
To the Editor,
Recently in this journal a comparison of hospital treatment guidelines and antibiotic use in Nordic hospitals was reported [Citation1]. Despite similar resistance rates among gram negative bacteria, differences in guidelines occurred for pyelonephritis and sepsis. We here evaluate the impact of infectious diseases consultation (IDC) on the outcomes among patients with infections caused by Gram-negative rod (GNR) bacteria.
This systematic literature review and meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement [Citation2] and the Meta-Analysis of Observational Studies in Epidemiology (MOOSE) guidelines [Citation3]. The review protocol was registered on the International Prospective Register for Systematic Reviews (PROSPERO) and is publicly available (CRD42021276285). Institutional review board approval was not required. The systematic literature search was performed on 11/21/2021 by a health sciences librarian (R. J. S.) trained in systematic review searching, using subject headings and keywords created for PubMed, Embase, Web of Science, CINAHL, and Cochrane CENTRAL. Original research manuscripts or abstracts which assessed the effect of IDC on mortality in patients with GNR infections were included. Our study focussed on studies with results adjusted for confounders. Editorials, review articles, commentaries, and animal studies were excluded. All potentially relevant studies collected were divided and independently screened by three of the reviewers (S.H., S.K. and H.S.).
Two of five independent reviewers (S.H., S.K., J.T., A.R.M., and T.K.) abstracted data from each study using a standardized abstraction form. Details of each study were tabulated, including study design, study period, population characteristics, source of GNR infections, isolated GNR species including the proportion that were drug resistant, and mortality. H.S. reviewed abstraction forms and served as a tie breaker. Fourteen authors were contacted for additional information, and five were able to provide additional information. The Downs and Black scale were used to evaluate the quality of the included studies. All questions were answered as intended except for question #27 regarding Power, which was changed to a yes/no answer with associated points. The primary outcome was all-cause mortality in studies reporting adjustment for confounders. We used adjusted odds ratios (ORs) when available, and crude or unadjusted numbers otherwise. The pooled OR and 95% confidence interval (CI) were calculated using random-effect models with inverse variance weighting. Heterogeneity was assessed with I2 estimation and the Cochran’s Q statistic test. A funnel plot was constructed to assess the publication bias, and the Harbord and Egger method was used to assess publication bias using the R 4.1.2 software. All meta-analyses were conducted using the Cochrane Review Manager (RevMan) version 5.4.
Among 5533 articles screened, a total of 21 studies met the inclusion criteria and were included in the final qualitative systematic literature review. Fifteen articles were excluded because it did not have complete data for the meta-analysis, did not adjust for confounders, or did not report the result for multivariable analysis, leaving six studies for quantitative synthesis [Citation4–9]. All of these six articles were retrospective cohort studies (). The proportion of patients who received IDC in each study was ranged from 41.2 to 72.1%. When the results of the six studies were pooled, IDC was associated with improved mortality with minimal heterogeneity (pooled OR = 0.19, 95%CI: 0.13 − 0.28, I2 = 20%) ().
Figure 1. Forest plots of the associations between infectious diseases consultation and mortality among patients with infections due to Gram-negative rod bacteria. CI: confidence interval; IDC: infectious diseases consultation; IV: inverse variance weighting; NIDC: non-infectious diseases consultation; SE: standard error.
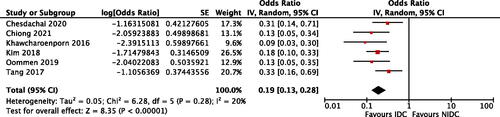
Table 1. Summary of the six studies included in the meta-analysis.
In addition to mortality, one study reported additional effects of IDC such as shorter inappropriate antibiotic duration, more frequent oral de-escalation in a timely manner, and surgical source control among patients with Pseudomonas aeruginosa bacteraemia [Citation5].
Although publication bias was suspected by the funnel plot method, there was no statistically significant evidence of publication bias when using the Harbord and Egger’s regression test.
Our systematic review and meta-analysis found that IDC was significantly associated with lower mortality among patients with GNR infections with minimal heterogeneity. As all of the included studies were retrospective cohort studies, confounding by patient characteristics could exist. For example, ID specialists are often consulted for critically ill or immunocompromised cases but not all GNR infections. Adjusting for factors associated with patient characteristics and treatment process is especially important, since GNR bacteria (including non-fermenters or MDR-GNRs) commonly infect chronically ill or immunosuppressed patients. Therefore, we believe the insights gained from this analysis may suggest the effectiveness of IDC in patients with GNR infections.
Our systematic literature review revealed that the rate of IDC varied greatly in patients with GNR infections. Given the association with improved survival demonstrated in our meta-analysis, IDC should be considered for wider populations with GNR infections, though we could not conclude which subpopulations benefitted the most from IDC. Further prospective data collection is required to answer this question.
Our study has several limitations. First, all of the studies included were retrospective studies and most of the studies did not originally aim to compare patients with IDC to those without IDC. Unmeasured confounders are likely to remain such as confounding by use of appropriate empiric antimicrobials. Second, there is a potential for publication bias although Harbord and Egger’s regression test was not statistically significant.
In conclusion, our study suggested that IDC might improve the outcomes of patients with GNR infections. Prospectively collected clinical information and patient characteristics in each study would help us to establish a greater degree of accuracy and the precise mechanisms how IDC might improve outcomes of patients with GNR infections.
Acknowledgments
The authors thank Drs. Jonathan D. Baghdadi, Kimberly C. Claeys, Christopher A. Jankowski, Tristan T. Timbrook, Renato Pascale and Zhiyong Zong for providing additional information about their studies. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Möller V, Östholm-Balkhed Å, Berild D, et al. Antibiotic resistance among pathogens compared to hospital treatment guidelines and antibiotic use in nordic hospitals 2010-2018. Infect Dis. 2021;53(8):607–618.
- Moher D, Liberati A, Tetzlaff J, PRISMA Group, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
- Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–2012.
- Chesdachai S, Kline S, Helmin D, et al. The effect of infectious diseases consultation on mortality in hospitalized patients with methicillin-resistant staphylococcus aureus, candida, and pseudomonas bloodstream infections. Open Forum Infect Dis. 2020;7(1):ofaa010.
- Chiong F, Wasef MS, Liew KC, et al. The impact of infectious diseases consultation on the management and outcomes of Pseudomonas aeruginosa bacteraemia in adults: a retrospective cohort study. BMC Infect Dis. 2021;21(1):671.
- Khawcharoenporn T, Chuncharunee A, Maluangnon C, et al. Active monotherapy and combination therapy for extensively drug-resistant Pseudomonas aeruginosa pneumonia. Int J Antimicrob Agents. 2018;52(6):828–834.
- Kim I, Kim WY, Jeoung ES, et al. Current status and survival impact of infectious disease consultation for multidrug-resistant bacteremia in ventilated patients: a single-center experience in korea. Acute Crit Care. 2018;33(2):73–82.
- Oommen JK, Cani E, Zeana C, et al. The 30-Day readmission and 30-Day mortality of hemodialysis patients with antibiotic-resistant gram-negative bacteremia. Open Forum Infect Dis 2018;6:S114.
- Tang G, Huang L, Zong Z. Impact of infectious disease consultation on clinical management and outcome of patients with bloodstream infection: a retrospective cohort study. Sci Rep. 2017;7(1):12898.