
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
As a response to the emergence of the new Omicron SARS-CoV-2 variant, on December 3, 2021, mandatory testing after entry to Norway was extended to include international travellers with a valid COVID-19 certificate. We aim to validate if mandatory testing upon arrival increased the proportion of travellers confirmed with a positive COVID-19 test after entry.
Methods
We used individual level data on registered travellers linked with data on COVID-19 testing and confirmed COVID-19 cases. The proportions of confirmed cases among international travellers before and after the requirement were introduced was analysed with an interrupted times series design.
Results
The proportion of travellers with an EU COVID-19 certificate tested at an official test station increased from 3% to 43% after mandatory testing was introduced. However, the proportion of all travellers confirmed with COVID-19 rose only marginally with 0.14 percentage point directly after the intervention (p-value .06). The results are limited by the absence of data on antigen tests taken by the traveller at home and missing data from travellers without a valid Norwegian ID.
Conclusions
Our findings suggest that the benefit of mandatory testing of all international travellers to Norway was marginal in the period directly after the emergence of the omicron variant. This result must be understood in the context of free of charge testing at official test centres, a government recommendation on a low threshold to test when experiencing symptoms in addition to limited surveillance of the compliance of the test after arrival requirement.
Introduction
COVID-19 screening after international travel has been mandatory in many countries during the pandemic, but its effectiveness in detecting infected travellers remain largely unexplored. In this study we assessed the added value of a mandatory testing requirement in early December 2021 in Norway.
As a response to rising numbers of COVID-19 cases, the Norwegian government expanded the number of persons that had to register entry to Norway by reintroducing mandatory registration for persons 16 years or older with a valid EU Digital COVID-19 Certificate on 26 November 2021 (https://www.regjeringen.no/no/aktuelt/nye-tiltak-ved-innreise-til-norge/id2888683/). Prior to this, registration and testing on arrival was only mandatory for travellers without a valid EU Digital COVID-19 Certificate. Six days later (2 December 2021), after the discovery of the omicron-variant, the government issued changes to the COVID-19 Regulations that stipulated that also persons arriving in Norway with a valid EU Digital COVID-19 Certificate must have a COVID-19 antigen test taken at the border (in effect from December 3), or if limited capacity at the border, within 24 h after arrival (https://www.regjeringen.no/no/aktuelt/alle-som-kommer-til-norge-ma-teste-seg-etter-ankomst/id2890574/). The traveller could, in the latter case, choose whether the test would be taken at a public testing station or at home. Tests taken at home were not monitored by a health professional. If the home-test was positive, the traveller was obliged to confirm the test result with a PCR test within 24 h.
The time interval of one week between the new requirement to register all travellers entering Norway and the introduction of mandatory testing allowed us to examine the relationship between the testing requirement on arrival and the proportion of travellers who were confirmed with COVID-19 after entry, using a pre-post design. If mandatory testing increased the proportion of detected cases among travellers to Norway, we should see a shift in the proportion of confirmed cases on arrival from before to after the requirement was implemented. The aim of this study was to investigate whether mandatory testing of travellers led to the detection of a higher proportion of cases among incoming travellers to Norway with an EU Digital COVID-19 Certificate. The requirement was introduced in a context when the Norwegian population was encouraged by authorities to have a low threshold for testing when symptomatic and when testing was free of charge at official test centres.
Materials and methods
Data was obtained from the Norwegian Institute of Public Health’s (NIPH) Emergency preparedness register for COVID-19 (Beredt-C19) [Citation1], including data from the digital entry registration system, provided by the Directorate for Civil Protection and Emergency Planning. Data from the entry registration system, e.g. COVID-19 certificate status, is self-registered, and may be erroneous, but since what the traveller registered did not affect whether the traveller could enter Norway during the study period, there is no reason to assume that this source of error changed from before to after the mandatory testing requirement entered into force.
Within Beredt C-19, data on entry can be linked to the National Population Registry through the unique personal identification number (PID). For persons registered with a valid PID it is possible to track whether they have been tested for COVID-19 at an official test station after entering Norway which is registered in the Norwegian Surveillance System for Communicable Diseases (MSIS). Travellers who were registered as tested on arrival were tested within day 0 and day 2 after the arrival date recorded in the digital entry registration system. Tests taken at home were not recorded in MSIS. To evaluate the reliability of the self-registered data on the EU Digital COVID Certificate, data on COVID-19 vaccination from the Norwegian Immunisation Registry (SYSVAK) was added based on the PID. SYSVAK records all COVID-19 vaccines administered in Norway, consequently correspondence between COVID-19 certificate status and vaccine status should be high, but not perfect as the pass could also be valid if the person had recently recovered from COVID-19 or if the vaccine was administered abroad.
We first calculated the proportion tested on arrival before and after mandatory testing was introduced and calculated the 95% binomial confidence interval for this proportion.
In the main analysis the outcome was the daily proportion of travellers, registered with a valid PID and self-registered as having a valid COVID-19 certificate, testing positive for COVID-19 at an official test station on arrival. We conducted an interrupted time series study by running a segmented linear regression model [Citation2–4]:
where
represents the outcome, at time t,
is a dummy variable coded as 0 in the pre-intervention period and 1 post-intervention and
is the time of the interruption.
represents the pre-intervention slope,
indicates changes in level immediately after the intervention, and
whether the slope has changed after the intervention. We tested for autocorrelation using Breusch-Godfrey test of first order.
Results
From November 26 to December 12, we found 412 520 registered travellers to Norway. Data on 6 681 travellers registered before 26 November 2021, lacked information on EU COVID-19 Certificate and was not included. summarises the sample before (26 Nov 2021–2 Dec 2021) and after mandatory testing was introduced (3 Dec 2021–12 Dec 2021). The average number of persons who registered each day did not change due to testing requirement. The correspondence between COVID-19 vaccine status as reported in SYSVAK and self-registration was high (above 90%). 113 804 travellers (29% of all travellers) did not provide a valid PID on registering their arrival and were thus not included in the analysis.
Table 1. Averaged daily number of travellers and COVID-19 test results, with and without EU COVID Certificate before (26.11.2021–02.12.2021), and after (03.12.2021–12.12.2021) mandatory testing for all.
Before mandatory testing was introduced, on average 568.9 daily arrivals were tested at an official testing station, with an average of 40.9 daily detected cases (on average 0.24% of all incoming travellers with a valid PID). After mandatory testing was introduced, 7 183.1 daily arrivals were tested, with an average of 65.6 cases (0.39% of all travellers with a valid PID).
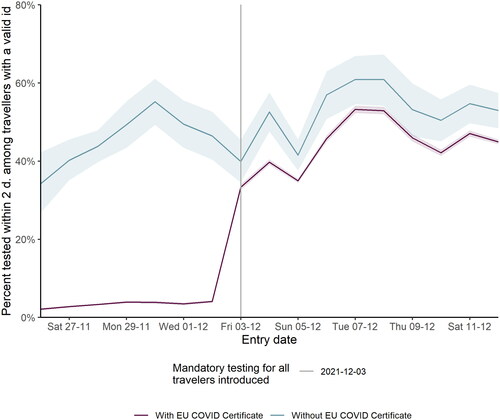
shows the proportion of all incoming travellers with an EU COVID-19 Certificate and a valid PID who were tested for COVID-19 on arrival. For persons with an EU COVID-19 Certificate, the proportion tested rose from 3.4% to 42.6% after the introduction of mandatory testing. Some travellers were exempted from the requirement, but they likely pertain to a very small proportion of all travellers.
Figure 1. Proportion of travellers tested at an official test station before and after mandatory testing for all was introduced.
shows the estimates from the interrupted times series model. As the Breusch-Godfrey test of first order autocorrelation was non-significant (p-value .93), the model was fitted with OLS. The coefficient of changes in level after the intervention was 0.0014 (p-value .06, 95% CI −0.00009 0.00293), and represents a 0.14 percentage point jump in the proportion who tested positive after the intervention. The coefficient of the slope shows no changes over time (p-value .034). The results are visualised in .
Figure 2. Proportion of travellers testing positive shown with dots, estimated best fit based on interrupted time series analysis shown as purple line. Orange line show the extension of the fit before interruption. Confidence band based a 95% confidence interval around the predicted values.
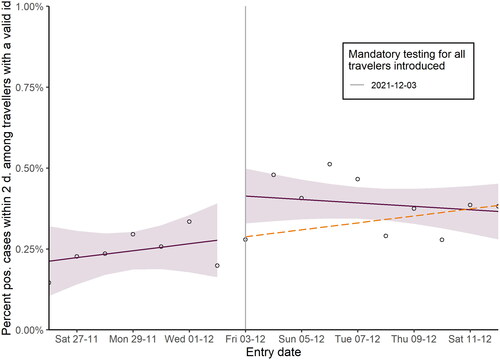
Table 2. Parameter estimates with 95% confidence interval in parenthesis.
The purple lines show the estimated trend before and after interruption. The counterfactual trend, i.e. the linear trend expected without the intervention, is shown in orange. The effect was not sustained over time, as the orange line and the purple line cross a few days after the interruption.
Discussion
The interrupted time analysis showed that introduction of mandatory testing of fully vaccinated persons was associated with only a slight increase in the proportion of confirmed cases on arrival, but the effect did not persist.
Mandatory testing at the border is logistically demanding and can lead to undesired effects such as gatherings of people due to queuing for testing. During the studied period, the test capacity in Norway was also increasingly under pressure. The added value of the measure must be weighed against the test capacity and the domestic and international incidence rates, as well as against other measures imposed at the border.
There are several explanations for the very slight increase of the proportion of confirmed cases. Firstly, travellers are often required to provide a negative test result prior to travel. Secondly, the test and trace policy might have effectively detected close contacts before the introduction of the requirement. Thirdly, the results could reflect lack of compliance with the new requirements. Lastly, in this time period the recommendation for the Norwegian population was to have a low threshold for testing when symptomatic, so symptomatic travellers with COVID-19 was most likely also detected before the mandatory testing was required.
A few modelling and observational studies have examined the effectiveness of screening at the border [Citation5,Citation6]. Generally, certainty of the evidence for many of the traveller related control measures is low [Citation6]. The overwhelming majority of studies examining screening, evaluated symptom/exposure‐based screening measures rather than test-based screening. The studies which looked at test-based- screening mainly looked at PCR-testing
One modelling study which examined the latter found that testing travellers reduced imported or exported cases as well as secondary cases [Citation7]. Observational studies [Citation8–12] reported that the proportion of cases detected among all positive cases varied from 58% to 90%, by comparing the number of PCR-positive persons on arrival with the number of persons testing positive during quarantine. Our studies suggest that many of these cases may have been detected regardless of whether testing was mandatory or not.
Our study is limited by missing results from home tests. Thus, we cannot determine the degree of compliance with the testing requirements, and the marginal increase in the proportion of travellers detected may also reflect a lack of compliance to the requirement, although the large increase in the proportion tested at an official test station suggests otherwise.
The testing requirement may be introduced as a mean to reduce mobility, as the requirement may deter leisure travel, and such reductions in mobility may in turn curb the spread of COVID-19. We did not evaluate whether the requirement had such an effect. Furthermore, the introduction of omicron is also expected to have led to a decrease in the number of travellers as a consequence of changes in restrictions in departure countries as well as in Norway.
The introduction of mandatory testing after entry after the emergence of the omicron variant, only marginally increased the proportion of detected cases among travellers with an EU COVID Certificate. The cost-benefit of screening incoming travellers should be compared with detecting more cases in the general population, e.g. by targeted measures based on test and trace recommendations and a low threshold for testing persons with symptoms.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Emergency preparedness register for COVID-19 (Beredt C19) [Internet]. Norwegian Institute of Public Health. 2021 [cited 2021 May 5]. https://www.fhi.no/en/id/infectious-diseases/coronavirus/emergency-preparedness-register-for-covid-19/
- Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. 2017;46(1):348–355.
- Wagner AK, Soumerai SB, Zhang F, et al. Segmented regression analysis of interrupted time series studies in medication use research. J Clin Pharm Ther. 2002;27(4):299–309.
- Kontopantelis E, Doran T, Springate DA, et al. Regression based quasi-experimental approach when randomisation is not an option: interrupted time series analysis. BMJ. 2015;350:h2750.
- Bou-Karroum L, Khabsa J, Jabbour M, et al. Public health effects of travel-related policies on the COVID-19 pandemic: a mixed-methods systematic review. J Infect. 2021;83(4):413–423. Oktober
- Burns J, Movsisyan A, Stratil JM, et al. International travel‐related control measures to contain the COVID‐19 pandemic: a rapid review. Cochrane Database Syst Rev. 2021;3:CD013717.
- Dickens BL, Koo JR, Lim JT, et al. Strategies at points of entry to reduce importation risk of COVID-19 cases and reopen travel. J Travel Med. 2020;27(8):taaa141.
- Al-Qahtani M, AlAli S, AbdulRahman A, et al. The prevalence of asymptomatic and symptomatic COVID-19 in a cohort of quarantined subjects. Int J Infect Dis. 2021;102:285–288.
- Al-Tawfiq JA, Sattar A, Al-Khadra H, et al. Incidence of COVID-19 among returning travelers in quarantine facilities: a longitudinal study and lessons learned. Travel Med Infect Dis. 2020;38:101901.
- Arima Y, Kutsuna S, Shimada T, July the COVID-19 Response Team, et al. Severe acute respiratory syndrome coronavirus 2 infection among returnees to Japan from wuhan, China, 2020. Emerg Infect Dis. 2020;26(7):1596–1600.
- Shaikh Abdul Karim S, Md Tahir FA, Mohamad UK, et al. Experience repatriation of citizens from epicentre using commercial flights during COVID-19 pandemic. Int J Emerg Med. 2020;13(1):50.
- Ng OT, Marimuthu K, Chia PY, et al. SARS-CoV-2 infection among travelers returning from wuhan, China. N Engl J Med. 2020;382(15):1476–1478.