
To the editor,
Recently in this journal, a difference in the severity between two outbreaks of coronavirus disease 2019 (COVID-19), one in March and the other in November 2020, was reported from Lomardy, Italy, a region heavily affected by COVID-19 [Citation1]. Among various explanations discussed by the authors, mutations in SARS-CoV-2 were mentioned, although without data on the virus variants. We here focussed on the importance of detailed knowledge on the severity of disease of various SARS-CoV-2 variants. Therefore, in this paper, we aimed to summarise through systematic review and meta-analysis the overall risk of severe illness COVID-19 caused by delta variant relative to other variants of SARS-CoV-2 from observational studies.
We performed a systematic literature search with no language restriction in electronic databases, which included PubMed, Google Scholar, Scopus, and preprint servers (medRxiv, Research Square, SSRN), to identify published studies, dated up to December 23, 2021. The search strategy in the electronic databases was built based on the following keywords and their MeSH terms (if applicable): ‘COVID-19’, ‘SARS-CoV-2’, ‘b.1.617’, and ‘delta’. Studies eligible for inclusion were observational studies reporting the adjusted estimates for COVID-19 associated severe illness between patients with COVID-19 infected with delta variant of SARS-CoV-2 and those infected with other variants except the Omicron variant. Two investigators (CSK and SSH) independently performed the literature screening to identify eligible studies. The outcome of interest was COVID-19 associated with severe illness, for example, admission to the intensive care unit, the requirement for invasive or non-invasive ventilation, mortality, and/or as defined by the authors.
Two investigators (CSK and DSR) extracted the study characteristics, which included the first author's surname, year of publication, study design, country where the study was performed, total number of patients, proportion of patients who have been fully vaccinated, proportion of patients with severe illness, adjusted estimate for severe illness, and covariates adjusted in the analysis. Meta-analysis with the random-effects model was used to estimate the pooled odds ratio of severe illness in patients with COVID-19 infected with SARS-CoV-2 of delta variant relative to their counterparts infected with other SARS-CoV-2 variants, at 95% confidence intervals. We examined the heterogeneity between studies using the I2 statistics and the χ2 test, with significant heterogeneity predetermined at 50% and p < 0.10, respectively. Newcastle-Ottawa Scale was used for critical appraisal of the quality of included observational studies [Citation2]. Two investigators (CSK and SSH) independently evaluated the quality of studies, and a Newcastle-Ottawa Scale of at least 7 indicating high quality. Consensus discussions between the two investigators were carried out to resolve disagreements on the inclusion of studies, extraction of study characteristics, and quality appraisal. All statistical analyses were performed using Meta XL, version 5.3 (EpiGear International, Queensland, Australia).
Our systematic literature search retrieved 4190 hits, of which 1315 were unique (titles retrieved after removing duplications). After screening against eligibility criteria, five observational studies [Citation3–7] were included, with a total of 13,396 patients with COVID-19 being analysed. summarises the characteristics of the five included studies [Citation3–7]. Across the included studies [Citation3–7], all were retrospective in design, with four database reviews [Citation3,Citation4,Citation6,Citation7] and one single-centered studies [Citation5]. The included studies [Citation3–7] originated from Indonesia [Citation3], South Africa [Citation4], the United States [Citation5], Singapore [Citation6], and Qatar [Citation7]. The average age of patients across the included studies ranged from 7.0 to 43.0. Age and sex were the most commonly adjusted covariates, followed by the presence of various comorbidities. All the included studies [Citation3–7] were deemed high quality with a Newcastle-Ottawa Scale of 8 ().
Table 1. Characteristics of included studies.
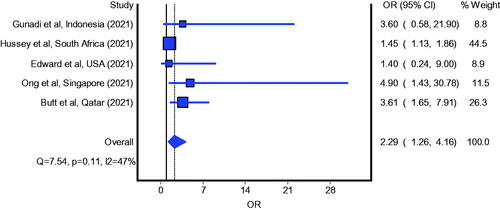
The definition of severe illness varied across the included studies; in both the studies reported by Gunadi et al. [Citation3] and Hussey et al. [Citation4] respectively, it was defined as COVID-19 associated mortality; in the study reported by Edward et al. [Citation5], as admission into intensive care unit; in the study reported by Ong et al. [Citation6], as need for oxygen therapy, admission into intensive care unit, or death; and in the study reported by Butt et al. [Citation7], as admission into intensive care unit, need for high-flow oxygen or mechanical ventilation, or death. The meta-analysis of five studies revealed significantly increased odds of severe illness in patients with COVID-19 infected with delta variant of SARS-CoV-2 relative to those infected with other SARS-CoV-2 variants; the estimated effect indicates increased severity (; pooled odds ratio = 2.29; 95% confidence interval: 1.26–4.16) and is with adequate evidence to reject the model hypothesis of ‘no significant difference’, at the current sample size.
Figure 1. Pooled odds ratio for mortality in patients with COVID-19 infected with SARS-CoV-2 of Delta variant compared to those infected with non-VOC.
The evidence to date pointed towards increased risk of severe illness in patients infected with SARS-CoV-2 of delta variant, compared to other SARS-CoV-2 variants (not Omicron variant), which might be due to the relatively increased viral load. Indeed, SARS-CoV-2 viral load has been identified as one of the predictors for disease severity in patients with COVID-19, and individuals infected with SARS-CoV-2 of delta variant could have viral loads up to 1260 times higher than those in people infected with the original strain [Citation8]. In addition, two of the S mutations of delta variant, namely L452R and the T478K, possibly lead to increased binding of Spike protein to angiotensin converting enzyme 2 (ACE2) and the stabilisation of the ACE2-Spike protein receptor binding domain (RBD) complex, and hence even more significant downregulation of ACE2, which could contribute to the pathogenicity. Regardless of the mechanisms, increased severity in patients with COVID-19 caused by delta variant suggests the need to develop assays that can rapidly distinguish circulating variants. Furthermore, our findings indicate that targeted interventions in patients infected with SARS-CoV-2 of delta variant should be considered, such as implementing a lower threshold for the initiation of pharmacotherapies which can reduce the risk of progression to severe illness (e.g. monoclonal antibodies [Citation9]). Importantly, in some of the included studies [Citation4,Citation5,Citation7], despite higher proportion of patients infected with delta variant had been fully vaccinated at the time of diagnosis, they were still at a higher risk of progressing to severe illness, suggesting reduced effectiveness of COVID-19 vaccines to protect against severe illness from COVID-19 caused by delta variant compared to other variants.
It should be noted that the studies included in our systematic review and meta-analysis are of the retrospective design, and thus the potential existence of biases and confounders and the inherent weakness to establish causal relationship. In addition, some of the included studies [Citation3,Citation6] are of small sample size and with wide confidence interval, which precludes precise risk estimates. Therefore, we await larger prospective studies in the future to confirm our findings. Lastly, due to a lack of studies available at the time of literature search, it is not possible to compare the risk of severe illness between patients infected with SARS-CoV-2 of delta variant and of Omicron variant.
Author contributions
CSK: Conceptualisation, Methodology, Writing – Original draft preparation; DSR: Data curation, Writing – Reviewing and editing; SSH: Methodology, Formal analysis, Writing – Reviewing and editing.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
References
- Borghesi A, Golemi S, Carapella N, et al. Lombardy, Northern Italy: COVID-19 second wave less severe and deadly than the first? A preliminary investigation. Infect Dis. 2021;53(5):370–375.
- Wells G, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2013. [cited 2021 Dec 24]. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- Gunadi Hakim MS, Wibawa H, Setiawaty V, et al. Is the infection of the SARS-CoV-2 Delta variant associated with the outcomes of COVID-19 patients? Front Med. 2021;8:780611.
- Hussey H, Davies MA, Heekes A, et al. Higher mortality associated with the SARS-CoV-2 Delta variant in the Western Cape, South Africa, using RdRp target delay as a proxy. medRxiv. 2021;2021.10.23.21265412.
- Edward PR, Lorenzo-Redondo R, Reyna ME, et al. Severity of illness caused by severe acute respiratory syndrome coronavirus 2 variants of concern in children: a single-center retrospective cohort study. Preprint. medRxiv. 2021;2021.10.23.21265402.
- Ong SWX, Chiew CJ, Ang LW, et al. Clinical and virological features of SARS-CoV-2 variants of concern: a retrospective cohort study comparing B.1.1.7 (alpha), B.1.315 (beta), and B.1.617.2 (Delta). Clin Infect Dis. 2021:ciab721.
- Butt AA, Dargham SR, Chemaitelly H, et al. Severity of illness in persons infected with the SARS-CoV-2 Delta variant vs beta variant in Qatar. JAMA Intern Med. 2022;182(2):197.
- Li B, Deng A, Li K, et al. Viral infection and transmission in a large well-traced outbreak caused by the Delta SARS-CoV-2 variant. Nat Commun. 2022;13(1):460.
- Kow CS, Ramachandram DS, Hasan SS. The use of neutralizing monoclonal antibodies and risk of hospital admission and mortality in patients with COVID-19: a systematic review and meta-analysis of randomized trials. Immunopharmacol Immunotoxicol. 2022;44(1):28–34.