing the repair composite into the uncured adhesive, the adhesive acts like a wetting agent occupying only the irregularities in the surface of the substrate. This study showed significantly increased bond strength for all adhesive groups when the adhesive was not cured before placement of the composite, both with and without bis-silane surface treatment, except Scotchbond Multi-Purpose three step (). The adhesive layer was not visible under light microscope in any group where the adhesive was uncured prior to composite placement, suggesting very intimate contact between old and new composite.
All specimens from groups A1b and B1b, Scotchbond Multi-Purpose uncured failed when being removed from the molds. This adhesive is in a group that has showed a great clinical success in posterior restorations in several studies trough the years [Citation30]. The failure occurred in the adhesive layer, which appeared not to have cured properly. It is believed that the repair composite squeezed the uncured adhesive from the surface of the old composite allowing intimate contact between the primer and the repair composite. The basic tertiary amine of the accelerator (co-initiator) for the photo-initiator in the repair composite is neutralized by ammonium groups formed from the acrylic acid and itaconic acid groups of the copolymer of the primer, and thereby the acceleration of radical formation is hindered for curing initiation [Citation31,Citation32].
Removing the superficial layer from an old composite and roughening with diamond bur are necessary to obtain micromechanical retention. In laboratory studies on composite repair, the standardized surface roughness is obtained by the use of silicon carbide sandpaper, simulating roughness obtained with a medium diamond bur [Citation13]. We observed using profile meter measurements that 320 grit sandpaper and medium diamond bur resulted in similar surface roughness. The adhesives tested were selected to represent the variety of adhesives available today. Scotchbond Multi-Purpose is a three step etch and rinse system and Clearfil SE, a two-step self-etch system, both with a water based primer. Scotchbond Universal is water/ethanol based and One Step Plus water/acetone based; both self-etch one step adhesives. Scotchbond Universal contains also small amounts of silane. The three self-etch adhesives rendered generally higher repair strength than the Scotchbond Multi-Purpose. Despite the difference in composition of monomer and solvents, the three self-etch adhesives all performed similarly. In a recent investigation using shear bond testing, Scotchbond Universal which contains some amount of silane, gave similar repair strength as Clearfil SE with preapplication of bis-silane [Citation17]. That finding was not supported by this study, where both adhesives were found to give similar repair bonding strength, with and without bis-silane preapplication.
Silane application increased bonding strength when repairing ceramic restorations [Citation33]. The use of silane has been reported to improve, reduce and have no effect on composite repair strength [Citation13,Citation17,Citation20,Citation21,Citation33–35]. In our earlier study, the highest repair strength was obtained using mechanical roughening, silane and an adhesive that rendered a thin bonding layer [Citation13]. Silane application is simple and safe and requires no extra armamentarium. Silane significantly increased micro-tensile bond strength for all adhesives tested and curing procedures (). Silane alone cannot replace the functions of an adhesive as a wetting agent that fills up surface irregularities in the substrate [Citation23]. It acts merely as an adhesion promoter or a coupling agent in addition to increase wettability [Citation36].
In most studies evaluating the effect of silane application on bond strength, one bottle prehydrolyzed silane solutions are used [Citation12,Citation20,Citation21,Citation34,Citation35,Citation37]. After opening the bottle, prehydrolyzed silane solutions have short shelf-life and may soon appear cloudy, losing the desired effect [Citation33]. In this study, two-bottle silane system was used which consists of unhydrolyzed silane in ethanol in one bottle and in acetic acid in the second one [Citation33]. Mixing of the two solutions initiates hydrolysis of the silane for use. This extends the life of the material considerably. Lundvall et al. found significantly higher bond strength when repairing porcelain with composite using two-bottle bis-silane, whereas one-bottle silane showed similar bond strength as the group without silane [Citation38]. The adhesion between resin based cement and dentin seemed not to be compromised if the dentin was exposed to silane [Citation39].
The possibility of obtaining chemical bond to a composite substrate decreases slowly in time due to post-curing and water uptake, leading to hydrolysis of available double bonds, leaving few carboxyl groups for chemical bonding to new composite [Citation8,Citation9,Citation40]. In laboratory studies on repair bond strength, aging of specimens is crucial for obtaining any meaningful results. A recent review article revealed that many studies used very short time span from fabrication of substrate specimens to repair composite placement and strength measurements [Citation37]. In 82% of studies the substrate specimens were only aged immersed in water, and in 44% of the studies for 48 h or less, without further aging treatment like thermal cycling. This short aging leads to overestimation of bond strength and makes comparison between surface treatments less meaningful. In specimens of six different composites aged only for few days the quantities of remaining methacrylate groups ranged from 25% to 48% [Citation41]. It has been demonstrated that under dry conditions it takes up to 14 days before the bond strength between the substrate and fresh composite starts to drop [Citation25]. It was, therefore, surprising that in a recent systematic review and meta-analysis, the minimum aging eligibility criteria for the substrate specimens was storage in water for only 24 h [Citation37]. Another peculiar eligibility criterion was the requirement for a control group, which was either untreated surface or ground composite surface with a dental bur or sandpaper without any adhesive layer. Both of these surfaces are never dealt with clinically. In laboratory studies, untreated surface is usually the Mylar™ matrix surface, exposing only resin. When a composite restoration is repaired, it is almost always resurfaced with a bur, exposing also filler particles. Furthermore, a composite repair most often includes both tooth structure and composite surface, where the use of an adhesive is mandatory. In this investigation, we decided to use the cohesive strength of the aged composite as a control for the desired or optimal repair strength. It is unrealistic to reach the cohesive strength of new material, since composite gradually loses strength as it ages [Citation13]. While there is no consensus on aging of either substrate composite or repaired specimens, it makes comparison between studies more realistic when the tensile strength of the aged specimens is used as control.
Preparation and application of specimens are critical for the results, since fractures within the substrate or the adherent can be technique related [Citation42]. Repair strength is force measured when the specimens fracture. If large portion of test specimens are cohesively fractured, little or no conclusion can be drawn from the results on repair strength. This has been the fact in a number of publications [Citation15,Citation20,Citation21,Citation34,Citation47,Citation48]. For example, in a recent investigation where more than 90% of specimens fractured cohesively the authors concluded that application of silane coupling agent did not improve the repair strength [Citation20]. Such statements are, to say the least, very misleading and based on misinterpretation of the results.
A recent review article reported that of all repair bond studies, 60% used shear testing [Citation37]. Some authors have criticized shear bond tests for producing stress concentrations in the substrate or the repair composite, leading to cohesive failures [Citation26,Citation43]. Heintze recommended shear testing to be abandoned due to critical and inadequate stress distribution and unreliable correlation to clinical outcome [Citation44]. This has led to an increase in the use of the time consuming and laborious micro-tensile testing, where more uniform stress distribution is believed to be obtained and the tensile forces concentrated in the interface to be tested [Citation45,Citation46]. Recently, Eliasson et al. [Citation13] introduced a much less time consuming micro-tensile testing method, where gluing the test rods into extension screws, attached to aligned long steel wires, secured more straight alignment of the test specimen. The tensile forces were also directed longitudinally from the ends of the specimen, distributing the forces more uniformly throughout the specimen. The many adhesive fractures observed in this investigation support this assumption and the results are more likely to represent the true repair strength. Based on the results all three hypotheses were rejected.
Conclusions
This investigation confirmed the results from our former study on composite repair, where application of freshly made silane and the use of a thin bonding layer rendered higher micro-tensile bond strength. The recommended procedure to obtain intimate contact between the two composites was to avoid curing the adhesive before composite placement. The composite repair became simpler and less time consuming by this procedure.
Clinical implication
A feasible clinical procedure for composite repair is after diamond bur roughening, acid etching and bis-silane application, to squeeze the repair composite into the uncured adhesive followed by curing.
Acknowledgements
The authors greatly appreciate and acknowledge the expert assistance of Mr. Erik Kleven for help in designing the micro-tensile testing procedure, Dr. Eystein I. Ruyter for valuable discussion on polymer chemistry and Mr. Jon-Eric Melsæter for drawing the schematic illustration. Thanks are also extended to Dr. Ronald K. Harris DDS, MSD for editorial assistance.
Disclosure statement
The authors report no conflicts of interest.
References
- Krejci I, Lieber CM, Lutz F. Time required to remove totally bonded tooth-colored posterior restorations and related tooth substance loss. Dent Mater. 1995;11:34–40.
- Blum IR, Lynch CD, Wilson NH. Teaching of direct composite restoration repair in undergraduate dental schools in the United Kingdom and Ireland. Eur J Dent Educ. 2012;16:e53–e58.
- Blum IR, Lynch CD, Wilson NH. Teaching of the repair of defective composite restorations in Scandinavian dental schools. J Oral Rehabil. 2012;39:210–216.
- Lynch CD, Blum IR, Frazier KB, et al. Repair or replacement of defective direct resin-based composite restorations: contemporary teaching in U.S. and Canadian dental schools. J Am Dent Assoc. 2012;143:157–163.
- Staxrud F, Tveit AB, Rukke HV, et al. Repair of defective composite restorations. A questionnaire study among dentists in the Public Dental Service in Norway. J Dent. 2016;52:50–54.
- Brosh T, Baharav H, Gross O, et al. The influence of surface loading and irradiation time during curing on mechanical properties of a composite. J Prosthet Dent. 1997;77:573–577.
- Malacarne J, Carvalho RM, de Goes MF, et al. Water sorption/solubility of dental adhesive resins. Dent Mater. 2006;22:973–980.
- Lagouvardos PE, Pissis P, Kyritsis A, et al. Water sorption and water-induced molecular mobility in dental composite resins. J Mater Sci Mater Med. 2003;14:753–759.
- Tarumi H, Torii M, Tsuchitani Y. Relationship between particle size of barium glass filler and water sorption of light-cured composite resin. Dent Mater J. 1995;14:37–44.
- Gordan VV, Garvan CW, Blaser PK, et al. A long-term evaluation of alternative treatments to replacement of resin-based composite restorations: results of a seven-year study. J Am Dent Assoc. 2009;140:1476–1484.
- Fernandez EM, Martin JA, Angel PA, et al. Survival rate of sealed, refurbished and repaired defective restorations: 4-year follow-up. Braz Dent J. 2011;22:134–139.
- Ozcan M, Koc-Dundar B. Composite-composite adhesion in dentistry: a systematic review and meta-analysis. J Adhes Sci Technol. 2014;28:2209–2229.
- Eliasson ST, Tibballs J, Dahl JE. Effect of different surface treatments and adhesives on repair bond strength of resin composites after one and 12 months of storage using an improved microtensile test method. Oper Dent. 2014;39:E206–E216.
- Hamano N, Chiang YC, Nyamaa I, et al. Effect of different surface treatments on the repair strength of a nanofilled resin-based composite. Dent Mater J. 2011;30:537–545.
- Maneenut C, Sakoolnamarka R, Tyas MJ. The repair potential of resin composite materials. Dent Mater. 2011;27:e20–e27.
- Özcan M, Barbosa SH, Melo RM, et al. Effect of surface conditioning methods on the microtensile bond strength of resin composite to composite after aging conditions. Dent Mater. 2007;23:1276–1282.
- Staxrud F, Dahl JE. Silanising agents promote resin-composite repair. Int Dent J. 2015;65:311–315.
- Imbery TA, Gray T, DeLatour F, et al. Evaluation of flexural, diametral tensile, and shear bond strength of composite repairs. Oper Dent. 2014;39:E250–E260.
- Tantbirojn D, Fernando C, Versluis A. Failure Strengths of Composite Additions and Repairs. Oper Dent. 2015;40:364–371.
- Cho SD, Rajitrangson P, Matis BA, et al. Effect of Er,Cr:YSGG laser, air abrasion, and silane application on repaired shear bond strength of composites. Oper Dent. 2013;38:E1–E9.
- da Costa TRF, Serrano AM, Atman APF, et al. Durability of composite repair using different surface treatments. J Dent. 2012;40:513–521.
- Ozcan M, Corazza PH, Marocho SMS, et al. Repair bond strength of microhybrid, nanohybrid and nanofilled resin composites: effect of substrate resin type, surface conditioning and ageing. Clin Oral Investig. 2013;17:1751–1758.
- Barcellos DC, Santos VMM, Niu LN, et al. Repair of composites: effect of laser and different surface treatments. Int J Adhes Adhes. 2015;59:1–6.
- Coelho PG, Calamia C, Harsono M, et al. Laboratory and FEA evaluation of dentin-to-composite bonding as a function adhesive layer thickness. Dent Mater. 2008;24:1297–1303.
- Dall'Oca S, Papacchini F, Goracci C, et al. Effect of oxygen inhibition on composite repair strength over time. J Biomed Mater Res Part B Appl Biomater. 2007;81:493–498.
- Van Noort R, Noroozi S, Howard IC, et al. A critique of bond strength measurements. J Dent. 1989;17:61–67.
- ISO/TS 11405:2015, Dentistry – testing of adhesion to tooth structure. 3rd ed. Geneva, Switzerland: International Standards Organization; 2015.
- Blum IR, Schriever A, Heidemann D, et al. The repair of direct composite restorations: an international survey of the teaching of operative techniques and materials. Eur J Dent Educ. 2003;7:41–48.
- Lise DP, Vieira LCC, Araujo E, et al. Tooth fragment reattachment: the natural restoration. Oper Dent. 2012;37:584–590.
- Van Meerbeek B, De Munck J, Yoshida Y, et al. Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper Dent. 2003;28:215–235.
- Ruyter IE, Monomer systems and polymerization. Utrect: Peter Szulc Publishing Co.; 1998.
- Nie J, Linden LA, Rabek JF, et al. A reappraisal of the photopolymerization kinetics of triethyleneglycol dimethacrylate initiated by camphorquinone-N,N-dimethyl-p-toluidine for dental purposes. Acta Polym. 1998;49:145–161.
- Lung CYK, Matinlinna JP. Aspects of silane coupling agents and surface conditioning in dentistry: an overview. Dent Mater. 2012;28:467–477.
- Rodrigues SA Jr, Ferracane JL, Della Bona A. Influence of surface treatments on the bond strength of repaired resin composite restorative materials. Dent Mater. 2009;25:442–451.
- Bonstein T, Garlapo D, Donarummo J Jr, et al. Evaluation of varied repair protocols applied to aged composite resin. J Adhes Dent. 2005;7:41–49.
- Ozcan M, Matinlinna JP, Vallittu PK. al. Effect of drying time of 3-methacryloxypropyl-trimethoxysilane on the shear bond strength of a composite resin to silica-coated base/noble alloys. Dent Mater. 2004;20:586–590.
- Valente LL, Sarkis Onofre R, Concalves AP, et al. Repair bond strength of dental composites: systemic review. Int J Adhes Adhes. 2016;69:15–26.
- Lundvall PK, Ruyter E, Ronold HJ, et al. Comparison of different etching agents and repair materials used on feldspathic porcelain. J Adhes Sci Technol. 2009;23:1177–1186.
- Graiff L, Piovan C, Vigolo P, et al. Shear bond strength between feldspathic CAD/CAM ceramic and human dentine for two adhesive cements. J Prosthodont. 2008;17:294–299.
- Burtscher P. Stability of radicals in cured composite materials. Dent Mater. 1993;9:218–221.
- Ruyter IE, Svendsen SA. Remaining methacrylate groups in composite restorative materials. Acta Odontol Scand. 1978;36:75–82.
- Gregory WA, Pounder B, Bakus E. Bond strengths of chemically dissimilar repaired composite resins. J Prosthet Dent. 1990;64:664–668.
- Della Bona A, van Noort R. Shear vs. tensile bond strength of resin composite bonded to ceramic. J Dent Res. 1995;74:1591–1596.
- Heintze SD. Clinical relevance of tests on bond strength, microleakage and marginal adaptation. Dent Mater. 2013;29:59–84.
- Scherrer SS, Cesar PF, Swain MV. Direct comparison of the bond strength results of the different test methods: a critical literature review. Dent Mater. 2010;26:E78–E93.
- Pashley DH, Carvalho RM, Sano H, et al. The microtensile bond test: a review. J Adhes Dent. 1999;1:299–309.
- Loomans BA, Cardoso MV, Roeters FJ, et al. Is there one optimal repair technique for all composites? Dent Mater. 2011;27:701–709.
- Hamano N, Chiang YC, Nyamaa I, et al. Repair of silorane-based dental composites: Influence of surface treatments. Dent Mater. 2012;28:894–902.